Abstract
Neutrophil activation can release neutrophil extracellular traps (NETs) in acute inflammation. NETs result in the release of human neutrophil elastase (HNE) and calprotectin, where the former can degrade the latter and generate protein fragments associated with neutrophil activity. We investigated this in chronic obstructive pulmonary disease (COPD) and idiopathic pulmonary fibrosis (IPF) using the novel neoepitope biomarker CPa9-HNE, quantifying a specific HNE-mediated fragment of calprotectin in serum. CPa9-HNE was compared to total calprotectin. Initially, CPa9-HNE was measured in healthy (n = 39), COPD (n = 67), and IPF (n = 16) serum using a neoepitope-specific competitive enzyme-linked immunosorbent assay. Then, a head-to-head comparison of CPa9-HNE and total calprotectin, a non-neoepitope, was conducted in healthy (n = 19), COPD (n = 25), and IPF (n = 19) participants. CPa9-HNE levels were significantly increased in COPD (p < 0.0001) and IPF subjects (p = 0.0001) when compared to healthy participants. Additionally, CPa9-HNE distinguished IPF (p < 0.0001) and COPD (p < 0.0001) from healthy participants more effectively than total calprotectin for IPF (p = 0.0051) and COPD (p = 0.0069). Here, CPa9-HNE also distinguished IPF from COPD (p = 0.045) participants, which was not observed for total calprotectin (p = 0.98). Neutrophil activity was significantly higher, as assessed via serum CPa9-HNE, for COPD and IPF compared to healthy participants. Additionally, CPa9-HNE exceeded the ability of non-neoepitope calprotectin serum measurements to separate healthy from lung disease and even COPD from IPF participants, indicating that neutrophil activity is essential for both COPD and IPF.
1. Introduction
Chronic obstructive pulmonary disease (COPD) affects millions globally and is a disease driven by inflammation where events of acute exacerbations significantly worsen respiratory symptoms [1,2]. The pathological manifestations and individual disease course are highly heterogeneous [2,3], for which classification systems have been developed to better stratify disease management [4]. Idiopathic pulmonary fibrosis (IPF) is an interstitial lung disease characterized by progressive pulmonary fibrosis and a severe disruption of the balance in extracellular matrix (ECM) remodeling but also inflammatory events that include increased neutrophil recruitment and activation [5]. IPF is a fast-progressing disease with a median survival of 3–5 years from the time of diagnosis [6,7]. Due to the heterogeneity between patients within both IPF and COPD, the disease progression is hard to predict. However, an early diagnosis could benefit patients due to earlier treatment initiation, potentially slowing disease progression. Additionally, the identification of disease phenotypes may enable personalized healthcare. Thus, new biomarkers with a diagnostic and/or a prognostic value are of interest for both COPD and IPF [2,6].
Neutrophils are a highly abundant immune cell type in human blood, act as first responders to tissue injury, and have a high turnover during pathological conditions [8]. Neutrophils have a rapid decay in blood when compared to other leukocytes; therefore, it is a requirement that assessment needs to be performed within hours after blood collection and their isolation, which may prove difficult in practice [9,10,11]. As part of the acute immune response, they are swiftly recruited to the site of injury, where they may interact with cellular and ECM components [12]. When the neutrophil is activated, neutrophil extracellular traps (NETs) are released via vital or suicidal NETosis as a response to inflammation induced by pathogens or other stimuli [13,14]. In vital NETosis, neutrophils can release secretory vesicles in the form of NETs. As part of suicidal NETosis, the neutrophil will undergo cell lysis and cell death to release NETs. Calprotectin is a heterodimeric protein mainly produced by neutrophils but also expressed by other immune cells such as macrophages and monocytes [15]. Calprotectin constitutes up to 60% of neutrophilic cytosolic protein content and is released in abundance as part of a NET response; however, passive calprotectin release from neutrophils has also been shown [15,16]. Furthermore, human neutrophil elastase (HNE) is released during a NET event and cleaves the otherwise proteolytically resistant calprotectin [17,18]. Calprotectin has various extracellular biological purposes, the most extensively studied function being its properties as a potent antimicrobial agent, which inhibits pathogen growth by scavenging and withholding transition metals [19,20]. Studies have indicated that released calprotectin can also act as a chemotactic trigger for immune cells and promote cell adhesion [21]. Additionally, subunits and complexes of calprotectin have been shown to stimulate the expression of pro-inflammatory cytokines at varying degrees, ultimately promoting an inflammatory state further [22,23,24,25]. Apart from inflammation-related responses, calprotectin has been suggested as an inducer of cell apoptosis [26,27,28,29]. Interestingly, previous findings have also indicated that the S100A9 subunit can promote fibroblast proliferation in vitro [30].
An increase in NETs in the sputum has previously been observed for COPD during acute exacerbations, where this increase also correlated to a disease in severity as determined by the Global Initiative for Obstructive Lung Disease (GOLD) classification system [31,32]. Furthermore, an increase in neutrophil activity and intact calprotectin has been associated with IPF phenotypes [5,33]. Previously, calprotectin has been suggested as a therapeutic target for IPF treatment, albeit inflammation and the role of immunity remain a debated subject regarding IPF pathology [34,35]. Immune suppressant treatment has been indicated to have a harmful effect, suggesting that the interplay of the immune system and fibrosis is complex, and the exact immune modulation approach may matter [36,37]. New tools are required to enable assessments that reflect the neutrophil activity or NETosis. Recently, the formation of a specific fragment of calprotectin generated by HNE, the neoepitope CPa9-HNE, has been described [16]. This neoepitope has been shown to be generated by activated, but not inactive, neutrophils in vitro. Furthermore, the stability of the neoepitope was demonstrated in stored blood samples, whereas calprotectin and neutrophils are known to have a short half-life in blood [38,39]. Thus, CPa9-HNE represents a novel and robust method of assessing neutrophil activity in blood by assessing the neoepitope of a specific degradation fragment. We hypothesized that CPa9-HNE could be a novel tool to further elucidate disease mechanisms related to neutrophil activity in COPD and IPF by a simple measurement of the generated neoepitope in stored serum samples since CPa9-HNE reflects the secretion and the degradation of calprotectin that is generated by activated neutrophils. Therefore, we investigated neutrophil activity in the serum of healthy, COPD, and IPF subjects by quantifying CPa9-HNE. Additionally, a head-to-head comparison of this newly developed CPa9-HNE assay and a commercial assay for a total calprotectin in serum was conducted to investigate if there was a difference in diagnostic power between a non-neoepitope and a neoepitope-specific calprotectin assay in IPF and COPD.
