Predicting the Absolute Risk of Ischemic Stroke in Asian Patients with Atrial Fibrillation: Comparing the COOL-AF Risk Score with CARS/mCARS Models for Absolute Risk and the CHA2DS2-VASc Score



Abstract
1. Introduction
2. Methods
2.1. Study Population
2.2. Study Protocol
2.3. Data Collection
2.4. Outcomes
2.5. Prediction of the Risk of SSE
2.6. Statistical Analysis
Model Validation
3. Results
3.1. Study Population and Outcomes
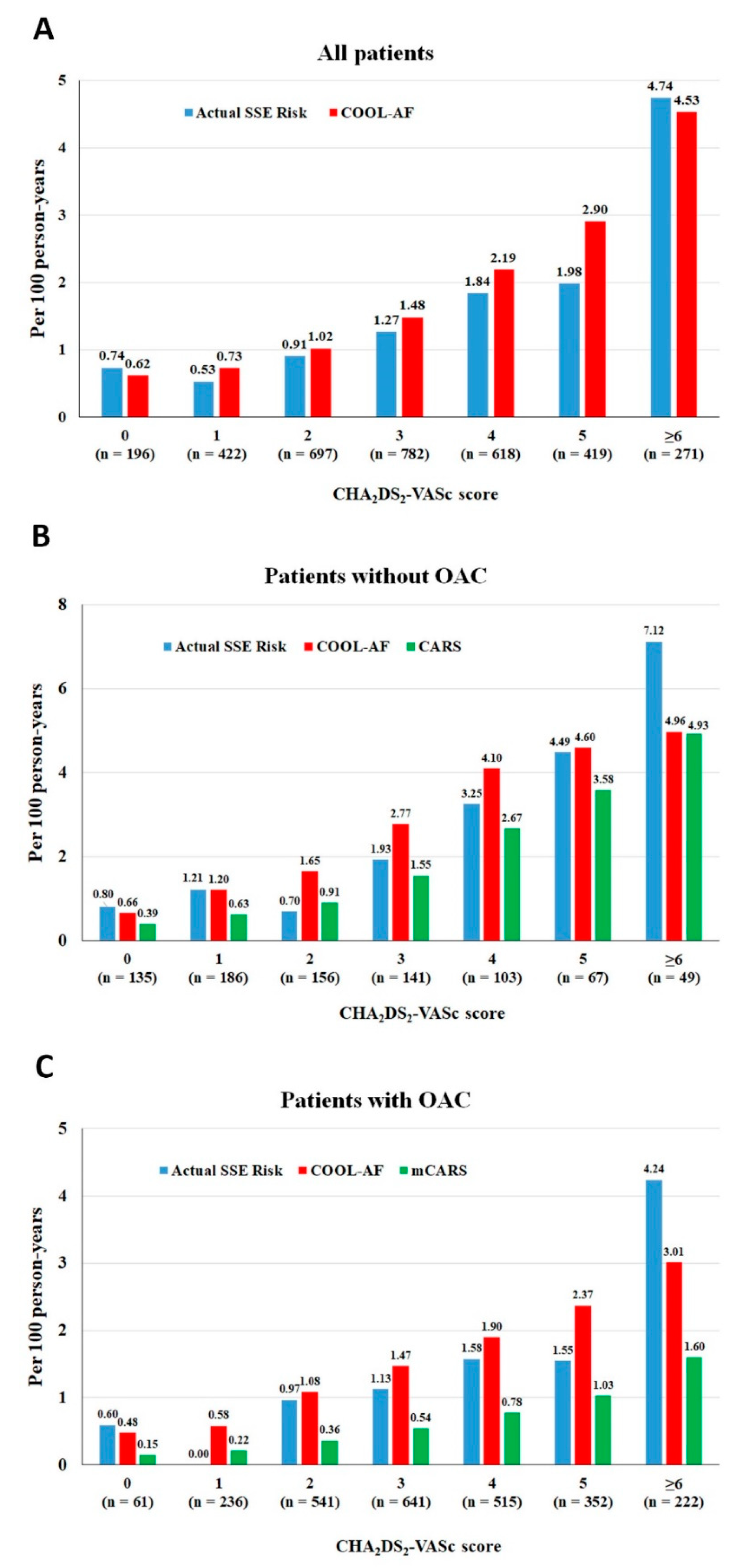
3.2. SSE Risk According to the COOL-AF Model, CARS, mCARS, and CHA2DS2-VASc Scores
3.3. Comparisons of the COOL-AF Model, CARS, mCARS, and CHA2DS2-VASc Scores
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Friberg, L.; Rosenqvist, M.; Lip, G.Y. Evaluation of risk stratification schemes for ischaemic stroke and bleeding in 182,678 patients with atrial fibrillation: The Swedish Atrial Fibrillation cohort study. Eur. Heart J. 2012, 33, 1500–1510. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomstrom-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2020, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- January, C.T.; Wann, L.S.; Calkins, H.; Chen, L.Y.; Cigarroa, J.E.; Cleveland, J.C., Jr.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; Furie, K.L.; et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients with Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J. Am. Coll. Cardiol. 2019, 74, 104–132. [Google Scholar] [CrossRef]
- Lip, G.Y.H.; Banerjee, A.; Boriani, G.; Chiang, C.E.; Fargo, R.; Freedman, B.; Lane, D.A.; Ruff, C.T.; Turakhia, M.; Werring, D.; et al. Antithrombotic Therapy for Atrial Fibrillation: CHEST Guideline and Expert Panel Report. Chest 2018, 154, 1121–1201. [Google Scholar] [CrossRef]
- Chao, T.F.; Joung, B.; Takahashi, Y.; Lim, T.W.; Choi, E.K.; Chan, Y.H.; Guo, Y.; Sriratanasathavorn, C.; Oh, S.; Okumura, K.; et al. 2021 Focused Update Consensus Guidelines of the Asia Pacific Heart Rhythm Society on Stroke Prevention in Atrial Fibrillation: Executive Summary. Thromb. Haemost. 2022, 122, 20–47. [Google Scholar] [CrossRef] [PubMed]
- Lip, G.Y.; Nieuwlaat, R.; Pisters, R.; Lane, D.A.; Crijns, H.J. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: The euro heart survey on atrial fibrillation. Chest 2010, 137, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Eckman, M.H.; Singer, D.E.; Rosand, J.; Greenberg, S.M. Moving the tipping point: The decision to anticoagulate patients with atrial fibrillation. Circ. Cardiovasc. Qual. Outcomes 2011, 4, 14–21. [Google Scholar] [CrossRef]
