
Cerebral Protection Strategies and Stroke in Surgery for Acute Type A Aortic Dissection

 ,
,  , , ,
, , ,
Abstract
1. Introduction
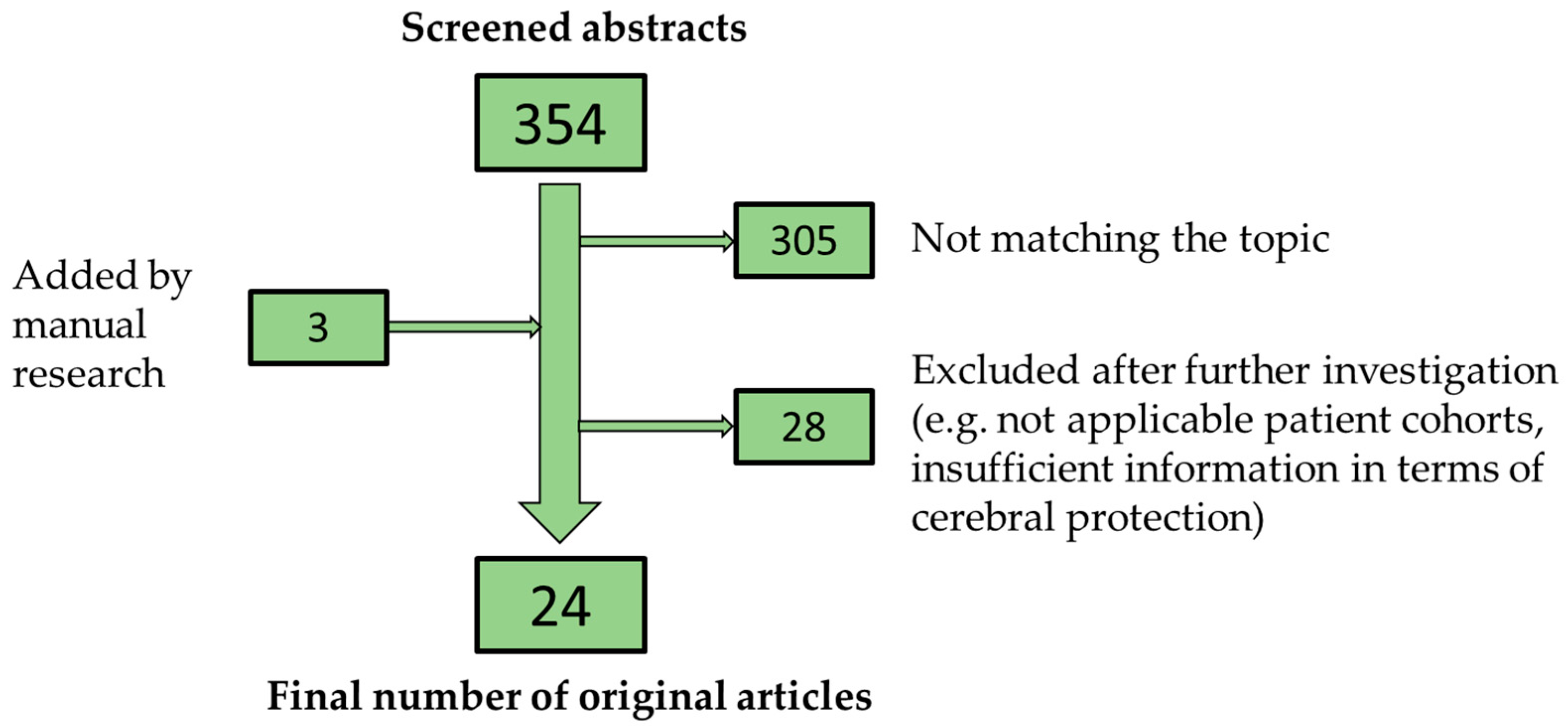
2. Materials and Methods
3. Results
3.1. Deep Hypothermic Circulatory Arrest
3.2. Retrograde Cerebral Perfusion
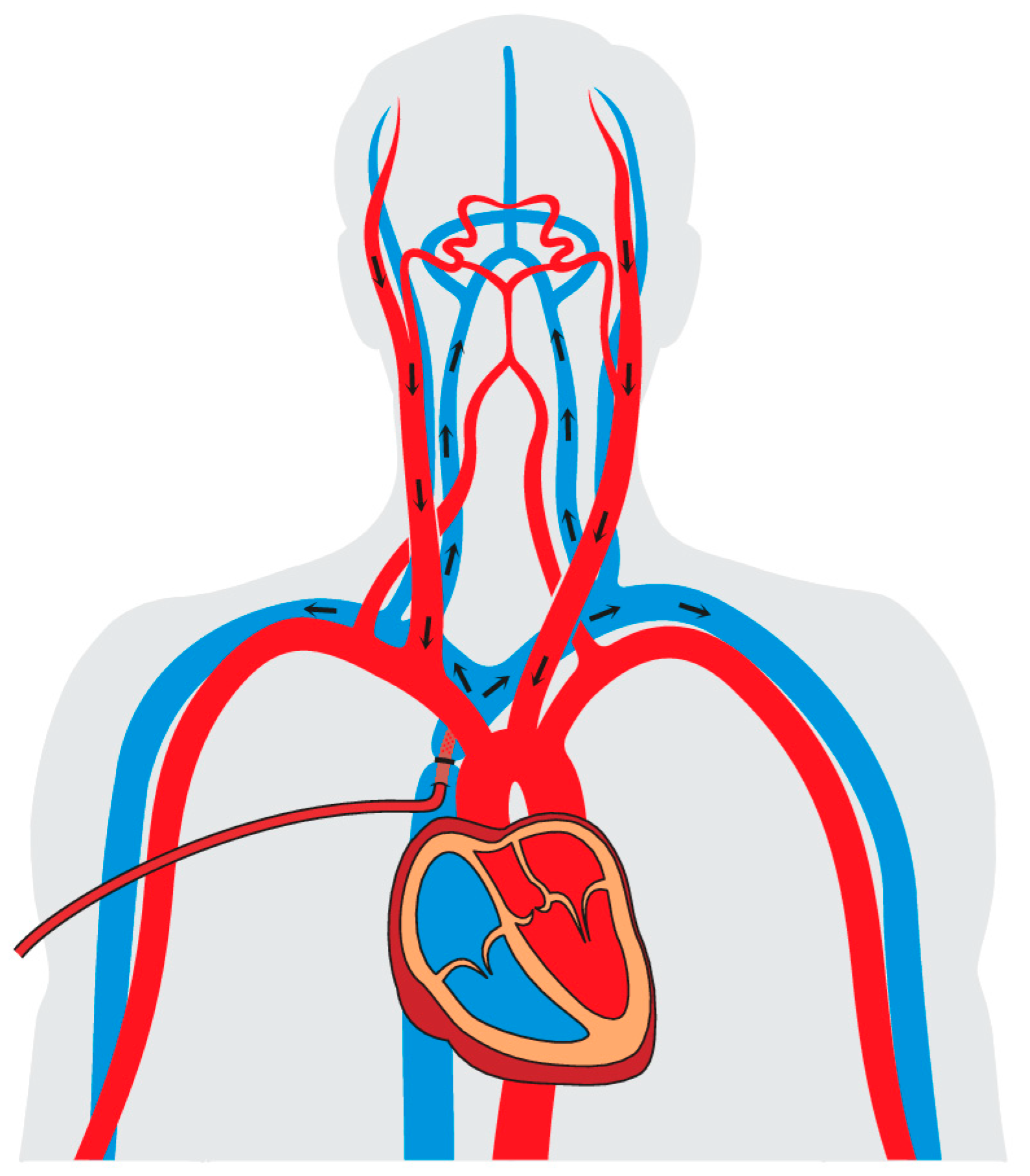
3.3. Antegrade Cerebral Perfusion
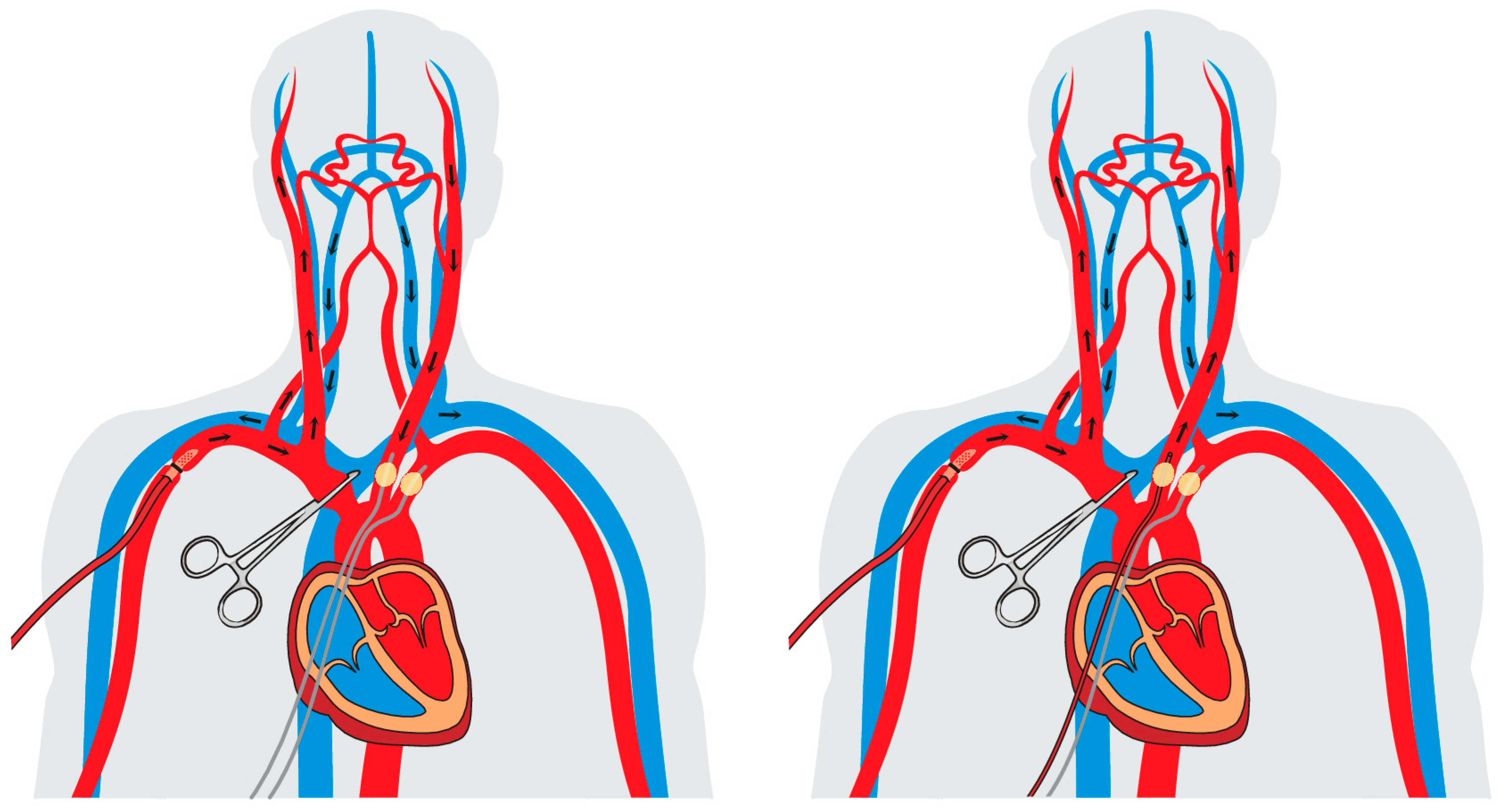
3.4. Unilateral or Bilateral?
3.5. Arterial Cannulation and Neuroprotection
3.6. Hypothermia and Neuroprotection
3.7. Monitoring for Neuroprotection
3.8. Neuroprotective Drugs
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACP | Antegrade cerebral perfusion |
| ATAAD | Acute type A aortic dissection |
| bACP | Bilateral antegrade cerebral perfusion |
| DHCA | Deep hypothermic circulatory arrest |
| NIRS | Near infrared spectroscopy |
| RCP | Retrograde cerebral perfusion |
| uACP | Unilateral antegrade cerebral perfusion |
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Author and Year | Number of Patients | Cerebral Protection Technique, n (%) | Preoperative Cerebral Malperfusion, n (%) | Mean Temperature, °C (±SD/Median) | Circulatory Arrest, Minutes (±SD/Median) | Neurological Outcome Defined as New Postoperative Neurological Deficit (*) or Permanent (PND) and Transient (TND) Neurological Deficit, n (%) | Identified Influencing Factors on Neurological Outcome |
|---|---|---|---|---|---|---|---|
| Montagner, 2022 [38] | n = 186 | uACP: 62 (33.3) bACP: 62 (33.3) RCP: 62 (33.3) | uACP: 12 (19.4) bACP: 10 (16.1) RCP: 8 (12.9) | uACP: 25 ± 4 bACP: 28 ± 3 RCP: 17 ± 3 | uACP: 33 ± 16 bACP: 38 ± 14 RCP: 35 ± 15 | uACP: 8 (12.9) * bACP: 7 (11.3) * RCP: 8 (12.9) * | n.a. |
| Song, 2022 [50] | n = 188 | uACP: 94 (50.0) bACP: 94 (50.0) | n.a. | uACP: 28 (27–28) bACP: 28 (27–28) | uACP: 41 (32–56) bACP: 43 (35–56) | uACP: PND 8 (8.5), TND 19 (20.2) bACP: 11 (11.8), TND 17 (18.1) | n.a. |
| Samanidis, 2021 [39] | n = 290 | ACP: 117 (40.3) RCP: 173 (59.7) | ACP: 14 (12.0) RCP: 32 (18.5) | ACP: 22 (21–23) RCP: 18 (17–21) | ACP: 33 (26–48) RCP: 26 (21–33) | ACP: PND 12 (10.3), TND 15 (12.8) RCP: PND 12 (6.9), TND 22 (12.7) | n.a. |
| Piperata, 2021 [55] | n = 378 | uACP: 189 (50.0) bACP: 189 (50.0) | uACP: 5 (3) bACP: 5 (3) | uACP: 28 (28–28) bACP: 28 (25–28) | uACP: 35 (28–44) bACP: 36 (28–44) | uACP: PND 8 (4.0), TND 21 (11.0) bACP: PND 26 (14.0), TND 23 (12.0) | Risk Factors:
|
| Benedetto, 2021 [22] | n = 1929 | uACP: 117 (6.1) bACP: 760 (39.4) RCP: 222 (11.5) DHCA: 830 (43.0) | uACP: 10 (8.5) bACP: 76 (10.0) RCP: 22 (9.9) DHCA: 52 (6.3) | n.a. | uACP: 35 ± 21 bACP: 44 ± 36 RCP: 31 ± 19 DHCA: 33 ± 22 | uACP: 11 (9.4) * bACP: 111 (14.6) * RCP: 29 (13.1) * DHCA: 118 (14.2) * | Risk Factors:
|
| Sun, 2021 [40] | n = 108 | ACP: 54 (50.0) RCP: 54 (50.0) | ACP: 2 (3.7) RCP: 2 (3.7) | ACP: 25 (n.a.) RCP: 18 (n.a.) | ACP: 88 ± 5 RCP: 63 ± 10 | ACP: PND 10 (18.5) RCP: PND 6 (11.1) | Risk Factors:
|
| Xue, 2021 [41] | n = 746 | uACP: 617 (82.7) bACP: 13 (1.8) RCP: 51 (6.8) DHCA: 65 (8.7) | Total: 82 (11.0) | Total: 21 (14–30) | Total: 29 ± 12 | Total: PND 35 (4.7) | Risk Factors:
|
| Angleitner, 2020 [52] | n = 184 | uACP: 93 (50.5) bACP: 91 (49.5) | uACP: 21 (22.6) bACP: 15 (16.5) | n.a. | uACP: 30 (25–45) bACP: 38 (30–57) | uACP: PND 18 (19.4), TND 9 (9.7) bACP: PND 17 (18.7), TND 7 (7.7) | n.a. |
| Norton, 2020 [53] | n = 307 | uACP: 140 (45.6) bACP: 167 (54.4) | uACP: 10 (7.1) bACP: 7 (4.2) | uACP: 20 (18–24) bACP: 17 (16–18) | uACP: 29 (23–38) bACP: 45 (38–55) | uACP: 9 (6.4) * bACP: 15 (9.0) * | n.a. |
| O’Hara, 2020 [21] | n = 6387 | ACP: 2950 (46.2) RCP: 1445 (22.6) No Cerebral Perfusion: 1992 (31.2) | n.a. | ACP: 22 (18–25) RCP: 18 (19–22) No Cerebral Perfusion: 19 (18–21) | ACP: 35 (26–48) RCP: 33 (25–45) No Cerebral Perfusion: 26 (20-34) | ACP: PND 369 (12.5) RCP: PND 162 (11.2) No Cerebral Perfusion: PND 277 (13.9) | Risk Factors:
|