2. Materials and Methods
2.1. Disease Cohorts
CPa9-HNE levels were assessed in serum samples from 39 healthy controls, 16 IPF participants, and 67 clinically stable COPD participants. Additionally, serum samples were collected four weeks later at a follow-up visit for 25 of the COPD participants who were clinically stable. For the second part of this study that compared CPa9-HNE with total calprotectin in the serum, 19 healthy controls, 19 IPF participants, and the 25 COPD participants that participated in the follow-up visit were evaluated using each assay head-to-head. Serum samples were stored at −80 °C until biomarker assessments.
After informed consent and approval by the appropriate Institutional Review Board/Independent Ethical Committee were obtained, the serum was collected from participants and healthy controls. Healthy and IPF subject samples were obtained from the commercial vendors BioIVT (West Sussex, UK) and Discovery Life Science (Los Osos, CA, USA), where available basic demographics are shown in Table 1. Serum samples from participants with COPD were collected for an observational study as described previously [40]. The study complies with the Declaration of Helsinki and Good Clinical Practice Guidelines; moreover, it has been approved by the local ethics committee (protocol number H-6-2013-014) [40]. All participants provided written informed consent before the performance of all study-related assessments. Inclusion criteria were a diagnosis of COPD made by a senior physician and forced expiratory volume during the first second (FEV1) was <80% of the predicted value. The exclusion criterion was an acute exacerbation of COPD leading to hospitalization within four weeks prior to blood sampling.

Table 1.
Basic demographics for healthy, IPF, and COPD participants for the two cohorts.
2.2. Biomarker Assessments
Calprotectin degradation mediated via HNE was quantified by targeting a specific degradation fragment in a stored serum using the robust, competitive enzyme-linked immunosorbent assay (ELISA) CPa9-HNE, as described previously (cat. no. 1031AE01, Nordic Bioscience, Herlev, Denmark) [16]. Briefly, CPa9-HNE quantifies a highly specific neoepitope of calprotectin in the S100A9 subunit generated via HNE. Biomarker values outside the quantification range were assigned either the lower or upper limit of quantification, as appropriate. Total calprotectin (S100A8/S100A9) measurements in the serum were conducted with a commercially available sandwich ELISA (cat. no. EK-MRP8/14, Bühlmann Laboratories, Schönenbuch, Switzerland) that did not target a neoepitope.
2.3. Statistical Analysis
Basic demographics were compared between groups using the Kruskal–Wallis χ2 test and two-tailed Mann–Whitney t-test, as appropriate. Indications of confounding effects were investigated with respect to age, sex, and body mass index (BMI) when available. A statistically significant difference between the disease groups and the healthy group was determined using the Kruskal–Wallis test with Dunn’s multiple comparisons test. A receiver-operating characteristics (ROC) curve analysis was used to determine the specificity and sensitivity of the disease groups compared to the healthy controls for the serum CPa9-HNE. FEV1% predicted and forced vital capacity (FVC) % predicted were evaluated for their correlation to CPa9-HNE levels using Spearman’s correlation test. Furthermore, for the 25 COPD subjects that had participated in a follow-up visit, CPa9-HNE levels were compared between the two time points using a two-tailed Wilcoxon matched-pairs signed-rank test. Lastly, a statistically significant difference was investigated for CPa9-HNE and the commercial calprotectin assay independently using a Kruskal–Wallis test with Dunn’s multiple comparisons test. A receiver-operating characteristics (ROC) curve analysis was used to determine the specificity and sensitivity between all subject groups in the serum for the CPa9-HNE (neoepitope) and the commercial total calprotectin (non-neoepitope) assay.
3. Results
3.1. Basic Demographics
Basic characteristics are listed in Table 1 for healthy controls, IPF, and COPD participants in cohorts 1 and 2. A significant difference in age was found between the subject groups, with healthy controls being the youngest in both cohorts 1 and 2. This mostly held true for each participant group in cohort 1 when conducting pairwise comparisons of age between healthy and COPD (p < 0.0001), healthy and IPF (p = 0.0051), but was not observed between the COPD and IPF participant groups (p = 0.1). In cohort 2, a statistical difference was found for all participant groups when conducting a pairwise comparison analysis for differences in age (p ≤ 004). Overall, sex distribution was also significantly different between the groups, which remained the case in cohort 1 for pairwise comparisons between healthy and COPD (p = 0.01), IPF and COPD (p = 0.001), with the exception of the IPF and healthy (p = 0.1) participant group. When conducting pairwise comparisons of the participant sex distribution in cohort 2, statistical significance was found between IPF and COPD (p = 0.005), IPF and healthy (p = 0.0009), but not between healthy and COPD (p = 0.4). The mean FVC % predicted was similar between COPD and IPF subjects when data were available. As expected, the mean FEV1% predicted was significantly lower for COPD compared to IPF subjects when data were available. Most COPD participants had severe disease by the GOLD standards; however, they were considered stable in disease at all visits.