- Ivany, E.; Lotto, R.R.; Lip, G.Y.H.; Lane, D.A. Managing Uncertainty: Physicians’ Decision Making for Stroke Prevention for Patients with Atrial Fibrillation and Intracerebral Hemorrhage. Thromb. Haemost. 2022, 122, 1603–1611. [Google Scholar] [CrossRef]
- Wankowicz, P.; Staszewski, J.; Debiec, A.; Nowakowska-Kotas, M.; Szylinska, A.; Rotter, I. Ischemic Stroke Risk Factors in Patients with Atrial Fibrillation Treated with New Oral Anticoagulants. J. Clin. Med. 2021, 10, 1223. [Google Scholar] [CrossRef]
- Lee, C.J.; Toft-Petersen, A.P.; Ozenne, B.; Phelps, M.; Olesen, J.B.; Ellinor, P.T.; Gislason, G.; Lip, G.Y.H.; Torp-Pedersen, C.; Gerds, T.A. Assessing absolute stroke risk in patients with atrial fibrillation using a risk factor-based approach. Eur. Heart J. Cardiovasc. Pharmacother. 2021, 7, f3–f10. [Google Scholar] [CrossRef]
- Ding, W.Y.; Rivera-Caravaca, J.M.; Marin, F.; Torp-Pedersen, C.; Roldan, V.; Lip, G.Y.H. Prediction of Residual Stroke Risk in Anticoagulated Patients with Atrial Fibrillation: mCARS. J. Clin. Med. 2021, 10, 3357. [Google Scholar] [CrossRef] [PubMed]
- Krittayaphong, R.; Kanjanarutjawiwat, W.; Wisaratapong, T.; Lip, G.Y.H. Improving risk prediction for death, stroke and bleeding in Asian patients with atrial fibrillation. Eur. J. Clin. Investig. 2022, 53, e13886. [Google Scholar] [CrossRef]
- Austin, P.C.; Lee, D.S.; Fine, J.P. Introduction to the Analysis of Survival Data in the Presence of Competing Risks. Circulation 2016, 133, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Wolff, R.F.; Moons, K.G.M.; Riley, R.D.; Whiting, P.F.; Westwood, M.; Collins, G.S.; Reitsma, J.B.; Kleijnen, J.; Mallett, S.; Groupdagger, P. PROBAST: A Tool to Assess the Risk of Bias and Applicability of Prediction Model Studies. Ann. Intern. Med. 2019, 170, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Van Calster, B.; On behalf of Topic Group ‘Evaluating Diagnostic Tests and Prediction Models’ of the STRATOS Initiative; McLernon, D.J.; van Smeden, M.; Wynants, L.; Steyerberg, E.W. Calibration: The Achilles heel of predictive analytics. BMC Med. 2019, 17, 230. [Google Scholar] [CrossRef]
- Riley, R.D.; Ensor, J.; Snell, K.I.; Debray, T.P.; Altman, D.G.; Moons, K.G.; Collins, G.S. External validation of clinical prediction models using big datasets from e-health records or IPD meta-analysis: Opportunities and challenges. BMJ 2016, 353, i3140. [Google Scholar] [CrossRef]
