
What Should Be the Focus of Treatment When Insomnia Disorder Is Comorbid with Depression or Anxiety Disorder?


 , ,
, ,  and
and
Abstract
:1. Introduction
- A national survey, consisting of seven statements regarding clinically related insomnia topics and including our focus statement, to understand current U.S. physician perspectives regarding insomnia treatments.
- A review of the current literature related to the treatment of insomnia where comorbid anxiety and depression are present.
- A meeting of the expert panel in their role as insomnia experts to assess the evidence, the strength of the literature presented and its implications for insomnia treatment and to identify clinical research that will enable improved outcomes.
2. Materials and Methods
2.1. National Survey
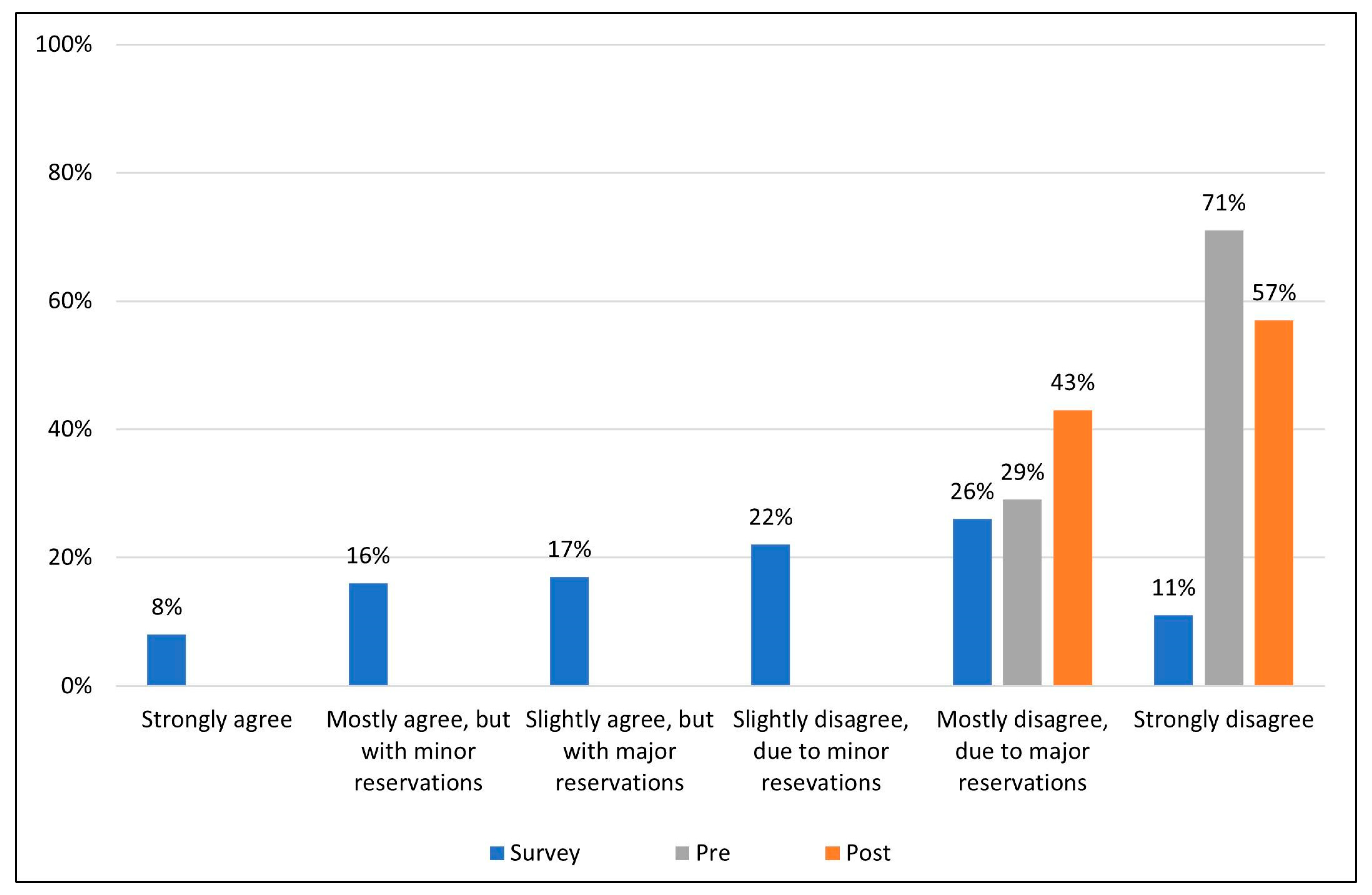
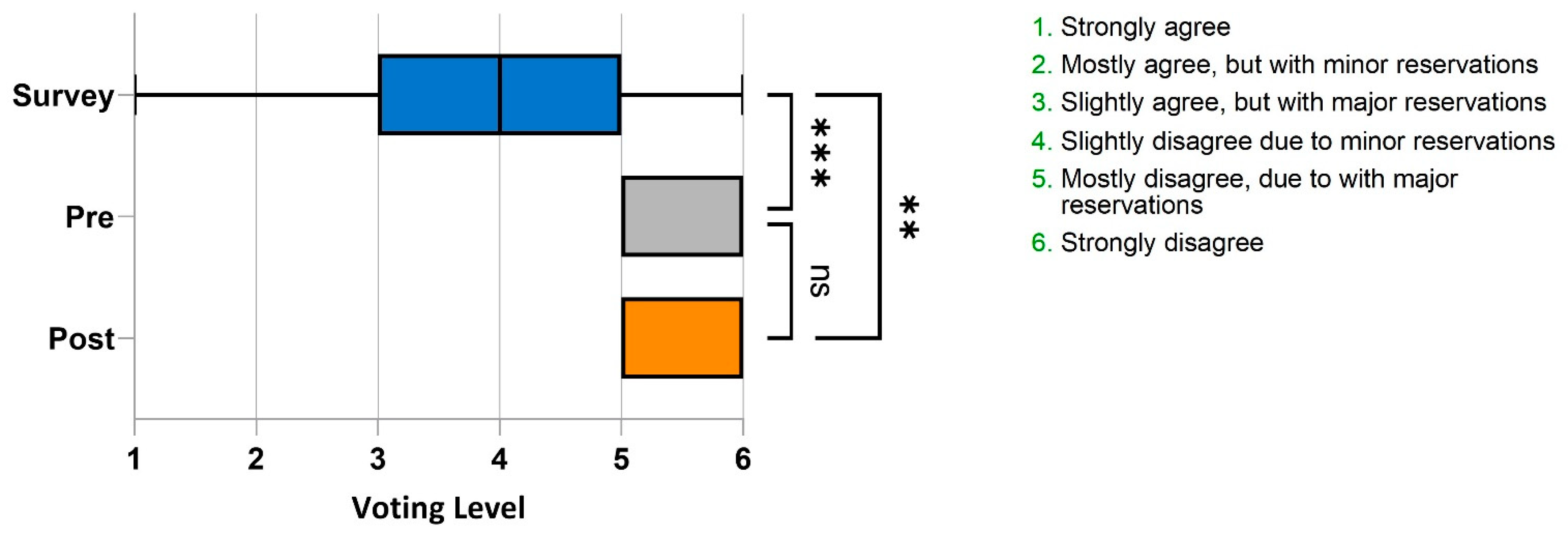
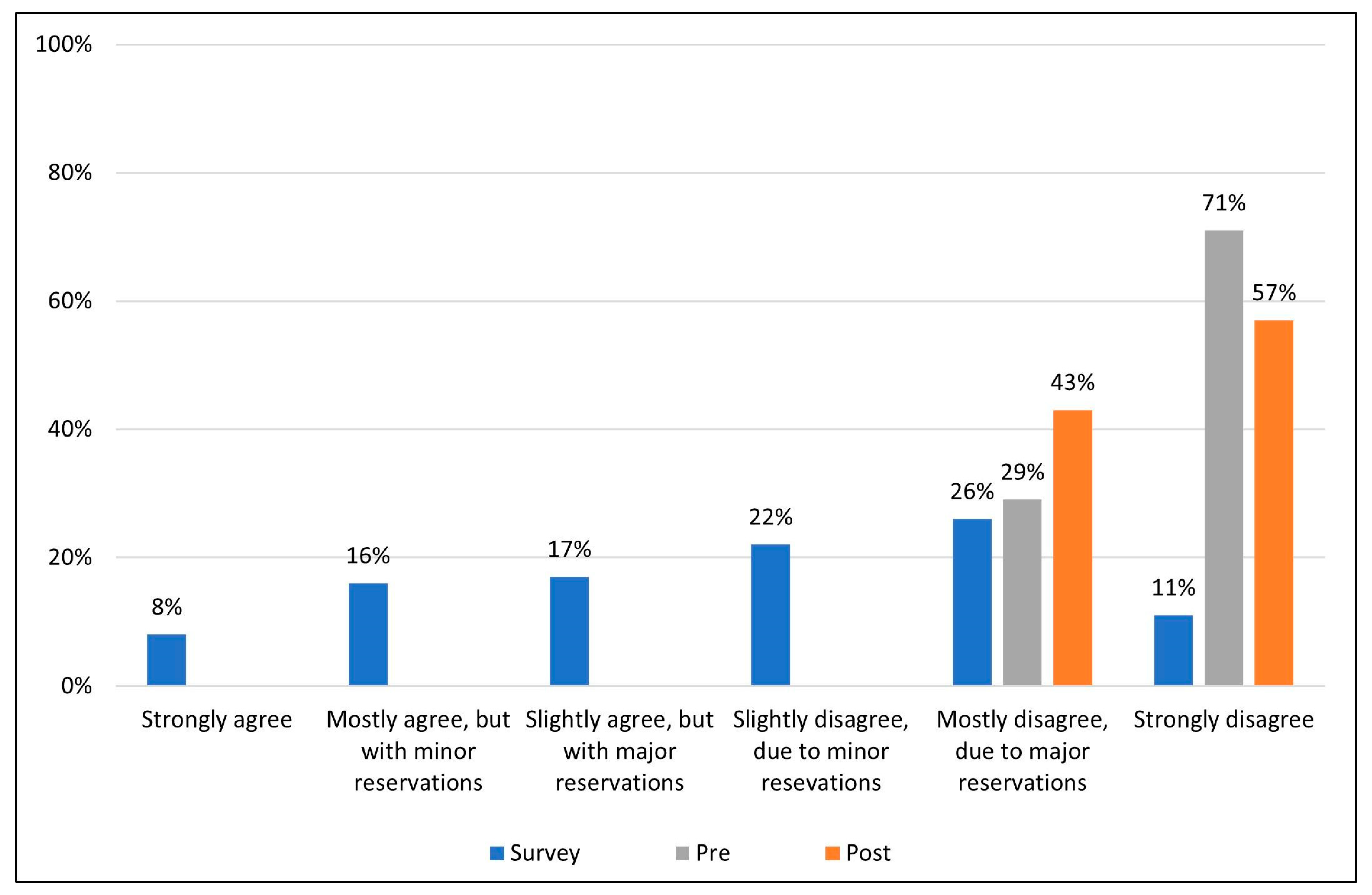
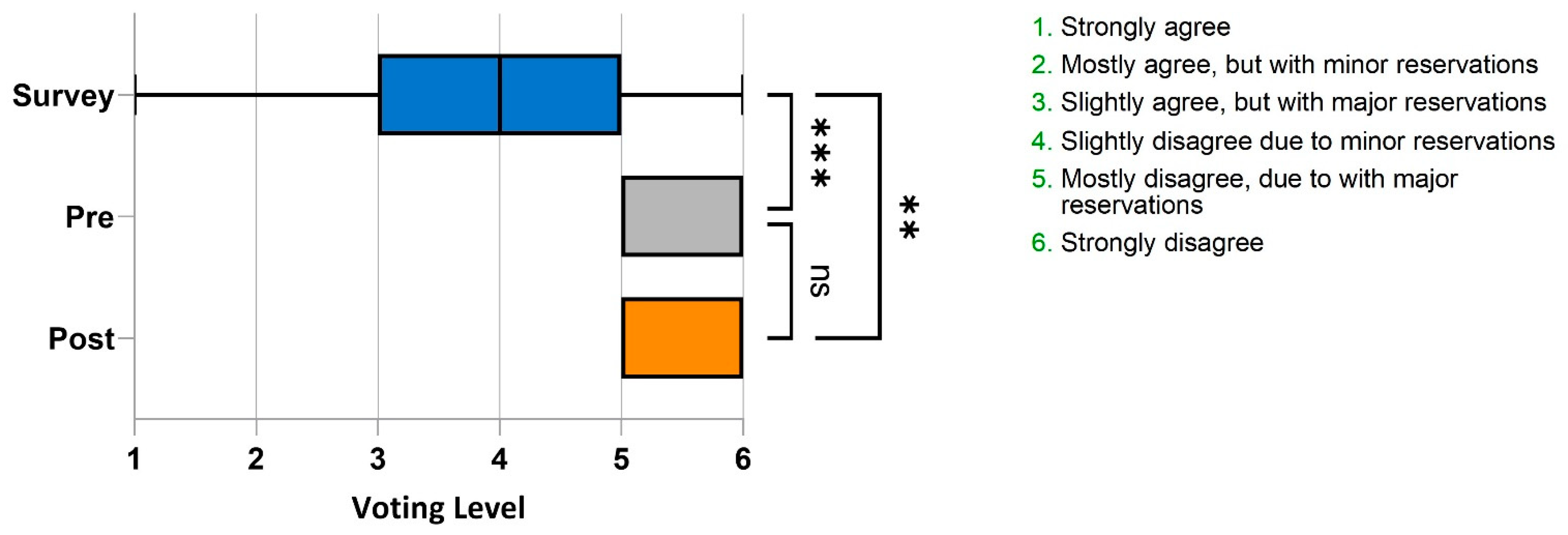
- Strongly agree.
- Mostly agree, but with minor reservations.
- Slightly agree, but with major reservations.
- Slightly disagree, due to minor reservations.
- Mostly disagree, due to major reservations.
- Strongly disagree.
2.2. Expert Panel and Literature Review
2.3. Nature of the Evidence
- Evidence obtained from meta-analysis, including at least one large, randomized controlled trial (RCT).
- Evidence obtained from either meta-analysis, including at least one small RCT, or from at least one well-designed large RCT.
- Evidence obtained from well-designed cohort or case–control studies.
- Evidence obtained from case series, case reports, or flawed clinical trials.
- Opinions of respected authorities based on clinical experience, descriptive studies, or reports of expert committees.
- Insufficient evidence to form an opinion.
