
The Very Long COVID: Persistence of Symptoms after 12–18 Months from the Onset of Infection and Hospitalization

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
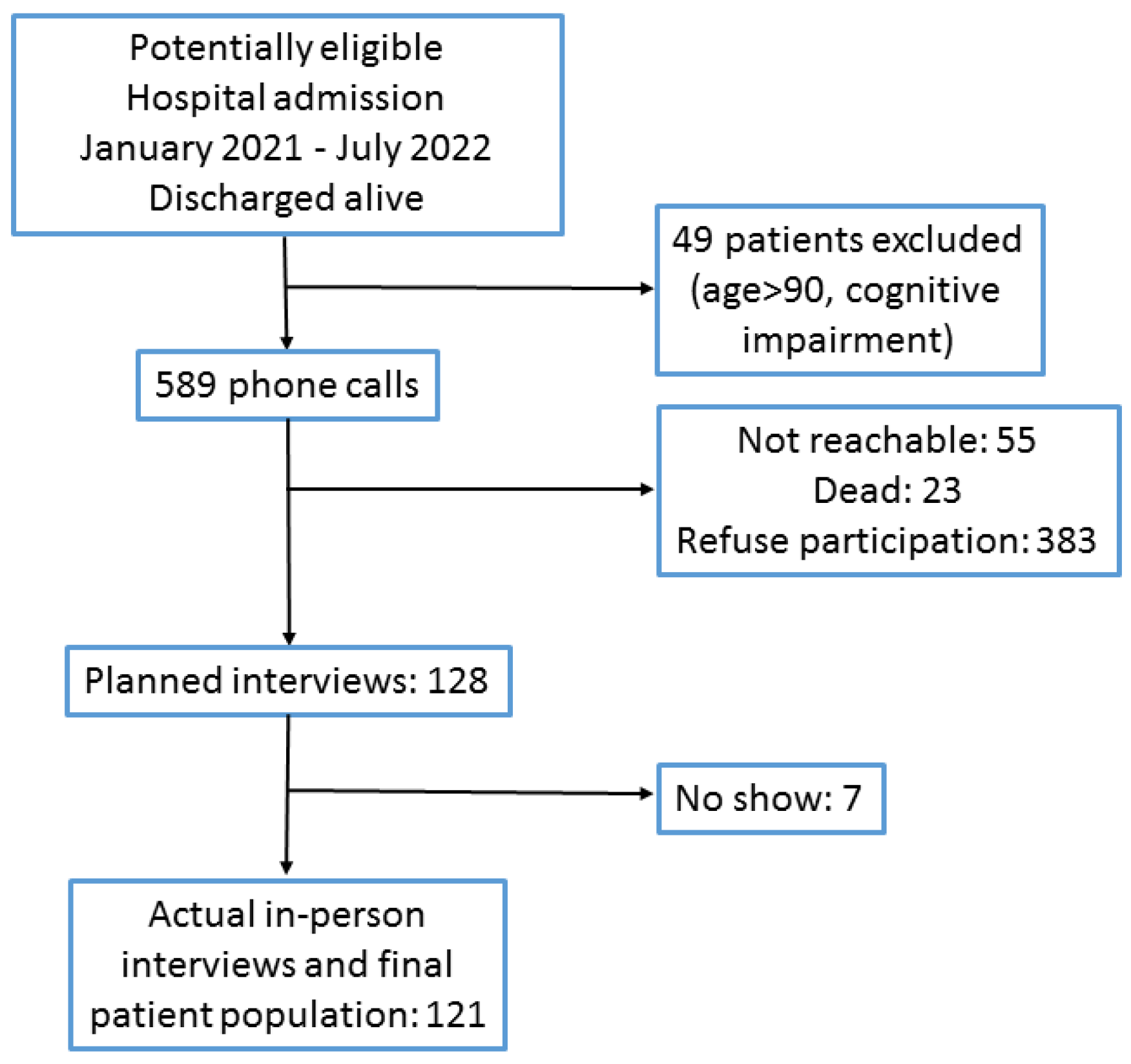
