

Roots and Root Canals Characterization of Permanent Mandibular Premolars Analyzed Using the Cone Beam and Micro Computed Tomography—A Systematic Review and Metanalysis

 ,
,  ,
,  ,
,  ,
,  , , , and
, , , and 
Abstract
:1. Introduction
2. Methodology
2.1. Registration and Protocol
Research Question
- Population: human mandibular premolars
- Intervention: CBCT or Micro CT
- Comparison: first premolar and second premolar with normal anatomy
- Outcome: anatomy of root, as well as root canal
- Study: retrospective radiographic imaging analysis
2.2. Search Strategy and Source
2.3. The Eligibility Criteria and Study Selection
2.4. Data Sources and Extraction
2.5. Assessment of Scientific Merit
2.6. Statistical Analysis
3. Results
3.1. Study Excerpt
3.2. Study Features
3.2.1. First Premolars
3.2.2. Second Premolars
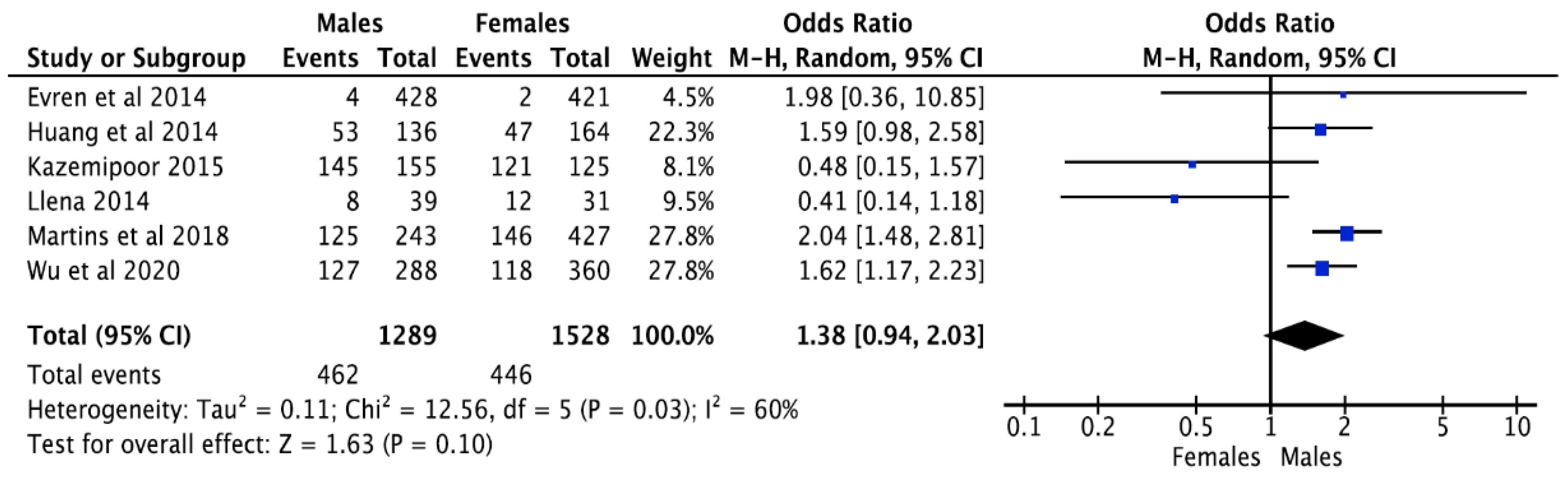
3.3. Second Root Canal and Root Prevalence Concerning Gender
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Karobari, M.I.; Parveen, A.; Mirza, M.B.; Makandar, S.D.; Nik Abdul Ghani, N.R.; Noorani, T.Y.; Marya, A. Root and root canal morphology classification systems. Int. J. Dent. 2021, 2021, 6682189. [Google Scholar] [CrossRef] [PubMed]
- Alfawaz, H.; Alqedairi, A.; Al-Dahman, Y.H.; Al-Jebaly, A.S.; Alnassar, F.A.; Alsubait, S.; Allahem, Z. Evaluation of root canal morphology of mandibular premolars in a Saudi population using cone beam computed tomography: A retrospective study. Saudi Dent. J. 2019, 31, 137–142. [Google Scholar] [CrossRef]
- Mirza, M.; Gufran, K.; Alhabib, O.; Alafraa, O.; Alzahrani, F.; Abuelqomsan, M.; Karobari, M.; Alnajei, A.; Afroz, M.; Akram, S. CBCT based study to analyze and classify root canal morphology of maxillary molars-a retrospective study. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 6550–6560. [Google Scholar] [PubMed]
- Awawdeh, L.; Al-Qudah, A. Root form and canal morphology of mandibular premolars in a Jordanian population. Int. Endod. J. 2008, 41, 240–248. [Google Scholar] [CrossRef]
- Bolhari, B.; Assadian, H.; Fattah, T. Evaluation of the root canal morphology of mandibular second premolars in an Iranian population. J. Dent. 2013, 10, 516. [Google Scholar]
- Bulut, D.G.; Kose, E.; Ozcan, G.; Sekerci, A.E.; Canger, E.M.; Sisman, Y. Evaluation of root morphology and root canal configuration of premolars in the Turkish individuals using cone beam computed tomography. Eur. J. Dent. 2015, 9, 551–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bürklein, S.; Heck, R.; Schäfer, E. Evaluation of the root canal anatomy of maxillary and mandibular premolars in a selected German population using cone-beam computed tomographic data. J. Endod. 2017, 43, 1448–1452. [Google Scholar] [CrossRef]
- Çalişkan, M.K.; Pehlivan, Y.; Sepetçioğlu, F.; Türkün, M.; Tuncer, S.Ş. Root canal morphology of human permanent teeth in a Turkish population. J. Endod. 1995, 21, 200–204. [Google Scholar] [CrossRef]
- Celikten, B.; Orhan, K.; Aksoy, U.; Tufenkci, P.; Kalender, A.; Basmaci, F.; Dabaj, P. Cone-beam CT evaluation of root canal morphology of maxillary and mandibular premolars in a Turkish Cypriot population. BDJ Open 2016, 2, 15006. [Google Scholar] [CrossRef] [Green Version]