3.2. Neutrophilic Activity, Quantified by the Neoepitope-Specific CPa9-HNE Assay, Is Significantly Increased in COPD and IPF Participants
Serum CPa9-HNE levels for healthy, COPD, and IPF subjects are illustrated in Figure 1A. A significant increase was seen in COPD (baseline median 247.4 [IQR 179.2–334.7] ng/mL, p < 0.0001) and IPF (median 161.0 [IQR 82.86–238.5] ng/mL, p = 0.0001) as compared to healthy subjects (median 18.94 [IQR 18.32–32.29] ng/mL). When comparing IPF and COPD participants of cohort 1, a trend was observed for the COPD group having a higher biomarker level than the IPF group (p = 0.06). A ROC analysis for COPD versus healthy subjects had an area under the curve (AUC) of 1.00 (95% CI 1.00–1.00, p < 0.0001; Figure 1B). IPF subjects had an AUC of 0.97 (95% CI 0.93–1.00) when compared to healthy controls (p < 0.0001; Figure 1C). To evaluate the stability of CPa9-HNE over time, 25 of the clinically stable COPD subjects were re-evaluated in serum at a four-week visit. CPa9-HNE levels remained stable over the four-week period with no significant change in concentration (follow-up median 273.8 [IQR 190.7–433.3] ng/mL, p = 0.0588), as shown in Figure 1D.
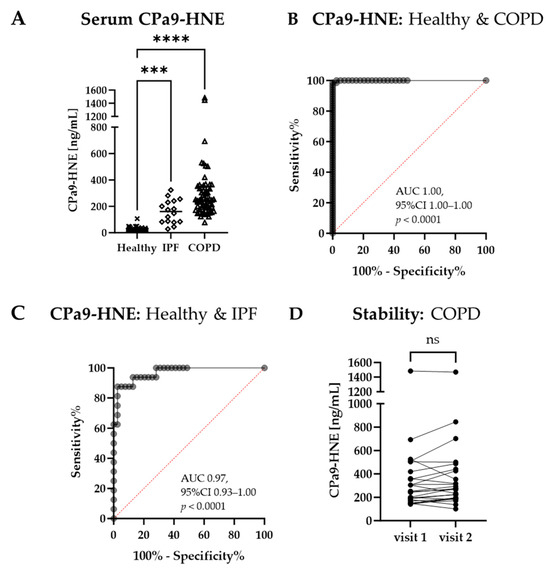
Figure 1.
Diagnostic potential of CPa9-HNE in COPD and IPF. (A) Serum CPa9-HNE levels in healthy (n = 39), COPD (n = 67), and IPF (n = 16). Data are shown as scatter dot plots with the median indicated with a line and individual participant values of healthy controls indicated with an X shape, IPF indicated with a diamond shape, and COPD indicated with a triangle shape. A statistically significant difference was determined using the Kruskal–Wallis test with Dunn’s multiple comparisons test comparing the COPD and IPF to the healthy subjects. (B) ROC analysis of COPD subjects as compared to healthy controls. (C) ROC analysis of IPF subjects as compared to healthy controls. (D) A parallel dot plot comparing serum CPa9-HNE levels at two visits four weeks apart for 25 clinically stable COPD participants, where data were analyzed using a two-tailed Wilcoxon matched-pairs signed rank. 95% CI, 95% confidence interval; AUC, area under the curve; IPF, idiopathic pulmonary fibrosis; COPD, chronic obstructive pulmonary disease; ns, no significance; and ROC, receiver-operating characteristics. *** p < 0.001; and **** p < 0.0001.
The clinical parameters listed in Table 1 for cohort 1 were investigated for associations with CPa9-HNE serum levels. FVC % predicted and CPa9-HNE showed a mild but significant negative correlation in COPD participants (r = −0.2577, p = 0.0488); however, not in IPF (r = 0.1859, p = 0.491). Healthy females (32.29 [IQR 18.32-47.33] ng/mL) had significantly higher CPa9-HNE levels than healthy males (18.32 [IQR 18.32-23.02] ng/mL; p = 0.0468). However, this difference was not observed for COPD participants (p = 0.975). No correlation between age and CPa9-HNE was found for any groups (p ≥ 0.3). Similarly, no correlation was found between BMI and CPa9-HNE in COPD participants (p = 0.8).