| Liu, 2020 [61] | n = 321 | uACP: 124 (38.6) bACP: 197 (61.4) | uACP: 5 (4.0) bACP: 11 (5.6) | uACP: 25 ± 0 bACP: 27 ± 1 | uACP: 27 ± 7 bACP: 26 ± 6 | uACP: PND 22 (17.7), TND 32 (25.8) bACP: PND 16 (8.1), TND 31 (15.7) | Risk Factors:
|
| Dong, 2020 [51] | n = 61 | uACP: 36 (59.0) bACP: 25 (41.0) | n.a. | uACP: 25 ± 1 bACP: 29 ± 1 | uACP: 29 ± 5 bACP: 16 ± 4 | uACP: PND 3 (8.3), TND 5 (13.9) bACP: PND 0 (0.0), TND 2 (8.0) | n.a. |
| Dumfarth, 2018 [14] | n = 303 | ACP: 202 (66.7) RCP: 45 (14.9) DHCA: 46 (15.2) Without: 10 (3.2) | Total: 17 (5.6) | Total: 21 ± 4 | Total: 45 ± 21 | Total: PND: 48 (15.8) | Risk Factors:
|
| Furukawa, 2017 [81] | n = 137 | ACP: 137 (100.0) | Total: 12 (8.8) | Total: 22–28 (n.a.) | n.a. | Total: PND: 4 (2.9) | Risk Factors:
|
| Keeling, 2017 [48] | n = 342 | uACP: 342 (100.0) | n.a. | Total: 26 ± 3 | Total: 39 ± 19 | Total: PND: 25 (7.3) TND: 20 (5.8) | n.a. |
| Zierer, 2017 [71] | n = 453 | uACP: 298 (66.0) bACP: 155 (34) | Total: 33 (7.0) | Total: 29 ± 1 | Total: 46 ± 23 | Total: PND: 27 (6.0) TND: 31 (7.0) | n.a. |
| Tong, 2017 [56] | n = 203 | uACP: 82 (40.4) bACP: 121 (59.6) | uACP: 4 (4.9) bACP: 5 (5.8) | uACP: 24 ± 1 bACP: 24 ± 1 | uACP: 23 ± 9 bACP: 24 ± 8 | uACP: PND 11 (16.9), TND 6 (9.2) bACP: PND 9 (8.4), TND 5 (4.7) | Risk Factors:
|
| Stamou, 2016 [42] | n = 324 | ACP: 84 (25.9) RCP: 55 (17.0) DHCA: 184 (56.8) | n.a. | ACP: 19 (8–26) RCP: 17 (10–20) DHCA: 19 (10–32) | ACP: 31 (0–71) RCP: 36 (4–61) DHCA: 17 (0–146) | ACP: 12 (14.3) * RCP: 12 (21.8) * DHCA: 26 (14.1) * | n.a. |
| Preventza, 2015 [49] | n = 157 | uACP: 90 (57.3) bACP: 63 (40.1) | uACP: 16 (18.6) bACP: 17 (27.9) | Total: 22–24 (n.a.) | uACP: 34 ± 11 bACP:46 ± 27 | uACP: PND 12 (13.6), TND 10 (11.4) bACP: PND 7 (11.3), TND 5 (8.2) | Risk Factors:
|
| Tokuda, 2014 [43] | n = 4128 | ACP: 2769 (67.1) RCP: 1359 (32.9) | n.a. | ACP: 25 ± 3 RCP: 23 ± 3 | n.a. | ACP: PND 311 (11.2), TND 121 (4.4) RCP: PND 132 (9.7), TND 61 (4.5) | n.a. |
| Wiedemann, 2013 [20] | n = 329 | ACP: 91 (27.7) RCP: 122 (37.0) DHCA: 116 (35.3) | ACP: 3 (3.3) RCP: 9 (7.4) DHCA: 8 (6.9) | ACP: 25 (n.a.) RCP: 18 (n.a.) DHCA: 18 (n.a.) | ACP: 30 (14–92) RCP: 30 (14–88) DHCA: 36 (12-88) | ACP: PND 11 (12) RCP: PND 15 (12) DHCA: PND 27 (23) | n.a. |
| Sugiura, 2012 [44] | n = 203 | ACP: 94 (46.3) RCP: 109 (53.7) | ACP: 3 (3.2) RCP: 1 (0.9) | ACP: 26 ± 1 RCP: 24 ± 1 | ACP:65 ± 15 RCP: 53 ± 16 | ACP: PND 11 (12.0), TND 32 (34) RCP: PND 10 (9.2), TND 41 (38) | n.a. |
| Lu, 2012 [54] | n = 263 | uACP: 135 (51.3) bACP: 128 (48.7) | n.a. | uACP: 16 ± 2 bACP: 18 ± 2 | uACP: 35 ± 15 bACP: 32 ± 14 | uACP: PND 14 (10.4), TND 9 (6.7) bACP: PND 16 (12.5), TND 7 (5.5) | n.a. |
| Krüger, 2011 [18] | n = 1558 | uACP: 628 (40.3) bACP: 453 (29.1) RCP: 34 (2.2) DHCA: 355 (22.8) Without: 88 (5.6) | uACP: 107 (17.0) bACP: 106 (23.4) DHCA: 76 (21.4) | n.a. | uACP: 32 ± 18 bACP: 38 ± 24 DHCA: 23 ± 14 | uACP: 79 (12.6) * bACP: 64 (14.1) * DHCA: 53 (15) * | n.a. |
References
- Pitts, L.; Montagner, M.; Kofler, M.; Van Praet, K.; Heck, R.; Buz, S.; Kurz, S.; Sündermann, S.; Hommel, M.; Falk, V.; et al. State of the Art Review: Surgical Treatment of Acute Type A Aortic Dissection. Surg. Technol. Int. 2021, 38. [Google Scholar] [CrossRef]
- Pitts, L.; Van Praet, K.M.; Montagner, M.; Kofler, M.; Falk, V.; Kempfert, J. David Procedure as Valve-Sparing Root Replacement. Surg. Technol. Int. 2022, 41. [Google Scholar] [CrossRef] [PubMed]
- Kurz, S.; Falk, V.; Kempfert, J.; Gieb, M.; Ruschinski, T.; Kukucka, M.; Tsokos, M.; Grubitzsch, H.; Herbst, H.; Semmler, J.; et al. Insight into the incidence of acute aortic dissection in the German region of Berlin and Brandenburg. Int. J. Cardiol. 2017, 241, 326–329. [Google Scholar] [CrossRef]
- Karck, M.; Conzelmann, L.; Easo, J.; Krüger, T.; Rylski, B.; Weigang, E.; Boening, A. German Registry for Acute Aortic Dissection Type A: Structure, Results, and Future Perspectives. Thorac. Cardiovasc. Surg. 2016, 65, 077–084. [Google Scholar] [CrossRef] [PubMed]