2.1. Patient Population and Study Procedures
2.2. Data Collection and Definitions
2.3. Statistical Analysis
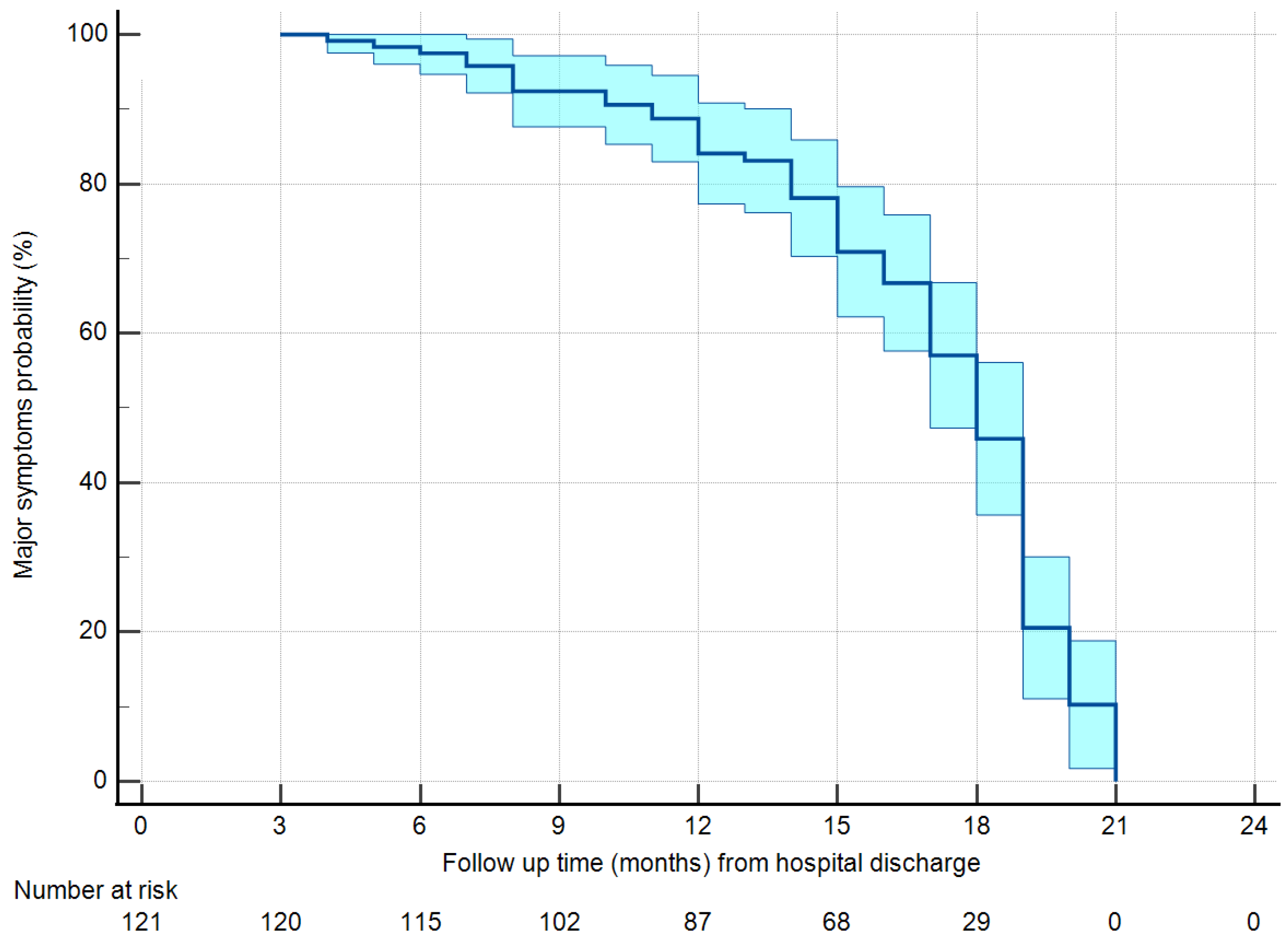
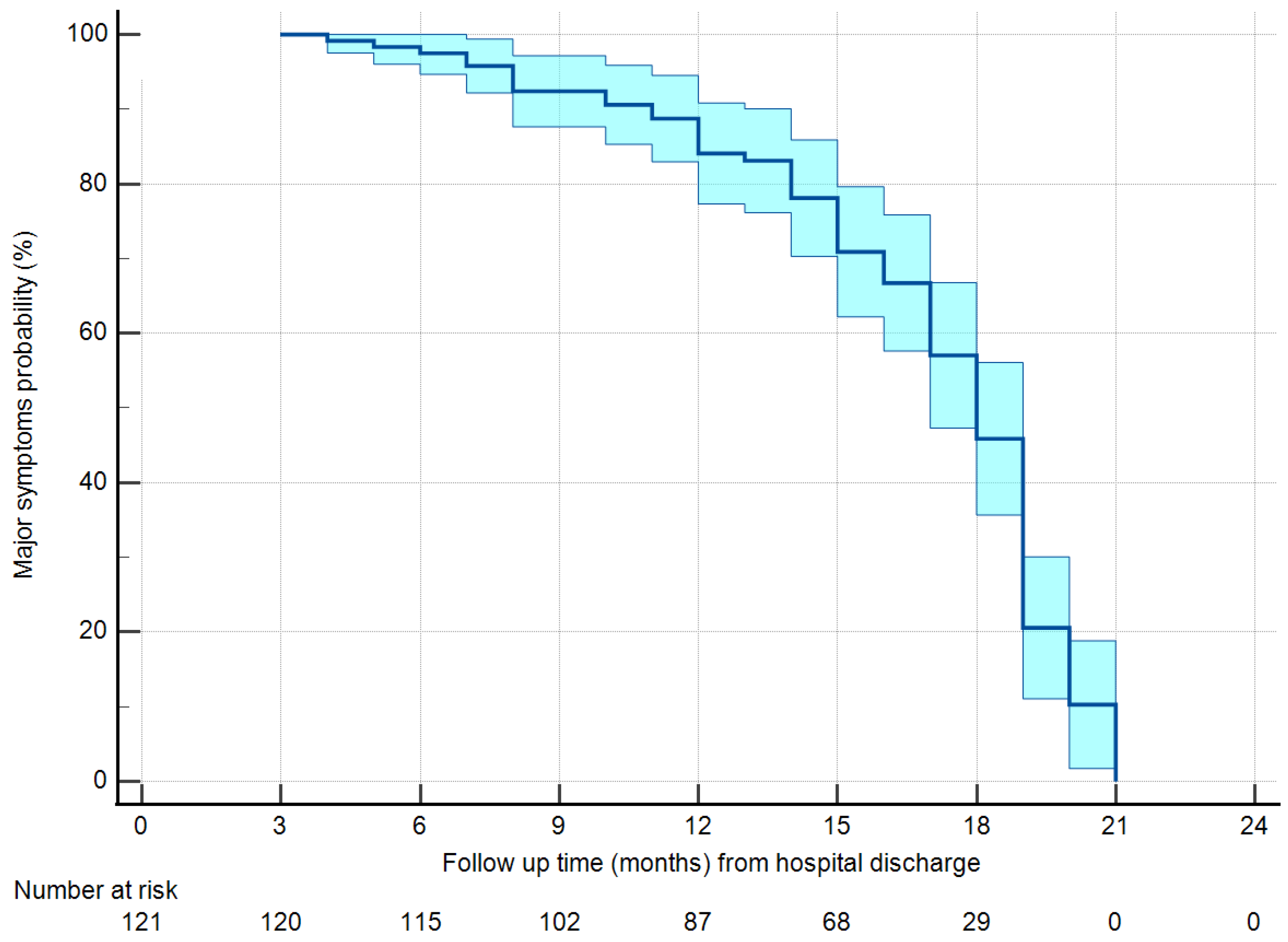
3. Results
4. Discussion
Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Post COVID-19 Condition (Long COVID). Available online: https://www.who.int/europe/news-room/fact-sheets/item/post-covid-19-condition (accessed on 7 January 2023).
