


Epidemiological and Immune Profile Analysis of Italian Subjects with Endometriosis and Multiple Sclerosis

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
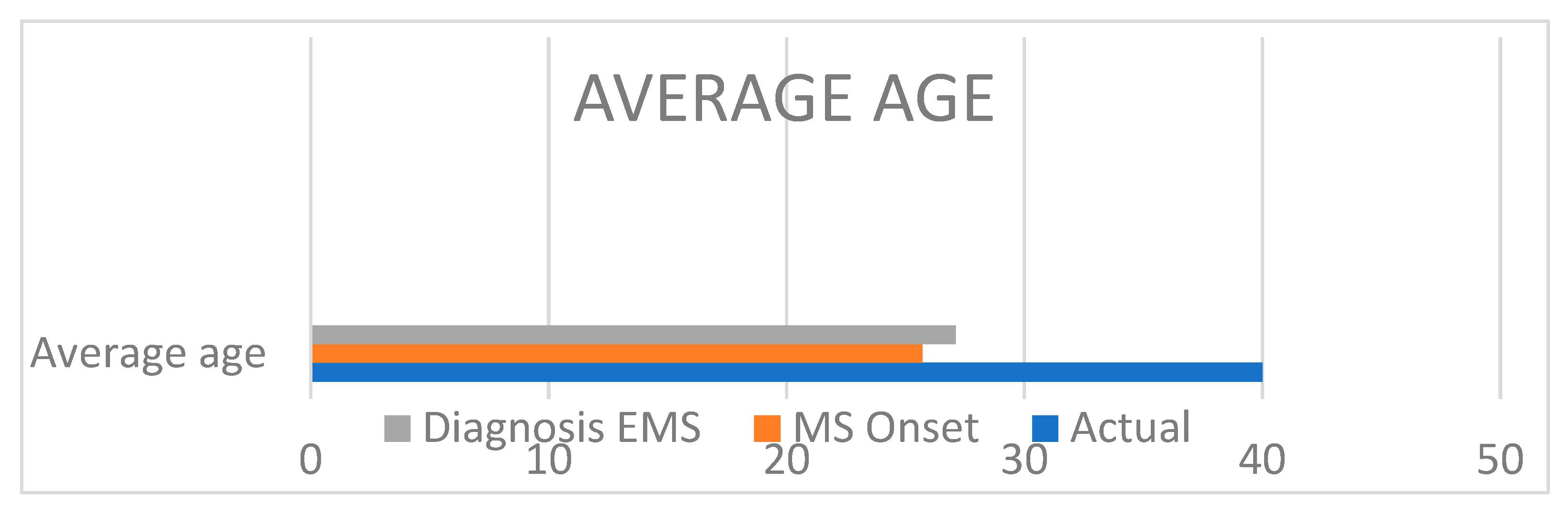
3.1. Epidemiological Analysis
3.2. Clinical Evaluation
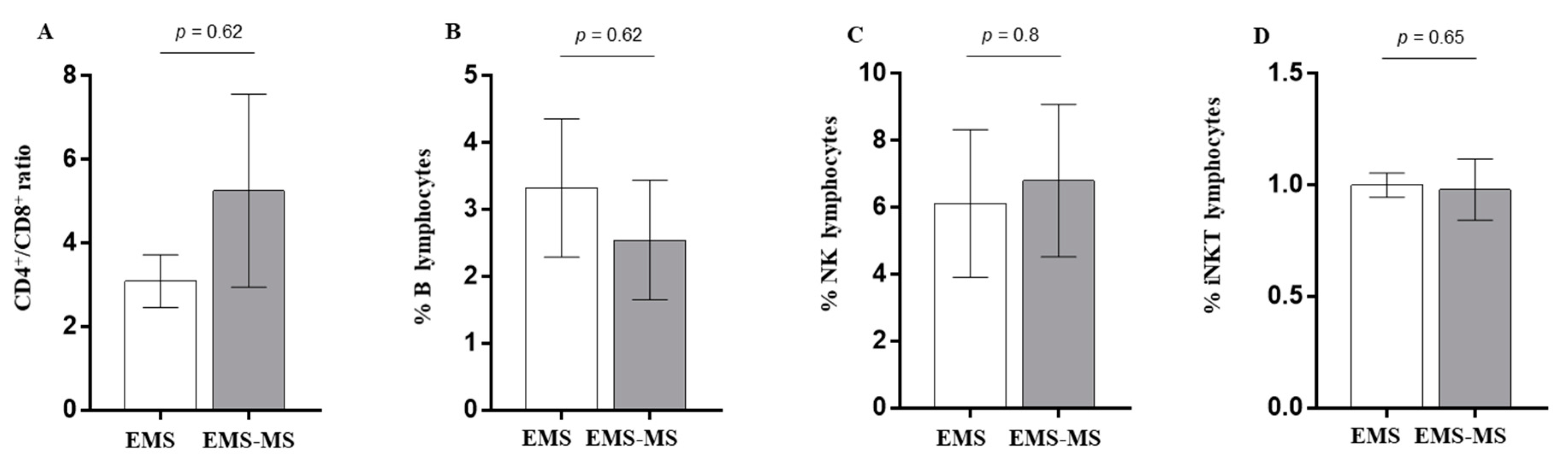
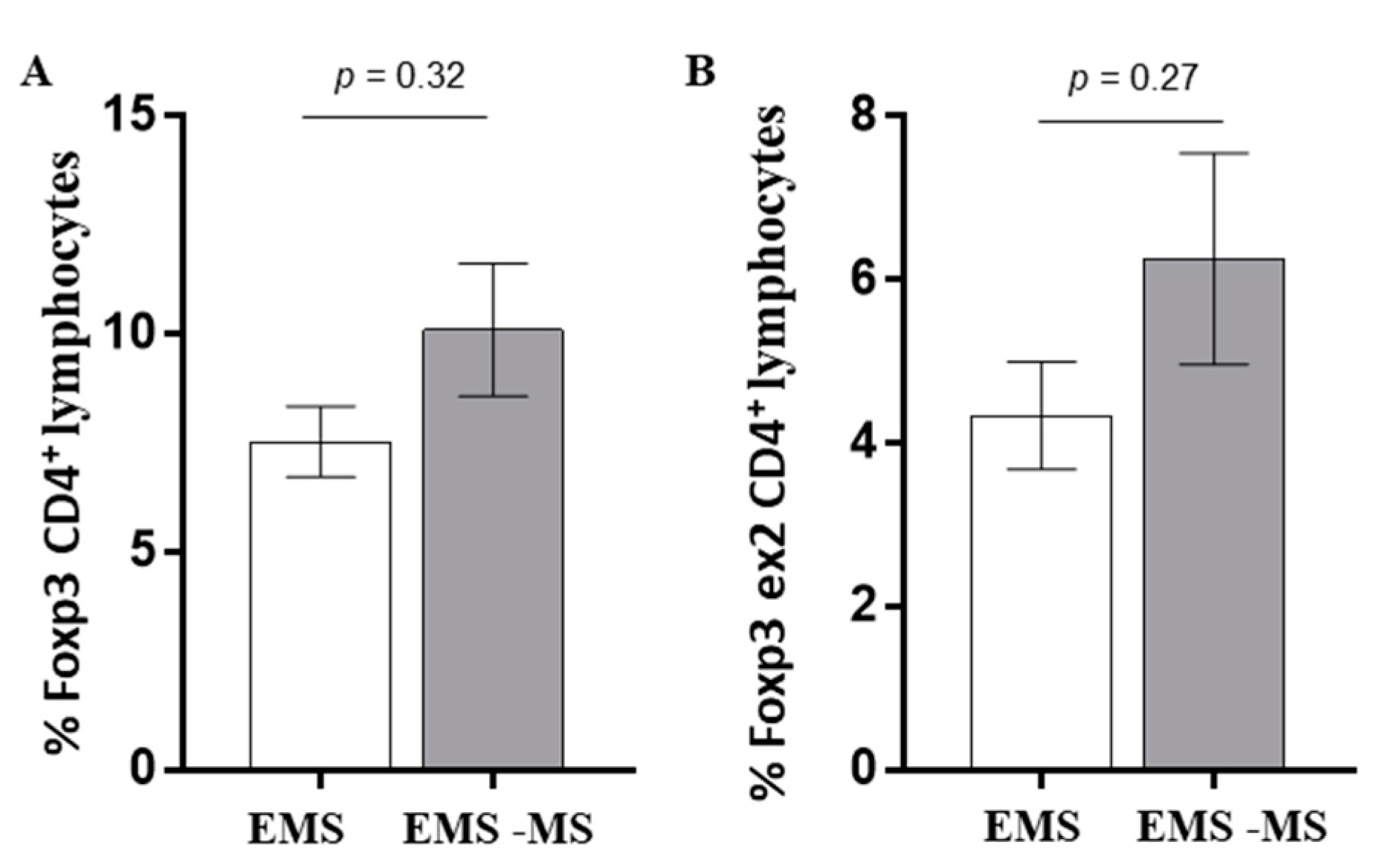
3.3. Immunological Pattern
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Saunders, P.T.K.; Horne, A.W. Endometriosis: Etiology, pathobiology, and therapeutic prospects. Cell 2021, 184, 2807–2824. [Google Scholar] [CrossRef]
- Taylor, H.S.; Kotlyar, A.M.; Flores, V.A. Endometriosis is a chronic systemic disease: Clinical challenges and novel innovations. Lancet 2021, 397, 839–852. [Google Scholar] [CrossRef] [PubMed]
- Gleicher, N.; el-Roeiy, A.; Confino, E.; Friberg, J. Is endometriosis an autoimmune disease? Obstet. Gynecol. 1987, 70, 115–122. [Google Scholar] [CrossRef]
- Maksym, R.B.; Hoffmann-Młodzianowska, M.; Skibińska, M.; Rabijewski, M.; Mackiewicz, A.; Kieda, C. Immunology and Immunotherapy of Endometriosis. J. Clin. Med. 2021, 10, 5879. [Google Scholar] [CrossRef]