- Iqbal, A.; Karobari, M.I.; Alam, M.K.; Khattak, O.; Alshammari, S.M.; Adil, A.H.; Noorani, T.Y.; Algarani, H.A.; Alonazi, M.A.; Sirivastava, K.C. Evaluation of root canal morphology in permanent maxillary and mandibular anterior teeth in Saudi subpopulation using two classification systems: A CBCT study. BMC Oral Health 2022, 22, 171. [Google Scholar] [CrossRef]
- Karobari, M.I.; Noorani, T.Y.; Halim, M.S.; Ahmed, H.M.A. Root and canal morphology of the anterior permanent dentition in Malaysian population using two classification systems: A CBCT clinical study. Aust. Endod. J. 2021, 47, 202–216. [Google Scholar] [CrossRef]
- Arıkan, N.F.Ö. Areas of Use for Micro-CT in Endodontics: A review. J. Med. Dent. Investig. 2020, 1, 1–11. [Google Scholar]
- Felsypremila, G.; Vinothkumar, T.S.; Kandaswamy, D. Anatomic symmetry of root and root canal morphology of posterior teeth in Indian subpopulation using cone beam computed tomography: A retrospective study. Eur. J. Dent. 2015, 9, 500–507. [Google Scholar] [CrossRef] [PubMed]
- Green, D. Double canals in single roots. Oral Surg. Oral Med. Oral Pathol. 1973, 35, 689–696. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Guo, B.; Li, K.-Z.; Zhang, R.; Tian, Y.-Y.; Wang, H. Cone-beam computed tomography study of root and canal morphology of mandibular premolars in a western Chinese population. BMC Med. Imaging 2012, 12, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SalarPour, M.; Mollashahi, N.F.; Mousavi, E.; SalarPour, E. Evaluation of the effect of tooth type and canal configuration on crown size in mandibular premolars by cone-beam computed tomography. Iran. Endod. J. 2013, 8, 153. [Google Scholar] [PubMed]
- Llena, C.; Fernandez, J.; Ortolani, P.S.; Forner, L. Cone-beam computed tomography analysis of root and canal morphology of mandibular premolars in a Spanish population. Imaging Sci. Dent. 2014, 44, 221–227. [Google Scholar] [CrossRef] [Green Version]
- Ok, E.; Altunsoy, M.; Nur, B.G.; Aglarci, O.S.; Çolak, M.; Güngör, E. A cone-beam computed tomography study of root canal morphology of maxillary and mandibular premolars in a Turkish population. Acta Odontol. Scand. 2014, 72, 701–706. [Google Scholar] [CrossRef]
- Shetty, A.; Hegde, M.N.; Tahiliani, D.; Shetty, H.; Bhat, G.T.; Shetty, S. A three-dimensional study of variations in root canal morphology using cone-beam computed tomography of mandibular premolars in a South Indian population. J. Clin. Diagn. Res. JCDR 2014, 8, ZC22. [Google Scholar] [CrossRef]
- Arslan, H.; Capar, I.D.; Ertas, E.T.; Ertas, H.; Akcay, M. A cone-beam computed tomographic study of root canal systems in mandibular premolars in a Turkish population: Theoretical model for determining orifice shape. Eur. J. Dent. 2015, 9, 011–019. [Google Scholar] [CrossRef]
- Hajihassani, N.; Roohi, N.; Madadi, K.; Bakhshi, M.; Tofangchiha, M. Evaluation of root canal morphology of mandibular first and second premolars using cone beam computed tomography in a defined group of dental patients in Iran. Scientifica 2017, 2017, 1504341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khademi, A.; Mehdizadeh, M.; Sanei, M.; Sadeqnejad, H.; Khazaei, S. Comparative evaluation of root canal morphology of mandibular premolars using clearing and cone beam computed tomography. Dent. Res. J. 2017, 14, 321. [Google Scholar]
