Abstract
High-volume extracorporeal membrane oxygenation (ECMO) centers generally have better outcomes than (new) low-volume ECMO centers, most likely achieved by a suitable exposure to ECMO cases. To achieve a higher level of training, simulation-based training (SBT) offers an additional option for education and extended clinical skills. SBT could also help to improve the interdisciplinary team interactions. However, the level of ECMO simulators and/or simulations (ECMO sims) techniques may vary in purpose. We present a structured and objective classification of ECMO sims based on the broad experience of users and the developer for the available ECMO sims as low-, mid-, or high-fidelity. This classification is based on overall ECMO sim fidelity, established by taking the median of the definition-based fidelity, component fidelity, and customization fidelity as determined by expert opinion. According to this new classification, only low- and mid-fidelity ECMO sims are currently available. This comparison method may be used in the future for the description of new developments in ECMO sims, making it possible for ECMO sim designers, users, and researchers to compare accordingly, and ultimately improve ECMO patient outcomes.
1. Introduction
Extracorporeal membrane oxygenation (ECMO) support is used for critical pulmonary and/or cardiac hemodynamic dysfunction refractory to conventional therapies [1,2]. ECMO is a type of organ support that substitutes the lungs and/or heart. To achieve this, blood is drained from a cannula located in a large vein (often femoral or jugular veins) for the peripheral configuration. Blood is oxygenated and carbon dioxide is removed. Pressurized blood flow returns back to the patient through a return cannula located in a major vein (veno-venous (VV) configuration, providing respiratory support) or in an artery (veno-arterial (VA) configuration, providing cardiorespiratory support). Gas exchange is achieved through an artificial polymethyl pentene (fiber) membrane (located in a gas interchanger or oxygenator) and the blood flow is generated by a centrifugal pump (in neonates, a roller pump may be alternatively used), see Figure 1.
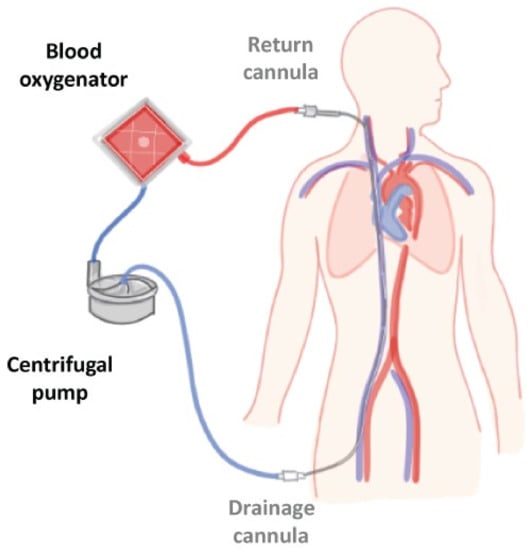
Figure 1.
Simplified representation of an ECMO system, with a veno-venous configuration draining blood from the femoral vein, oxygenation and carbon dioxide removal, and returning blood through the jugular vein back to the patient. Adjusted image from Martins Costa, et al. [3].
Through blood contact with artificial structures and depending on the patient’s condition, the coagulation system may be activated. Therefore, patients on ECMO support usually receive anticoagulation to prevent thrombotic events. Thrombotic and hemorrhagic events, as well as infections, are the most frequent complications [4]. These complications may lead to life-threatening conditions and should promptly be identified and urgently solved. Additionally, the cannulation process (generally carried out via the Seldinger technique) is associated with a relatively high risk of complications [5]. Because of the high and life-threatening complication risks, nursing care should be performed cautiously, making in-hospital and out-hospital transports challenging. All these factors make the clinical scenario very complex for the involved clinical staff. Despite the complexity of the ECMO system and clinical environment, the use of ECMO in recent years has been increasing, especially in the adult population. Most recently, good results have been evidenced with its use during the COVID-19 pandemic and, in some instances, in refractory cardiac arrest [6,7]. This expansion of indications has increased healthcare entities’ interest in training their teams in this technique.
Results after using ECMO are typically better in high-volume centers, with the general recommendation for concentrating cases in a few centers [8,9]. These better outcomes are mainly related to a superior level of training of the ECMO team, achieved by a suitable clinical demand. However, new and low-volume centers could also reach good results when the ECMO team receives adequate multidisciplinary and high-quality training [10,11].
A simulation is an education modality that significantly benefits training medical teams working in specialized and highly technical clinical scenarios [12]. Recently, it has gained popularity for educating individuals and teams to improve patient safety and optimize healthcare quality. The Extracorporeal Life Support Organization (ELSO), the referent ECMO international society, stresses the importance of using simulation-based training (SBT) in training the ECMO team (www.elso.org accessed on 10 October 2022). Aside from the importance of debriefing-based methodologies, optimized technical equipment is essential to enhance the learning process. Various simulators designed by different companies and institutions are now available for ECMO training and are currently being used by different entities. These devices have specific features which are conceivably essential to adapt in detail to the necessities of the different entities delivering ECMO training, each with particular objectives and teaching-targeted disciplines, such as intensive care, cardiology, and clinical perfusion.
Currently, only SBT programs have been reviewed and compared, but not ECMO sims themselves. Some developers, such as Alhomsi, et al. [13], tried to compare their work to different ECMO sims but lacked guidelines for comparison, making them subjective. Therefore, this study presents a structured and objective way of classifying available ECMO sims.
2. Materials and Methods
Following the PRISMA (preferred reporting items for systematic reviews and meta-analyses) scoping guidelines [14], this scoping review aims to identify characteristics and specific training media to include in ECMO simulations and simulators (ECMO sims). In addition, desk research was carried out to gather relevant literature for recent developments [13,15,16,17,18,19,20,21,22,23,24,25] and commercially available ECMO sims [26,27,28,29,30,31,32,33,34,35,36,37,38,39].