- Chopra, V.; Flanders, S.A.; O’Malley, M.; Malani, A.N.; Prescott, H.C. Sixty-Day Outcomes Among Patients Hospitalized with COVID-19. Ann. Intern. Med. 2021, 174, 576–578. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef] [PubMed]
- Arnold, D.T.; Hamilton, F.W.; Milne, A.; Morley, A.J.; Viner, J.; Attwood, M.; Noel, A.; Gunning, S.; Hatrick, J.; Hamilton, S.; et al. Patient outcomes after hospitalisation with COVID-19 and implications for follow-up: Results from a prospective UK cohort. Thorax 2021, 76, 399–401. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Pérez, O.; Merino, E.; Leon-Ramirez, J.M.; Andres, M.; Ramos, J.M.; Arenas-Jiménez, J.; Asensio, S.; Sanchez, R.; Ruiz-Torregrosa, P.; Galan, I.; et al. COVID19-ALC research group. Post-acute COVID-19 syndrome. Incidence and risk factors: A Mediterranean cohort study. J. Infect. 2021, 82, 378–383. [Google Scholar] [CrossRef] [PubMed]
- Halpin, S.J.; McIvor, C.; Whyatt, G.; Adams, A.; Harvey, O.; McLean, L.C.; Kemp, S.; Corrado, J.; Singh, R.; Collins, T.; et al. Postdischarge symptoms and rehabilitation needs in survivors of COVID-19 infection: A cross-sectional evaluation. J. Med. Virol. 2021, 93, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, L.G.; Gourna Paleoudis, E.; Lesky-Di Bari, D.; Nyirenda, T.; Friedman, T.; Gupta, A.; Rasouli, L.; Zetkulic, M.; Balani, B.; Ogedegbe, C.; et al. Persistence of symptoms and quality of life at 35 days after hospitalization for COVID-19 infection. PLoS ONE 2020, 15, e0243882. [Google Scholar] [CrossRef] [PubMed]
- Garrigues, E.; Janvier, P.; Kherabi, Y.; Le Bot, A.; Hamon, A.; Gouze, H.; Doucet, L.; Berkani, S.; Oliosi, E.; Mallart, E.; et al. Post-discharge persistent symptoms and health-related quality of life after hospitalization for COVID-19. J. Infect. 2020, 81, e4–e6. [Google Scholar] [CrossRef]
- Novelli, L.; Raimondi, F.; Carioli, G.; Carobbio, A.; Pappacena, S.; Biza, R.; Trapasso, R.; Anelli, M.; Amoroso, M.; Allegri, C.; et al. HPG23 Covid19 Study Group. One-year mortality in COVID-19 is associated with patients’ comorbidities rather than pneumonia severity. Respir. Med. Res. 2022, 83, 100976. [Google Scholar]
- Ortega-Paz, L.; Arévalos, V.; Fernández-Rodríguez, D.; Jiménez-Díaz, V.; Bañeras, J.; Campo, G.; Rodríguez-Santamarta, M.; Díaz, J.F.; Scardino, C.; Gómez-Álvarez, Z.; et al. CV COVID-19 registry investigators. One-year cardiovascular outcomes after coronavirus disease 2019: The cardiovascular COVID-19 registry. PLoS ONE 2022, 17, e0279333. [Google Scholar] [CrossRef]
- Watanabe, A.; So, M.; Iwagami, M.; Fukunaga, K.; Takagi, H.; Kabata, H.; Kuno, T. One-year follow-up CT findings in COVID-19 patients: A systematic review and meta-analysis. Respirology 2022, 27, 605–616. [Google Scholar] [CrossRef] [PubMed]
- Cavaco, S.; Sousa, G.; Gonçalves, A.; Dias, A.; Andrade, C.; Pereira, D.; Aires, E.A.; Moura, J.; Silva, L.; Varela, R.; et al. Predictors of cognitive dysfunction one-year post COVID-19. Neuropsychology, 2023; epub ahead of print. [Google Scholar] [CrossRef]
- Kalak, G.; Jarjou’i, A.; Bohadana, A.; Wild, P.; Rokach, A.; Amiad, N.; Abdelrahman, N.; Arish, N.; Chen-Shuali, C.; Izbicki, G. Prevalence and Persistence of Symptoms in Adult COVID-19 Survivors 3 and 18 Months after Discharge from Hospital or Corona Hotels. J. Clin. Med. 2022, 11, 7413. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Canales, L.G.; Muñoz-Corona, C.; Barrera-Chávez, I.; Viloria-Álvarez, C.; Macías, A.E.; Guaní-Guerra, E. Quality of Life and Persistence of Symptoms in Outpatients after Recovery from COVID-19. Medicina 2022, 58, 1795. [Google Scholar] [CrossRef] [PubMed]
- Arjun, M.C.; Singh, A.K.; Pal, D.; Das, K.; Alekhya, G.; Venkateshan, M.; Mishra, B.; Patro, B.K.; Mohapatra, P.R.; Subba, S.H. Characteristics and predictors of Long COVID among diagnosed cases of COVID-19. PLoS ONE 2022, 17, e0278825. [Google Scholar] [CrossRef] [PubMed]
- UKHSA Review Shows Vaccinated Less Likely to Have Long COVID than Unvaccinated. Available online: https://www.gov.uk/government/news/ukhsa-review-shows-vaccinated-less-likely-to-have-long-covid-than-unvaccinated (accessed on 13 January 2022).