3.3. The Neoepitope CPa9-HNE Had Superior Diagnostic Power to Identify Disease and Healthy Participants Compared to Non-Neoepitope Measurements in the Serum
The calprotectin neoepitope CPa9-HNE was compared head-to-head with a commercial assay for total calprotectin. As seen in Figure 2A, a significant increase in the neoepitope CPa9-HNE for both COPD and IPF participants was again observed when compared to the healthy controls in this cohort: CPa9-HNE levels were significantly elevated in COPD (median 273.8 [IQR 190.7–433.3] ng/mL, p < 0.0001) and IPF (120.3 [IQR 81.40–211.0] ng/mL, p = 0.0005) as compared to healthy controls (median 44.04 [IQR 44.04–46.52] ng/mL). Moreover, COPD subjects had significantly higher CPa9-HNE levels than IPF (p = 0.0111). As seen in Figure 2D, non-neoepitope calprotectin serum levels were also significantly elevated in COPD (median 182.7 [IQR 63.14–332.9] µg/mL, p = 0.0219) and IPF (median 208.5 [IQR 128.8–303.4] µg/mL, p = 0.0137) when compared to healthy controls (median 94.69 [IQR 61.46–185.3] µg/mL). However, there was no significant difference between COPD and IPF participants for non-neoepitope total calprotectin measurements (p > 0.9999). CPa9-HNE biomarker levels had an AUC of 1.00 for both IPF (95% CI 0.99–1.00, p < 0.0001) and COPD (95% CI 1.00–1.00, p < 0.0001) when compared to healthy controls (Figure 2B,C). Total serum calprotectin levels in IPF and COPD had an AUC of 0.76 (95% CI 0.60–0.90, p = 0.0051) and 0.75 (95% CI 0.60–0.91, p = 0.0069), respectively, when compared to healthy controls (Figure 2E,F). Additionally, CPa9-HNE biomarker levels had an AUC of 0.68 (95%CI 0.52–0.84), p = 0.045) between IPF and COPD subjects, where total calprotectin had an AUC of 0.50 (95%CI 0.33–0.67, p = 0.98). Clinical parameters listed in Table 1 for cohort 2 were investigated for associations of CPa9-HNE or non-neoepitope calprotectin levels. For the COPD participants, a negative correlation was found for FVC % predicted and CPa9-HNE (r = −0.458, p = 0.0280) but not when measuring calprotectin (r = 0.178, p = 0.418). No correlation was found for FEV % predicted for CPa9-HNE (r = 0.249, p = 0.251) or intact calprotectin (r = −0.258, p = 0.234) measurements. No correlations were found between any of the remaining parameters listed or biomarker measurements.
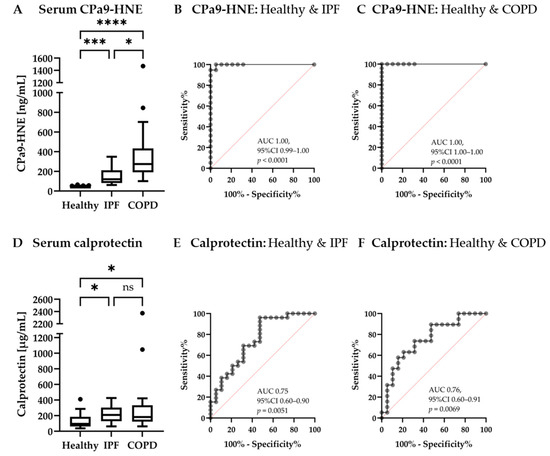
Figure 2.
Diagnostic potential of CPa9-HNE (neoepitope) and calprotectin (non-neoepitope) measurements for serum CPa9-HNE (A) and serum calprotectin (D) levels were compared for 19 healthy controls; 19 participants with an IPF diagnosis, and the 25 COPD participants in a head-to-head comparison, showing data as Tukey’s boxplot with possible outliers indicated as dots ROC analysis was performed for CPa9-HNE in IPF (B) and COPD (C) when compared to healthy controls, as well as for total calprotectin in IPF (E) and COPD (F) when compared to healthy controls. 95% CI, 95% confidence interval; AUC, area under the curve; IPF, idiopathic pulmonary fibrosis; COPD, chronic obstructive pulmonary disease; ns, no significance; and ROC, receiver-operating characteristics. * p < 0.05; *** p < 0.001; and **** p < 0.0001.
4. Discussion
In the current study, we showed that serum CPa9-HNE was highly upregulated in COPD and IPF compared to healthy controls. Interestingly, the neoepitope-specific marker, CPa9-HNE, separated the disease groups from the healthy group to a larger extent than non-neoepitope measurements for calprotectin in a head-to-head comparison. The serological biomarker CPa9-HNE is associated with the degradation of calprotectin via HNE, which is generated during a NET response from neutrophils [16], thus reflecting the neutrophil activity assessed in stored serum samples. COPD is characterized by chronic inflammation [2,41], which is in line with the current results showing highly elevated serum levels of CPa9-HNE compared to healthy controls. IPF is mainly characterized by fibrosis; however, participants may experience chronic inflammation to some extent [5], which is also in line with the results shown in this study, where CPa9-HNE was significantly increased in IPF compared to healthy controls but to a lesser extent for total calprotectin. CPa9-HNE was able to identify COPD and IPF subjects from healthy controls with high AUCs as computed using ROC analyses. Hence, neutrophil activity may be distinctly different when comparing COPD and IPF to healthy participants. Additionally, CPa9-HNE serum levels in COPD were significantly increased compared to IPF in cohort 2 (Figure 2A) while showing a trend in cohort 1 (Figure 1A), which is in line with COPD having chronic inflammation as a disease hallmark and while fibrotic changes better characterize IPF.
Levels of the serum CPa9-HNE remained stable over a four-week period in COPD participants that were deemed clinically stable, suggesting that CPa9-HNE does not fluctuate and is a stable measure of neutrophil activity over time. Despite the lack of a recent exacerbation event for these COPD participants, a distinct observation was the two outliers with very high serum CPa9-HNE. None of the available basic demographics could explain the very high levels seen in these individuals. However, the participant who participated in the follow-up visit remained clinically stable and at a stable high CPa9-HNE level over time. This suggests that even high levels of neutrophil activity may be found in stable participants, indicating a stable inflammatory state.