2.1. Desk Research
The in- and exclusion criteria for the literature collection were as follows:
- Research material is derived from (online) databases, including: PubMed, Web of Science Core Collection, and Google (Scholar);
- Research material is taken from its original source;
- The literature contains information regarding ECMO sims;
- The information applies to the comparison of ECMO sims;
- The literature has not been retracted;
- No case studies are used unless the importance of the study can be argued;
- No review studies are included in the literature to process specific device developments;
- The language of the literature material should be available in English.
A list of key concepts related to ECMO sims was created, and for each key concept synonyms, narrow terms, and broader terms were drawn up and used in search queries, see Table S1: Desk Research. The search results’ relevance was noted in a table to keep an overview of the processed work, e.g., the search query TITLE-ABS-KEY(ecmo AND Simulator) in Scopus Elsevier was sorted by relevance and provided 38 results of which 10 were relevant. The bibliography of all the relevant literature was read thoroughly to identify all the applicable literature. Selected literature was then reviewed by all authors and relevant information was summarized in the literature database. The examination of this literature lead to an overview of the developed and commercially available ECMO sims.
2.2. Fidelity Classification
To distinguish the level of fidelity between the ECMO sims, fidelity was categorized into: low-fidelity, mid-fidelity, and high-fidelity. Furthermore, the overall fidelity was derived from the median of the definition-based fidelity, component fidelity, and customization fidelity.
2.2.1. Definition-Based Fidelity
To determine the fidelity classification of ECMO sims, existing definitions were used, when possible, i.e., definition-based fidelity (DBF). These definitions have been derived from established dictionaries, standards, and literature, such as the oxford dictionary, the International Organization for Standardization (ISO), and The ELSO Red Book [40] (Table A1). According to the Healthcare Simulation Dictionary [41], DBF can be divided into four sub-categories: conceptual fidelity, functional fidelity, physical fidelity, and psychological fidelity. For conceptual fidelity, the differentiation between computational, physical, or a combination of both was determined. This was deduced from the available information about the ECMO sim. The level of functional, physical, and psychological fidelity was assigned by the authors’ educated guess based on the available ECMO information. When the level of fidelity was determined to be low, a minus (−) was assigned. When mid, a plus-minus (+/−) was appointed, and a plus (+) was set to the ECMO sim when high. Eventually, the median of these last three fidelities was calculated to determine the DBF classification and was agreed upon by all co-authors. As DBF classification is subjective, this classification was weighed alongside the component fidelity and the customization fidelity for improved objectiveness.
2.2.2. Component Fidelity
Component fidelity is based on the main components of ECMO: diagnostics, circuit priming, circuit monitoring, cannulation, connection ECMO/oxygenator, gas exchange, hemodynamics, weaning, decannulation, and (clinical) scenarios [42]. Based on the available information about the ECMO sim, the authors determined whether a component was included in the design or not. In case a component was included, it was specified if it was included computationally (C), physically (P), or as a combination of both. A total score out of 10 possible components determined whether the component fidelity is low, mid, or high. Low-fidelity was assigned to ECMO sims when the total ECMO components were ≤3, mid-fidelity was assigned when the total ECMO components were 4 to 7, while high fidelity was assigned when the total number of ECMO components were ≥8.
2.2.3. Customization Fidelity
Customization fidelity was based on the ability to adjust ECMO sim parameters to create more diverse patient-related scenarios. Similar to the component fidelity, the authors, based on the available ECMO sim information, determined whether a parameter was included in the design. The six parameters considered for ECMO sims were sex, age, body size, race, disease and/or anatomy, and BMI/fat percentage. These parameters were chosen to influence the ECMO procedure. Race was left out of a secondary classification for computational or a combination of computational and physical ECMO sims without representation of the patient, resulting in five parameters. Low customization fidelity was based on ≤2/6 or 1/5, mid-fidelity customization was between 2/6 and 5/6 or between 1/5 and 5/5, while high fidelity customization was achieved when ≥5/6 or 5/5.
2.2.4. Overall Fidelity
Finally, the median of the outcomes of all these fidelity types was calculated for each ECMO sim to determine the overall fidelity. Based on these outcomes, the ECMO sims were compared to each other and allocated to overall low-, mid-, and high-fidelity ECMO sims.
3. Results
Fidelity is “The ability of the simulation to reproduce the reactions, interactions, and responses of the real-world counterpart. It is not constrained to a certain type of simulation modality, and higher levels of fidelity are not required for a simulation to be successful” [41]. As stated, the different levels of fidelity do not affect the success of the simulation. However, the realism of the simulation (low-, mid-, or high-fidelity) needs to correspond to the training activity for it to be a success. For a complete list of the definitions, see Appendix A Table A1.
3.1. Definition-Based Fidelity
In this review, a total of thirty ECMO sims have been found, of which 26 ECMO simulations and simulators (ECMO sims) could be processed for classification in this review, see Supplementary File S1: Graphical Summary of ECMO sims. The classification of the ECMO sims based on the currently existing definitions is displayed in the definition-based fidelity (DBF) table, see Table S2: Definition-Based Fidelity.
According to our findings, 10 (38%) ECMO sims were computational (C), 7 (27%) ECMO sims were purely physical (P), and the other 9 (35%) ECMO sims were a combination of computational and physical (C + P). Furthermore, from these ECMO sims, 9 (35%) were of low-fidelity (C = 4; P = 4; C + P = 1), 12 (46%) were of mid-fidelity (C = 6; P = 1; C + P = 5), and 5 (19%) were of high-fidelity (C = 0; P = 2; C + P = 3). This shows that there are currently no high-fidelity computational ECMO sims available.
