
The Burden of Rheumatoid Arthritis: Findings from the 2019 Global Burden of Diseases Study and Forecasts for 2030 by Bayesian Age-Period-Cohort Analysis


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Overview and Data Sources
2.2. Global, Regional, and Country-Specific Burden of RA
2.3. Sociodemographic Index (SDI) and Risk Factors
2.4. Statistical Analysis
3. Results
3.1. Global Level
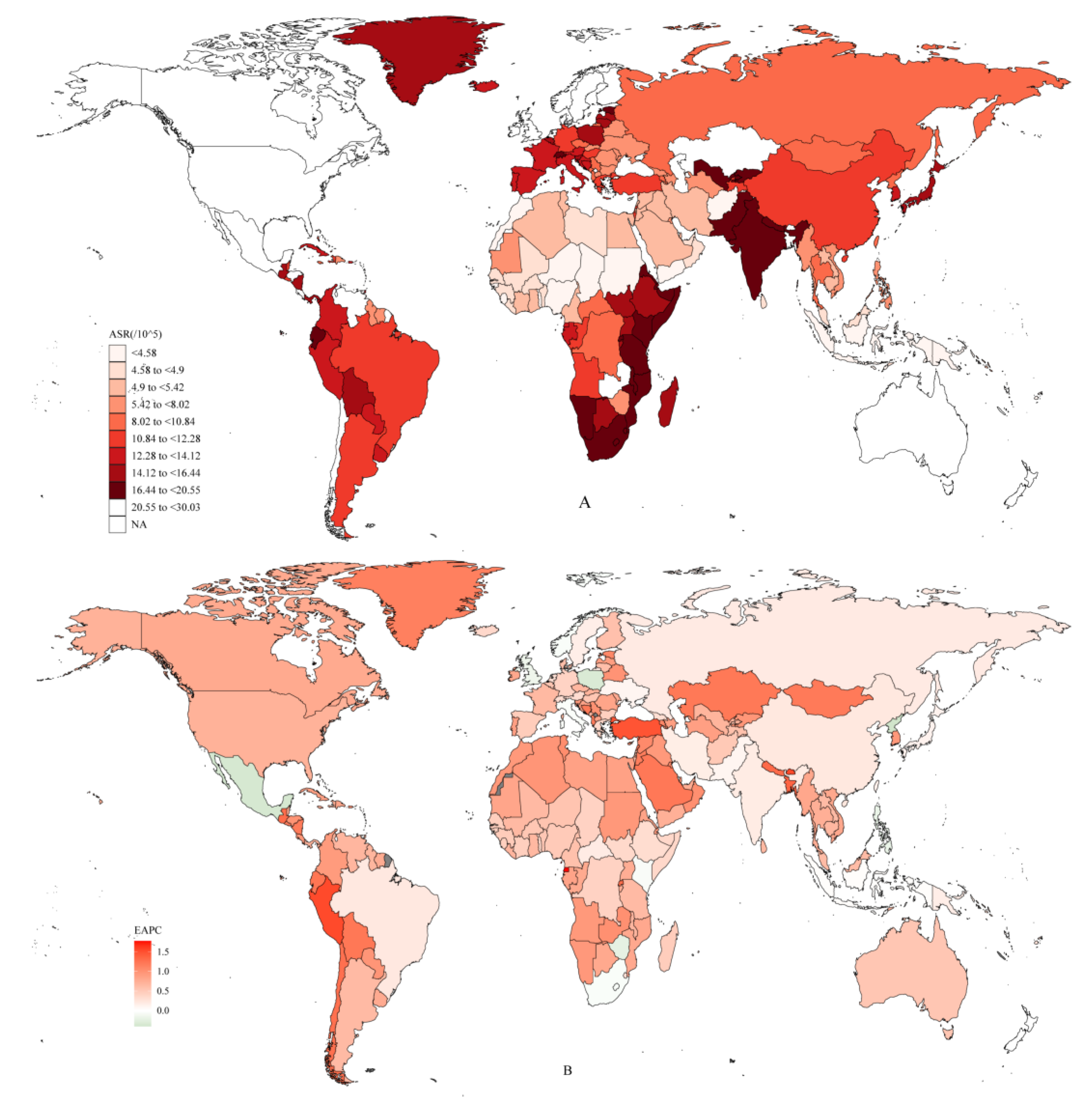
3.2. National Level
3.3. The Association between the ASR and SDI, the EAPC and ASR, and HDI
3.4. Risk Factors
3.5. ASR Forecasts for 2030 by Bayesian Age-Period-Cohort Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Radu, A.-F.; Bungau, S.G. Management of Rheumatoid Arthritis: An Overview. Cells 2021, 10, 2857. [Google Scholar] [CrossRef] [PubMed]
- Hyndman, I.J. Rheumatoid Arthritis: Past, Present and Future Approaches to Treating the Disease. Int. J. Rheum. Dis. 2017, 20, 417–419. [Google Scholar] [CrossRef] [PubMed]
- Dedmon, L.E. The Genetics of Rheumatoid Arthritis. Rheumatology 2020, 59, 2661–2670. [Google Scholar] [CrossRef] [PubMed]
- Karami, J.; Aslani, S.; Jamshidi, A.; Garshasbi, M.; Mahmoudi, M. Genetic Implications in the Pathogenesis of Rheumatoid Arthritis; an Updated Review. Gene 2019, 702, 8–16. [Google Scholar] [CrossRef] [PubMed]
- McInnes, I.B.; Schett, G. The Pathogenesis of Rheumatoid Arthritis. N. Engl. J. Med. 2011, 365, 2205–2219. [Google Scholar] [CrossRef]
- Papakonstantinou, D. Work Disability and Rheumatoid Arthritis: Predictive Factors. Work 2021, 69, 1293–1304. [Google Scholar] [CrossRef]
- Hsieh, P.-H.; Wu, O.; Geue, C.; McIntosh, E.; McInnes, I.B.; Siebert, S. Economic Burden of Rheumatoid Arthritis: A Systematic Review of Literature in Biologic Era. Ann. Rheum. Dis. 2020, 79, 771–777. [Google Scholar] [CrossRef]
- Cross, M.; Smith, E.; Hoy, D.; Nolte, S.; Ackerman, I.; Fransen, M.; Bridgett, L.; Williams, S.; Guillemin, F.; Hill, C.L.; et al. The Global Burden of Hip and Knee Osteoarthritis: Estimates from the Global Burden of Disease 2010 Study. Ann. Rheum. Dis. 2014, 73, 1323–1330. [Google Scholar] [CrossRef]
- Sebbag, E.; Felten, R.; Sagez, F.; Sibilia, J.; Devilliers, H.; Arnaud, L. The World-Wide Burden of Musculoskeletal Diseases: A Systematic Analysis of the World Health Organization Burden of Diseases Database. Ann. Rheum. Dis. 2019, 78, 844–848. [Google Scholar] [CrossRef]
- Safiri, S.; Kolahi, A.A.; Hoy, D.; Smith, E.; Bettampadi, D.; Mansournia, M.A.; Almasi-Hashiani, A.; Ashrafi-Asgarabad, A.; Moradi-Lakeh, M.; Qorbani, M.; et al. Global, Regional and National Burden of Rheumatoid Arthritis 1990-2017: A Systematic Analysis of the Global Burden of Disease Study 2017. Ann. Rheum. Dis. 2019, 78, 1463–1471. [Google Scholar] [CrossRef]