- Chao, T.F.; Lip, G.Y.; Liu, C.J.; Tuan, T.C.; Chen, S.J.; Wang, K.L.; Lin, Y.J.; Chang, S.L.; Lo, L.W.; Hu, Y.F.; et al. Validation of a Modified CHA2DS2-VASc Score for Stroke Risk Stratification in Asian Patients with Atrial Fibrillation: A Nationwide Cohort Study. Stroke 2016, 47, 2462–2469. [Google Scholar] [CrossRef]
- Chao, T.F.; Wang, K.L.; Liu, C.J.; Lin, Y.J.; Chang, S.L.; Lo, L.W.; Hu, Y.F.; Tuan, T.C.; Chung, F.P.; Liao, J.N.; et al. Age Threshold for Increased Stroke Risk Among Patients with Atrial Fibrillation: A Nationwide Cohort Study From Taiwan. J. Am. Coll. Cardiol. 2015, 66, 1339–1347. [Google Scholar] [CrossRef]
- Gorog, D.A.; Gue, Y.X.; Chao, T.F.; Fauchier, L.; Ferreiro, J.L.; Huber, K.; Konstantinidis, S.V.; Lane, D.A.; Marin, F.; Oldgren, J.; et al. Assessment and mitigation of bleeding risk in atrial fibrillation and venous thromboembolism: A Position Paper from the ESC Working Group on Thrombosis, in collaboration with the European Heart Rhythm Association, the Association for Acute CardioVascular Care and the Asia-Pacific Heart Rhythm Society. Europace 2022, 24, 1844–1871. [Google Scholar] [CrossRef]
- Kim, H.K.; Tantry, U.S.; Smith, S.C., Jr.; Jeong, M.H.; Park, S.J.; Kim, M.H.; Lim, D.S.; Shin, E.S.; Park, D.W.; Huo, Y.; et al. The East Asian Paradox: An Updated Position Statement on the Challenges to the Current Antithrombotic Strategy in Patients with Cardiovascular Disease. Thromb. Haemost. 2021, 121, 422–432. [Google Scholar] [CrossRef]
- Krittayaphong, R.; Winijkul, A.; Methavigul, K.; Wongtheptien, W.; Wongvipaporn, C.; Wisaratapong, T.; Kunjara-Na-Ayudhya, R.; Boonyaratvej, S.; Komoltri, C.; Kaewcomdee, P.; et al. Risk profiles and pattern of antithrombotic use in patients with non-valvular atrial fibrillation in Thailand: A multicenter study. BMC Cardiovasc. Disord. 2018, 18, 174. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Yang, H.L.; Gu, L.; Hui, J.; Omorogieva, O.; Ren, M.X.; Wang, X.H. Current status and factors influencing oral anticoagulant therapy among patients with non-valvular atrial fibrillation in Jiangsu province, China: A multi-center, cross-sectional study. BMC Cardiovasc. Disord. 2020, 20, 22. [Google Scholar] [CrossRef] [PubMed]
- Ruff, C.T.; Giugliano, R.P.; Braunwald, E.; Hoffman, E.B.; Deenadayalu, N.; Ezekowitz, M.D.; Camm, A.J.; Weitz, J.I.; Lewis, B.S.; Parkhomenko, A.; et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: A meta-analysis of randomised trials. Lancet 2014, 383, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Kundnani, N.R.; Rosca, C.I.; Sharma, A.; Tudor, A.; Rosca, M.S.; Nisulescu, D.D.; Branea, H.S.; Mocanu, V.; Crisan, D.C.; Buzas, D.R.; et al. Selecting the right anticoagulant for stroke prevention in atrial fibrillation. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 4499–4505. [Google Scholar] [CrossRef] [PubMed]