- Gasser, S.; Stastny, L.; Kofler, M.; Krapf, C.; Bonaros, N.; Grimm, M.; Dumfarth, J. Rapid Response in Type A Aortic Dissection: Is There a Decisive Time Interval for Surgical Repair? Thorac. Cardiovasc Surg. 2021, 69, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Gasser, S.; Stastny, L.; Kofler, M.; Zujs, V.; Krapf, C.; Semsroth, S.; Ströhle, M.; Grimm, M.; Dumfarth, J. Surgery out of office hours for type A aortic dissection: Does night-time and weekend surgery worsen outcome? Interact. Cardiovasc. Thorac. Surg. 2020, 31, 806–812. [Google Scholar] [CrossRef] [PubMed]
- Zaschke, L.; Habazettl, H.; Thurau, J.; Matschilles, C.; Göhlich, A.; Montagner, M.; Falk, V.; Kurz, S.D. Acute type A aortic dissection: Aortic Dissection Detection Risk Score in emergency care–surgical delay because of initial misdiagnosis. Eur. Hear. J. Acute Cardiovasc. Care 2020, 9, S40–S47. [Google Scholar] [CrossRef] [PubMed]
- Matschilles, C.; Mochmann, H.-C.; Syrmas, G.; Zaschke, L.; Kurz, S. Interhospital transfer of patients suffering from acute aortic dissection by helicopter and ground-based emergency medical services. Resuscitation 2018, 130, e136. [Google Scholar] [CrossRef]
- Isselbacher, E.M.; Preventza, O.; Black, I.J.H.; Augoustides, J.G.; Beck, A.W.; Bolen, M.A.; Braverman, A.C.; Bray, B.E.; Brown-Zimmerman, M.M.; Chen, E.P.; et al. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation 2022, 146, e334–e482. [Google Scholar] [CrossRef]
- Dumfarth, J.; Peterss, S.; Luehr, M.; Etz, C.D.; Schachner, T.; Kofler, M.; Ziganshin, B.A.; Ulmer, H.; Grimm, M.; Elefteriades, J.A.; et al. Acute type A dissection in octogenarians: Does emergency surgery impact in-hospital outcome or long-term survival? Eur J Cardiothorac Surg. 2017, 51, 472–477. [Google Scholar] [CrossRef]
- Dumfarth, J.; Peterss, S.; Kofler, M.; Plaikner, M.; Ziganshin, B.A.; Schachner, T.; Tranquilli, M.; Grimm, M.; Elefteriades, J.A. In DeBakey Type I Aortic Dissection, Bovine Aortic Arch Is Associated With Arch Tears and Stroke. Ann. Thorac. Surg. 2017, 104, 2001–2008. [Google Scholar] [CrossRef] [PubMed]
- Dumfarth, J.; Kofler, M.; Stastny, L.; Gasser, S.; Plaikner, M.; Semsroth, S.; Krapf, C.; Schachner, T.; Bonaros, N.; Grimm, M. Immediate surgery in acute type A dissection and neurologic dysfunction: Fighting the inevitable? Ann. Thorac. Surg. 2020, 110, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Gasser, S.; Stastny, L.; Kofler, M.; Krapf, C.; Bonaros, N.; Grimm, M.; Dumfarth, J. Type A aortic dissection is more aggressive in women. Eur. J. Cardio-Thoracic Surg. 2022, 62, ezac040. [Google Scholar] [CrossRef]
- Dumfarth, J.; Kofler, M.; Stastny, L.; Plaikner, M.; Krapf, C.; Semsroth, S.; Grimm, M. Stroke after emergent surgery for acute type A aortic dissection: Predictors, outcome and neurological recovery†. Eur. J. Cardio-Thoracic Surg. 2018, 53, 1013–1020. [Google Scholar] [CrossRef] [PubMed]
- Weigang, E.; Czerny, M.; Zierer, A.; Khaladj, N.; Schoenhoff, F.; Carrel, T.P.; Blettner, M.; Hoffmann, I.; Etz, C.; Englberger, L. The Impact of Pre-Operative Malperfusion on Outcome in Acute Type A Aortic Dissection: Results From the GERAADA Registry. J. Am. Coll. Cardiol. 2015, 65, 2628–2635. [Google Scholar] [CrossRef]
- Gega, A.; Rizzo, J.A.; Johnson, M.H.; Tranquilli, M.; Farkas, E.A.; Elefteriades, J.A. Straight Deep Hypothermic Arrest: Experience in 394 Patients Supports Its Effectiveness as a Sole Means of Brain Preservation. Ann. Thorac. Surg. 2007, 84, 759–767. [Google Scholar] [CrossRef]
- Svensson, L.G.; Crawford, E.S.; Hess, K.R.; Coselli, J.S.; Raskin, S.; A Shenaq, S.; Safi, H.J. Deep hypothermia with circulatory arrest. Determinants of stroke and early mortality in 656 patients. J. Thorac. Cardiovasc. Surg. 1993, 106, 19–28. [Google Scholar] [CrossRef]