3.2. Component Fidelity
The results from the component fidelity were different from those results from the DBF, see Table S3: Component Fidelity. Out of the 26 ECMO sims, 9 (35%) were of low-fidelity, and 17 (65%) were of mid-fidelity. According to component fidelity, there are no high-fidelity ECMO sims. The hemodynamic effect was mimicked in most designs as 19 ECMO sims (73%) which included this either computationally (12), physically (5), or a combination of both (2). Clinical scenarios were just as often implemented in the design (C = 10; P = 1; C + P = 8). Cannulation was second-most included in 17 (65%) of the designed ECMO sims. Contrary to cannulation, decannulation was only (specifically) included in three ECMO sims (12%) and none of the ECMO sims (0%) had included weaning to their design.
3.3. Customization Fidelity
The final measured fidelity is the customization fidelity, Table S4: Customization Fidelity. Most (54%) ECMO sims did not have the option to model patient-specific scenarios. This resulted in 23 (88%) ECMO sims with low-fidelity and only 3 (12%) ECMO sims with mid-fidelity. The majority (38%) of the ECMO sims were able to adjust disease and/or anatomy parameter(s) but none (0%) of the ECMO sims were able to change sex. For customization fidelity, there were no high-fidelity classified ECMO sims as well.
3.4. Overall Fidelity
Taking the median of the fidelity mentioned above resulted in overall fidelity, see Table 1.

Table 1.
Overall fidelity classification of ECMO sims derived from definition-based, component, and customization fidelity.
Furthermore, 10 (38%) low-, 16 (62%) mid-, and no high-fidelity ECMO sims currently exist (Table 2). According to Table 2, none (0%) of the ECMO sims with a low overall fidelity managed to achieve a high definition-based, component, or customization fidelity. In fact, all ECMO sims with a low overall fidelity also have a low customization fidelity.
Table 2.
Summary of the overall fidelity classification of ECMO sims derived from definition-based, component, and customization fidelity.
Table 2 also shows that 5 (31%) out of the 16 mid-fidelity ECMO sims were determined to be of high definition-based fidelity. However, none of them reached a high overall fidelity based on our method. These 16 mid-fidelity ECMO sims could also not achieve a high component or customization fidelity.
Furthermore, Table 2 displays that only 3 (12%) out of the 26 ECMO sims could achieve a mid-fidelity level for the customization fidelity. On the other hand, 0 (0%) of the 26 ECMO sims managed to achieve high customization fidelity. Moreover, 17 (65%) out of the 26 ECMO sims achieved a mid-component fidelity status.
4. Discussion
This review aimed to collect current ECMO simulations and simulators (ECMO sims) and determine their level of fidelity through an objective classification method. We present a structured and objective classification method of ECMO sims created by a diverse and experienced group of users, researchers, and developers. This classification method is based on the overall ECMO sim fidelity, established by taking the median of the definition-based fidelity, component fidelity, and customization fidelity. Combined, a more objective overall fidelity was defined, resulting in a low-, mid-, or high-fidelity classification. According to this new classification, only low- and mid-fidelity ECMO sims are currently available.
4.1. Fidelity Classification
ECMO sims were only incorporated in the review if it was explicitly mentioned that they could be applied for ECMO training. Only information that was provided by the developers was processed. To provide the full spectrum of correct information on all the different ECMO sims, authors or companies were asked for additional official and public documentation when necessary.
The current classification fidelity of the ECMO sims is based on existing vocabulary defined and used by experts in the field (e.g., the International Nursing Association for Clinical and Simulation Learning, INACSL [43]). Therefore, all authors were asked to apply the terminology for component classification and other fidelities to allow for unequivocal definitions in ECMO practice.
The definition-based fidelity is based on the current way of (subjectively) classifying ECMO sims. However, Alhomsi, et al. [13] compared their work to different ECMO sims but lacked guidelines for comparison, making it subjective to the assessor. Other reviews [44,45,46] often put focus on the simulation-based education aspect. Because of these reasons, an objective review study about ECMO sims does not currently exist.
Therefore, component and customization fidelity were added to the mix to objectify the classification. The latter two only require the executor to identify parameters present in the ECMO sim, making the classification for these fidelity types the primary objective. Furthermore, for this review, all authors were asked to provide feedback on the preliminary classifications to improve objectivity. Due to the different backgrounds of the authors, the authors do not only represent many of the stakeholders, but the ECMO sims could be reviewed from a broad perspective, increasing objectivity. It is therefore encouraged that future ECMO sim classifications, using this method, are performed by a diverse group of assessors.
The reviewed ECMO sims could also use this method to increase their overall fidelity. e.g., the five ECMO sims [15,31,32,38,39] with a mid-overall fidelity and a high definition-based fidelity could look into the component and customization fidelity. By including more components and/or patient-specific parameters, they could increase these fidelity levels, e.g., if Curtis Life Research [31], Erler Zimmer [32], and The Simulator Company [39] would reach a high customization fidelity, their (median) overall fidelity would change from mid to high.
4.2. Limitations
Despite a thorough search, our ECMO sim database may not be complete. Additionally, only articles and literature written in the English language were included, so some ECMO sims may have been left out. Multiple search engines, such as Google Scholar, Scopus, PubMed, and regular Google searches, were consulted to avert the possibility of missing out on information by the latter. All bibliographies of included literature were also screened to identify other helpful literature. Although, a careful search strategy was used, some ECMO sims had no public information and were therefore not included in this review (e.g., Fresenius Heart and Lung App). In addition, this overview is accurate until 31 October 2022. This list may be updated in the future when new ECMO sims are developed.