- Hart, R.G.; Pearce, L.A.; Aguilar, M.I. Meta-analysis: Antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann. Intern. Med. 2007, 146, 857–867. [Google Scholar] [CrossRef] [PubMed]
- Ho, C.W.; Ho, M.H.; Chan, P.H.; Hai, J.J.; Cheung, E.; Yeung, C.Y.; Lau, K.K.; Chan, K.H.; Lau, C.P.; Lip, G.Y.; et al. Ischemic stroke and intracranial hemorrhage with aspirin, dabigatran, and warfarin: Impact of quality of anticoagulation control. Stroke 2015, 46, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Litwinowicz, R.; Bartus, M.; Ceranowicz, P.; Kapelak, B.; Lakkireddy, D.; Bartus, K. Stroke risk reduction after left atrial appendage occlusion in elderly patients with atrial fibrillation: Long-term results. Pol. Arch. Intern. Med. 2018, 128, 327–329. [Google Scholar] [CrossRef]
- Litwinowicz, R.; Burysz, M.; Mazur, P.; Kapelak, B.; Bartus, M.; Lakkireddy, D.; Lee, R.J.; Malec-Litwinowicz, M.; Bartus, K. Endocardial versus epicardial left atrial appendage exclusion for stroke prevention in patients with atrial fibrillation: Midterm follow-up. J. Cardiovasc. Electrophysiol. 2021, 32, 93–101. [Google Scholar] [CrossRef]
- Vuddanda, V.L.K.; Turagam, M.K.; Umale, N.A.; Shah, Z.; Lakkireddy, D.R.; Bartus, K.; McCausland, F.R.; Velagapudi, P.; Mansour, M.; Heist, E.K. Incidence and causes of in-hospital outcomes and 30-day readmissions after percutaneous left atrial appendage closure: A US nationwide retrospective cohort study using claims data. Heart Rhythm. Off. J. Heart Rhythm. Soc. 2020, 17, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Bartus, K.; Litwinowicz, R.; Natorska, J.; Zabczyk, M.; Undas, A.; Kapelak, B.; Lakkireddy, D.; Lee, R.J. Coagulation factors and fibrinolytic activity in the left atrial appendage and other heart chambers in patients with atrial fibrillation: Is there a local intracardiac prothrombotic state? (HEART-CLOT study). Int. J. Cardiol. 2020, 301, 103–107. [Google Scholar] [CrossRef]
- Bartus, K.; Elbey, M.A.; Kanuri, S.H.; Lee, R.; Litwinowicz, R.; Natorska, J.; Zabczyk, M.; Bartus, M.; Kapelak, B.; Malecki, M.T.; et al. Metabolic effects of the left atrial appendage exclusion (the heart hormone study). J. Cardiovasc. Electrophysiol. 2022, 33, 2064–2071. [Google Scholar] [CrossRef] [PubMed]