- Martins, J.N.; Marques, D.; Mata, A.; Caramês, J. Root and root canal morphology of the permanent dentition in a Caucasian population: A cone-beam computed tomography study. Int. Endod. J. 2017, 50, 1013–1026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martins, J.N.; Francisco, H.; Ordinola-Zapata, R. Prevalence of C-shaped configurations in the mandibular first and second premolars: A cone-beam computed tomographic in vivo study. J. Endod. 2017, 43, 890–895. [Google Scholar] [CrossRef] [PubMed]
- Martins, J.N.; Gu, Y.; Marques, D.; Francisco, H.; Caramês, J. Differences on the root and root canal morphologies between Asian and white ethnic groups analyzed by cone-beam computed tomography. J. Endod. 2018, 44, 1096–1104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martins, J.N.; Ordinola-Zapata, R.; Marques, D.; Francisco, H.; Caramês, J. Differences in root canal system configuration in human permanent teeth within different age groups. Int. Endod. J. 2018, 51, 931–941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedemonte, E.; Cabrera, C.; Torres, A.; Jacobs, R.; Harnisch, A.; Ramírez, V.; Concha, G.; Briner, A.; Brizuela, C. Root and canal morphology of mandibular premolars using cone-beam computed tomography in a Chilean and Belgian subpopulation: A cross-sectional study. Oral Radiol. 2018, 34, 143–150. [Google Scholar] [CrossRef]
- Razumova, S.; Brago, A.; Khaskhanova, L.; Howijieh, A.; Barakat, H.; Manvelyan, A. A cone-beam computed tomography scanning of the root canal system of permanent teeth among the Moscow population. Int. J. Dent. 2018, 2018, 2615746. [Google Scholar] [CrossRef] [Green Version]
- Corbella, S.; Baruffaldi, M.; Perondi, I.; Taschieri, S. Surgically-oriented anatomical study of mandibular premolars: A CBCT study. J. Clin. Exp. Dent. 2019, 11, e877. [Google Scholar] [CrossRef]
- Corbella, S.; Baruffaldi, M.; Perondi, I.; Taschieri, S. Cone-beam computed tomography investigation of the anatomy of permanent mandibular premolars in a cohort of Caucasians. J. Investig. Clin. Dent. 2019, 10, e12373. [Google Scholar] [CrossRef] [Green Version]
- Büyükbayram, I.K.; Sübay, R.K.; Çolakoğlu, G.; Elçin, M.A.; Sübay, M.O. Investigation using cone beam computed tomography analysis, of radicular grooves and canal configurations of mandibular premolars in a Turkish subpopulation. Arch. Oral Biol. 2019, 107, 104517. [Google Scholar] [CrossRef]
- Mashyakhy, M.; Gambarini, G. Root and root canal morphology differences between genders: A comprehensive in-vivo CBCT study in a Saudi population. Acta Stomatol. Croat. Int. J. Oral Sci. Dent. Med. 2019, 53, 231–246. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.Y.Y.; Parolia, A.; Chuah, S.R.; Bhatia, S.; Mutalik, S.; Pau, A. Root canal morphology of permanent teeth in a Malaysian subpopulation using cone-beam computed tomography. BMC Oral Health 2019, 19, 14. [Google Scholar] [CrossRef] [PubMed]