- Kruger, T.; Weigang, E.; Hoffmann, I.; Blettner, M.; Aebert, H. Cerebral protection during surgery for acute aortic dissection type A: Results of the German Registry for Acute Aortic Dissection Type A (GERAADA). Circulation 2011, 124, 434–443. [Google Scholar] [CrossRef]
- Czerny, M.; Fleck, T.; Zimpfer, D.; Dworschak, M.; Hofmann, W.; Hutschala, D.; Dunkler, D.; Ehrlich, M.; Wolner, E.; Grabenwoger, M. Risk factors of mortality and permanent neurologic injury in patients undergoing ascending aortic and arch repair. J. Thorac. Cardiovasc. Surg. 2003, 126, 1296–1301. [Google Scholar] [CrossRef]
- Wiedemann, D.; Kocher, A.; Dorfmeister, M.; Vadehra, A.; Mahr, S.; Laufer, G.; Ehrlich, M. Effect of cerebral protection strategy on outcome of patients with Stanford type A aortic dissection. J. Thorac. Cardiovasc. Surg. 2013, 146, 647–655.e1. [Google Scholar] [CrossRef]
- O’Hara, D.; McLarty, A.; Sun, E.; Itagaki, S.; Tannous, H.; Chu, D.; Egorova, N.; Chikwe, J. Type-A Aortic Dissection and Cerebral Perfusion: The Society of Thoracic Surgeons Database Analysis. Ann. Thorac. Surg. 2020, 110, 1461–1467. [Google Scholar] [CrossRef] [PubMed]
- Benedetto, U.; Dimagli, A.; Cooper, G.; Uppal, R.; Mariscalco, G.; Krasopoulos, G.; Goodwin, A.; Trivedi, U.; Kendall, S.; Sinha, S.; et al. Neuroprotective strategies in acute aortic dissection: An analysis of the UK National Adult Cardiac Surgical Audit. Eur. J. Cardio-Thoracic Surg. 2021, 60, 1437–1444. [Google Scholar] [CrossRef] [PubMed]
- Safi, H.J.; Letsou, G.V.; Iliopoulos, D.C.; Subramaniam, M.H.; Miller, C.C., 3rd; Hassoun, H.; Asimacopoulos, P.J.; Baldwin, J.C. Impact of retrograde cerebral perfusion on ascending aortic and arch aneurysm repair. Ann. Thorac. Surg. 1997, 63, 1601–1607. [Google Scholar] [CrossRef] [PubMed]
- Estrera, A.L.; Miller, C.C.; 3rd Lee, T.Y.; Shah, P.; Safi, H.J. Ascending and transverse aortic arch repair: The impact of retrograde cerebral perfusion. Circulation 2008, 118 (Suppl. 14), S160–S166. [Google Scholar] [CrossRef] [PubMed]
- Okita, Y.; Takamoto, S.; Ando, M.; Morota, T.; Matsukawa, R.; Kawashima, Y. Mortality And Cerebral Outcome In Patients Who Underwent Aortic Arch Operations Using Deep Hypothermic Circulatory Arrest With Retrograde Cerebral Perfusion: No Relation Of Early Death, Stroke, And Delirium To The Duration Of Circulatory Arrest. J. Thorac. Cardiovasc. Surg. 1998, 115, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Ueda, Y.; Okita, Y.; Aomi, S.; Koyanagi, H.; Takamoto, S. Retrograde cerebral perfusion for aortic arch surgery: Analysis of risk factors. Ann. Thorac. Surg. 1999, 67, 1879–1882. [Google Scholar] [CrossRef]
- Bonser, R.; Wong, C.; Harrington, D.; Pagano, D.; Wilkes, M.; Clutton-Brock, T.; Faroqui, M. Failure of retrograde cerebral perfusion to attenuate metabolic changes associated with hypothermic circulatory arrest. J. Thorac. Cardiovasc. Surg. 2002, 123, 943–950. [Google Scholar] [CrossRef]
- Yerlioglu, M.; Wolfe, D.; Mezrow, C.K.; Weisz, D.J.; Midulla, P.S.; Zhang, N.; Shiand, H.H.; Bodian, C.; Griepp, R.B. The effect of retrograde cerebral perfusion after particulate embolization to the brain. J. Thorac. Cardiovasc. Surg. 1995, 110, 1470–1485. [Google Scholar] [CrossRef]
- Mills, N.L.; Ochsner, J.L. Massive air embolism during cardiopulmonary bypass. Causes, prevention, and management. J. Thorac. Cardiovasc. Surg. 1980, 80, 708–717. [Google Scholar] [CrossRef]
- Estrera, A.L.; Miller, C.C.; Lee, T.-Y.; Shah, P.; Irani, A.D.; Ganim, N.; Abdullah, S.; Safi, H.J. Integrated cerebral perfusion for hypothermic circulatory arrest during transverse aortic arch repairs☆. Eur. J. Cardio-Thoracic Surg. 2010, 38, 293–298. [Google Scholar] [CrossRef]
- Tian, D.H.; Weller, J.; Hasmat, S.; Oo, A.; Forrest, P.; Kiat, H.; Yan, T.D. Adjunct retrograde cerebral perfusion provides superior outcomes compared with hypothermic circulatory arrest alone: A meta-analysis. J. Thorac. Cardiovasc. Surg. 2018, 156, 1339–1348.e7. [Google Scholar] [CrossRef] [PubMed]