3. Results
3.1. Survey Results
3.2. Literature Review
3.3. Quality and Impact of Evidence
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. DSM-5 Task Force, 5th ed.; American Psychiatric Publishing, Inc.: Arlington, VA, USA, 2013; pp. 1–991. [Google Scholar] [CrossRef]
- Morin, C.M.; Jarrin, D.C. Epidemiology of Insomnia: Prevalence, Course, Risk Factors, and Public Health Burden. Sleep Med. Clin. 2022, 17, 173–191. [Google Scholar] [CrossRef] [PubMed]
- Morin, C.M.; Edinger, J.D.; Beaulieu-Bonneau, S.; Ivers, H.; Krystal, A.D.; Guay, B.; Bélanger, L.; Cartwright, A.; Simmons, B.; Lamy, M.; et al. Effectiveness of Sequential Psychological and Medication Therapies for Insomnia Disorder: A Randomized Clinical Trial. JAMA Psychiatry 2020, 77, 1107–1115. [Google Scholar] [CrossRef] [PubMed]
- Kyle, S.D.; Morgan, K.; Espie, C.A. Insomnia and health-related quality of life. Sleep Med. Rev. 2010, 14, 69–82. [Google Scholar] [CrossRef] [PubMed]
- Baglioni, C.; Battagliese, G.; Feige, B.; Spiegelhalder, K.; Nissen, C.; Voderholzer, U.; Lombardo, C.; Riemann, D. Insomnia as a predictor of depression: A meta-analytic evaluation of longitudinal epidemiological studies. J. Affect. Disord. 2011, 135, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Breslau, N.; Roth, T.; Rosenthal, L.; Andreski, P. Sleep disturbance and psychiatric disorders: A longitudinal epidemiological study of young adults. Biol. Psychiatry 1996, 39, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Hertenstein, E.; Feige, B.; Gmeiner, T.; Kienzler, C.; Spiegelhalder, K.; Johann, A.; Jansson-Fröjmark, M.; Palagini, L.; Rücker, G.; Riemann, D.; et al. Insomnia as a predictor of mental disorders: A systematic review and meta-analysis. Sleep Med. Rev. 