It has previously been reported that there is no association between age and BMI with CPa9-HNE serum levels [16], which is in line with observations in this study when data were available. Previously, low BMI has been related to disease severity in COPD in addition to progression, risk of hospitalization, mortality, and tolerability to certain therapies in IPF [42,43]. Thus, a limitation of this study includes the lack of BMI data for the IPF and healthy participant group, even though current data do not indicate this. In the healthy group, a difference was observed between sexes within cohort 1, but this was not the case in any other group in this study. It was not possible to establish if there was a sex-related difference in the IPF group due to the low number of females present in both cohorts. Thus, a limitation of this study was the participants not being matched in age or sex, which could potentially have an effect on their CPa9-HNE levels, although the data of this study or others do not suggest this. In previous studies, serum CPa9-HNE levels for healthy controls have been reported at a median of 42.7 ng/mL [16], which is in line with the second healthy control group (n = 19, median 44.04 ng/mL) but different from the control group in cohort 1 (n = 39, median 18.94 ng/mL). Limited information was available for the healthy control groups for both cohorts, where future studies with more comprehensive information might offer a more precise characterization of CPa9-HNE in healthy subjects.
In general, CPa9-HNE was not associated with spirometry measures, albeit a negative correlation between FVC and CPa9-HNE was shown in the COPD participants. No correlation was observed for FVC and FEV1 with IPF and COPD, respectively. However, it is more appropriate to consider CPa9-HNE as a measure of disease activity rather than severity when considering that it is generated during NETosis from activated neutrophils as part of inflammation [16]. Therefore, we theorize that CPa9-HNE might be seen in flares during periods of high disease activity when observed over time for the participant, whereas levels would be expected to be lower in periods of inactive disease. This is supported by previous observations in inflammatory bowel diseases, where CPa9-HNE serum levels correlated with endoscopic disease activity for ulcerative colitis and Crohn’s disease [16]. However, future studies are needed to fully elaborate on the role of CPa9-HNE related to disease activity and/or the severity in COPD and IPF with larger and well-described cohorts. Since CPa9-HNE reflects neutrophil activity, it might potentially predict and characterize inflammatory events more easily than current tools. Currently, the rapid decay of neutrophils in blood samples usually demands neutrophil activity assessment quickly after blood collection [11,44], where neutrophilic count does not reflect disease activity. In contrast, the stability of CPa9-HNE neoepitope storage has been shown in serum samples by testing neoepitope recovery over at least four freeze/thaw cycles and storage at room temperature for >24 h and longer at 4 °C [16].
The neoepitope-specific CPa9-HNE biomarker was compared to the commercial MRP8/14 assay, measuring total non-neoepitope calprotectin in a direct comparison. Significantly elevated levels of both CPa9-HNE and total calprotectin were found for both COPD and IPF compared to healthy controls. However, CPa9-HNE had the best ability to distinguish the disease groups from the healthy reference group, where the AUC for CPa9-HNE in IPF and COPD was equal to 1.00, and the AUC for non-neoepitope calprotectin measurements in IPF and COPD were 0.75 and 0.76, respectively, thus showing a relevance for neoepitope measurements in disease characterization. Moreover, it was also possible to distinguish IPF from COPD participants (Figure 2A) using CPa9-HNE, which was not possible with measurements of total calprotectin (Figure 2D). These results highlight the difference between measuring a specific cleavage site mediated by protease activity, a neoepitope, in calprotectin versus measuring total calprotectin since the neoepitope signifies both release of calprotectin but also its degradation with HNE at the specific cleavage site [16,45]. Moreover, it has also been demonstrated that different neoepitopes, despite their same protein origin, have different meanings, e.g., some being indicators of protein production while others proteolytic degradation [46,47,48], highlighting that the specific epitope is important [49].
Limitations to the current study include the lack of data availability on smoking history for the IPF and healthy participant groups, where it would be interesting to incorporate smoking history for all participant groups to investigate and compare biomarker levels between all participant groups. Future studies should aim to include this information. Additionally, the subject groups investigated in this study had a lower number of participants, non-matched in clinical parameters; therefore, this study served as a proof-of-concept study that should be expanded upon in the future.
5. Conclusions
We have demonstrated in this study that calprotectin degradation via HNE is significantly upregulated in COPD and IPF, signified by the serological biomarker CPa9-HNE that quantifies a neoepitope of a calprotectin degradation fragment that is associated with neutrophil activity. The results of this study support that neutrophil activity is an essential common denominator for both disease indications, which can be easily assessed even in stored serum samples via CPa9-HNE. COPD subjects had the most pronounced increase in CPa9-HNE, which is in line with it being a more inflammatory-driven disease. Moreover, CPa9-HNE was better at distinguishing the groups of healthy, COPD, and IPF than total calprotectin serum measurements, highlighting the importance of assessing neutrophil activity in these participants and the benefit of neoepitope measurements in connection with lung diseases. Future studies are needed to elucidate the role of neutrophil activity and the full potential of CPa9-HNE as a neoepitope-specific biomarker for the lung diseases investigated here and other diseases with an inflammatory component.
Author Contributions
All authors participated in data analysis and interpretation. A.H.H. had primary responsibility for statistical analyses. J.H.M. developed the CPa9-HNE assay and provided guidance related to assay performance. J.M.B.S., D.J.L. and M.A.K. contributed with continuous academic guidance throughout the study. A.H.H. drafted the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by the Danish Research Foundation.
Institutional Review Board Statement
All participants provided written informed consent before performing all study-related assessments. According to the qualified vendors BioIVT and Discovery Life Science, healthy and IPF sample collection was collected in compliance with the Ethics Committee recommendations, where all guidelines, regulations, and best practices meet or exceed the US and EU regulatory requirements. COPD participants were collected as part of an observational study, which complies with the Declaration of Helsinki and Good Clinical Practice Guidelines that were approved by the Capital Region of Denmark Ethics Committee (protocol number H-6-2013-014).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets and/or data analysis generated during the study are not publicly available due to restrictions of Danish data protection laws; however, they are available from the corresponding author upon reasonable request.
Acknowledgments
The authors acknowledge everyone involved with this work, herein participants and medical, nursing, and technical staff involved with serum samples. Furthermore, the technical staff were involved with biomarker assessments.