- Ghoreishi, M.; Sundt, T.M.; Cameron, D.E.; Holmes, S.D.; Roselli, E.E.; Pasrija, C.; Gammie, J.S.; Patel, H.J.; Bavaria, J.E.; Svensson, L.G.; et al. Factors associated with acute stroke after type A aortic dissection repair: An analysis of the Society of Thoracic Surgeons National Adult Cardiac Surgery Database. J. Thorac. Cardiovasc. Surg. 2019, 159, 2143–2154.e3. [Google Scholar] [CrossRef] [PubMed]
- Usui, A.; Abe, T.; Murase, M. Early clinical results of retrograde cerebral perfusion for aortic arch operations in Japan. Ann. Thorac. Surg. 1996, 62, 94–104. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, A.; Chehadi, M.; Smith, H.N.; Hassan, M.; Sandhu, H.K.; Miller, C.C., 3rd; Safi, H.J.; Estrera, A.L. Deep Hypothermic Circulatory Arrest With Retrograde Cerebral Perfusion: How Long Is Safe? Ann. Thorac. Surg. 2022; Online ahead of print. [Google Scholar]
- Filgueiras, C.L.; Ryner, L.; Ye, J.; Yang, L.; Ede, M.; Sun, J.; Kozlowski, P.; Summers, R.; Saunders, J.K.; Salerno, T.A.; et al. Cerebral protection during moderate hypothermic circulatory arrest: Histopathology and magnetic resonance spectroscopy of brain energetics and intracellular pH in pigs. J. Thorac. Cardiovasc. Surg. 1996, 112, 1073–1080. [Google Scholar] [CrossRef] [PubMed]
- Zierer, A.; Aybek, T.; Risteski, P.; Dogan, S.; Wimmer-Greinecker, G.; Moritz, A. Moderate hypothermia (30 degrees C) for surgery of acute type A aortic dissection. Thorac. Cardiovasc. Surg. 2005, 53, 74–79. [Google Scholar] [CrossRef]
- Nakahara, Y.; Tsukioka, Y.; Tateishi, R.; Ono, S.; Shioya, M.; Itoda, Y.; Kanemura, T. Safety of retrograde cerebral perfusion under moderate hypothermia for hemiarch replacement. Gen. Thorac. Cardiovasc. Surg. 2022, 70, 842–849. [Google Scholar] [CrossRef]
- Montagner, M.; Kofler, M.; Pitts, L.; Heck, R.; Buz, S.; Kurz, S.; Falk, V.; Kempfert, J. Matched comparison of 3 cerebral perfusion strategies in open zone-0 anastomosis for acute type A aortic dissection. Eur. J. Cardio-Thoracic. Surg. 2022, 62, ezac214. [Google Scholar] [CrossRef]
- Samanidis, G.; Kanakis, M.; Khoury, M.; Balanika, M.; Antoniou, T.; Giannopoulos, N.; Stavridis, G.; Perreas, K. Antegrade and Retrograde Cerebral Perfusion During Acute Type A Aortic Dissection Repair in 290 Patients. Hear. Lung Circ. 2021, 30, 1075–1083. [Google Scholar] [CrossRef]
- Sun, S.; Chien, C.-Y.; Fan, Y.-F.; Wu, S.-J.; Li, J.-Y.; Tan, Y.-H.; Hsu, K.-H. Retrograde cerebral perfusion for surgery of type A aortic dissection. Asian J. Surg. 2021, 44, 1529–1534. [Google Scholar] [CrossRef]
- Xue, Y.; Liu, C.; Mi, L.; Chen, Y.; Wang, D. Risk factors for cerebral complications after type A aortic dissection surgery: Single center’s experience. Ann. Palliat. Med. 2021, 10, 7458–7467. [Google Scholar] [CrossRef]
- Stamou, S.C.; Rausch, L.A.; Kouchoukos, N.T.; Lobdell, K.W.; Khabbaz, K.; Murphy, E.; Hagberg, R.C. Comparison between antegrade and retrograde cerebral perfusion or profound hypothermia as brain protection strategies during repair of type A aortic dissection. Ann. Cardiothorac. Surg. 2016, 5, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Tokuda, Y.; Miyata, H.; Motomura, N.; Oshima, H.; Usui, A.; Takamoto, S.; Japan Adult Cardiovascular Database Organization. Brain Protection During Ascending Aortic Repair for Stanford Type A Acute Aortic Dissection Surgery. Circ. J. 2014, 78, 2431–2438. [Google Scholar] [CrossRef] [PubMed]
- Sugiura, T.; Imoto, K.; Uchida, K.; Minami, T.; Yasuda, S. Comparative study of brain protection in ascending aorta replacement for acute type A aortic dissection: Retrograde cerebral perfusion versus selective antegrade cerebral perfusion. Gen. Thorac. Cardiovasc. Surg. 2012, 60, 645–648. [Google Scholar] [CrossRef] [PubMed]
