
Managing Small Airway Disease in Patients with Severe Asthma: Transitioning from the “Silent Zone” to Achieving “Quiet Asthma”

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
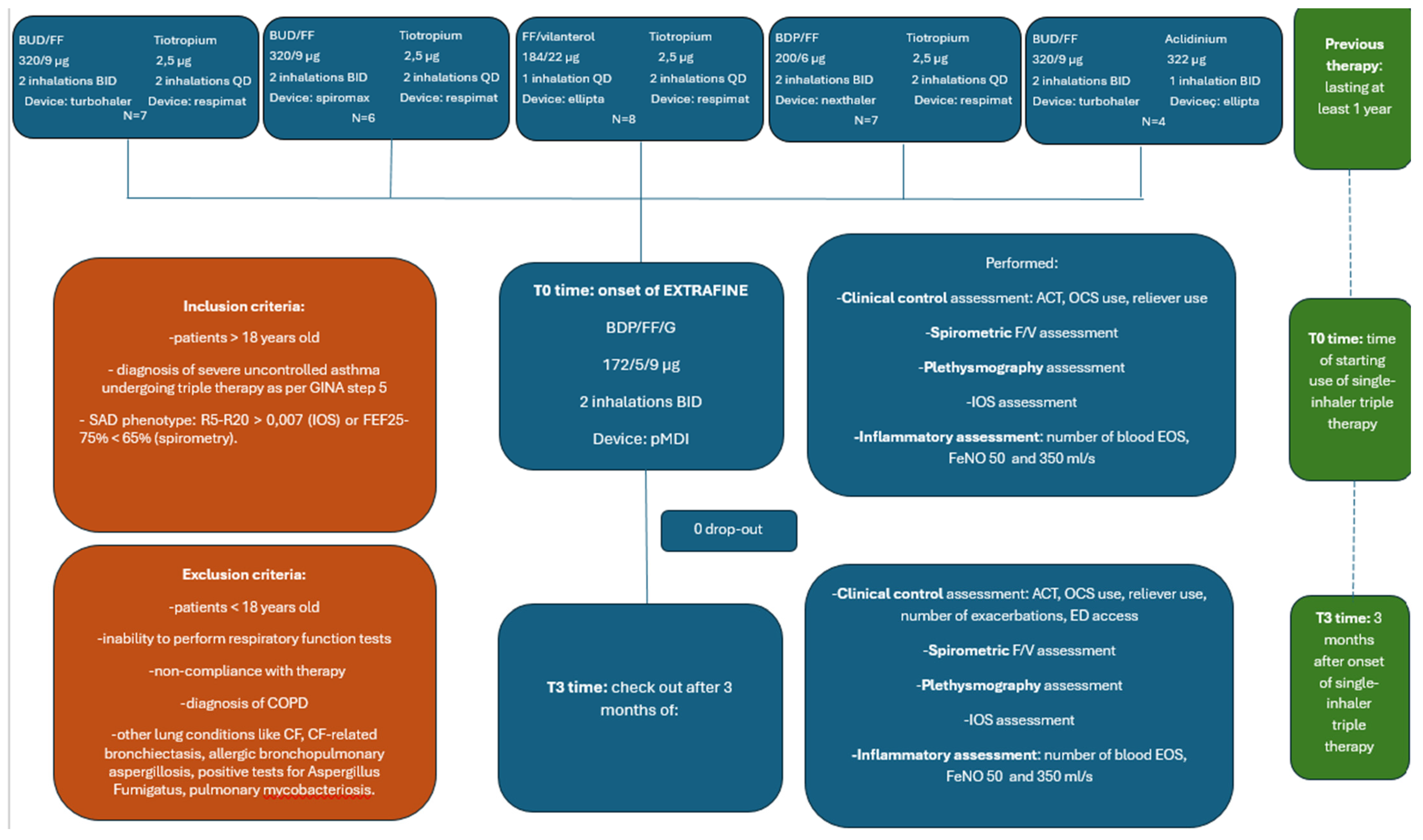
2.1. Study Design
2.2. Patients
2.3. Questionnaires
2.4. Lung Function
2.5. Impulse Oscillometry System (IOS)
2.6. Measurement of Exhaled Nitric Oxide (FeNO) 50 and 350 mL/s
2.7. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nunes, C.; Pereira, A.M.; Morais-Almeida, M. Asthma costs and social impact. Asthma Res. Pract. 2017, 3, 1. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Asthma 2023. Available online: www.ginasthma.org (accessed on 22 October 2023).