Conflicts of Interest
All authors are employees at Nordic Bioscience A/S, a company involved with the discovery and development of biomarkers where S.R.R., J.H.M. M.A.K., D.J.L. and J.M.B.S. are shareholders. A.H.H., J.H.M., M.A.K., D.J.L. and J.M.B.S. contributed to the invention of CPa9-HNE.
Abbreviations
The area under the curve (AUC), body-mass index (BMI), chronic obstructive pulmonary disease (COPD), specific calprotectin protein fragment generated by human neutrophil elastase (CPa9-HNE), enzyme-linked immunosorbent assay (ELISA), forced expiratory volume during the first second (FEV1), forced vital capacity (FVC), Global Initiative for Obstructive Lung Disease (GOLD), human neutrophil elastase (HNE), idiopathic pulmonary fibrosis (IPF), neutrophil extracellular traps (NETs), receiver operating characteristics (ROC), standard deviation (SD), and years (yrs).
References
- Gershon, A.S.; Warner, L.; Cascagnette, P.; Victor, J.C.; To, T. Lifetime risk of developing chronic obstructive pulmonary disease: A longitudinal population study. Lancet 2011, 378, 991–996. [Google Scholar] [CrossRef]
- Brandsma, C.; Berge, M.V.D.; Hackett, T.; Brusselle, G.; Timens, W. Recent advances in chronic obstructive pulmonary disease pathogenesis: From disease mechanisms to precision medicine. J. Pathol. 2020, 250, 624–635. [Google Scholar] [CrossRef]
- Pavord, I.D.; Jones, P.W.; Burgel, P.-R.; Rabe, K.F. Exacerbations of COPD. Int. J. Chron. Obstruct Pulmon. Dis. 2016, 11, 21. [Google Scholar] [PubMed]
- Aramburu, A.; Arostegui, I.; Moraza, J.; Barrio, I.; Aburto, M.; García-Loizaga, A.; Uranga, A.; Zabala, T.; Quintana, J.M.; Esteban, C. COPD classification models and mortality prediction capacity. SSRN Electron. J. 2019, 14, 605–613. [Google Scholar] [CrossRef] [PubMed]
- O’Dwyer, D.N.; Ashley, S.L.; Moore, B.B. Influences of innate immunity, autophagy, and fibroblast activation in the pathogenesis of lung fibrosis. Am. J. Physiol.-Lung Cell. Mol. Physiol. 2016, 311, L590–L601. [Google Scholar] [CrossRef] [PubMed]
- Brett, L.; Harold, R.C.; Talmadge, E.K.J. Clinical course and prediction of survival in ideopathic pulmonary fibrosis. Am. J. Respir. Crit. Care Med. 2011, 183, 431–440. [Google Scholar]
- Wolters, P.J.; Blackwell, T.S.; Eickelberg, O.; E Loyd, J.; Kaminski, N.; Jenkins, G.; Maher, T.M.; Molina-Molina, M.; Noble, P.W.; Raghu, G.; et al. Time for a change: Is idiopathic pulmonary fibrosis still idiopathic and only fibrotic? Lancet Respir. Med. 2018, 6, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Kolaczkowska, E.; Kubes, P. Neutrophil recruitment and function in health and inflammation. Nat. Rev. Immunol. 2013, 13, 159–175. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, A.; Beard, L.J.; Thong, Y.H. Early decay of human neutrophil chemotactic responsiveness following isolation from peripheral blood. Clin. Exp. Immunol. 1980, 39, 532–537. [Google Scholar]
- Oh, H.; Siano, B.; Diamond, S. Neutrophil isolation protocol. J. Vis. Exp. 2008, 17, 745. [Google Scholar]
- Monceaux, V.; Chiche-Lapierre, C.; Chaput, C.; Witko-Sarsat, V.; Prevost, M.-C.; Taylor, C.T.; Ungeheuer, M.-N.; Sansonetti, P.J.; Marteyn, B.S. Anoxia and glucose supplementation preserve neutrophil viability and function. Blood 2016, 128, 993–1002. [Google Scholar] [CrossRef] [PubMed]
- Padmanabhan, J.; Gonzalez, A.L. The Effects of Extracellular Matrix Proteins on Neutrophil-Endothelial Interaction—A Roadway to Multiple Therapeutic Opportunities. Yale J. Biol. Med. 2012, 85, 167–185. [Google Scholar] [PubMed]
- Li, T.; Zhang, Z.; Li, X.; Dong, G.; Zhang, M.; Xu, Z.; Yang, J. Neutrophil Extracellular Traps: Signaling Properties and Disease Relevance. Mediat. Inflamm. 2020, 2020, 9254087. [Google Scholar] [CrossRef] [PubMed]
- Yipp, B.G.; Kubes, P. NETosis: How vital is it? Blood 2013, 122, 2784–2794. [Google Scholar] [CrossRef] [PubMed]
- Stříž, I.; Trebichavský, I. Calprotectin—A pleiotropic molecule in acute and chronic inflammation. Physiol. Res. 2004, 53, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Mortensen, J.H.; Sinkeviciute, D.; Manon-Jensen, T.; Domislović, V.; McCall, K.; Thudium, C.S.; Brinar, M.; Önnerfjord, P.; Goodyear, C.S.; Krznarić, Z.; et al. A specific calprotectin neo-epitope [CPa9-HNE] in serum from inflammatory bowel disease patients is associated with neutrophil activity and endoscopic severity. J. Crohn’s Colitis 2022, 16, 1447–1460. [Google Scholar] [CrossRef] [PubMed]