2019, 43, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Roth, T.; Jaeger, S.; Jin, R.; Kalsekar, A.; Stang, P.E.; Kessler, R.C. Sleep problems, comorbid mental disorders, and role functioning in the national comorbidity survey replication. Biol. Psychiatry 2006, 60, 1364–1371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institutes of Health. National Institutes of Health State of the Science Conference statement on Manifestations and Management of Chronic Insomnia in Adults, 13–15 June 2005. Sleep 2005, 28, 1049–1057. [Google Scholar] [CrossRef] [Green Version]
- American Psychiatric Association. DSM-3 Task Force, 3rd ed.; American Psychiatric Publishing, Inc.: Arlington, VA, USA, 1980; pp. 1–567. ISBN 0890420181. [Google Scholar]
- American Psychiatric Association. DSM-4 Task Force, 4th ed.; American Psychiatric Publishing, Inc.: Arlington, VA, USA, 1994; pp. 1–943. ISBN 0890420254. [Google Scholar]
- Ohayon, M.M.; Roth, T. Place of chronic insomnia in the course of depressive and anxiety disorders. J. Psychiatr. Res. 2003, 37, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Ohayon, M.M.; Riemann, D.; Morin, C.; Reynolds, C.F., 3rd. Hierarchy of insomnia criteria based on daytime consequences. Sleep Med. 2012, 13, 52–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Academy of Sleep Medicine. The International Classification of Sleep Disorders, 3rd ed.; (ICSD-3); American Academy of Sleep Medicine: Darien, IL, USA, 2014; ISBN 0965722023. [Google Scholar]
- Belleville, G.; Ivers, H.; Bélanger, L.; Blais, F.C.; Morin, C.M. Sequential Treatment of Comorbid Insomnia and Generalized Anxiety Disorder. J. Clin. Psychol. 2016, 72, 880–896. [Google Scholar] [CrossRef] [PubMed]