- Kim, L.H.Y.; Saleh, C.; Whalen-Browne, A.; O’Byrne, P.M.; Chu, D.K. Triple vs dual inhaler therapy and asthma outcomes in moderate to severe asthma: A systematic review and meta-analysis. JAMA 2021, 325, 2466–2479. [Google Scholar] [CrossRef] [PubMed]
- Buels, K.S.; Fryer, A.D. Muscarinic receptor antagonists: Effects on pulmonary function. Handb. Exp. Pharmacol. 2012, 208, 317–341. [Google Scholar] [CrossRef]
- Canonica, G.W.; Colombo, G.L.; Bruno, G.M.; Di Matteo, S.; Martinotti, C.; Blasi, F.; Bucca, C.; Crimi, N.; Paggiaro, P.; Pelaia, G.; et al. Shadow cost of oral corticosteroids-related adverse events: A pharmacoeconomic evaluation applied to real-life data from the Severe Asthma Network in Italy (SANI) registry. World Allergy Organ. J. 2019, 12, 100007. [Google Scholar] [CrossRef] [PubMed]
- Anderson, W.C.I.I.I.; Szefler, S.J. Cost-effectiveness and comparative effectiveness of biologic therapy for asthma: To biologic or not to biologic? Ann. Allergy Asthma Immunol. 2019, 122, 367–372. [Google Scholar] [CrossRef] [PubMed]
- Virchow, J.C.; Kuna, P.; Paggiaro, P.; Papi, A.; Singh, D.; Corre, S.; Zuccaro, F.; Vele, A.; Kots, M.; Georges, G.; et al. Single inhaler extra-fine triple therapy in uncontrolled asthma (TRIMARAN and TRIGGER): Two double-blind, parallel-group, randomised, controlled phase 3 trials. Lancet 2019, 394, 1737–1749. [Google Scholar] [CrossRef] [PubMed]
- Cazzola, M.; Calzetta, L.; Rogliani, P.; Puxeddu, E.; Facciolo, F.; Matera, M.G. Interaction between corticosteroids and muscarinic antagonists in human airways. Pulm. Pharmacol. Ther. 2016, 36, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kraft, M.; Richardson, M.; Hallmark, B.; Billheimer, D.; Van den Berge, M.; Fabbri, L.M.; Van der Molen, T.; Nicolini, G.; Papi, A.; Rabe, K.F.; et al. The role of small airway dysfunction in asthma control and exacerbations: A longitudinal, observational analysis using data from the ATLANTIS study. Lancet Respir. Med. 2022, 10, 661–668. [Google Scholar] [CrossRef] [PubMed]
- Cottini, M.; Licini, A.; Lombardi, C.; Bagnasco, D.; Comberiati, P.; Berti, A. Small airway dysfunction and poor asthma control: A dangerous liaison. Clin. Mol. Allergy 2021, 19, 7. [Google Scholar] [CrossRef]