- Svensson, L.G.; Blackstone, E.H.; Apperson-Hansen, C.; Ruggieri, P.M.; Ainkaran, P.; Naugle, R.I.; Lima, B.; Roselli, E.E.; Cooper, M.; Somogyi, D.; et al. Implications from neurologic assessment of brain protection for total arch replacement from a randomized trial. J. Thorac. Cardiovasc. Surg. 2015, 150, 1140–1147.e11. [Google Scholar] [CrossRef] [PubMed]
- De Paulis, R.; Czerny, M.; Weltert, L.; Bavaria, J.; Borger, M.A.; Carrel, T.P.; Etz, C.D.; Grimm, M.; Loubani, M.; Pacini, D.; et al. Current trends in cannulation and neuroprotection during surgery of the aortic arch in Europe. Eur. J. Cardiothorac. Surg. 2015, 47, 917–923. [Google Scholar] [CrossRef] [PubMed]
- El-Sayed Ahmad, A.; Papadopoulos, N.; Risteski, P.; Hack, T.; Ay, M.; Moritz, A.; Zierer, A. Is More than One Hour of Selective Antegrade Cerebral Perfusion in Moderate-to-Mild Systemic Hypothermic Circulatory Arrest for Surgery of Acute Type A Aortic Dissection Safe? Thorac. Cardiovasc. Surg. 2018, 66, 215–221. [Google Scholar]
- Keeling, W.B.; Leshnower, B.G.; Hunting, J.C.; Binongo, J.; Chen, E.P. Hypothermia and Selective Antegrade Cerebral Perfusion Is Safe for Arch Repair in Type A Dissection. Ann. Thorac. Surg. 2017, 104, 767–772. [Google Scholar] [CrossRef]
- Preventza, O.; Simpson, K.H.; Cooley, D.A.; Cornwell, L.; Bakaeen, F.G.; Omer, S.; Rodriguez, V.; de la Cruz, K.I.; Rosengart, T.; Coselli, J.S. Unilateral Versus Bilateral Cerebral Perfusion for Acute Type A Aortic Dissection. Ann. Thorac. Surg. 2015, 99, 80–87. [Google Scholar] [CrossRef]
- Song, S.J.; Kim, W.K.; Kim, T.H.; Song, S.W. Unilateral versus bilateral antegrade cerebral perfusion during surgical repair for patients with acute type A aortic dissection. JTCVS Open 2022, 11, 37–48. [Google Scholar] [CrossRef]
- Dong, S.-B.; Xiong, J.-X.; Zhang, K.; Zheng, J.; Xu, S.-D.; Liu, Y.-M.; Sun, L.-Z.; Pan, X.-D. Different hypothermic and cerebral perfusion strategies in extended arch replacement for acute type a aortic dissection: A retrospective comparative study. J. Cardiothorac. Surg. 2020, 15, 1–8. [Google Scholar] [CrossRef]
- Angleitner, P.; Stelzmueller, M.-E.; Mahr, S.; Kaider, A.; Laufer, G.; Ehrlich, M. Bilateral or unilateral antegrade cerebral perfusion during surgery for acute type A dissection. J. Thorac. Cardiovasc. Surg. 2020, 159, 2159–2167.e2. [Google Scholar] [CrossRef] [PubMed]
- Norton, E.L.; Wu, X.; Kim, K.M.; Patel, H.J.; Deeb, G.M.; Yang, B. Unilateral is comparable to bilateral antegrade cerebral perfusion in acute type A aortic dissection repair. J. Thorac. Cardiovasc. Surg. 2019, 160, 617–625.e5. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.; Sun, X.; Hong, T.; Yang, S.; Song, K.; Lai, H.; Hu, K.; Wang, C. Bilateral Versus Unilateral Antegrade Cerebral Perfusion in Arch Reconstruction for Aortic Dissection. Ann. Thorac. Surg. 2012, 93, 1917–1920. [Google Scholar] [CrossRef]
- Piperata, A.; Watanabe, M.; Pernot, M.; Metras, A.; Kalscheuer, G.; Avesani, M.; Barandon, L.; Peltan, J.; Lorenzoni, G.; Jorgji, V.; et al. Unilateral versus bilateral cerebral perfusion during aortic surgery for acute type A aortic dissection: A multicentre study. Eur. J. Cardio-Thoracic Surg. 2021, 61, 828–835. [Google Scholar] [CrossRef] [PubMed]
- Tong, G.; Zhang, B.; Zhou, X.; Tao, Y.; Yan, T.; Wang, X.; Lu, H.; Sun, Z.; Zhang, W. Bilateral versus unilateral antegrade cerebral perfusion in total arch replacement for type A aortic dissection. J. Thorac. Cardiovasc. Surg. 2017, 154, 767–775. [Google Scholar] [CrossRef] [PubMed]
- Papantchev, V.; Stoinova, V.; Aleksandrov, A.; Todorova-Papantcheva, D.; Hristov, S.; Petkov, D.; Nachev, G.; Ovtscharoff, W. The role of Willis circle variations during unilateral selective cerebral perfusion: A study of 500 circles. Eur. J. Cardio-Thoracic Surg. 2013, 44, 743–753. [Google Scholar] [CrossRef] [PubMed]
- Urbanski, P.P.; Lenos, A.; Blume, J.C.; Ziegler, V.; Griewing, B.; Schmitt, R.; Diegeler, A.; Dinkel, M. Does anatomical completeness of the circle of Willis correlate with sufficient cross-perfusion during unilateral cerebral perfusion? Eur. J. Cardiothorac. Surg. 2008, 33, 402–408. [Google Scholar] [CrossRef]