- Carney, C.E.; Edinger, J.D.; Kuchibhatla, M.; Lachowski, A.M.; Bogouslavsky, O.; Krystal, A.D.; Shapiro, C.M. Cognitive Behavioral Insomnia Therapy for Those with Insomnia and Depression: A Randomized Controlled Clinical Trial. Sleep 2017, 40, zsx019. [Google Scholar] [CrossRef] [PubMed]
- Manber, R.; Edinger, J.D.; Gress, J.L.; San Pedro-Salcedo, M.G.; Kuo, T.F.; Kalista, T. Cognitive behavioral therapy for insomnia enhances depression outcome in patients with comorbid major depressive disorder and insomnia. Sleep 2008, 4, 489–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blom, K.; Susanna Jernelöv, S.; Rück, C.; Lindefors, N.; Kaldo, V. Three-Year Follow-Up Comparing Cognitive Behavioral Therapy for Depression to Cognitive Behavioral Therapy for Insomnia, for Patients with Both Diagnoses. Sleep 2017, 40, zsx108. [Google Scholar] [CrossRef] [Green Version]
- Edinger, J.D.; Arnedt, J.T.; Bertisch, S.M.; Carney, C.E.; Harrington, J.J.; Lichstein, K.L.; Sateia, M.J.; Troxel, W.M.; Zhou, E.S.; Kazmi, U.; et al. Behavioral and psychological treatments for chronic insomnia disorder in adults: An American Academy of Sleep Medicine systematic review, meta-analysis, and GRADE assessment. J. Clin. Sleep Med. 2021, 17, 263–298. [Google Scholar] [CrossRef]
- Fava, M.; McCall, W.V.; Krystal, A.; Wessel, T.; Rubens, R.; Caron, J.; Amato, D.; Roth, T. Eszopiclone co-administered with fluoxetine in patients with insomnia coexisting with major depressive disorder. Biol. Psychiatry 2006, 11, 1052–1060. [Google Scholar] [CrossRef]
- Fava, M.; Asnis, G.M.; Shrivastava, R.; Lydiard, B.; Bastani, B.; Sheehan, D.V.; Roth, T. Improved insomnia symptoms and sleep-related next-day functioning in patients with comorbid major depressive disorder and insomnia following concomitant zolpidem extended-release 12.5 mg and escitalopram treatment: A randomized controlled trial. J. Clin. Psychopharmacol. 2011, 7, 914–928. [Google Scholar] [CrossRef]