- Cottini, M.; Bondi, B.; Bagnasco, D.; Braido, F.; Passalacqua, G.; Licini, A.; Lombardi, C.; Berti, A.; Comberiati, P.; Landi, M.; et al. Impulse oscillometry defined small airway dysfunction in asthmatic patients with normal spirometry: Prevalence, clinical associations, and impact on asthma control. Respir. Med. 2023, 218, 107391. [Google Scholar] [CrossRef]
- Thomas, M.; Kay, S.; Pike, J.; Williams, A.; Rosenzweig, J.R.; Hillyer, E.V.; Price, D. The asthma control test™ (ACT) as a predictor of GINA guideline-defined asthma control: Analysis of a multinational cross-sectional survey. Prim. Care Respir. J. 2009, 18, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Plaza, V.; Fernández-Rodríguez, C.; Melero, C.; Cosío, B.G.; Entrenas, L.M.; de Llano, L.P.; Gutiérrez-Pereyra, F.; Tarragona, E.; Palomino, R.; López-Viña, A.; et al. Validation of the “test of the adherence to inhalers” (TAI) for asthma and COPD patients. J. Aerosol Med. Pulm. Drug Deliv. 2016, 29, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed]
- Stanojevic, S.; Kaminsky, D.A.; Miller, M.R.; Thompson, B.; Aliverti, A.; Barjaktarevic, I.; Cooper, B.G.; Culver, B.; Derom, E.; Hall, G.L.; et al. ERS/ATS technical standard on interpretive strategies for routine lung function tests. Eur. Respir. J. 2022, 60, 2101499. [Google Scholar] [CrossRef] [PubMed]
- Oostveen, E.; MacLeod, D.; Lorino, H.; Farré, R.; Hantos, Z.; Desager, K.; Marchal, F.; ERS Task Force on Respiratory Impedance Measurements. The forced oscillation technique in clinical practice: Methodology, recommendations and future developments. Eur. Respir. J. 2003, 22, 1026–1041. [Google Scholar] [CrossRef] [PubMed]
- Oppenheimer, B.W.; Goldring, R.M.; Herberg, M.E.; Hofer, I.S.; Reyfman, P.A.; Liautaud, S.; Rom, W.N.; Reibman, J.; Berger, K.I. Distal airway function in symptomatic subjects with normal spirometry following World Trade Center dust exposure. Chest 2007, 132, 1275–1282. [Google Scholar] [CrossRef] [PubMed]
- Horváth, I.; Barnes, P.J.; Loukides, S.; Sterk, P.J.; Högman, M.; Olin, A.C.; Amann, A.; Antus, B.; Baraldi, E.; Bikov, A.; et al. A European Respiratory Society technical standard: Exhaled biomarkers in lung disease. Eur. Respir. J. 2017, 49, 1600965. [Google Scholar] [CrossRef] [PubMed]