- Rajakeerthi, R.; Nivedhitha, M.S.B. Use of cone beam computed tomography to identify the morphology of maxillary and mandibular premolars in Chennai population. Braz. Dent. Sci. 2019, 22, 55–62. [Google Scholar] [CrossRef] [Green Version]
- Shemesh, A.; Lalum, E.; Itzhak, J.B.; Levy, D.H.; Lvovsky, A.; Levinson, O.; Solomonov, M. Radicular grooves and complex root morphologies of mandibular premolars among Israeli population. J. Endod. 2020, 46, 1241–1247. [Google Scholar] [CrossRef]
- Alghamdi, F.T.; Khalil, W.A. Root canal morphology and symmetry of mandibular second premolars using cone-beam computed tomography. Oral Radiol. 2022, 38, 126–138. [Google Scholar] [CrossRef] [PubMed]
- Al-Zubaidi, S.M.; Almansour, M.I.; Alshammari, A.S.; Al Mansour, N.N.; Alshammari, A.F.; Altamimi, Y.S.; Madfa, A.A. Root and canal morphology of mandibular premolars in a Saudi subpopulation: A cone-beam computed tomography study. Int. J. Dent. 2022, 2022, 4038909. [Google Scholar] [CrossRef] [PubMed]
- Thanaruengrong, P.; Kulvitit, S.; Navachinda, M.; Charoenlarp, P. Prevalence of complex root canal morphology in the mandibular first and second premolars in Thai population: CBCT analysis. BMC Oral Health 2021, 21, 449. [Google Scholar] [CrossRef] [PubMed]
- Moreno, J.O.; Duarte, M.L.; Marceliano-Alves, M.F.; Alves, F.R.; Siqueira, J.F., Jr.; Provenzano, J.C. Micro-computed tomographic evaluation of root canal morphology in mandibular first premolars from a Colombian population. Acta Odontológica Latinoam. 2021, 34, 50–55. [Google Scholar] [CrossRef]
- Martins, J.N.; Marques, D.; Francisco, H.; Caramês, J. Gender influence on the number of roots and root canal system configuration in human permanent teeth of a Portuguese subpopulation. Quintessence Int 2018, 49, 103–111. [Google Scholar]
- Mashyakhy, M.; Chourasia, H.R.; Halboub, E.; Almashraqi, A.A.; Khubrani, Y.; Gambarini, G. Anatomical variations and bilateral symmetry of roots and root canal system of mandibular first permanent molars in Saudi Arabian population utilizing cone-beam computed tomography. Saudi Dent. J. 2019, 31, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Kazemipoor, M.; Hajighasemi, A.; Hakimian, R. Gender difference and root canal morphology in mandibular premolars: A cone-beam computed tomography study in an Iranian population. Contemp. Clin. Dent. 2015, 6, 401. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.; Hu, D.Q.; Xin, B.C.; Sun, D.G.; Ge, Z.P.; Su, J.Y. Root canal morphology of maxillary and mandibular first premolars analyzed using cone-beam computed tomography in a Shandong Chinese population. Medicine 2020, 99. [Google Scholar] [CrossRef]
- Yang, H.; Tian, C.; Li, G.; Yang, L.; Han, X.; Wang, Y. A cone-beam computed tomography study of the root canal morphology of mandibular first premolars and the location of root canal orifices and apical foramina in a Chinese subpopulation. J. Endod. 2013, 39, 435–438. [Google Scholar] [CrossRef] [PubMed]
- Monsarrat, P.; Arcaute, B.; Peters, O.A.; Maury, E.; Telmon, N.; Georgelin-Gurgel, M.; Maret, D. Interrelationships in the variability of root canal anatomy among the permanent teeth: A full-mouth approach by cone-beam CT. PloS ONE 2016, 11, e0165329. [Google Scholar] [CrossRef] [PubMed]