- Fava, M.; Asnis, G.M.; Shrivastava, R.; Lydiard, B.; Bastani, B.; Sheehan, D.; Roth, T. Zolpidem extended-release improves sleep and next-day symptoms in comorbid insomnia and generalized anxiety disorder. J. Clin. Psychopharmacol. 2009, 29, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Nierenberg, A.A.; Husain, M.M.; Trivedi, M.H.; Fava, M.; Warden, D.; Wisniewski, S.R. Residual symptoms after remission of major depressive disorder with citalopram and risk of relapse: A STAR*D report. Psychol. Med. 2010, 40, 41–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perlis, M.L.; Giles, D.E.; Buysse, D.J.; Tu, X.; Kupfer, D.J. Self-reported sleep disturbance as a prodromal symptom in recurrent depression. J. Affect. Disord. 1997, 42, 209–212. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Keywords | Limits | Abstracts Reviewed | Exclusion Criteria | Publications Selected for Presentation |
|---|---|---|---|---|
| “Insomnia comorbidities AND depression” | date limits set for inclusion from 2011–2021 and limited to clinical trials or randomized control trials | 87 | Observational study, low participant number, no control group, or involved an insomnia medication without FDA approved indication for treatment for insomnia | 5 |
| “Insomnia comorbidities AND anxiety” | date limits set for inclusion from 2011–2021 and limited to clinical trials or randomized control trials | 53 | Observational study, low participant number, no control group, or involved an insomnia medication without FDA approved indication for treatment for insomnia | 3 |