- Dweik, R.A.; Boggs, P.B.; Erzurum, S.C.; Irvin, C.G.; Leigh, M.W.; Lundberg, J.O.; Olin, A.-C.; Plummer, A.L.; Taylor, D.R.; on behalf of the American Thoracic Society Committee on Interpretation of Exhaled Nitric Oxide Levels (FENO) for Clinical Applications. An official ATS clinical practice guideline: Interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Am. J. Respir. Crit. Care Med. 2011, 184, 602–615. [Google Scholar] [CrossRef] [PubMed]
- Carr, T.F.; Altisheh, R.; Zitt, M. Small airways disease and severe asthma. World Allergy Organ. J. 2017, 10, 20. [Google Scholar] [CrossRef]
- Lipworth, B.; Manoharan, A.; Anderson, W. Unlocking the quiet zone: The small airway asthma phenotype. Lancet Respir. Med. 2014, 2, 497–506. [Google Scholar] [CrossRef]
- Usmani, O.S.; Singh, D.; Spinola, M.; Bizzi, A.; Barnes, P.J. The prevalence of small airways disease in adult asthma: A systematic literature review. Respir. Med. 2016, 116, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Kerstjens, H.A.; Engel, M.; Dahl, R.; Paggiaro, P.; Beck, E.; Vandewalker, M.; Sigmund, R.; Seibold, W.; Moroni-Zentgraf, P.; Bateman, E.D. Tiotropium in asthma poorly controlled with standard combination therapy. N. Engl. J. Med. 2012, 367, 1198–1207. [Google Scholar] [CrossRef] [PubMed]
- Hoshino, M.; Ohtawa, J.; Akitsu, K. Effects of the addition of tiotropium on airway dimensions in symptomatic asthma. Allergy Asthma Proc. 2016, 37, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Muiser, S.; Gosens, R.; van den Berge, M.; Kerstjens, H.A.M. Understanding the role of long-acting muscarinic antagonists in asthma treatment. Ann. Allergy Asthma Immunol. 2022, 128, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Rogliani, P.; Matera, M.G.; Facciolo, F.; Page, C.; Cazzola, M.; Calzetta, L. Beclomethasone dipropionate, formoterol fumarate and glycopyrronium bromide: Synergy of triple combination therapy on human airway smooth muscle ex vivo. Br. J. Pharmacol. 2020, 177, 1150–1163. [Google Scholar] [CrossRef] [PubMed]
- Mead, J. The lung’s “quiet zone”. N. Engl. J. Med. 1970, 282, 1318–1319. [Google Scholar] [CrossRef]