- Boschetti, E.; Silva-Sousa, Y.T.C.; Mazzi-Chaves, J.F.; Leoni, G.B.; Versiani, M.A.; Pécora, J.D.; Saquy, P.C.; Sousa, M.D.D. Micro-CT evaluation of root and canal morphology of mandibular first premolars with radicular grooves. Braz. Dent. J. 2017, 28, 597–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sierra-Cristancho, A.; González-Osuna, L.; Poblete, D.; Cafferata, E.A.; Carvajal, P.; Lozano, C.P.; Vernal, R. Micro-tomographic characterization of the root and canal system morphology of mandibular first premolars in a Chilean population. Sci. Rep. 2021, 11, 1–10. [Google Scholar] [CrossRef]
- Ordinola-Zapata, R.; Monteiro Bramante, C.; Gagliardi Minotti, P.; Cavalini Cavenago, B.; Gutmann, J.L.; Moldauer, B.I.; Versiani, M.A.; Hungaro Duarte, M.A. Micro-CT evaluation of C-shaped mandibular first premolars in a Brazilian subpopulation. Int. Endod. J. 2015, 48, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Karobari, M.I.; Arshad, S.; Noorani, T.Y.; Ahmed, N.; Basheer, S.N.; Peeran, S.W.; Marya, A.; Marya, C.M.; Messina, P.; Scardina, G.A. Root and root canal configuration characterization using microcomputed tomography: A systematic review. J. Clin. Med. 2022, 11, 2287. [Google Scholar] [CrossRef]
- Parekh, V.; Shah, N.; Joshi, H. Root canal morphology and variations of mandibular premolars by clearing technique: An in vitro study. J. Contemp. Dent. Pract. 2011, 12, 318–321. [Google Scholar]
- Rahimi, S.; Shahi, S.; Yavari, H.R.; Reyhani, M.F.; Ebrahimi, M.E.; Rajabi, E. A stereomicroscopy study of root apices of human maxillary central incisors and mandibular second premolars in an Iranian population. J. Oral Sci. 2009, 51, 411–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Habib, A.A.; Kalaji, M.N. Root canal configurations of the first and second mandibular premolars in the population of north Syria. J. Taibah Univ. Med. Sci. 2015, 10, 391–395. [Google Scholar] [CrossRef] [Green Version]
- Rahimi, S.; Shahi, S.; Yavari, H.R.; Manafi, H.; Eskandarzadeh, N. Root canal configuration of mandibular first and second premolars in an Iranian population. J. Dent. Res. Dent. Clin. Dent. Prospect. 2017, 1, 59–64. [Google Scholar]
- Sikri, V.; Sikri, P. Mandibular premolars: Aberrations in pulp space morphology. Indian J. Dent. Res. Off. Publ. Indian Soc. Dent. Res. 1994, 5, 9–14. [Google Scholar]
- Singh, S.; Pawar, M. Root canal morphology of South Asian Indian mandibular premolar teeth. J. Endod. 2014, 40, 1338–1341. [Google Scholar] [CrossRef]
- Yadav, R.K.; Ashutosh, C.A.; Tikku, A.; Rathinavel, C. Root canal morphology of mandibular second premolars in a north Indian subpopulation. Int. J. Sci. Res. Publ. 2013, 3, 1–4. [Google Scholar]
- Kharouf, N.; Haikel, Y.; Mancino, D. Root anatomy of mandibular second premolars in French subpopulation: A retrospective observational case series. Contemp. Clin. Dent. 2019, 10, 494. [Google Scholar] [CrossRef]
- Vertucci, F.J. Root canal morphology and its relationship to endodontic procedures. Endod. Top. 2005, 10, 3–29. [Google Scholar] [CrossRef]