- Stephan, J.R.; Nolan, E.M. Calcium-induced tetramerization and zinc chelation shield human calprotectin from degradation by host and bacterial extracellular proteases. Chem. Sci. 2015, 7, 1962–1975. [Google Scholar] [CrossRef]
- Nacken, W.; Kerkhoff, C. The hetero-oligomeric complex of the S100A8/S100A9 protein is extremely protease resistant. FEBS Lett. 2007, 581, 5127–5130. [Google Scholar] [CrossRef]
- Hood, M.I.; Skaar, E.P. Nutritional immunity: Transition metals at the pathogen–host interface. Nat. Rev. Microbiol. 2012, 10, 525–537. [Google Scholar] [CrossRef]
- Monteith, A.J.; Skaar, E.P. The impact of metal availability on immune function during infection. Trends Endocrinol. Metab. 2021, 32, 916–928. [Google Scholar] [CrossRef]
- Ryckman, C.; Vandal, K.; Rouleau, P.; Talbot, M.; Tessier, P.A. Proinflammatory activities of S100: Proteins S100A8, S100A9, and S100A8/A9 induce neutrophil chemotaxis and adhesion. J. Immunol. 2003, 170, 3233–3242. [Google Scholar] [CrossRef]
- Cesaro, A.; Anceriz, N.; Plante, A.; Pagé, N.; Tardif, M.R.; Tessier, P.A. An inflammation loop orchestrated by S100A9 and calprotectin is critical for development of arthritis. PLoS ONE 2012, 7, e45478. [Google Scholar] [CrossRef]
- Simard, J.C.; Cesaro, A.; Chapeton-Montes, J.; Tardif, M.; Antoine, F.; Girard, D.; Tessier, P.A. S100A8 and S100A9 induce cytokine expression and regulate the NLRP3 inflammasome via ROS-dependent activation of NF-κB1. PLoS ONE 2013, 8, e72138. [Google Scholar] [CrossRef]
- Gao, H.; Hou, J.; Meng, H.; Zhang, X.; Zheng, Y.; Peng, L. Proinflammatory effects and mechanisms of calprotectin on human gingival fibroblasts. J. Periodontal Res. 2017, 52, 975–983. [Google Scholar] [CrossRef]
- Marinković, G.; Grauen Larsen, H.; Yndigegn, T.; Szabo, I.A.; Mares, R.G.; De Camp, L.; Weiland, M.; Tomas, L.; Goncalves, I.; Nilsson, J.; et al. Inhibition of pro-inflammatory myeloid cell responses by short-term S100A9 blockade improves cardiac function after myocardial infarction. Eur. Heart J. 2019, 40, 2713–2723. [Google Scholar] [CrossRef] [PubMed]
- Qin, F.; Song, Y.; Li, Z.; Zhao, L.; Zhang, Y.; Geng, L. S100A8/A9 induces apoptosis and inhibits metastasis of CasKi human cervical cancer cells. Pathol. Oncol. Res. 2010, 16, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Zali, H.; Rezaei-Tavirani, M.; Kariminia, A.; Yousefi, R.; Shokrgozar, M.A. Evaluation of growth inhibitory and apoptosis inducing activity of human calprotectin on the human gastric cell line (AGS). Iran. Biomed. J. 2008, 12, 7–14. [Google Scholar] [PubMed]
- Shabani, F.; Mahdavi, M.; Imani, M.; Hosseinpour-Feizi, M.A.; Gheibi, N. Calprotectin (S100A8/S100A9)-induced cytotoxicity and apoptosis in human gastric cancer AGS cells: Alteration in expression levels of Bax, Bcl-2, and ERK2. Hum. Exp. Toxicol. 2020, 39, 1031–1045. [Google Scholar] [CrossRef] [PubMed]
- Yui, S.; Nakatani, Y.; Hunter, M.J.; Chazin, W.J.; Yamazaki, M. Implication of extracellular zinc exclusion by recombinant human calprotectin (MRP8 and MRP14) from target cells in its apoptosis-inducing activity. Mediat. Inflamm. 2002, 11, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Shibata, F.; Ito, A.; Ohkuma, Y.; Mitsui, K.-I. Mitogenic Activity of S100A9 (MRP-14). Biol. Pharm. Bull. 2005, 28, 2312–2314. [Google Scholar] [CrossRef][Green Version]
- Grabcanovic-Musija, F.; Obermayer, A.; Stoiber, W.; Krautgartner, W.-D.; Steinbacher, P.; Winterberg, N.; Bathke, A.C.; Klappacher, M.; Studnicka, M. Neutrophil extracellular trap (NET) formation characterises stable and exacerbated COPD and correlates with airflow limitation. Respir. Res. 2015, 16, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Dicker, A.J.; Crichton, M.L.; Pumphrey, E.G.; Cassidy, A.J.; Suarez-Cuartin, G.; Sibila, O.; Furrie, E.; Fong, C.J.; Ibrahim, W.; Brady, G.; et al. Neutrophil extracellular traps are associated with disease severity and microbiota diversity in patients with chronic obstructive pulmonary disease. J. Allergy Clin. Immunol. 2017, 141, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Machahua, C.; Guler, S.A.; Horn, M.P.; Planas-Cerezales, L.; Montes-Worboys, A.; Geiser, T.K.; Molina-Molina, M.; Funke-Chambour, M. Serum calprotectin as new biomarker for disease severity in idiopathic pulmonary fibrosis: A cross-sectional study in two independent cohorts. BMJ Open Respir. Res. 2021, 8, e000827. [Google Scholar] [CrossRef] [PubMed]