- Romero-Rodríguez, E.; Pérula-de Torres, L.Á.; Castro-Jiménez, R.; González-Lama, J.; Jiménez-García, C.; González-Bernal, J.J.; González-Santos, J.; Vélez-Santamaría, R.; Sánchez-González, E.; Santamaría-Peláez, M. Hospital admission and vaccination as predictive factors of long COVID-19 symptoms. Front. Med. 2022, 9, 1016013. [Google Scholar] [CrossRef] [PubMed]
- Bellan, M.; Apostolo, D.; Albè, A.; Crevola, M.; Errica, N.; Ratano, G.; Tonello, S.; Minisini, R.; D’Onghia, D.; Baricich, A.; et al. Determinants of long COVID among adults hospitalized for SARS-CoV-2 infection: A prospective cohort study. Front. Immunol. 2022, 13, 1038227. [Google Scholar] [CrossRef] [PubMed]
- Brunvoll, S.H.; Nygaard, A.B.; Fagerland, M.W.; Holland, P.; Ellingjord-Dale, M.; Dahl, J.A.; Søraas, A. Post-acute symptoms 3-15 months after COVID-19 among unvaccinated and vaccinated individuals with a breakthrough infection. Int. J. Infect. Dis. 2023, 126, 10–13. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | Mild | Moderate | Severe | p |
|---|---|---|---|---|
| N = 19 | N = 68 | N = 34 | ||
| Age at hospital admission (years) | 59.5 (15.3) | 66.3 (11.6) | 63.6 (14.6) | 0.129 |
| Gender male | 12 (63.2) | 46 (67.6) | 22 (64.7) | 0.916 |
| Body mass index (kg/m2) | 25.3 (4.1) | 27.5 (6.0) | 29.4 (6.0) | 0.047 |
| Hospital stay (days) | 8 (6–18) | 14 (10–20) | 23 (16–32) | 0.001 |
| Unit of admission | ||||
| Ward | 19 (100) | 67 (98.5) | 30 (91.2) | 0.205 |
| ICU | 0 (0) | 1 (1.5) | 3 (8.8) | |
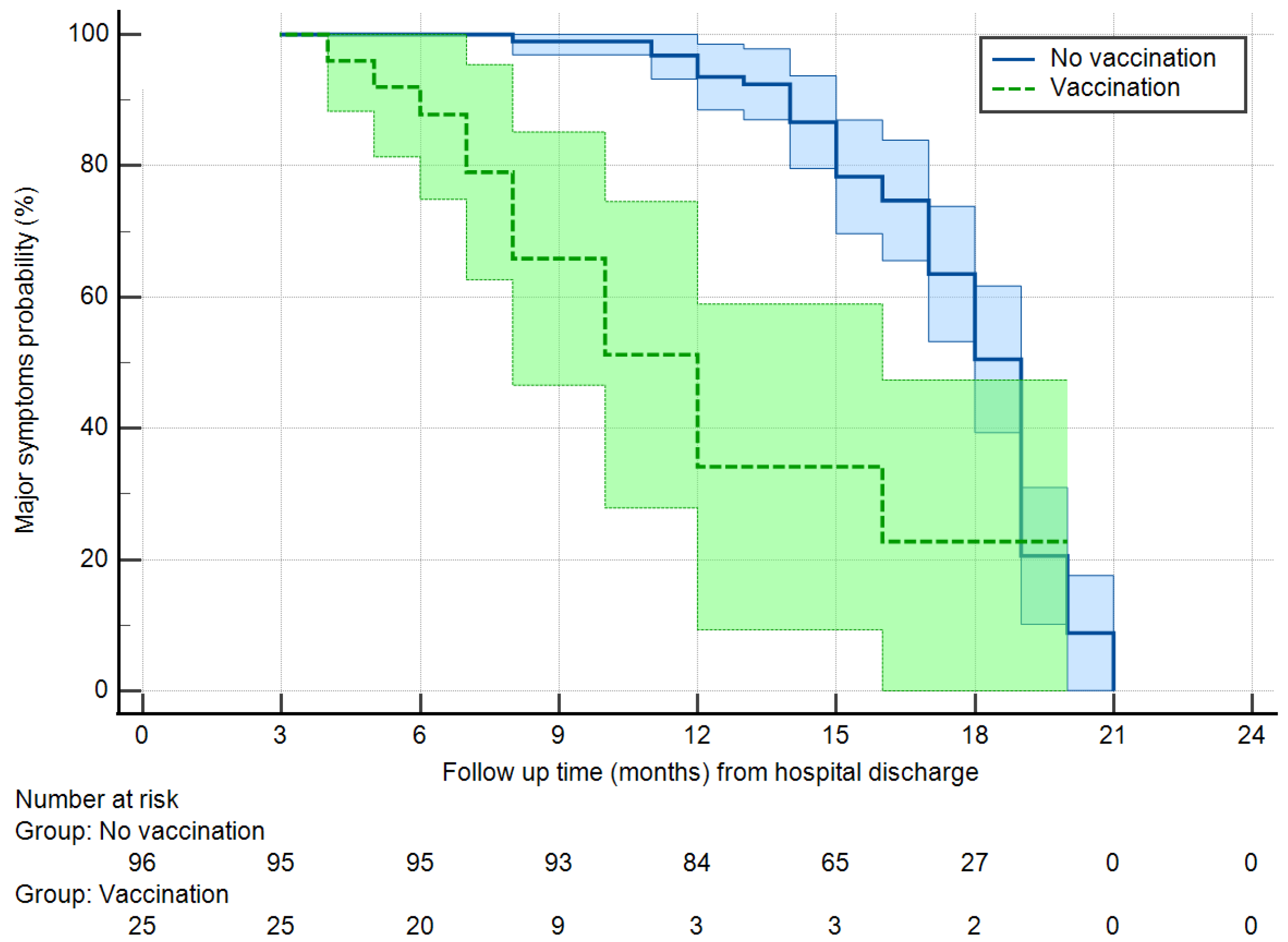
| Vaccination (at least 2 doses) | 7 (36.8) | 14 (19.1) | 4 (11.8) | 0.096 |
| Obesity | 3 (15.8) | 14 (20.6) | 11 (32.4) | 0.294 |
| Arterial hypertension | 5 (26.3) | 32 (47.1) | 18 (52.9) | 0.34 |
| Diabetes | 3 (15.8) | 11 (16.2) | 6 (17.6) | 0.978 |
| Coronaropathy | 2 (10.5) | 15 (22.1) | 3 (8.8) | 0.177 |
| Heart failure | 0 (0) | 7 (10.3) | 2 (5.9) | 0.293 |
| Smoking habit | 0.008 | |||
| No | 11 (58) | 33 (48.5) | 15 (44.1) | |