- Cross, M.; Smith, E.; Hoy, D.; Carmona, L.; Wolfe, F.; Vos, T.; Williams, B.; Gabriel, S.; Lassere, M.; Johns, N.; et al. The Global Burden of Rheumatoid Arthritis: Estimates from the Global Burden of Disease 2010 Study. Ann. Rheum. Dis. 2014, 73, 1316–1322. [Google Scholar] [CrossRef]
- GBD 2019 Diseases and Injuries Collaborators Global Burden of 369 Diseases and Injuries in 204 Countries and Territories, 1990-2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [CrossRef]
- GBD 2019 Risk Factors Collaborators Global Burden of 87 Risk Factors in 204 Countries and Territories, 1990-2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [CrossRef]
- Kamal, A.; Ali, A.A.; Irfan, S. Socio Demographic Determinants of BMI of Pakistani Women: An Evidence from PDHS (2017-18) Using Quantile Regression Analysis. J. Pak. Med. Assoc. 2021, 71, 1069–1075. [Google Scholar] [CrossRef]
- Kamangar, F.; Nasrollahzadeh, D.; Safiri, S.; Sepanlou, S.G.; Fitzmaurice, C.; Ikuta, K.S.; Bisignano, C.; Islami, F.; Roshandel, G.; Lim, S.S.; et al. The Global, Regional, and National Burden of Oesophageal Cancer and Its Attributable Risk Factors in 195 Countries and Territories, 1990-2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 582–597. [Google Scholar] [CrossRef]
- Liu, Z.; Jiang, Y.; Yuan, H.; Fang, Q.; Cai, N.; Suo, C.; Jin, L.; Zhang, T.; Chen, X. The Trends in Incidence of Primary Liver Cancer Caused by Specific Etiologies: Results from the Global Burden of Disease Study 2016 and Implications for Liver Cancer Prevention. J. Hepatol. 2019, 70, 674–683. [Google Scholar] [CrossRef]
- Li, S.; Chen, H.; Man, J.; Zhang, T.; Yin, X.; He, Q.; Yang, X.; Lu, M. Changing Trends in the Disease Burden of Esophageal Cancer in China from 1990 to 2017 and Its Predicted Level in 25 Years. Cancer Med. 2021, 10, 1889–1899. [Google Scholar] [CrossRef]
- Wu, X.; Du, J.; Li, L.; Cao, W.; Sun, S. Bayesian Age-Period-Cohort Prediction of Mortality of Type 2 Diabetic Kidney Disease in China: A Modeling Study. Front. Endocrinol. 2021, 12, 767263. [Google Scholar] [CrossRef]
- Chen, W.-Q.; Zheng, R.-S.; Zeng, H.-M. Bayesian Age-Period-Cohort Prediction of Lung Cancer Incidence in China. Thorac. Cancer 2011, 2, 149–155. [Google Scholar] [CrossRef]
- England, B.R.; Thiele, G.M.; Anderson, D.R.; Mikuls, T.R. Increased Cardiovascular Risk in Rheumatoid Arthritis: Mechanisms and Implications. BMJ 2018, 361, k1036. [Google Scholar] [CrossRef]
- van der Woude, D.; van der Helm-van Mil, A.H.M. Update on the Epidemiology, Risk Factors, and Disease Outcomes of Rheumatoid Arthritis. Best Pract. Res. Clin. Rheumatol. 2018, 32, 174–187. [Google Scholar] [CrossRef] [PubMed]