- Araki, K.; Kinoshita, R.; Tomonobu, N.; Gohara, Y.; Tomida, S.; Takahashi, Y.; Senoo, S.; Taniguchi, A.; Itano, J.; Yamamoto, K.-I.; et al. The heterodimer S100A8/A9 is a potent therapeutic target for idiopathic pulmonary fibrosis. J. Mol. Med. 2020, 99, 131–145. [Google Scholar] [CrossRef] [PubMed]
- Butler, M.W.; Keane, M.P. The role of immunity and inflammation in IPF pathogenesis. In Idiopathic Pulmonary Fibrosis: A Comprehensive Clinical Guide; Springer Nature: Cham, Switzerland, 2019; pp. 97–131. [Google Scholar]
- The Idiopathic Pulmonary Fibrosis Clinical Research Network; Raghu, G.; Anstrom, K.J.; King, T.E., Jr.; Lasky, J.A.; Martinez, F.J. Prednisone, Azathioprine, and N-Acetylcysteine for Pulmonary Fibrosis. N. Engl. J. Med. 2012, 366, 1968–1977. [Google Scholar] [CrossRef] [PubMed]
- Wells, A.U.; Kelleher, W.P. Idiopathic pulmonary fibrosis pathogenesis and novel approaches to immunomodulation: We must not be tyrannized by the PANTHER data. Am. J. Respir. Crit. Care Med. 2013, 187, 677–679. [Google Scholar] [CrossRef]
- Fagerhol, M.K.; Nielsen, H.G.; Vetlesen, A.; Sandvik, K.; Lyberg, T. Increase in plasma calprotectin during long-distance running. Scand. J. Clin. Lab. Investig. 2005, 65, 211–220. [Google Scholar] [CrossRef]
- Summers, C.; Rankin, S.M.; Condliffe, A.M.; Singh, N.; Peters, A.M.; Chilvers, E.R. Neutrophil kinetics in health and disease. Trends Immunol. 2010, 31, 318–324. [Google Scholar] [CrossRef]
- Sand, J.M.; Martinez, G.; Midjord, A.-K.; Karsdal, M.A.; Leeming, D.J.; Lange, P. Characterization of serological neo-epitope biomarkers reflecting collagen remodeling in clinically stable chronic obstructive pulmonary disease. Clin. Biochem. 2016, 49, 1144–1151. [Google Scholar] [CrossRef]
- Ritchie, A.I.; Wedzicha, J.A. Definition, Causes, Pathogenesis, and Consequences of Chronic Obstructive Pulmonary Disease Exacerbations. Clin. Chest Med. 2020, 41, 421–438. [Google Scholar] [CrossRef]
- Sun, Y.; Milne, S.; Jaw, J.E.; Yang, C.X.; Xu, F.; Li, X.; Obeidat, M.; Sin, D.D. BMI is associated with FEV1 decline in chronic obstructive pulmonary disease: A meta-analysis of clinical trials. Respir. Res. 2019, 20, 236. [Google Scholar] [CrossRef] [PubMed]
- Zinellu, A.; Carru, C.; Pirina, P.; Fois, A.G.; Mangoni, A.A. A Systematic Review of the Prognostic Significance of the Body Mass Index in Idiopathic Pulmonary Fibrosis. J. Clin. Med. 2023, 12, 498. [Google Scholar] [CrossRef] [PubMed]
- Quach, A.; Glowik, S.; Putty, T.; Ferrante, A. Delayed Blood Processing Leads to Rapid Deterioration in the Measurement of the Neutrophil Respiratory Burst by the Dihydrorhodamine-123 Reduction Assay. Cytom. Part B Clin. Cytom. 2019, 96, 389–396. [Google Scholar] [CrossRef]
- Lorenzo, P.; Aspberg, A.; Saxne, T.; Önnerfjord, P. Quantification of cartilage oligomeric matrix protein (COMP) and a COMP neoepitope in synovial fluid of patients with different joint disorders by novel automated assays. Osteoarthr. Cartil. 2017, 25, 1436–1442. [Google Scholar] [CrossRef]
- Jenkins, R.G.; Simpson, J.K.; Saini, G.; Bentley, J.H.; Russell, A.M.; Braybrooke, R.; Molyneaux, P.L.; McKeever, T.M.; Wells, A.U.; Flynn, A.; et al. Longitudinal change in collagen degradation biomarkers in idiopathic pulmonary fibrosis: An analysis from the prospective, multicentre PROFILE study. Lancet Respir. Med. 2015, 3, 462–472. [Google Scholar] [CrossRef]
- Rønnow, S.R.; Langholm, L.L.; Sand, J.M.B.; Thorlacius-Ussing, J.; Leeming, D.J.; Manon-Jensen, T.; Tal-Singer, R.; Miller, B.E.; Karsdal, M.A.; Vestbo, J. Specific elastin degradation products are associated with poor outcome in the ECLIPSE COPD cohort. Sci. Rep. 2019, 9, 4064. [Google Scholar] [CrossRef]
- Organ, L.A.; Duggan, A.-M.R.; Oballa, E.; Taggart, S.C.; Simpson, J.K.; Kang’ombe, A.R.; Braybrooke, R.; Molyneaux, P.L.; North, B.; Karkera, Y.; et al. Biomarkers of collagen synthesis predict progression in the PROFILE idiopathic pulmonary fibrosis cohort. Respir. Res. 2019, 20, 148. [Google Scholar] [CrossRef] [PubMed]
- Karsdal, M.A.; Genovese, F.; Rasmussen, D.G.K.; Bay-Jensen, A.C.; Mortensen, J.H.; Nielsen, S.H.; Willumsen, N.; Jensen, C.; Manon-Jensen, T.; Jennings, L.; et al. Considerations for understanding protein measurements: Identification of formation, degradation and more pathological relevant epitopes. Clin. Biochem. 2021, 97, 11–24. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).