| Previous | 4 (21.1) | 32 (47) | 19 (56) | |
| Ongoing | 4 (21.1) | 3 (4.4) | 0 (0) | |
| Atrial fibrillation | 0 (0) | 7 (10.3) | 4 (11.8) | 0.315 |
| Active cancer previous 5 years | 5 (26.3) | 5 (7.4) | 1 (2.9) | 0.013 |
| COPD | 2 (10.5) | 3 (4.4) | 1 (2.9) | 0.452 |
| Chronic kidney failure | 0 (0) | 6 (8.8) | 2 (5.9) | 0.384 |
| Previous CVA | 2 (10.5) | 1 (1.5) | 3 (8.8) | 0.13 |
| Anxiety | 3 (15.8) | 9 (13.2) | 7 (20.6) | 0.629 |
| Depression | 3 (15.8) | 6 (8.8) | 5 (14.7) | 0.56 |
| Chronic liver failure | 1 (5.3) | 3 (4.4) | 0 (0) | 0.438 |
| Item | All | Mild | Moderate | Severe | p |
|---|---|---|---|---|---|
| N = 121 | N = 19 | N = 68 | N = 34 | ||
| Follow-up time (months) | 17 (12–18) | 12 (8–17) | 17 (12–18) | 17 (14–19) | 0.011 |
| Symptoms after discharge | 112 (95.6) | 15 (78.9) | 75 (95.6) | 32 (94.1) | 0.046 |
| Major physical symptoms | |||||
| Resolved | 38 (31.4) | 12 (63.2) | 26 (38.2) | 9 (26.5) | |
| Ongoing | 74 (61.2) | 7 (36.8) | 42 (61.8) | 25 (73.5) | 0.031 |
| Work capacity reduced | 39 (32.2) | 4 (21.1) | 21 (30.9) | 14 (41.2) | 0.303 |
| Fever | 5 (4.1) | 3 (15.8) | 2 (2.9) | 0 (0) | 0.016 |
| Resolved | 4 (3.3) | 2 (10.5) | 2 (2.9) | 0 (0) | |
| Ongoing | 1 (0.8) | 1 (5.3) | 0 (0) | 0.348 | |
| Fatigue | 86 (71.1) | 11 (57.9) | 50 (73.5) | 25 (73.5) | 0.386 |
| Resolved | 26 (21.5) | 4 (21.1) | 15 (22.1) | 7 (20.6) | |
| Ongoing | 60 (49.6) | 7 (36.8) | 35 (51.5) | 17 (50) | 0.596 |
| Cough | 29 (24) | 4 (21.1) | 16 (23.5) | 9 (26.5) | 0.911 |
| Resolved | 9 (7.4) | 1 (5.3) | 6 (8.8) | 2 (5.9) | |
| Ongoing | 20 (16.5) | 3 (15.8) | 10 (14.7) | 7 (20.6) | 0.919 |
| Dyspnea | 59 (48.8) | 1 (5.3) | 37 (54.4) | 21 (61.8) | 0.001 |
| Resolved | 8 (6.6) | 0 (0) | 4 (5.9) | 4 (11.8) | |
| Ongoing | 51 (42.1) | 1 (5.3) | 33 (48.5) | 17 (50) | 0.001 |
| Chest pain | 12 (9.9) | 1 (5.3) | 7 (10.3) | 4 (11.8) | 0.845 |
| Resolved | 3 (2.5) | 1 (5.3) | 1 (1.5) | 1 (2.9) | |
