
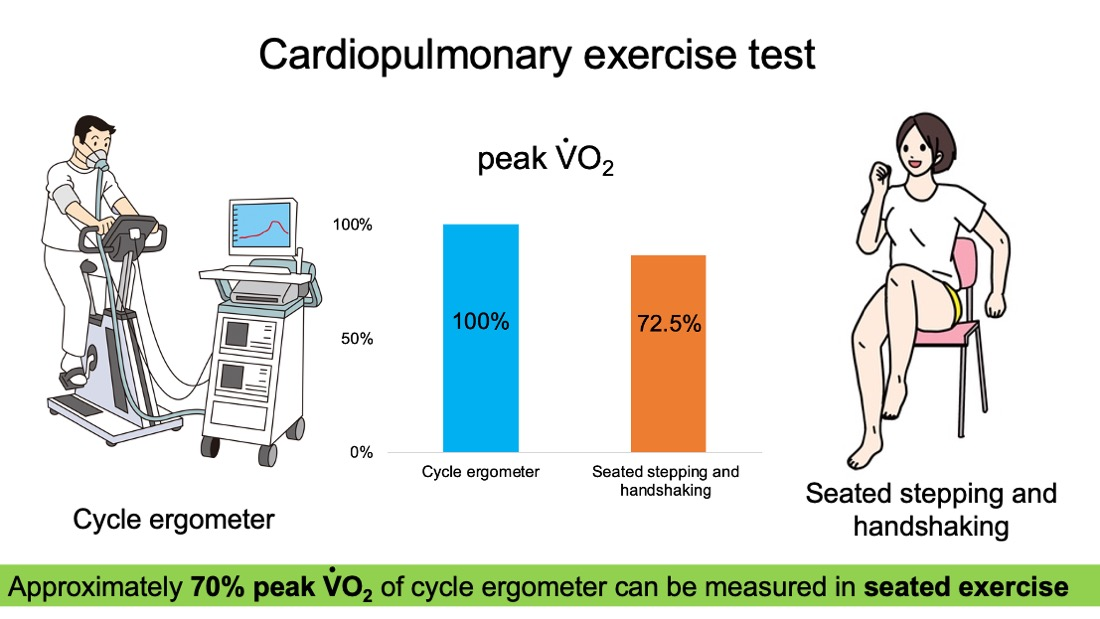
Feasibility of Seated Stepping and Handshaking as a Cardiopulmonary Exercise Testing: A Pilot Study
 , , ,
, , ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. CE-CPX
2.2. SHS-CPX
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kohzuki, M.; Sakata, T.; Kawamura, T. A paradigm shift in rehabilitation medicine: From “adding life to years” to “adding life to years and years to life”. Asian J. Hum. Serv. 2012, 2, 1–7. [Google Scholar]
- Johnson, M.; Meltz, K.; Hart, K.; Schmudlach, M.; Clarkson, L.; Bormzn, K. Validity of the Actical activity monitor for assessing steps and energy expenditure during walking. J. Sports Sci. 2015, 33, 769–776. [Google Scholar] [CrossRef] [PubMed]
- Kodama, S.; Saito, K.; Tanaka, S.; Maki, M.; Yachi, Y.; Asumi, M.; Sugawara, A.; Totsuka, K.; Shimano, H.; Ohashi, Y.; et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: A meta-analysis. JAMA 2009, 301, 2024–2035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beekley, M.D.; Brechue, W.F.; DeHoyos, D.V.; Garzarella, L.; Werber-Zion, G.; Pollock, M. Cross-validation of the YMCA submaximal cycle ergometer test to predict VO2max. Res. Q. Exerc. Sport. 2004, 75, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Billinger, S.A.; Loudon, J.K.; Gajewski, B.J. Validity of a total body recumbent stepper exercise test to assess cardiorespiratory fitness. J. Strength Cond. Res. 2008, 22, 1556–1562. [Google Scholar] [CrossRef] [PubMed]
- Noonan, V.; Dean, E. Submaximal exercise testing: Clinical application and interpretation. Phys. Ther. 2000, 80, 782–807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Billinger, S.A.; Tseng, B.Y.; Kluding, P.M. Modified total-body recumbent stepper exercise test for assessing peak oxygen consumption in people with chronic stroke. Phys. Ther. 2008, 88, 1188–1195. [Google Scholar] [CrossRef] [PubMed]
- Herda, A.A.; Lentz, A.A.; Mattlage, A.E.; Sisante, J.F.; Billinger, S.A. Cross-validation of the recumbent stepper submaximal exercise test to predict peak oxygen uptake in older adults. Phys. Ther. 2014, 94, 722–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heyward, V.; Gibson, A. Advanced Fitness Assessment and Exercise Prescription, 7th ed.; Human Kinetics Inc.: Champaign, IL, USA, 2013; pp. 99–119. [Google Scholar]
- Nakamura, K.; Ohira, M.; Yokokawa, Y.; Nagasawa, Y. Validity and reproducibility of an incremental sit-to-stand exercise test for evaluating anaerobic threshold in young, healthy individuals. J. Sports Sci. Med. 2015, 14, 708–715. [Google Scholar] [PubMed]