- Postma, D.S.; Brightling, C.; Baldi, S.; Van den Berge, M.; Fabbri, L.M.; Gagnatelli, A.; Papi, A.; Van der Molen, T.; Rabe, K.F.; Siddiqui, S.; et al. Exploring the relevance and extent of small airways dysfunction in asthma (ATLANTIS): Baseline data from a prospective cohort study. Lancet Respir. Med. 2019, 7, 402–416. [Google Scholar] [CrossRef]
- Knox-Brown, B.; Mulhern, O.; Feary, J.; Amaral, A.F.S. Spirometry parameters used to define small airways obstruction in population-based studies: Systematic review. Respir. Res. 2022, 23, 67. [Google Scholar] [CrossRef]
- Kaminsky, D.A.; Simpson, S.J.; Berger, K.I.; Calverley, P.; de Melo, P.L.; Dandurand, R.; Dellacà, R.L.; Farah, C.S.; Farré, R.; Hall, G.L.; et al. Clinical significance and applications of oscillometry. Eur. Respir. Rev. 2022, 31, 210208. [Google Scholar] [CrossRef]
- Menzies-Gow, A.; Bafadhel, M.; Busse, W.W.; Casale, T.B.; Kocks, J.W.H.; Pavord, I.D.; Szefler, S.J.; Woodruff, P.G.; de Giorgio-Miller, A.; Trudo, F.; et al. An expert consensus framework for asthma remission as a treatment goal. J. Allergy. Clin. Immunol. 2020, 145, 757–765. [Google Scholar] [CrossRef]
- Lommatzsch, M.; Buhl, R.; Canonica, G.W.; Ribas, C.D.; Nagase, H.; Brusselle, G.G.; Jackson, D.J.; Pavord, I.D.; Korn, S.; Milger, K.; et al. Pioneering a paradigm shift in asthma management: Remission as a treatment goal. Lancet Respir. Med. 2024, 12, 96–99. [Google Scholar] [CrossRef] [PubMed]
- Canonica, G.W.; Blasi, F.; Carpagnano, G.E.; Guida, G.; Heffler, E.; Paggiaro, P.; Allegrini, C.; Antonelli, A.; Aruanno, A.; Bacci, E.; et al. Severe Asthma Network Italy Definition of Clinical Remission in Severe Asthma: A Delphi Consensus. J. Allergy Clin. Immunol. Pract. 2023, 11, 3629–3637. [Google Scholar] [CrossRef] [PubMed]
- Upham, J.W.; Le Lievre, C.; Jackson, D.J.; Masoli, M.; Wechsler, M.E.; Price, D.B.; Panel, D. Defining a Severe Asthma Super-Responder: Findings from a Delphi Process. J. Allergy Clin. Immunol. Pract. 2021, 9, 3997–4004. [Google Scholar] [CrossRef] [PubMed]
- Portacci, A.; Dragonieri, S.; Carpagnano, G.E. Super-Responders to Biologic Treatment in Type 2-High Severe Asthma: Passing Fad or a Meaningful Phenotype? J. Allergy Clin. Immunol. Pract. 2023, 11, 1417–1420. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Parameters | |