Not all ECMO sims include specific simulation components in the same way. For example, some included gas exchange by changing the color of the blood in the lines. In contrast, others included gas exchange by adjusting the parameters digitally, and some had a combination of both. Therefore, the tables include how certain components are processed in the ECMO sims (computational: C; physical: P; or a combination of both: C + P). However, a similar approach does not mean similar quality. This also goes for the component and customization fidelity.
A quality threshold can be established through the verification and validation of an ECMO sim. However, an ECMO sim’s fidelity level and/or goals must be allocated before a design can be verified and/or validated, because verification and validation of, e.g., a low ECMO sim focusing solely on cannulation might be completely different from a mid-fidelity whole body ECMO sim. Therefore, this was separated from our methodology and is considered to be future work. However, we emphasize the importance of the verification and/or validation of simulations and simulators in general.
4.3. Future Prospective
We believe this method can fill the gap for developing, comparing, and classifying ECMO sims. For new developments, the method can be used for decision making on what to include to achieve a certain level of fidelity, e.g., according to this method, high component fidelity is achieved when at least 8 out of the 10 components have been included in the design and a high customization fidelity is obtained when at least 5 out of 6 (or 5) parameters have been included. This also means that when aiming for a mid (or low) fidelity classification, a developer can estimate how many components and/or parameters to include in the design to achieve this level. For research, it is now clear what has already been developed, and what still needs improvement (e.g., customizability).
For ECMO simulation-based training (SBT), this classification method helps clinicians to select the most suitable ECMO sim for the intended training purpose, e.g., cannulation or circuit monitoring. Indeed, selecting the right ECMO sim could help to achieve the set SBT goals faster. It could therefore in the future be interesting to develop a selection tool, based on this method, to aid this decision-making process. Furthermore, objective classification of simulations and simulators, as shown in this work, could be used beyond ECMO SBT. Applying this method in other (medical) fields could help to improve development, selection, and the comparison of simulations and simulators used for SBT.
Therefore, it could be helpful if organizations, such as the Extracorporeal Life Support Organization (ELSO), would promote the standardization of the classification in an objective manner. Our method could be the foundation for this matter.
Finally, the implementation and effectiveness of virtual reality and mixed reality in an ECMO sim could be explored in the future.
5. Conclusions
An overall fidelity was created to objectively classify based on definition-based, com-ponent, and customization fidelity. According to our new method, no high-fidelity ECMO sims currently exist, urging for the development of a high-fidelity simulator to improve ECMO-team training and potentially improve patient out-comes. This comparison method may be used in the future for the description of newly developed ECMO sims.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/jcm12051765/s1, Supplementary File S1: Graphical Summary of ECMO sims; Table S1: Desk Research; Table S2: Definition-Based Fidelity; Table S3: Component Fidelity; Table S4: Customization Fidelity.
Author Contributions
Conceptualization, W.C.D., J.A. and F.R.H.; methodology, W.C.D., J.A. and F.R.H., validation, W.C.D.; formal analysis, W.C.D., J.A. and F.R.H.; investigation, W.C.D.; resources, W.C.D., J.A., J.S. and J.R.; data curation, W.C.D., J.A. and F.R.H.; writing—original draft preparation, W.C.D.; writing—review and editing, W.C.D., L.F., J.S., P.T., J.R., V.O., M.P., M.D., J.A. and F.R.H.; visualization, W.C.D. and F.R.H.; supervision, F.R.H. and J.A.; project administration, W.C.D., F.R.H. and J.A.; funding acquisition, J.A. and F.R.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the 2022 “Boost Your Research” Fund in the Priority Program SPP 2014 “Towards an Implantable Lung” by the DFG, the German Research Foundation, grant number 20003297 UKA.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable, all data is shared in this manuscript and its supplements.
Conflicts of Interest
The authors declare no conflict of interest. The funder had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Appendix A
Established nomenclature based on existing literature (Table A1, left column) and slight changes based on our expert opinion when these definitions are applied to the field of ECMO simulation.
Table A1.
Nomenclature created out of existing definitions. The first column shows the word, the second column cites the definition found in the literature, the third column displays the source in which the definition was found, and the fourth column presents an altered definition in case the literature definitions did not correlate with the specific application of ECMO.
Table A1.
Nomenclature created out of existing definitions. The first column shows the word, the second column cites the definition found in the literature, the third column displays the source in which the definition was found, and the fourth column presents an altered definition in case the literature definitions did not correlate with the specific application of ECMO.