- Jiang, L.; Yan, Y.; Liu, Z.; Wang, Y. Inflammation and endometriosis. Front. Biosci. Landmark Ed. 2016, 21, 941–948. [Google Scholar] [CrossRef] [PubMed]
- Shigesi, N.; Kvaskoff, M.; Kirtley, S.; Feng, Q.; Fang, H.; Knight, J.C.; Missmer, S.A.; Rahmioglu, N.; Zondervan, K.T.; Becker, C.M. The association between endometriosis and autoimmune diseases: A systematic review and meta-analysis. Hum. Reprod. Update 2019, 25, 486–503. [Google Scholar] [CrossRef]
- Sinaii, N.; Cleary, S.D.; Ballweg, M.L.; Nieman, L.K.; Stratton, P. High rates of autoimmune and endocrine disorders, fibromyalgia, chronic fatigue syndrome and atopic diseases among women with endometriosis: A survey analysis. Hum. Reprod. 2002, 17, 2715–2724. [Google Scholar] [CrossRef]
- Nielsen, N.M.; Jørgensen, K.T.; Pedersen, B.V.; Rostgaard, K.; Frisch, M. The co-occurrence of endometriosis with multiple sclerosis, systemic lupus erythematosus and Sjogren syndrome. Hum. Reprod. 2011, 26, 1555–1559. [Google Scholar] [CrossRef] [PubMed]
- Katiyar, A.; Sharma, S.; Singh, T.P.; Kaur, P. Identification of Shared Molecular Signatures Indicate the Susceptibility of Endometriosis to Multiple Sclerosis. Front. Genet. 2018, 9, 42. [Google Scholar] [CrossRef]
- Zhang, T.; De Carolis, C.; Man, G.C.W.; Wang, C.C. The link between immunity, autoimmunity and endometriosis: A literature update. Autoimmun. Rev. 2018, 17, 945–955. [Google Scholar] [CrossRef]
- Eisenberg, V.H.; Zolti, M.; Soriano, D. Is there an association between autoimmunity and endometriosis? Autoimmun. Rev. 2012, 11, 806–814. [Google Scholar] [CrossRef]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Lee, S.Y.; Koo, Y.J.; Lee, D.H. Classification of endometriosis. Yeungnam Univ. J. Med. 2021, 38, 10–18. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Atlas Multiple Sclerosis Resources in the World 2008; World Health Organization: Geneva, Switzerland, 2008; pp. 14–15. ISBN 9789241563758. Available online: https://apps.who.int/iris/bitstream/handle/10665/43968/9789241563758_eng.pdf (accessed on 25 February 2023).