- Bartus, K.; Kanuri, S.H.; Litwinowicz, R.; Ali Elbey, M.; Natorska, J.; Zabczyk, M.; Bartus, M.; Kapelak, B.; Gopinnathannair, R.; Garg, J.; et al. Long Term Impact of Epicardial Left Atrial Appendage Ligation on Systemic Hemostasis: Laa Homeostasis-2. J. Clin. Med. 2022, 11, 1495. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | SSE (n = 134) | No SSE (n = 3271) | p-Value |
|---|---|---|---|
| Age (years) | 73.5 ± 9.7 | 67.6 ± 11.3 | <0.001 * |
| Female gender | 73 (54.5%) | 1351 (41.3%) | 0.002 * |
| BMI (kg/m2) | 24.6 ± 4.8 | 25.2 ± 4.7 | 0.172 |
| Time after diagnosis of AF (years) | 3.8 ± 4.9 | 3.4 ± 4.3 | 0.327 |
| Atrial fibrillation | 0.504 | ||
| Paroxysmal | 39 (29.1%) | 1109 (33.9%) | |
| Persistent | 28 (20.9%) | 617 (18.9%) | |
| Permanent | 67 (50.0%) | 1545 (47.2%) | |
| Symptomatic AF | 103 (76.9%) | 2517 (76.9%) | 0.982 |
| History of heart failure | 43 (32.1%) | 870 (26.6%) | 0.160 |
| History of CAD | 26 (19.4%) | 521 (15.9%) | 0.283 |
| CIED | 14 (10.4%) | 327 (10.0%) | 0.865 |
| History of ischemic stroke/TIA | 32 (23.9%) | 560 (17.1%) | 0.043 * |
| Diabetes mellitus | 45 (33.6%) | 794 (24.3%) | 0.014 * |
| Hypertension | 109 (81.3%) | 2221 (67.9%) | 0.001 * |
| Smoking | 25 (18.7%) | 653 (20.0%) | 0.710 |
| Dyslipidemia | 77 (57.5%) | 1840 (56.3%) | 0.782 |
| Renal replacement therapy | 4 (3.0%) | 36 (1.1%) | 0.070 |
| Dementia | 1 (0.7%) | 28 (0.9%) | 0.892 |
| Systemic embolism | 3 (2.2%) | 22 (0.7%) | 0.073 |
| History of peripheral vascular disease | 6 (4.5%) | 38 (1.2%) | 0.007 * |
| History of stent use | 9 (6.7%) | 244 (7.5%) | 0.748 |
| History of CABG | 5 (3.7%) | 60 (1.8%) | 0.111 |
| History of alcohol abuse, | 5 (3.7%) | 135 (4.1%) | 0.821 |
| History of bleeding | 19 (14.2%) | 305 (9.3%) | 0.060 |
| CKD | 101 (75.4%) | 1655 (50.6%) | <0.001 * |
| Anemia | 76 (56.7%) | 1217 (37.2%) | <0.001 * |
| Anticoagulant | 92 (68.7%) | 2476 (75.4%) | 0.064 |
| Warfarin | 87 (64.9%) | 2253 (68.9%) | 0.333 |
| NOACs | 5 (3.7%) | 223 (6.8%) | 0.161 |
| CHA2DS2-VASc | n | COOL-AF (All) | COOL-AF (No OAC) | COOL-AF (OAC) | CARS (No OAC) | mCARS (OAC) | Actual SSE Risk (95% CI) | Actual SSE Risk (95% CI) (No OAC) | Actual SSE Risk (95% CI) (OAC) |
|---|---|---|---|---|---|---|---|---|---|
| 0 | 196 | 0.62 (0.11–1.59) | 0.66 (0.06–1.90) | 0.48 (0.01–2.64) | 0.39 (0.01–2.19) | 0.15 (0.01–0.80) | 0.74 (0.20–1.86) | 0.8 (0.16–2.30) | 0.6 (0.01–3.28) |