| Word | Literature Definition | Source | Our Definition |
|---|---|---|---|
| Cannulation | “A thin tube inserted into a vein or body cavity to administer medication, drain off fluid, or insert a surgical instrument”. “Cannulae are integral parts of the circuit and provide the intravascular connections to the patient”. | [47] [42] | Technique to insert a tube, also known as cannulae, into a vessel (vein or artery). Cannulae are integral parts of the circuit and provide the intravascular connections to the patient. |
| (Clinical) Scenarios | “A deliberately designed simulation experience (also known as a case), that provides participants with an opportunity to meet identified objectives. The scenario provides a context for the simulation and can vary in length and complexity, depending on the objectives.” [48,49,50,51,52] | Taken from source(s) in [43] | A deliberately designed simulation experience (also known as a case), that provides participants with an opportunity to meet identified objectives. The scenario provides a clinically plausible context for the simulation and can vary in length and complexity, depending on the objectives. |
| Circuit priming | “The prime is recirculated through a reservoir until all bubbles are removed”. “The ECLS circuit is primed under sterile conditions”. | [40] | The prime is recirculated through a reservoir until all bubbles are removed (de-airing) before connection to the patient. “The ECLS circuit is primed under sterile conditions” |
| Circuit monitoring | “a device used for observing, checking, or keeping a continuous record of something”. “Circuit monitoring is required to ensure the proper functionality of the circuit and to guide proper management. Common circuit monitoring techniques include flow, pressure, and saturation monitoring through integrated or external sensors”. | [47] [42] | A method used for observing, checking, or keeping a continuous record of flows, pressures, blood features, and other attributes. Circuit monitoring is required to ensure the proper functionality of the circuit and to guide effective patient management. Common circuit monitoring techniques include integrated or external sensors to detect blood flow, pressures, pump speed (rotations per minute), and oxygen saturation. |
| Component fidelity | N/A | N/A | Fidelity based on the main components of ECMO: diagnostics, circuit priming, circuit monitoring, cannulation, connection ECMO/oxygenator, gas exchange, hemodynamics, weaning, decannulation, and (clinical) scenarios [42] |
| Computational (simulator) | “using or relating to computers” “relating to the process of mathematical calculation” | [47] | A simulation relating to the process of mathematical calculations performed by a computer. |
| Conceptual fidelity | “In health care simulation, ensures that all elements of the scenario relate to each other in a realistic way so that the case makes sense as a whole to the learner(s) (For example: Vital signs are consistent with the diagnosis)”. | [41] | N/A |
| Connection oxygenator | “the action of linking one thing with another”, in this case the oxygenator with the accompanying equipment. | [47] | N/A |
| Customization (fidelity) | “modify (something) to suit a particular individual or task” | [47] | “modify (something) to suit a particular individual or task”, in this case the patient simulator related parameters: sex, age, size, race, disease and/or anatomy, and fat percentage/BMI. |
| Decannulation | “Extubation of a cannula” | [53] | Removal of a cannula. |
| Diagnosis/diagnostics | “The identification of the nature of an illness or other problem by examination of the symptoms”. | [47] | N/A |
| Environmental fidelity | “The degree to which the simulated environment (manikin, room, tools, equipment, moulage, and sensory props) replicates reality and appearance of the real environment”. | [41] | N/A |
| (Definition-based) Fidelity | “The ability of the simulation to reproduce the reactions, interactions, and responses of the real-world counterpart. It is not constrained to a certain type of simulation modality, and higher levels of fidelity are not required for a simulation to be successful”. | [41] | N/A |
| Functional fidelity | “The degree in which the equipment used in the simulation responds to the participant’s actions; e.g., a static ventilator would offer low functional fidelity compared to a working ventilator in a simulation requiring a ventilator alarm”. | [41] | N/A |
| Gas exchange | “The ability to simulate lung function through the use of an artificial lung”. “Oxygen and CO2 diffuse between the gas and the blood as a function of the gradient between the partial pressures on each side”. | [42] [40] | N/A |
| Hemodynamics | “Relating to the flow of blood within the organs and tissues of the body” “…the distribution of blood flow and blood pressure in the vascular system. The main factors involved are the pulsatile driving pressure generated by the heart, the flow characteristics of blood, and the geometric structure and mechanical properties of the vessels. … In medical contexts, the term “hemodynamics” often refers to basic measures of cardiovascular function, such as arterial pressure or cardiac output.” | [47] [54] | Basic measures of cardiovascular function, relating to blood flow and pressure in the vascular system, and perfusion within the organs and tissues of the body. The main factors involved are the pulsatile driving pressure generated by the heart, the flow characteristics of blood, and the geometric structure and mechanical properties of the vessels. |
| High-fidelity simulator | “A term often used to refer to the broad range of full-body manikins that have the ability to mimic, at a very high level, human body functions”. | [41] | A term often used to refer to the broad range of full-body models or manikins that have the ability to mimic, at a very high level, human body functions. |