| “Insomnia comorbidities AND depression” | date limits set for inclusion from 2011–2021 and limited to meta-analysis | 23 | Observational study, low participant number, no control group, or involved an insomnia medication without FDA approved indication for treatment for insomnia | 1 |
| “Insomnia comorbidities AND anxiety” | date limits set for inclusion from 2011–2021 and limited to meta-analysis | 18 | Observational study, low participant number, no control group, or involved an insomnia medication without FDA approved indication for treatment for insomnia | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morin, C.M.; Bertisch, S.M.; Pelayo, R.; Watson, N.F.; Winkelman, J.W.; Zee, P.C.; Krystal, A.D. What Should Be the Focus of Treatment When Insomnia Disorder Is Comorbid with Depression or Anxiety Disorder? J. Clin. Med. 2023, 12, 1975. https://doi.org/10.3390/jcm12051975
Morin CM, Bertisch SM, Pelayo R, Watson NF, Winkelman JW, Zee PC, Krystal AD. What Should Be the Focus of Treatment When Insomnia Disorder Is Comorbid with Depression or Anxiety Disorder? Journal of Clinical Medicine. 2023; 12(5):1975. https://doi.org/10.3390/jcm12051975
Chicago/Turabian StyleMorin, Charles M., Suzanne M. Bertisch, Rafael Pelayo, Nathaniel F. Watson, John W. Winkelman, Phyllis C. Zee, and Andrew D. Krystal. 2023. "What Should Be the Focus of Treatment When Insomnia Disorder Is Comorbid with Depression or Anxiety Disorder?" Journal of Clinical Medicine 12, no. 5: 1975. https://doi.org/10.3390/jcm12051975
APA StyleMorin, C. M., Bertisch, S. M., Pelayo, R., Watson, N. F., Winkelman, J. W., Zee, P. C., & Krystal, A. D. (2023). What Should Be the Focus of Treatment When Insomnia Disorder Is Comorbid with Depression or Anxiety Disorder? Journal of Clinical Medicine, 12(5), 1975. https://doi.org/10.3390/jcm12051975