- Pineda, F.; Kuttler, Y. Mesiodistal and buccolingual roentgenographic investigation of 7,275 root canals. Oral Surg. Oral Med. Oral Pathol. 1972, 33, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Zillich, R.; Dowson, J. Root canal morphology of mandibular first and second premolars. Oral Surg. Oral Med. Oral Pathol. 1973, 36, 738–744. [Google Scholar] [CrossRef]
- Briseño-Marroquín, B.; Paqué, F.; Maier, K.; Willershausen, B.; Wolf, T.G. Root canal morphology and configuration of 179 maxillary first molars by means of micro–computed tomography: An ex vivo study. J. Endod. 2015, 41, 2008–2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyoshi, S.; Fujiwara, J.; YNakata, T.T.; Yamamoto, K. Bifurcated root canals and crown diameter. J. Dent. Res. 1977, 56, 1425. [Google Scholar] [CrossRef] [PubMed]
- Sert, S.; Bayirli, G.S. Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population. J. Endod. 2004, 30, 391–398. [Google Scholar] [CrossRef]
- Weine, F.S.; Healey, H.J.; Gerstein, H.; Evanson, L. Canal configuration in the mesiobuccal root of the maxillary first molar and its endodontic significance. Oral Surg. Oral Med. Oral Pathol. 1969, 28, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Ingle, J.I.; Bakland, L.K.; Baumgartner, J.C. Ingle’s Endodontics, 6th ed.; BC Decker: Hamilton, ON, Canada, 2008; pp. 342–345. [Google Scholar]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Searched Strategies | Results |
|---|---|---|
| PubMed | “configuration of root and canal” OR “morphology root and canal” OR “root and canal system” AND “mandibular premolars AND “morphology” OR “anatomy”AND “Cone-Beam Computed Tomography” OR “MICRO CT” | 1148 |
| Science Direct | “mandibular premolars” AND “morphology of root and canal” AND “anatomy” OR “morphology” AND “CBCT” OR “MICRO CT” | 578 |
| Web of Science | “CBCT” OR “Micro CT” AND “Premolar” AND “morphology” | 583 |
| Google Scholar | “mandibular Premolar “,”CBCT”,”Micro CT”,”Root canal” | 1162 |
| Total | 3471 |
|
| Author | Country | Sample Size | RCC-Frequency (%) | Roots (n; %) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| RCC | Ve (1984) | I | II | III | IV | V | VI | VII | VIII | 1 | 2 | 3 | |||
| We (1969) | I | II | III | ||||||||||||
| Br (2015) | 1–1–1/1 | 2–2–1/1 | 1–2–1/1 | 2–2–2/2 | 1–1–2/2 | 2–1–2/2 | 1–2–1/2 | 1–1–3/3 | |||||||
| Yu et al., 2012 [15] | CHN | 178 | CBCT | 97.2 | 0.55 | 0 | 0 | 1.7 | 0 | 0 | 0 | 0.55 | 100 | 0 | 0 |
| Salarpour et al., 2013 [16] | IRN | 41 | CBCT | 75.6 | – | – | – | 22 | – | – | – | 2.4 | 100 | 0 | 0 |
| LLena et al., 2014 [17] | ESP | 53 | CBCT | 90.6 | 1.8 | – | – | 7.5 | – | – | – | – | 100 | 0 | 0 |
| Ok et al., 2014 [18] | TUR | 1345 | CBCT | 98.5 | 0.1 | 0.07 | 0.6 | 0.5 | 0 | 0 | 0.2 | – | – | – | – |
| Shetty et al., 2014 [19] | IND | 814 | CBCT | 93.5 | 1.4 | 0.2 | 0 | 3.9 | 0 | 0 | 0.1 | 0.7 | 100 | 0 | 0 |
| Arslan et al., 2015 [20] | TUR | 133 | CBCT | 92.4 | 2.2 | 0.7 | 0 | 1.5 | 0 | 0 | 0 | 2.9 | 96.2 | 3.8 | 0 |
| Bulut et al., 2015 [6] | TUR | 549 | CBCT | 98.9 | 0.2 | 0.4 | 0 | 0.5 | 0 | 0 | 0 | 0 | 98.9 | 1.1 | 0 |
| Felsypremila et al., 2015 [13] | IND | 398 | CBCT | 98.4 | 0 | 0 | 0 | 0.8 | 0 | 0 | 0 | 0.8 | – | – | – |
| Çelikten et al., 2016 [9] | TUR | 433 | CBCT | 96.6 | 1.1 | 1.1 | – | 1.1 | – | – | – | – | – | – | – |