| Ongoing | 9 (7.4) | 0 (0) | 6 (8.8) | 3 (8.8) | 0.62 |
| Palpitations | 13 (10.7) | 1 (5.3) | 8 (11.8) | 4 (11.8) | 0.215 |
| Resolved | 2 (1.7) | 0 (0) | 0 (0) | 2 (5.9) | |
| Ongoing | 11 (9.0) | 1 (5.3) | 8 (11.8) | 2 (5.9) | 0.17 |
| Headache | 14 (11.6) | 2 (10.5) | 7 (10.3) | 5 (14.7) | 0.211 |
| Resolved | 2(1.7) | 0 (0) | 2 (2.9) | 0 (0) | |
| Ongoing | 12 (9.9) | 2 (10.5) | 5 (7.4) | 5 (14.7) | 0.582 |
| Major neuropsychological | 58 (47.9) | 7 (36.8) | 35 (51.5) | 16 (47.1) | 0.525 |
| symptoms | |||||
| Resolved | 0 (0) | 2 (5.3) | 2 (2.9) | ||
| Ongoing | 54 (44.6) | 7 (36.8) | 33 (48.5) | 14 (41.2) | 0.592 |
| Anxiety | 26 (21.5) | 3 (15.8) | 16 (23.5) | 7 (20.6) | 0.76 |
| Resolved | 2 (1.7) | 0 (0) | 0 (0) | 2 (5.9) | |
| Ongoing | 24 (19.8) | 3 (15.8) | 16 (23.5) | 5 (14.7) | 0.177 |
| Depression | 24 (19.8) | 2 (10.5) | 14 (20.6) | 8 (23.5) | 0.509 |
| Resolved | 2 (1.7) | 0 (0) | 0 (0) | 2 (0) | |
| Ongoing | 22 (18.1) | 2 (10.5) | 14 (20.6) | 6 (17.6) | 0.183 |
| Sleep disturbances | 36 (29.8) | 3 (15.8) | 22 (32.4) | 11 (32.4) | 0.35 |
| Resolved | 3 (2.5) | 1 (5.3) | 1 (1.5) | 1 (2.9) | |
| Ongoing | 33 (27.3) | 2 (10.5) | 21 (30.9) | 10 (29.4) | 0.425 |
| Memory dysfunction | 46 (38) | 6 (31.6) | 26 (38.2) | 14 (41.2) | 0.787 |
| Resolved | 4 (3.3) | 1 (5.3) | 2 (2.9) | 1 (2.9) | |
| Ongoing | 42 (34.7) | 5 (26.3) | 24 (35.3) | 13 (38.2) | 0.916 |
| Brain fog | 29 (24) | 4 (21.1) | 17 (25) | 8 (23.5) | 0.936 |
| Resolved | 4 (3.3) | 1 (5.3) | 2 (2.9) | 1 (2.9) | |
| Ongoing | 25 (20.6) | 3 (15.8) | 15 (22.1) | 7 (20.6) | 0.966 |
| Paresthesia | 31 (25.6) | 1 (5.3) | 21 (30.9) | 9 (25.5) | 0.077 |
| Resolved | 6 (5.0) | 0 (0) | 3 (4.4) | 3 (8.8) | |
| Ongoing | 26 (20.6) | 1 (5.3) | 18 (26.5) | 5 (14.7) | 0.13 |
| Muscle pain | 39 (32.2) | 6 (31.6) | 22 (32.4) | 11 (32.4) | 0.998 |
| Resolved | 7 (5.8) | 1 (5.3) | 5 (7.4) | 1 (2.9) | |
| Ongoing | 32 (26.5) | 5 (26.3) | 17 (25) | 10 (29.4) | 0.919 |