- Nociti, V.; Romozzi, M. Multiple Sclerosis and Autoimmune Comorbidities. J. Pers. Med. 2022, 12, 1828. [Google Scholar] [CrossRef] [PubMed]
- Alviggi, C.; Carrieri, P.B.; Pivonello, R.; Scarano, V.; Pezzella, M.; De Placido, G.; Colao, A.; Matarese, G. Association of pelvic endometriosis with alopecia universalis, autoimmune thyroiditis and multiple sclerosis. J. Endocrinol. Investig. 2006, 29, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Izumi, G.; Koga, K.; Takamura, M.; Makabe, T.; Satake, E.; Takeuchi, A.; Taguchi, A.; Urata, Y.; Fujii, T.; Osuga, Y. Involvement of immune cells in the pathogenesis of endometriosis. J. Obstet. Gynaecol. Res. 2018, 44, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Witz, C.A.; Montoya, I.A.; Dey, T.D.; Schenken, R.S. Characterization of lymphocyte subpopulations and T cell activation in endometriosis. Am. J. Reprod. Immunol. 1994, 32, 173–179. [Google Scholar] [CrossRef]
- Sospedra, M.; Martin, R. Immunology of multiple sclerosis. Annu. Rev. Immunol. 2005, 23, 683–747. [Google Scholar] [CrossRef]
- Drossman, D.A.; Thompson, W.G. The irritable bowel syndrome: Review and a graduated multicomponent treatment approach. Ann. Intern. Med. 1992, 116 Pt 1, 1009–1016. [Google Scholar] [CrossRef]
- Shafrir, A.L.; Farland, L.V.; Shah, D.K.; Harris, H.R.; Kvaskoff, M.; Zondervan, K.; Missmer, S.A. Risk for and consequences of endometriosis: A critical epidemiologic review. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 51, 1–15. [Google Scholar] [CrossRef]
- Horne, A.W.; Missmer, S.A. Pathophysiology, diagnosis, and management of endometriosis. BMJ 2022, 379, e070750. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Actual Age | Age at Diagnosis | Bmi | Dysmenorrhea | Menses | Stage (afs) | Surgery | Therapy | Pregnancy |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 40 | 20 | 26 | YES | Regular | 3 | NO | Dienogest (2019) | ND |
| 2 | 32 | 23 | 24 | NO | Regular | 4 | YES | NO | NO |
| 3 | 30 | 18 | 25 | NO | Regular | 4 | NO | Dienogest (2019) | YES |
| 4 | 36 | 20 | 26 | YES | Regular | 3 | NO | NO | YES |
| 5 | 42 | 25 | 27 | YES | Regular | 3 | NO | NO | NO |
| 6 | 40 | 22 | 24 | NO | Regular | 3 | NO | NO | ND |
| 7 | 39 | 34 | 26 | NO | Regular | 3 | NO | NO | ND |
| 8 | 42 | 35 | 25 | YES | Regular | 4 | NO | NO | ND |
| Patient | Actual Age | BMI | Pregnancy |
|---|---|---|---|
| 1 | 43 | 27 | ND |
| 2 | 28 | 26 | YES |
| 3 | 28 | 28 | ND |
| 4 | 46 | 26 | YES |
| 5 | 36 | 28 | YES |
| 6 | 48 | 25 | ND |
| 7 | 47 | 26 | ND |
| 8 | 42 | 25 | ND |
| 9 | 35 | 26 | YES |