| High-fidelity simulation | “In health care simulation, high-fidelity refers to simulation experiences that are extremely realistic and provide a high level of interactivity and realism for the learner [55]. It can apply to any mode or method of simulation; for example: human, manikin, task trainer, or virtual reality.” | Taken from source in [41] | N/A |
| Immersive simulation | “A simulation session influenced by participants’ characteristics, experiences, level of training, and preparation for the case or task,. The perceived physical, conceptual and emotional fidelity, the appropriate level of challenge, and the simulators and actors can all affect the simulation experience” [56] | Taken from source in [41] | N/A |
| Low-fidelity | “Not needing to be controlled or programmed externally for the learner to participate [57]; examples include case studies, role playing, or task trainers used to support students or professionals in learning a clinical situation or practice (Adapted from [58])”. | Taken from source in [41] | N/A |
| Manikin/mannikin | “A jointed model of the human body, used in anatomy or as an artist’s lay figure”. | [47] | N/A |
| Mid-fidelity | “Use of computer technology to assist learners in developing competencies in skills” | [59] | Use of (computer) technology to assist learners in developing competencies in skills. |
| Overall fidelity | N/A | N/A | The definite fidelity of an ECMO simulation or simulator derived from definition-based, component, and customization fidelity. |
| Physical fidelity | “The degree to which the simulation looks, sounds, and feels like the actual task” [60] | Taken from source in [41] | N/A |
| Physical (simulator) | See also Physical fidelity. | N/A | Simulations substituting an object (or person) for an, often simplified, material representation as a real-life counterpart. |
| Psychological fidelity | “The degree of perceived realism, including psychological factors such as emotions, beliefs, and self-awareness of participants in simulation scenarios” [61]. | Taken from source in [41] | N/A |
| Realism | “Refers to the physical characteristics of the activity, semantical aspects of the activity (theories and conceptual relations–if A happens then B occurs), and/or the phenomenal aspects of the activity (emotions, beliefs, and thoughts experienced).” | [41] | N/A |
| Simulation | “A technique that creates a situation or environment to allow persons to experience a representation of a real event for the purpose of practice, learning, evaluation, testing, or to gain understanding of systems or human actions”. | [41] | N/A |
| Simulation fidelity | “The physical, semantic, emotional, and experiential accuracy that allows persons to experience a simulation as if they were operating in an actual activity (SSH)” | [41] | N/A |
| Weaning | “Accustom (someone) to managing without something which they have become dependent on” “The transition to normal patient circulation and physiology from extracorporeal circulation”. | [47] [62] | Accustom (someone) to managing without ECMO which they have become dependent on. Also known as: the transition to normal patient circulation and physiology from extracorporeal circulation. |
References
- Brodie, D.; Bacchetta, M. Extracorporeal Membrane Oxygenation for ARDS in Adults. N. Engl. J. Med. 2012, 366, 1905–1914. [Google Scholar] [CrossRef] [PubMed]
- Eckman, P.M.; Katz, J.N.; El Banayosy, A.; Bohula, E.A.; Sun, B.; van Diepen, S. Veno-Arterial Extracorporeal Membrane Oxygenation for Cardiogenic Shock: An Introduction for the Busy Clinician. Circulation 2019, 140, 2019–2037. [Google Scholar] [CrossRef] [PubMed]
- Costa, A.M.; Halfwerk, F.; Wiegmann, B.; Neidlin, M.; Arens, J. Trends, Advantages and Disadvantages in Combined Extracorporeal Lung and Kidney Support from a Technical Point of View. Front. Med. Technol. 2022, 4, 909990. [Google Scholar] [CrossRef] [PubMed]
- Nunez, J.I.; Gosling, A.F.; O’Gara, B.; Kennedy, K.F.; Rycus, P.; Abrams, D.; Brodie, D.; Shaefi, S.; Garan, A.R.; Grandin, E.W. Bleeding and thrombotic events in adults supported with venovenous extracorporeal membrane oxygenation: An ELSO registry analysis. Intensive Care Med. 2022, 48, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Pavlushkov, E.; Berman, M.; Valchanov, K. Cannulation techniques for extracorporeal life support. Ann. Transl. Med. 2017, 5, 70. [Google Scholar] [CrossRef]
- Supady, A.; Combes, A.; Barbaro, R.P.; Camporota, L.; Diaz, R.; Fan, E.; Giani, M.; Hodgson, C.; Hough, C.L.; Karagiannidis, C.; et al. Respiratory indications for ECMO: Focus on COVID-19. Intensive Care Med. 2022, 48, 1326–1337. [Google Scholar] [CrossRef]
- Belohlavek, J.; Smalcova, J.; Rob, D.; Franek, O.; Smid, O.; Pokorna, M.; Horak, J.; Mrazek, V.; Kovarnik, T.; Zemanek, D.; et al. Effect of Intra-arrest Transport, Extracorporeal Cardiopulmonary Resuscitation, and Immediate Invasive Assessment and Treatment on Functional Neurologic Outcome in Refractory Out-of-Hospital Cardiac Arrest: A Randomized Clinical Trial. JAMA 2022, 327, 737–747. [Google Scholar] [CrossRef]
- Combes, A.; Brodie, D.; Bartlett, R.; Brochard, L.; Brower, R.; Conrad, S.; De Backer, D.; Fan, E.; Ferguson, N.; Fortenberry, J.; et al. Position paper for the organization of extracorporeal membrane oxygenation programs for acute respiratory failure in adult patients. Am. J. Respir. Crit. Care Med. 2014, 190, 488–496. [Google Scholar] [CrossRef]
- Barbaro, R.P.; Odetola, F.O.; Kidwell, K.M.; Paden, M.L.; Bartlett, R.H.; Davis, M.M.; Annich, G.M. Association of hospital-level volume of extracorporeal membrane oxygenation cases and mortality. Analysis of the extracorporeal life support organization registry. Am. J. Respir. Crit. Care Med. 2015, 191, 894–901. [Google Scholar] [CrossRef]