- Urbanski, P.P.; Thamm, T.; Bougioukakis, P.; Irimie, V.; Prasad, P.; Diegeler, A.; Lenos, A. Efficacy of unilateral cerebral perfusion for brain protection in aortic arch surgery. J. Thorac. Cardiovasc. Surg. 2019, 159, 365–371.e1. [Google Scholar] [CrossRef]
- Angeloni, E.; Melina, G.; Refice, S.K.; Roscitano, A.; Capuano, F.; Comito, C.; Sinatra, R. Unilateral Versus Bilateral Antegrade Cerebral Protection During Aortic Surgery: An Updated Meta-Analysis. Ann. Thorac. Surg. 2015, 99, 2024–2031. [Google Scholar] [CrossRef]
- Liu, Z.; Wang, C.; Zhang, X.; Wu, S.; Fang, C.; Pang, X. Effect of different types of cerebral perfusion for acute type A aortic dissection undergoing aortic arch procedure, unilateral versus bilateral. BMC Surg. 2020, 20, 1–8. [Google Scholar] [CrossRef]
- Berger, T.; Kreibich, M.; Mueller, F.; Breurer-Kellner, L.; Rylski, B.; Kondov, S.; Schröfel, H.; Pingpoh, C.; Beyersdorf, F.; Siepe, M.; et al. Risk factors for stroke after total aortic arch replacement using the frozen elephant trunk technique. Interact. Cardiovasc. Thorac. Surg. 2022, 34, 865–871. [Google Scholar] [CrossRef] [PubMed]
- Etz, C.D.; von Aspern, K.; Silva, J.D.R.E.; Girrbach, F.F.; Leontyev, S.; Luehr, M.; Misfeld, M.; Borger, M.; Mohr, F.W. Impact of Perfusion Strategy on Outcome After Repair for Acute Type A Aortic Dissection. Ann. Thorac. Surg. 2014, 97, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-H.; Lee, S.H.; Lee, S.; Youn, Y.-N.; Yoo, K.-J.; Joo, H.-C. Axillary artery cannulation reduces early embolic stroke and mortality after open arch repair with circulatory arrest. J. Thorac. Cardiovasc. Surg. 2019, 159, 772–778.e4. [Google Scholar] [CrossRef] [PubMed]
- Hussain, A.; Uzzaman, M.; Mohamed, S.; Khan, F.; Butt, S.; Khan, H. Femoral versus axillary cannulation in acute type A aortic dissections: A meta-analysis. J. Card. Surg. 2021, 36, 3761–3769. [Google Scholar] [CrossRef] [PubMed]
- Rylski, B.; Czerny, M.; Beyersdorf, F.; Kari, F.A.; Siepe, M.; Adachi, H.; Yamaguchi, A.; Itagaki, R.; Kimura, N. Is right axillary artery cannulation safe in type A aortic dissection with involvement of the innominate artery? J. Thorac. Cardiovasc. Surg. 2016, 152, 801–807.e1. [Google Scholar] [CrossRef]
- Khaladj, N.; Shrestha, M.; Peterss, S.; Strueber, M.; Karck, M.; Pichlmaier, M.; Haverich, A.; Hagl, C. Ascending aortic cannulation in acute aortic dissection type A: The Hannover experience☆☆☆. Eur. J. Cardio-Thoracic Surg. 2008, 34, 792–796. [Google Scholar] [CrossRef]
- Sicim, H.; Demirdas, E.; Bolcal, C. Direct bilateral carotid artery cannulation can be better strategy for acute aortic dissection involving both carotid arteries. J. Card. Surg. 2021, 36, 3977–3980. [Google Scholar] [CrossRef]
- Kusadokoro, S.; Kimura, N.; Hori, D.; Hattori, M.; Matsunaga, W.; Itagaki, R.; Yuri, K.; Mieno, M.; Nakamura, M.; Yamaguchi, A. Utility of double arterial cannulation for surgical repair of acute type A dissection. Eur. J. Cardio-Thoracic Surg. 2020, 57, 1068–1075. [Google Scholar] [CrossRef]
- Zhu, Y.; Lingala, B.; Baiocchi, M.; Tao, J.J.; Toro Arana, V.; Khoo, J.W.; Williams, K.M.; Traboulsi, A. A-R.; Hammond, H.C.; Lee, A.M.; et al. Type A Aortic Dissection-Experience Over 5 Decades: JACC Historical Breakthroughs in Perspective. J. Am. Coll. Cardiol. 2020, 76, 1703–1713. [Google Scholar] [CrossRef]
- Zierer, A.; Ahmad, A.E.-S.; Papadopoulos, N.; Detho, F.; Risteski, P.; Moritz, A.; Diegeler, A.; Urbanski, P.P. Fifteen years of surgery for acute type A aortic dissection in moderate-to-mild systemic hypothermia†. Eur. J. Cardio-Thoracic Surg. 2016, 51, 97–103. [Google Scholar] [CrossRef]
- Leshnower, B.G.; Thourani, V.H.; Halkos, M.E.; Sarin, E.L.; Keeling, W.B.; Lamias, M.J.; Guyton, R.A.; Chen, E.P. Moderate Versus Deep Hypothermia With Unilateral Selective Antegrade Cerebral Perfusion for Acute Type A Dissection. Ann. Thorac. Surg. 2015, 100, 1563–1569. [Google Scholar] [CrossRef] [PubMed]