| Age (yrs) m ± sd | 58.59 ± 15.03 |
| Sex Female n (%) | 17 (53.1) |
| Life Style | |
| BMI (kg/m2) m ± sd | 26.65 ± 4.88 |
| Smoke n (%) No Ex | 19 (59.4) 13 (40.6) |
| Pack/year m ± sd | 9.32 ± 16.02 |
| Characteristics of asthma | |
| Atopic yes n (%) | 26 (81.3) |
| Duration of disease years m ± sd | 21.28 ± 14.23 |
| Age of diagnosis (years) m ± sd | 26.75 ± 16.78 |
| Exacerbations last year (n) m ± sd | 2.78 ± 2.82 |
| First Aid visits last year (n) m ± sd | 0.25 ± 0.50 |
| Average reliever usage last month (n) m ± sd | 1.03 ± 1.59 |
| OCS cycles last year (n) m ± sd | 1.68 ± 1.90 |
| OCS dose last year (mg) m ± sd | 17.65 ± 12.88 |
| Baseline Therapy | |
| Course of antibiotics last year n (%) 0 1 2 | 17 (53.1) 12 (37.5) 3 (9.4) |
| LTRA yes n (%) | 4 (12.5) |
| Comorbidities | |
| EGPA yes n (%) | 3 (9.4) |
| Eosinophilic Pneumonia yes n (%) | 0 (0) |
| Hypereosinophilic syndrome yes n (%) | 0 (0) |
| Rhinosinusitis yes n (%) | 4 (12.5) |
| Nasal Polyposis yes n (%) | 7 (21.9) |
| Urticaria yes n (%) | 2 (6.3) |
| Vocal Cord Dysfunction yes n (%) | 3 (9.4) |
| COPD yes n (%) | 0 (0) |
| Bronchiectasis yes n (%) | 3 (9.4) |
| GERD yes n (%) | 9 (28.1) |
| OSAS yes n (%) | 6 (18.8) |
| Depressive Anxious Syndrome yes n (%) | 3 (9.4) |
| Parameters | T0 Time | T3 Time | p Value |
|---|---|---|---|
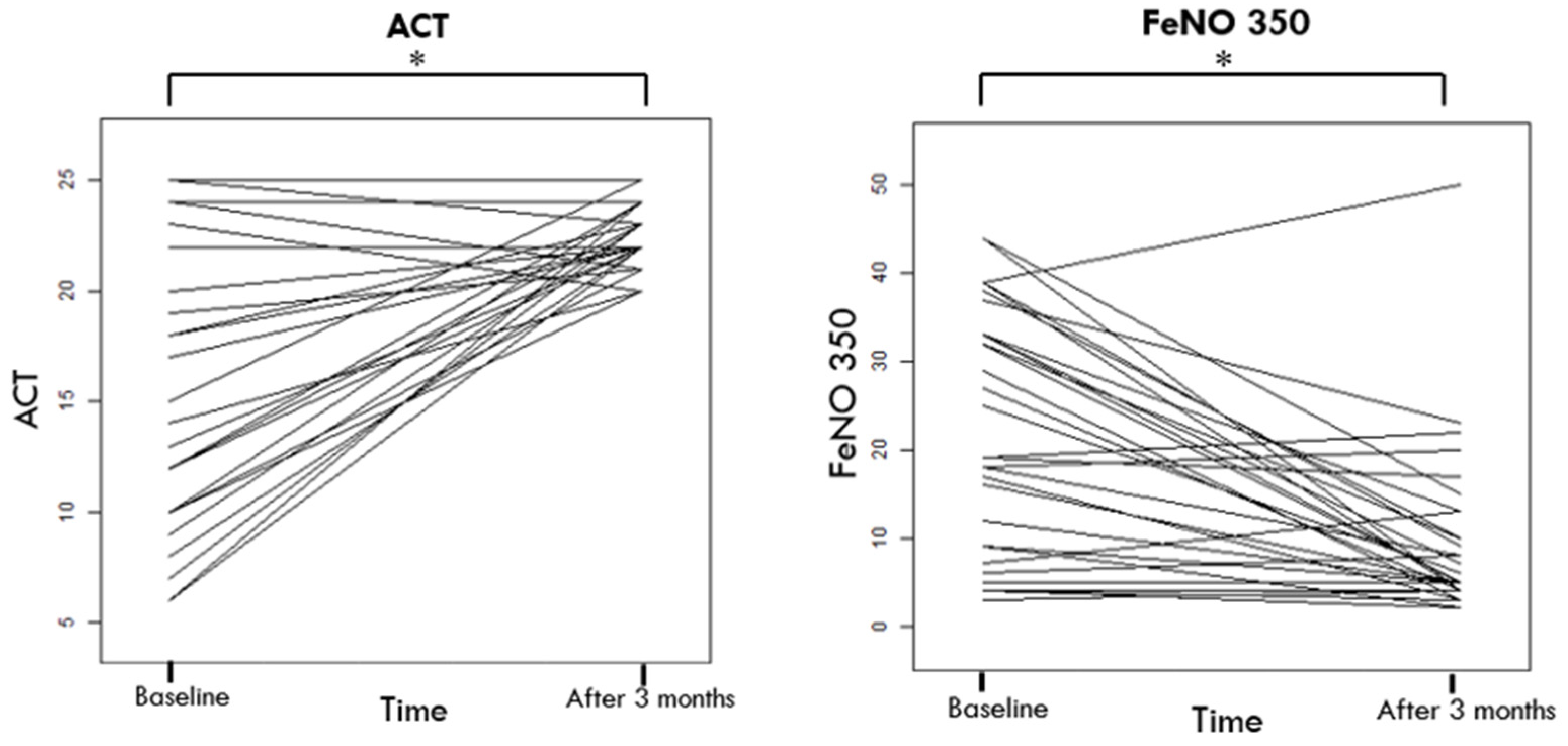
| ACT m ± sd | 15.75 ± 5.92 | 22.53 ± 1.45 | <0.001 |
| Average reliver usage last month (n) m ± sd | 1.03 ± 1.59 | 0.25 ± 0.76 | 0.008 |
| %FEV1 m ± sd | 73.20 ± 22.86 | 73.90 ± 24.06 | 0.843 |
| FEV1 (l) m ± sd | 2.27 ± 0.99 | 2.30 ±0.99 | 0.736 |
| %FVC m ± sd | 84.85 ± 19.57 | 86.37 ± 15.65 | 0.623 |
| FVC (l) m ± sd | 3.21 ± 0.79 | 3.41 ± 1.14 | 0.199 |
| %FEV1/FVC m ± sd | 67.16 ± 12.75 | 67.88 ± 12.49 | 0.698 |
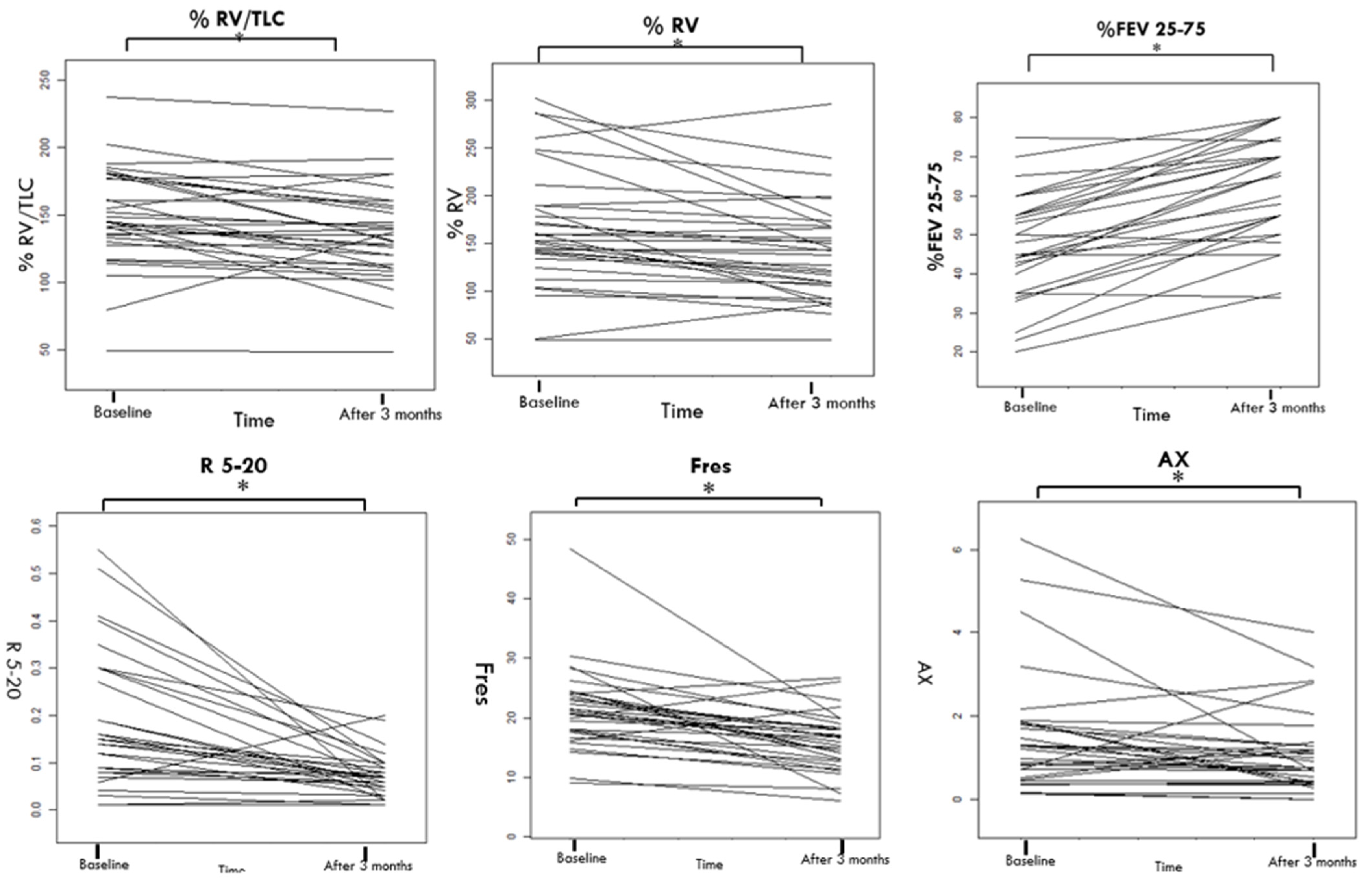
| %FEV25–75 m ± sd | 48.53 ± 13.31 | 63.62 ± 13.46 | <0.001 |
| %Rtot m ± sd | 145.80 ± 86.72 | 151.35 ± 67.05 | 0.739 |
| %TLC m ± sd | 106.47 ± 22.38 | 101.78 ± 22.01 | 0.101 |
| TLC (l) m ± sd | 6.24 ± 1.16 | 5.84 ± 1.19 | 0.058 |