- Rabie, A.A.; Azzam, M.H.; Al-Fares, A.A.; Abdelbary, A.; Mufti, H.N.; Hassan, I.F.; Chakraborty, A.; Oza, P.; Elhazmi, A.; Alfoudri, H.; et al. Implementation of new ECMO centers during the COVID-19 pandemic: Experience and results from the Middle East and India. Intensive Care Med. 2021, 47, 887–895. [Google Scholar] [CrossRef]
- Nagaoka, E.; Arai, H.; Ugawa, T.; Masuda, T.; Ochiai, K.; Tamaoka, M.; Kurashima, N.; Oi, K.; Fujiwara, T.; Yoshida, M.; et al. Efficacy of multidisciplinary team approach with extracorporeal membrane oxygenation for COVID-19 in a low volume ECMO center. Artif. Organs 2021, 45, 1061–1067. [Google Scholar] [CrossRef]
- Gaba, D.M.; DeAnda, A. A comprehensive anesthesia simulation environment: Re-creating the operating room for research and training. Anesthesiology 1988, 69, 387–394. [Google Scholar] [CrossRef]
- Alhomsi, Y.; Alsalemi, A.; Noorizadeh, M.; Bensaali, F.; Meskin, N.; Hssain, A.A. A Modular Approach for a Patient Unit for Extracorporeal Membrane Oxygenation Simulator. Membranes 2021, 11, 424. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Allan, C.K.; Pigula, F.; Bacha, E.A.; Emani, S.; Fynn-Thompson, F.; Thiagarajan, R.R.; Imprescia, A.; Hayes, G.; Weinstock, P. An extracorporeal membrane oxygenation cannulation curriculum featuring a novel integrated skills trainer leads to improved performance among pediatric cardiac surgery trainees. Simul. Healthc. 2013, 8, 221–228. [Google Scholar] [CrossRef]
- Broman, M.; Frenckner, B.; Bjällmark, A.; Broomé, M. Recirculation during Veno-Venous Extra-Corporeal Membrane Oxygenation—A Simulation Study. Int. J. Artif. Organs 2015, 38, 23–30. [Google Scholar] [CrossRef]
- Colasanti, S.; Piemonte, V.; Devolder, E.; Zieliński, K.; Vandendriessche, K.; Meyns, B.; Fresiello, L. Development of a computational simulator of the extracorporeal membrane oxygenation and its validation with in vitro measurements. Artif. Organs 2021, 45, 399–410. [Google Scholar] [CrossRef]
- Endo, T.; Kagaya, Y.; Arata, Y.; Imai, H. Long-term efficacy of an extracorporeal membrane oxygenation simulation with a novel, low-cost vascular model “Endo-Circuit”. Acute Med. Surg. 2017, 4, 79–88. [Google Scholar] [CrossRef]
- Lansdowne, W.; Machin, D.; Grant, D.J. Development of the Orpheus Perfusion Simulator for Use in High-fidelity Extracorporeal Membrane Oxygenation Simulation. J. ExtraCorporeal Technol. 2012, 44, 250–255. [Google Scholar]
- Mahmoud, A.; Hssain, A.A.; Alinier, G.; Hassan, I.; Khurshid, U.; Abducarim, A.; Mahmud, S.; Abdallah, O.; Mohamed, E.; Alsalemi, A.; et al. Preliminary Implementation of the Next Generation Cannulation Simulator. IEEE Stud. Conf. Res. Dev. 2019, 2019, 243–247. [Google Scholar]
- Palmer, D.; Aspenleiter, M.; da Silva, J.; Castro-Medina, M.; Morell, V.; Sharma, M.; Viegas, M. A High-Fidelity Surgical Model and Perfusion Simulator Used to Demonstrate ECMO Cannulation, Initiation, and Stabilization. J. ExtraCorporeal Technol. 2019, 51, 6. [Google Scholar]
- Palmer, D.; Aspenleiter, M.; da Silva, J.; Da Fonseca da Silva, L.; Medina-Castro, M.; Grayson, M.; Morell, V.; Palmer, A.; Sharma, M.; Stebler, J.; et al. A High-Fidelity Percutaneous Model Used to Demonstrate ECMO Cannulation. J. ExtraCorporeal Technol. 2021, 53, 208–213. [Google Scholar] [CrossRef]
- Puslecki, M.; Ligowski, M.; Kiel, M.; Dabrowski, M.; Stefaniak, S.; Sip, M.; Maciejewski, A.; Dabrowska, A.; Kiel-Puslecka, I.; Kłosiewicz, T.; et al. Prototype of extracorporeal membrane oxygenation (ECMO) therapy simulator used in regional ECMO program. J. Thorac. Dis. 2018, 10, 5073–5079. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.L.; Grisham, L.M.; Scott, J.; Mogan, C.; Prescher, H.; Biffar, D.; Jarred, J.; Meyer, R.J.; Hamilton, A.J. Construction of a reusable, high-fidelity model to enhance extracorporeal membrane oxygenation training through simulation. Adv. Neonatal Care 2014, 14, 103–109. [Google Scholar] [CrossRef]
- Zanella, A.; Salerno, D.; Scaravilli, V.; Giani, M.; Castagna, L.; Magni, F.; Carlesso, E.; Cadringher, P.; Bombino, M.; Grasselli, G.; et al. A mathematical model of oxygenation during venovenous extracorporeal membrane oxygenation support. J. Crit. Care 2016, 36, 178–186. [Google Scholar] [CrossRef]
- 3-Dmed. ECMO Simulation Kit. Available online: https://www.3-dmed.com/wp-content/uploads/2019/05/ECMO-Simulation-Kit.pdf (accessed on 10 October 2022).
- Califia Patient Simulator. Available online: https://www.biomedsimulation.com/califia-3-0/ (accessed on 11 October 2022).
- Califia Lung Simulator. Available online: https://www.biomedsimulation.com/califia-lung/ (accessed on 11 October 2022).
- Parallel Simulator. Available online: https://www.chalicemedical.com/products/parallel-simulator/ (accessed on 12 October 2022).
- ECMO Trainer Evolution III. Available online: https://www.crea-plast.com/en/45-ecmo-trainer (accessed on 12 October 2022).
- Eigenflow ECMO Simulator. Available online: https://curtisliferesearch.com/eigenflow-ecmo-simulator/ (accessed on 10 October 2022).
- ECMO Trainer Professional MK2. Available online: https://erler-zimmer.de/shop/en/10953 (accessed on 31 October 2022).
- ECMO Training Simulator. Available online: https://healtheng.illinois.edu/about/researchareas/simulationeducation/ecmo (accessed on 24 October 2022).
- Hybrids Vita. Available online: https://hybrids-vita.com/en.html (accessed on 30 November 2022).
- MSE ECMO Simulator. Available online: http://www.ecmosimulation.com/ (accessed on 17 December 2022).
- Harvi ECMO. Available online: https://harvi.online/site/welcome/harvi-ecmo/ (accessed on 12 October 2022).
- ECMOjo Simulator. Available online: https://ecmojo.sourceforge.net/ (accessed on 12 October 2022).
- RediStik ECMO Cannulation Trainer. Available online: https://www.youtube.com/watch?v=0wt5EHxH3CM (accessed on 11 November 2022).
- E-SIM Pro. Available online: https://www.thesimulatorcompany.com/e-sim-pro (accessed on 12 October 2022).