| 1 | 422 | 0.73 (0.30–1.36) | 1.2 (0.44–2.60) | 0.58 (0.16–1.48) | 0.63 (0.13–1.81) | 0.22 (0.01–1.17) | 0.53 (0.19–1.13) | 1.21 (0.44–2.60) | 0 (0.00–0.00) |
| 2 | 697 | 1.02 (0.60–1.56) | 1.65 (0.64–3.30) | 1.08 (0.61–1.73) | 0.91 (0.24–2.30) | 0.36 (0.12–0.83) | 0.91 (0.52–1.43) | 0.7 (0.14–2.01) | 0.97 (0.52–1.60) |
| 3 | 782 | 1.48 (0.97–2.06) | 2.77 (1.30–4.98) | 1.47 (0.94–2.15) | 1.55 (0.56–3.33) | 0.54 (0.25–1.03) | 1.27 (0.82–1.83) | 1.93 (0.76–3.91) | 1.13 (0.67–1.73) |
| 4 | 618 | 2.19 (1.52–3.04) | 4.1 (1.92–7.36) | 1.9 (1.21–2.76) | 2.67 (1.06–5.42) | 0.78 (0.37–1.41) | 1.84 (1.21–2.60) | 3.25 (1.38–6.31) | 1.58 (0.96–2.37) |
| 5 | 419 | 2.9 (1.96–4.09) | 4.6 (1.78–9.13) | 2.37 (1.44–3.57) | 3.58 (1.30–7.68) | 1.03 (0.46–1.92) | 1.98 (1.21–2.98) | 4.49 (1.78–9.13) | 1.55 (0.83–2.56) |
| ≥6 | 271 | 4.53 (3.03–6.51) | 4.96 (1.61–11.55) | 3.01 (1.71–4.86) | 4.93 (1.61–11.55) | 1.60 (0.69–3.15) | 4.74 (3.22–6.72) | 7.12 (3.08–14.07) | 4.24 (2.69–6.37) |
| All | 3405 | 1.76 (1.47–2.02) | 2.22 (1.60–2.88) | 1.61 (1.29–1.90) | 1.46 (0.99–2.04) | 0.66 (0.47–0.87) | 1.51 (1.26–1.78) | 1.93 (1.37–2.57) | 1.37 (1.09–1.66) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krittayaphong, R.; Winijkul, A.; Sairat, P.; Lip, G.Y.H. Predicting the Absolute Risk of Ischemic Stroke in Asian Patients with Atrial Fibrillation: Comparing the COOL-AF Risk Score with CARS/mCARS Models for Absolute Risk and the CHA2DS2-VASc Score. J. Clin. Med. 2023, 12, 2449. https://doi.org/10.3390/jcm12072449
Krittayaphong R, Winijkul A, Sairat P, Lip GYH. Predicting the Absolute Risk of Ischemic Stroke in Asian Patients with Atrial Fibrillation: Comparing the COOL-AF Risk Score with CARS/mCARS Models for Absolute Risk and the CHA2DS2-VASc Score. Journal of Clinical Medicine. 2023; 12(7):2449. https://doi.org/10.3390/jcm12072449
Chicago/Turabian StyleKrittayaphong, Rungroj, Arjbordin Winijkul, Poom Sairat, and Gregory Y. H. Lip. 2023. "Predicting the Absolute Risk of Ischemic Stroke in Asian Patients with Atrial Fibrillation: Comparing the COOL-AF Risk Score with CARS/mCARS Models for Absolute Risk and the CHA2DS2-VASc Score" Journal of Clinical Medicine 12, no. 7: 2449. https://doi.org/10.3390/jcm12072449
APA StyleKrittayaphong, R., Winijkul, A., Sairat, P., & Lip, G. Y. H. (2023). Predicting the Absolute Risk of Ischemic Stroke in Asian Patients with Atrial Fibrillation: Comparing the COOL-AF Risk Score with CARS/mCARS Models for Absolute Risk and the CHA2DS2-VASc Score. Journal of Clinical Medicine, 12(7), 2449. https://doi.org/10.3390/jcm12072449