- Fiems, C.L.; Bales, M.; Ganley, S.; Michel, D.; Rice, K.; Silverman, K. Reliability of a recumbent stepper submaximal exercise test after traumatic brain injury. Phys. Theory Pract. 2022, 38, 2896–2904. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Zhan, L.; Sun, S.; Peng, W.; Sun, Y. Validity of a newly-designed rectilinear stepping ergometer submaximal exercise test to assess cardiorespiratory fitness. J. Sports Sci. Med. 2017, 16, 357–364. [Google Scholar] [PubMed]
- Bennett, H.; Parfitt, G.; Davison, K.; Eston, R. Validity of submaximal step tests to estimate maximal oxygen uptake in healthy adults. Sports Med. 2016, 46, 737–750. [Google Scholar] [CrossRef] [PubMed]
- Ashley, J.D.; Shelley, J.H.; Sun, J.; Song, J.; Trent, J.A.; Ambrosio, L.D.; Larson, D.J.; Larson, R.D.; Yabluchanskiy, A.; Kellawan, J.M. Cerebrovascular responses to graded exercise in young healthy males and females. Physiol. Rep. 2020, 8, e14622. [Google Scholar] [CrossRef] [PubMed]
- Nordgren, B.; Fridén, C.; Jansson, E.; Österlund, T.; Grooten, W.J.; Opava, C.H.; Rickenlund, A. Criterion validation of two submaximal aerobic fitness tests, the self-monitoring Fox-walk test and the Åstrand cycle test in people with rheumatoid arthritis. BMC Musculoskelet Disord. 2014, 15, 305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agostoni, P.; Dumitrescu, D. How to perform and report a cardiopulmonary exercise test in patients with chronic heart failure. Int. J. Cardiol. 2019, 1, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Levett, D.; Jack, S.; Swart, M.; Carlisle, J.; Wilson, J.; Snowden, C.; Riley, M.; Danjoux, G.; Ward, S.; Older, P.; et al. Perioperative Exercise Testing and Training Society (POETTS). Perioperative cardiopulmonary exercise testing (CPET): Consensus clinical guidelines on indications, organization, conduct, and physiological interpretation. Br. J. Anaesth. 2018, 120, 484–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parreira, V.F.; Janaudis-Ferreira, T.; Evans, R.A.; Mathur, S.; Goldstein, R.S.; Brooks, D. Measurement properties of the incremental shuttle walk test. A systematic review. Chest 2014, 145, 1357–1369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buckley, J.; Sim, J.; Eston, R.; Hession, R.; Fox, R. Reliability and validity of measures taken during the Chester step test to predict aerobic power and to prescribe aerobic exercise. Br. J. Sports Med. 2004, 38, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Sykes, K.; Roberts, A. The Chester step test—A simple yet effective tool for aerobic capacity. Physiotherapy 2004, 90, 183–188. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 20) | Men (n = 14) | Women (n = 6) | |