| %RV m ± sd | 165.70 ± 63.51 | 141.65 ± 52.11 | 0.001 |
| RV (l) m ± sd | 3.24 ± 1.29 | 2.86 ± 0.94 | 0.008 |
| %RV/TLC m ± sd | 147.58 ± 37.06 | 135.09 ± 34.38 | 0.002 |
| RV/TLC m ± sd | 51.61 ± 14.37 | 46.24 ± 14.94 | 0.003 |
| R5–20 kPa·L−1·s−1 IQ (25; 75) | 0.14 (0.08; 0.29) | 0.07 (0.04; 0.09) | <0.001 |
| Fres Hz IQ (25; 75) | 20.90 (17.69; 24.14) | 16.33 (12.77; 18.38) | <0.001 |
| AX kPa/L IQ (25; 75) | 1.25 (0.48; 1.18) | 0.77 (0.43; 1.30) | 0.009 |
| X5 kPa·L−1·s−1 IQ (25; 75) | −1.20 (−1.47; −0.9) | −0.55 (−0.80; −0.50) | <0.001 |
| Eosinophils (n/μL) m ± sd | 262.59 ± 276.80 | 250.21 ± 259.29 | 0.160 |
| FeNO 50 (ppb) m ± sd | 12.28 ± 11.76 | 13.96 ± 16.84 | 0.639 |
| FeNO350 (ppb) m ± sd | 21.81 ± 13.83 | 9.31 ± 9.44 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carpagnano, G.E.; Portacci, A.; Dragonieri, S.; Montagnolo, F.; Iorillo, I.; Lulaj, E.; Maselli, L.; Buonamico, E.; Quaranta, V.N. Managing Small Airway Disease in Patients with Severe Asthma: Transitioning from the “Silent Zone” to Achieving “Quiet Asthma”. J. Clin. Med. 2024, 13, 2320. https://doi.org/10.3390/jcm13082320
Carpagnano GE, Portacci A, Dragonieri S, Montagnolo F, Iorillo I, Lulaj E, Maselli L, Buonamico E, Quaranta VN. Managing Small Airway Disease in Patients with Severe Asthma: Transitioning from the “Silent Zone” to Achieving “Quiet Asthma”. Journal of Clinical Medicine. 2024; 13(8):2320. https://doi.org/10.3390/jcm13082320
Chicago/Turabian StyleCarpagnano, Giovanna Elisiana, Andrea Portacci, Silvano Dragonieri, Francesca Montagnolo, Ilaria Iorillo, Ernesto Lulaj, Leonardo Maselli, Enrico Buonamico, and Vitaliano Nicola Quaranta. 2024. "Managing Small Airway Disease in Patients with Severe Asthma: Transitioning from the “Silent Zone” to Achieving “Quiet Asthma”" Journal of Clinical Medicine 13, no. 8: 2320. https://doi.org/10.3390/jcm13082320
APA StyleCarpagnano, G. E., Portacci, A., Dragonieri, S., Montagnolo, F., Iorillo, I., Lulaj, E., Maselli, L., Buonamico, E., & Quaranta, V. N. (2024). Managing Small Airway Disease in Patients with Severe Asthma: Transitioning from the “Silent Zone” to Achieving “Quiet Asthma”. Journal of Clinical Medicine, 13(8), 2320. https://doi.org/10.3390/jcm13082320