- Blum, A.; Adawi, M. Rheumatoid Arthritis (RA) and Cardiovascular Disease. Autoimmun. Rev. 2019, 18, 679–690. [Google Scholar] [CrossRef] [PubMed]
- Gioia, C.; Lucchino, B.; Tarsitano, M.G.; Iannuccelli, C.; Di Franco, M. Dietary Habits and Nutrition in Rheumatoid Arthritis: Can Diet Influence Disease Development and Clinical Manifestations? Nutrients 2020, 12, 1456. [Google Scholar] [CrossRef] [PubMed]
- Sturgeon, J.A.; Finan, P.H.; Zautra, A.J. Affective Disturbance in Rheumatoid Arthritis: Psychological and Disease-Related Pathways. Nat. Rev. Rheumatol. 2016, 12, 532–542. [Google Scholar] [CrossRef]
- Cutolo, M.; Seriolo, B.; Villaggio, B.; Pizzorni, C.; Craviotto, C.; Sulli, A. Androgens and Estrogens Modulate the Immune and Inflammatory Responses in Rheumatoid Arthritis. Ann. N. Y. Acad. Sci. 2002, 966, 131–142. [Google Scholar] [CrossRef]
- Cush, J.J. Rheumatoid Arthritis: Early Diagnosis and Treatment. Rheum. Dis. Clin. North Am. 2022, 48, 537–547. [Google Scholar] [CrossRef]
- Cush, J.J. Rheumatoid Arthritis: Early Diagnosis and Treatment. Med. Clin. North Am. 2021, 105, 355–365. [Google Scholar] [CrossRef]
- Abbasi, M.; Mousavi, M.J.; Jamalzehi, S.; Alimohammadi, R.; Bezvan, M.H.; Mohammadi, H.; Aslani, S. Strategies toward Rheumatoid Arthritis Therapy; the Old and the New. J. Cell. Physiol. 2019, 234, 10018–10031. [Google Scholar] [CrossRef]
- Rahimizadeh, P.; Rezaieyazdi, Z.; Behzadi, F.; Hajizade, A.; Lim, S.I. Nanotechnology as a Promising Platform for Rheumatoid Arthritis Management: Diagnosis, Treatment, and Treatment Monitoring. Int. J. Pharm. 2021, 609, 121137. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cai, Y.; Zhang, J.; Liang, J.; Xiao, M.; Zhang, G.; Jing, Z.; Lv, L.; Nan, K.; Dang, X. The Burden of Rheumatoid Arthritis: Findings from the 2019 Global Burden of Diseases Study and Forecasts for 2030 by Bayesian Age-Period-Cohort Analysis. J. Clin. Med. 2023, 12, 1291. https://doi.org/10.3390/jcm12041291
Cai Y, Zhang J, Liang J, Xiao M, Zhang G, Jing Z, Lv L, Nan K, Dang X. The Burden of Rheumatoid Arthritis: Findings from the 2019 Global Burden of Diseases Study and Forecasts for 2030 by Bayesian Age-Period-Cohort Analysis. Journal of Clinical Medicine. 2023; 12(4):1291. https://doi.org/10.3390/jcm12041291
Chicago/Turabian StyleCai, Yuanqing, Jianan Zhang, Jialin Liang, Mofan Xiao, Guangyang Zhang, Zhaopu Jing, Leifeng Lv, Kai Nan, and Xiaoqian Dang. 2023. "The Burden of Rheumatoid Arthritis: Findings from the 2019 Global Burden of Diseases Study and Forecasts for 2030 by Bayesian Age-Period-Cohort Analysis" Journal of Clinical Medicine 12, no. 4: 1291. https://doi.org/10.3390/jcm12041291