- Brogan, T.V.; Lequier, L.; Lorusso, R.; MacLaren, G.; Peek, G. Extracorporeal Life Support: The ELSO Red Book, 5th ed.; Extracorporeal Life Support Organization: Ann Arbor, MI, USA, 2017. [Google Scholar]
- Lioce, L.; Downing, D.; Chang, T.P.; Robertson, J.M.; Anderson, M.; Diaz, D.A.; Spain, A.E. The Terminology and Concepts Working Group. In Healthcare Simulation Dictionary, 2nd ed.; Lioce, L., Lopreiato, J., Spain, A.E., Eds.; Agency for Healthcare Research and Quality: Rockville, MD, Australia, 2020. [Google Scholar]
- Vercaemst, L.; Maul, T.M.; Arens, J.; Toomasian, J.M. Chapter 3: The Circuit. In Extracorporeal Life Support: The ELSO Red Book, 6th ed.; Extracorporeal Life Support Organization: Ann Arbor, MI, USA, 2022. [Google Scholar]
- INACSL Standards Committee. INACSL Standards of Best Practice: Simulation Simulation Glossary. Clin. Simul. Nurs. 2016, 12, S39–S47. [Google Scholar] [CrossRef]
- Glass, K.M. Research in ECMO Simulation: A Review of the Literature. In Comprehensive Healthcare Simulation: ECMO Simulation; Comprehensive Healthcare Simulation; Springer: Midtown Manhattan, NY, USA, 2021; pp. 147–152. [Google Scholar]
- Han, P.K.; Purkey, N.J.; Kuo, K.W.; Ryan, K.R.; Woodward, A.L.; Jahadi, O.; Prom, N.L.; Halamek, L.P.; Johnston, L.C. A Scoping Review and Appraisal of Extracorporeal Membrane Oxygenation Education Literature. ATS Sch. 2022, 3, 468–484. [Google Scholar] [CrossRef]
- Alinier, G.; Oriot, D. Simulation-based education: Deceiving learners with good intent. Adv. Simul. 2022, 7, 8. [Google Scholar] [CrossRef]
- Oxford University Press. Oxford Dictionary of English; Oxford University Press: New York, NY, USA, 2022. [Google Scholar]
- Waxman, K.T. The development of evidence-based clinical simulation scenarios: Guidelines for nurse educators. J. Nurs. Educ. 2010, 49, 29–35. [Google Scholar] [CrossRef]
- Rudolph, J.W.; Raemer, D.B.; Simon, R. Establishing a safe container for learning in simulation: The role of the presimulation briefing. Simul. Healthc. 2014, 9, 339–349. [Google Scholar] [CrossRef]
- Alinier, G. Developing High-Fidelity Health Care Simulation Scenarios: A Guide for Educators and Professionals. Simul. Gaming 2010, 42, 9–26. [Google Scholar] [CrossRef]
- Aschenbrenner, D.S.; Milgrom, L.B.; Settles, J. Designing simulation scenarios to promote learning. In Simulation in Nursing Education: From Conceptualization to Evaluation; Wolters Kluwer Health: New York, NY, USA, 2012. [Google Scholar]
- Lioce, L.; Meakim, C.H.; Fey, M.K.; Chmil, J.V.; Mariani, B.; Alinier, G. Standards of Best Practice: Simulation Standard IX: Simulation Design. Clin. Simul. Nurs. 2015, 11, 309–315. [Google Scholar] [CrossRef]
- Miller-Keane, O.T. Miller-Keane Encyclopedia & Dictionary of Medicine, Nursing & Allied Health, 7th ed.; Elsevier: Amsterdam, The Netherlands, 2003; p. 2344. [Google Scholar]
- Secomb, T.W. Hemodynamics. Compr. Physiol. 2016, 6, 975–1003. [Google Scholar] [CrossRef]
- INACSL Standards Committee. INACSL Standards of Best Practice: Simulation sm: Operations. Clin. Simul. Nurs. 2017, 13, 681–687. [Google Scholar] [CrossRef]
- Hamstra, S.J.; Brydges, R.; Hatala, R.; Zendejas, B.; Cook, D.A. Reconsidering fidelity in simulation-based training. Acad. Med. 2014, 89, 387–392. [Google Scholar] [CrossRef]
- Palaganas, J.C.; Maxworthy, J.C.; Epps, C.A.; Mancini, M.E. Defining Excellence in Simulation Programs, 1st ed.; LWW: Philadelphia, PA, USA, 2014. [Google Scholar]
- National League for Nursing Simulation Innovation Resource Center (NLN-SIRC). Available online: http://sirc.nln.org/mod/glossary/view.php?id¼183 (accessed on 8 November 2022).
- Akhtar-Danesh, N.; Baxter, P.; Valaitis, R.K.; Stanyon, W.; Sproul, S. Nurse Faculty Perceptions of Simulation Use in Nursing Education. West. J. Nurs. Res. 2009, 31, 312–329. [Google Scholar] [CrossRef]
- Alexander, A.; Sidman, J.; Brunyé, T.T.; Weil, S.A. From Gaming to Training: A Review of Studies on Fidelity, Immersion, Presence, and Buyin and Their Effects on Transfer in PC-Based Simulations and Games. DARWARS Train. Impact Group 2005, 5, 1–14. [Google Scholar]
- Dieckmann, P.; Rall, M. Designing a Scenario as a Simulated Clinical Experience: The TuPASS Scenario Script. In Clinical Simulation: Operations, Engineering, and Management, 1st ed.; Academic Press: Cambridge, MA, USA, 2008; pp. 541–550. [Google Scholar]
- ISO/TS 23810:2018; Cardiovascular Implants and Artificial Organs—Checklists for Use of Extracorporeal Circulation Equipment. ISO: Geneva, Switzerland, 2018.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).