|---|---|---|---|
| Age (years) | 27.8 ± 4.4 | 27.5 ± 4.8 | 28.5 ± 3.8 |
| Height (cm) | 169.1 ± 6.3 | 171.9 ± 5.1 | 162.5 ± 3.3 |
| Body weight (kg) | 63.5 ± 11.6 | 66.7 ± 12.2 | 56.0 ± 4.7 |
| Body mass index (kg/m2) | 22.1 ± 3.2 | 22.5 ± 3.7 | 21.2 ± 1.6 |
| CE-CPX | SHS-CPX | p-Value | 95% CI | |
|---|---|---|---|---|
| Resting cardiopulmonary function | ||||
| Heart rate (bpm) | 79.3 ± 9.4 | 75.1 ± 9.7 | 0.0918 | −9.15 to 0.75 |
| Systolic blood pressure (mmHg) | 125.6 ± 13.2 | 122.3 ± 13.5 | 0.1378 | −7.876 to 1.176 |
| Diastolic blood pressure (mmHg) | 81.4 ± 11.8 | 81.3 ± 9.7 | 0.9530 | −5.411 to 5.111 |
| Peak cardiopulmonary function | ||||
| Peak (mL/min/kg) | 40.4 ± 11.3 | 28.9 ± 8.0 | <0.0001 | −14.48 to −7.29 |
| Respiratory exchange ratio | 1.17 ± 0.04 | 1.09 ± 0.05 | <0.0001 | −0.105 to −0.050 |
| Heart rate (bpm) | 190.6 ± 8.9 | 172.1 ± 12.6 | <0.0001 | −24.96 to −11.84 |
| Systolic blood pressure (mmHg) | 143.6 ± 31.8 | 143.6 ± 16.6 | 0.9937 | −13.19 to 13.09 |
| Diastolic blood pressure (mmHg) | 79.5 ± 18.2 | 81.8 ± 11.7 | 0.4777 | −4.347 to 8.947 |
| Completion time (s) | 1052.8 ± 143.7 | 609.1 ± 96.2 | <0.0001 | −506.9 to −380.6 |
| Peak workload (watt) | 202.5 ± 60.1 | - | - | - |
| Peak workload (beat/min) | - | 133.3 ± 7.9 | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imashiro, K.; Nishioka, Y.; Teramura, K.; Hashimoto, H.; Kimura, H.; Tanabe, N.; Taniguchi, Y.; Nakai, K.; Umemoto, Y.; Ito, T.; et al. Feasibility of Seated Stepping and Handshaking as a Cardiopulmonary Exercise Testing: A Pilot Study. J. Clin. Med. 2023, 12, 2140. https://doi.org/10.3390/jcm12062140
Imashiro K, Nishioka Y, Teramura K, Hashimoto H, Kimura H, Tanabe N, Taniguchi Y, Nakai K, Umemoto Y, Ito T, et al. Feasibility of Seated Stepping and Handshaking as a Cardiopulmonary Exercise Testing: A Pilot Study. Journal of Clinical Medicine. 2023; 12(6):2140. https://doi.org/10.3390/jcm12062140
Chicago/Turabian StyleImashiro, Kyosuke, Yasuko Nishioka, Kenzo Teramura, Hiromi Hashimoto, Hiroki Kimura, Naoya Tanabe, Yasuhiro Taniguchi, Koya Nakai, Yasunori Umemoto, Tomoyuki Ito, and et al. 2023. "Feasibility of Seated Stepping and Handshaking as a Cardiopulmonary Exercise Testing: A Pilot Study" Journal of Clinical Medicine 12, no. 6: 2140. https://doi.org/10.3390/jcm12062140