| Bürklein et al., 2017 [7] | GER | 871 | CBCT | 39 | 1.1 | 0.1 | 1.4 | 57.1 | 0.5 | 0.3 | 0.3 | 0 | 98.6 | 1.3 | 0.1 |
| Hajihassani et al., 2017 [21] | IRN | 57 | CBCT | 80.7 | 1.8 | 7 | 0 | 8.8 | 1.8 | 0 | 0 | 0 | 100 | 0 | 0 |
| F | |||||||||||||||
| 43 | M | 74.7 | 4.7 | 16.3 | 0 | 4.7 | 0 | 0 | 0 | 0 | 100 | 0 | 0 | ||
| Khademi et al., 2017 [22] | IRN | 182 (Ma2P & Ma1P) | CBCT | 92.3 | 0 | 2.2 | 2.2 | 3.3 | 0 | 0 | 0 | 0 | – | – | – |
| Martins et al., 2017 [23] | PRT | 833 | CBCT | 95.7 | 0.8 | 1.3 | 0.5 | 1.4 | – | – | – | – | 99.9 | 0.1 | 0 |
| Martins et al., 2017 [23] | PRT | 821 | CBCT | 95.8 | 0.8 | 1.2 | 0.5 | 1.3 | 0 | 0 | 0 | 0.3 | 99.9 | 0.1 | 0 |
| Martins et al., 2017 [24] | CHN | 235 | CBCT | 99.6 | 0.4 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 100 | 0 | 0 |
| PRT | 858 | 95.7 | 0.8 | 1.3 | 0.5 | 1.4 | 0 | 0 | 0 | 0.3 | 99.9 | 0.1 | 0 | ||
| Martins et al., 2018 [25] | PRT | 331 | CBCT | 94.3 | 0.6 | 2.1 | 0.6 | 1.5 | 0 | 0 | 0 | 0.9 | 99.7 | 0.3 | 0 |
| M | |||||||||||||||
| 527 | F | 96.6 | 0.9 | 0.8 | 0.4 | 1.3 | 0 | 0 | 0 | 0 | 100 | 0 | 0 | ||
| Martins et al., 2018 [26] | PRT (age ≤ 20) | 13 | CBCT | 69.2 | 0 | 7.7 | 0 | 7.7 | 0 | 0 | 0 | 15.4 | – | – | – |
| 251 | 21–40 | 98.8 | 0 | 0.4 | 0 | 0.8 | 0 | 0 | 0 | 0 | – | – | – | ||
| 395 | 41–60 | 96.2 | 1.3 | 1.3 | 0.2 | 0.8 | 0 | 0 | 0 | 0.2 | – | – | – | ||
| 199 | ≥ 61 | 92.5 | 1 | 2 | 1.5 | 3 | 0 | 0 | 0 | 0 | – | – | – | ||
| Pedemonte et al., 2018 [27] | BEL | 101 | CBCT | 92.1 | – | 3 | – | 5 | – | – | – | 1 | 98 | 2 | 0 |
| Comp | CHL | 100 | 95 | – | 2 | – | 2 | – | – | – | 0 | 99 | 1 | 0 | |
| – | |||||||||||||||
| Razumova et al., 2018 [28] | RUS | 443 | CBCT | 90.1 | . | . | 9.9 | – | – | – | – | – | 99.8 | 0.2 | 0 |
| Alfawaz et al., 2019 [2] | SAU | 172 | CBCT | 90.1 | 3.5 | 0 | 1.7 | 1.2 | 0 | 0 | 3.5 | 0 | 95.3 | 3.5 | 1.2 |
| F | |||||||||||||||
| 171 | M | 90.1 | 5.3 | 0.6 | 3.5 | 0.6 | 0 | 0 | 0 | 0 | 95.9 | 4.1 | 0 | ||
| Corbella et al., 2019 [29] | ITA | 100 | CBCT | 95 | 0 | 1 | 4 | 0 | 0 | 0 | 0 | 0 | 97 | 3 | 0 |
| Corbella et al., 2019 [30] | ITA | 88 | CBCT | 95.5 | 0 | 0 | 4.5 | 0 | 0 | 0 | 0 | 0 | 96.6 | 3.4 | 0 |
| Kaya Buyukbayram et al., 2019 [31] | TUR | 264 | CBCT | 97.7 | 0 | 1.1 | 0 | 0.38 | 0 | 0 | 0 | 0.8 | 100 | 0 | 0 |
| Mashyakhy and Gambarini 2019 [32] | SAU | 188 | CBCT | 94.7 | 0 | 2.7 | 0 | 1.6 | 0 | 0 | 0 | 1.1 | 100 | 0 | 0 |
| M | |||||||||||||||
| 191 | F | 99 | 0 | 0.5 | 0 | 0 | 0 | 0 | 0 | 0.5 | 100 | 0 | 0 | ||
| Pan et al., 2019 [33] | MYS | 399 | CBCT | 99.5 | 0.3 | – | 0.3 | – | – | – | – | – | 100 | 0 | 0 |
| Rajakeerthi and Nivedhitha 2019 [34] | IND | 200 | CBCT | 55.3 | 8.8 | 6.1 | 4.4 | 15.8 | 3.5 | 1.8 | 4.4 | 0 | 89.5 | 7 | 3.5 |
| M | |||||||||||||||
| F | 57 | 7 | 8.1 | 5.8 | 9.3 | 2.3 | 5.8 | 4.7 | 0 | 90.7 | 5.8 | 3.5 | |||
| Shemesh et al., 2020 [35] | ISR | 1678 (M 831/F 847) | CBCT | 96.4 | 0.6 | 1.7 | 0.1 | 0.6 | 0 | 0 | 0.1 | 0.5 | 99.5 | 0.5 | – |
| M | |||||||||||||||
| F | 97.6 | 0.1 | 1.1 | 0.5 | 0 | 0 | 0.3 | 0.2 | 99.8 | 0.2 | – | ||||
| Alghamdi [36] F 2021 | SaudiArabia | 1200 600 M, 600 F | CBCTM | 97.5 | 1.33 | 0.17 | 0.67 | 0.17 | 0.17 | 98.83 | 1.17 | ||||