| Joint pain | 45 (37.2) | 5 (26.3) | 27 (39.7) | 13 (38.2) | 0.559 |
| Resolved | 3 (2.5) | 1 (5.3) | 2 (2.9) | 0 (0) | |
| Ongoing | 42 (34.7) | 4 (21.1) | 25 (36.8) | 13 (38.2) | 0.533 |
| Residual sensory deficit | 48 (39.6) | 3 (15.8) | 30 (44.1) | 15 (44.1) | 0.068 |
| Sight | 19 (15.7) | 1 (5.3) | 8 (11.8)1 | 0 (29.4) | 0.037 |
| Smell | 5 (4.1) | 1 (5.3) | 2 (2.9) | 2 (5.9) | 0.786 |
| Hearing | 12 (9.9) | 1 (5.3) | 10 (14.7) | 1 (2.9) | 0.543 |
| Taste | 12 (9.9) | 0 (0) | 10 (14.7) | 2 (5.9) | 0.653 |
| Age class | <50 | 50–60 | 61–70 | 70–80 | >80 | p |
|---|---|---|---|---|---|---|
| N = 17 | N = 26 | N = 28 | N = 35 | N = 15 | ||
| Vaccination | 4 (23.5) | 5 (19.2) | 5 (17.9) | 5 (14.3) | 6 (40) | 0.338 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ranucci, M.; Baryshnikova, E.; Anguissola, M.; Pugliese, S.; Ranucci, L.; Falco, M.; Menicanti, L. The Very Long COVID: Persistence of Symptoms after 12–18 Months from the Onset of Infection and Hospitalization. J. Clin. Med. 2023, 12, 1915. https://doi.org/10.3390/jcm12051915
Ranucci M, Baryshnikova E, Anguissola M, Pugliese S, Ranucci L, Falco M, Menicanti L. The Very Long COVID: Persistence of Symptoms after 12–18 Months from the Onset of Infection and Hospitalization. Journal of Clinical Medicine. 2023; 12(5):1915. https://doi.org/10.3390/jcm12051915
Chicago/Turabian StyleRanucci, Marco, Ekaterina Baryshnikova, Martina Anguissola, Sara Pugliese, Luca Ranucci, Mara Falco, and Lorenzo Menicanti. 2023. "The Very Long COVID: Persistence of Symptoms after 12–18 Months from the Onset of Infection and Hospitalization" Journal of Clinical Medicine 12, no. 5: 1915. https://doi.org/10.3390/jcm12051915
APA StyleRanucci, M., Baryshnikova, E., Anguissola, M., Pugliese, S., Ranucci, L., Falco, M., & Menicanti, L. (2023). The Very Long COVID: Persistence of Symptoms after 12–18 Months from the Onset of Infection and Hospitalization. Journal of Clinical Medicine, 12(5), 1915. https://doi.org/10.3390/jcm12051915