| Patient | Age at Diagnosis | Dysmenorrhea | Pain (Nrs Scale) | Menses | Usg | Stage (afs) | Surgery | Therapy |
|---|---|---|---|---|---|---|---|---|
| 1 | 28 | YES | 3 | Regular | Endometrioma | 3 | NO | NO |
| 2 | 22 | YES | 3 | Regular | Endometrioma | 3 | NO | NO |
| 3 | 20 | YES | 4 | Regular | Endometrioma | 3 | NO | Dienogest (2016–2018) |
| 4 | 27 | YES | 3 | Regular | Endometrioma | 3 | NO | NO |
| 5 | 21 | NO | 0 | Regular | Endometrioma | 3 | NO | NO |
| 6 | 35 | NO | 0 | Oligomenorrhea | Endometrioma | 3 | NO | NO |
| 7 | 42 | NO | 0 | Regular | Retrocervical Nodule | 4 | NO | NO |
| 8 | 30 | NO | 0 | Regular | Endometrioma+ Lus Nodule | 4 | NO | NO |
| 9 | 19 | YES | 3 | Oligomenorrhea | Endometrioma+ Lus Nodule | 4 | NO | NO |
| Patient | Onset Age | Edss | Type | Therapy |
|---|---|---|---|---|
| 1 | 27 | 4.5 | RR | Ocrelizumab |
| 2 | 24 | 3.5 | RR | Natalizumab |
| 3 | 21 | 1.5 | RR | Fingolimod |
| 4 | 25 | 2.5 | RR | Interferon Beta |
| 5 | 23 | 3 | RR | Glatiramer |
| 6 | 31 | 2 | RR | Glatiramer |
| 7 | 23 | 6 | RR | Dimethyl Fumarate |
| 8 | 26 | 2.5 | RR | Glatiramer |
| 9 | 32 | 1.5 | RR | Glatiramer |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zizolfi, B.; Foreste, V.; Bonavita, S.; Rubino, V.; Ruggiero, G.; Brescia Morra, V.; Lanzillo, R.; Carotenuto, A.; Boscia, F.; Taglialatela, M.; et al. Epidemiological and Immune Profile Analysis of Italian Subjects with Endometriosis and Multiple Sclerosis. J. Clin. Med. 2023, 12, 2043. https://doi.org/10.3390/jcm12052043
Zizolfi B, Foreste V, Bonavita S, Rubino V, Ruggiero G, Brescia Morra V, Lanzillo R, Carotenuto A, Boscia F, Taglialatela M, et al. Epidemiological and Immune Profile Analysis of Italian Subjects with Endometriosis and Multiple Sclerosis. Journal of Clinical Medicine. 2023; 12(5):2043. https://doi.org/10.3390/jcm12052043
Chicago/Turabian StyleZizolfi, Brunella, Virginia Foreste, Simona Bonavita, Valentina Rubino, Giuseppina Ruggiero, Vincenzo Brescia Morra, Roberta Lanzillo, Antonio Carotenuto, Francesca Boscia, Maurizio Taglialatela, and et al. 2023. "Epidemiological and Immune Profile Analysis of Italian Subjects with Endometriosis and Multiple Sclerosis" Journal of Clinical Medicine 12, no. 5: 2043. https://doi.org/10.3390/jcm12052043
APA StyleZizolfi, B., Foreste, V., Bonavita, S., Rubino, V., Ruggiero, G., Brescia Morra, V., Lanzillo, R., Carotenuto, A., Boscia, F., Taglialatela, M., & Guida, M. (2023). Epidemiological and Immune Profile Analysis of Italian Subjects with Endometriosis and Multiple Sclerosis. Journal of Clinical Medicine, 12(5), 2043. https://doi.org/10.3390/jcm12052043