| F | 98.33 | 1 | 0 | 0.5 | 0.17 | 0 | 97.83 | 2.17 | |||||||
| Zubaidi SM [37] 2022 | SaudiArabia | 493 | CBCT | (91.10) | (5.7) | (0.2) | (2.8) | 0 (0) | 1 (0.2) | 0 (0) | 0 (0) | 99.2 | 0.8 | ||
| Thanaruengrong [38] 2021 | Thailand | 538 | CBCT | 98 | 0.2 | 0.4 | 1.5 | 537 (99.8) | 1 (0.2) | – | |||||
| Moreno [39] JO 2021 | Brazil | 50 | Micro CT | 40 | 4 | 24 | 4 | 28 | |||||||
| Study | Country | Total JBI Score |
|---|---|---|
| Yu et al., 2012 [15] | CHN | 7 |
| Salarpour et al., 2013 [16] | IRI | 9 |
| Llena et al., 2014 [17] | ESP | 7 |
| Ok et al., 2014 [18] | TUR | 8 |
| Shetty et al., 2014 [19] | IND | 8 |
| Bulut et al., 2015 [6] | TUR | 9 |
| Celikten et al., 2016 [9] | TUR | 8 |
| Martins et al., 2017 [23] | PRT | 7 |
| Bu€rklein et al., 2017 [7] | GER | 7 |
| Hajihassani et al., 2017 [21] | IRI | 7 |
| Pedemonte et al. 2018 [27] | BEL | 9 |
| Corbella et al., 2019 [30] | ITA | 7 |
| Pan et al., 2019 [33] | MAS | 9 |
| Thanaruengrong et al., 2021 [38] | Thailand | 8 |
| Zubaidi SM et al., 2022 [37] | Saudi Arabia | 9 |
| RCC-Frequency Numerical | Roots Numerical | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ve (1984) | I | II | III | IV | V | VI | VII | VIII | 1 | 2 | 3 | |
| We (1969) | I | II | III | |||||||||
| Br (2015) | 1–1–1/1 | 2–2–1/1 | 1–2–1/1 | 2–2–2/2 | 1–1–2/2 | 2–1–2/2 | 1–2–1/2 | 1–1–3/3 | ||||
| Pooled prevalence% | 74.34 | 2.2 | 2.5 | 3.75 | 15.45 | 0.44 | 0.13 | 0.1 | 0.95 | 85.20 | 11.20 | 2.50 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karobari, M.I.; Assiry, A.A.; Lin, G.S.S.; Almubarak, H.; Alqahtani, S.A.; Tasleem, R.; Mustafa, M.; Luke, A.M.; Shetty, K.P.; Noorani, T.Y.; et al. Roots and Root Canals Characterization of Permanent Mandibular Premolars Analyzed Using the Cone Beam and Micro Computed Tomography—A Systematic Review and Metanalysis. J. Clin. Med. 2023, 12, 2183. https://doi.org/10.3390/jcm12062183
Karobari MI, Assiry AA, Lin GSS, Almubarak H, Alqahtani SA, Tasleem R, Mustafa M, Luke AM, Shetty KP, Noorani TY, et al. Roots and Root Canals Characterization of Permanent Mandibular Premolars Analyzed Using the Cone Beam and Micro Computed Tomography—A Systematic Review and Metanalysis. Journal of Clinical Medicine. 2023; 12(6):2183. https://doi.org/10.3390/jcm12062183
Chicago/Turabian StyleKarobari, Mohmed Isaqali, Ali A. Assiry, Galvin Sim Siang Lin, Hussain Almubarak, Saleh Ali Alqahtani, Robina Tasleem, Mohammed Mustafa, Alexander Maniangat Luke, Krishna Prasad Shetty, Tahir Yusuf Noorani, and et al. 2023. "Roots and Root Canals Characterization of Permanent Mandibular Premolars Analyzed Using the Cone Beam and Micro Computed Tomography—A Systematic Review and Metanalysis" Journal of Clinical Medicine 12, no. 6: 2183. https://doi.org/10.3390/jcm12062183
APA StyleKarobari, M. I., Assiry, A. A., Lin, G. S. S., Almubarak, H., Alqahtani, S. A., Tasleem, R., Mustafa, M., Luke, A. M., Shetty, K. P., Noorani, T. Y., & Scardina, G. A. (2023). Roots and Root Canals Characterization of Permanent Mandibular Premolars Analyzed Using the Cone Beam and Micro Computed Tomography—A Systematic Review and Metanalysis. Journal of Clinical Medicine, 12(6), 2183. https://doi.org/10.3390/jcm12062183