- Leshnower, B.G.; Myung, R.J.; Thourani, V.H.; Halkos, M.E.; Kilgo, P.D.; Puskas, J.D.; Chen, E.P. Hemiarch Replacement at 28 °C: An Analysis of Mild and Moderate Hypothermia in 500 Patients. Ann. Thorac. Surg. 2012, 93, 1910–1916. [Google Scholar] [CrossRef]
- Pupovac, S.S.; Hemli, J.M.; Bavaria, J.E.; Patel, H.J.; Trimarchi, S.; Pacini, D.; Bekeredjian, R.; Chen, E.P.; Myrmel, T.; Ouzounian, M.; et al. Moderate vs Deep Hypothermia in Type A Acute Aortic Dissection Repair: Insights from IRAD. Ann. Thorac. Surg. 2021, 112, 1893–1899. [Google Scholar] [CrossRef] [PubMed]
- Etz, C.D.; Luehr, M.; Kari, F.A.; Lin, H.M.; Kleinman, G.; Zoli, S.; Plestis, K.A.; Griepp, R.B. Selective cerebral perfusion at 28 degrees C--is the spinal cord safe? Eur. J. Cardiothorac. Surg. 2009, 36, 946–955. [Google Scholar] [CrossRef]
- Kamiya, H.; Hagl, C.; Kropivnitskaya, I.; Böthig, D.; Kallenbach, K.; Khaladj, N.; Martens, A.; Haverich, A.; Karck, M. The safety of moderate hypothermic lower body circulatory arrest with selective cerebral perfusion: A propensity score analysis. J. Thorac. Cardiovasc. Surg. 2007, 133, 501–509.e2. [Google Scholar] [CrossRef] [PubMed]
- Göbölös, L.; Philipp, A.; Ugocsai, P.; Foltan, M.; Thrum, A.; Miskolczi, S.; Pousios, D.; Khawaja, S.; Budra, M.; Ohri, S. Reliability of different body temperature measurement sites during aortic surgery. Perfusion 2013, 29, 75–81. [Google Scholar] [CrossRef]
- Montagner, M.; Kofler, M.; Seeber, F.; Pitts, L.; Starck, C.; Sündermann, S.H.; Kurz, S.; Grubitzsch, H.; Falk, V.; Kempfert, J. The arch remodelling stent for DeBakey I acute aortic dissection: Experience with 100 implantations. Eur. J. Cardio-Thoracic Surg. 2022, 62, ezac384. [Google Scholar] [CrossRef]
- Krüger, T.; Hoffmann, I.; Blettner, M.; Borger, M.A.; Schlensak, C.; Weigang, E.; on behalf of the GERAADA Investigators. Intraoperative neuroprotective drugs without beneficial effects? Results of the German Registry for Acute Aortic Dissection Type A (GERAADA). Eur. J. Cardio-Thoracic Surg. 2013, 44, 939–946. [Google Scholar] [CrossRef]
- Fernández Suárez, F.E.; Fernández Del Valle, D.; González Alvarez, A.; Pérez-Lozano, B. Intraoperative care for aortic surgery using circulatory arrest. J. Thorac. Dis. 2017, 9, S508–S520. [Google Scholar] [CrossRef]
- Furukawa, T.; Uchida, N.; Takahashi, S.; Yamane, Y.; Mochizuki, S.; Yamada, K.; Mochizuki, T.; Sueda, T. Management of cerebral malperfusion in surgical repair of acute type A aortic dissection. Eur. J. Cardio-Thoracic Surg. 2017, 52, 327–332. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pitts, L.; Kofler, M.; Montagner, M.; Heck, R.; Iske, J.; Buz, S.; Kurz, S.D.; Starck, C.; Falk, V.; Kempfert, J. Cerebral Protection Strategies and Stroke in Surgery for Acute Type A Aortic Dissection. J. Clin. Med. 2023, 12, 2271. https://doi.org/10.3390/jcm12062271
Pitts L, Kofler M, Montagner M, Heck R, Iske J, Buz S, Kurz SD, Starck C, Falk V, Kempfert J. Cerebral Protection Strategies and Stroke in Surgery for Acute Type A Aortic Dissection. Journal of Clinical Medicine. 2023; 12(6):2271. https://doi.org/10.3390/jcm12062271
Chicago/Turabian StylePitts, Leonard, Markus Kofler, Matteo Montagner, Roland Heck, Jasper Iske, Semih Buz, Stephan Dominik Kurz, Christoph Starck, Volkmar Falk, and Jörg Kempfert. 2023. "Cerebral Protection Strategies and Stroke in Surgery for Acute Type A Aortic Dissection" Journal of Clinical Medicine 12, no. 6: 2271. https://doi.org/10.3390/jcm12062271
APA StylePitts, L., Kofler, M., Montagner, M., Heck, R., Iske, J., Buz, S., Kurz, S. D., Starck, C., Falk, V., & Kempfert, J. (2023). Cerebral Protection Strategies and Stroke in Surgery for Acute Type A Aortic Dissection. Journal of Clinical Medicine, 12(6), 2271. https://doi.org/10.3390/jcm12062271