Abstract
This study investigated the effects of amnioreduction before physical examination-indicated cerclage on pregnancy outcomes using a propensity score matching analysis. This multicenter retrospective cohort study included women who underwent cerclage operations due to painless cervical dilation in the second trimester (14–28 weeks). The primary outcome was the time from operation until delivery. Secondary outcomes included preterm birth rate and neonatal outcomes. Primary and secondary outcomes were compared between those with amnioreduction and those without amnioreduction. Of 103 women, 31 received preoperative amnioreduction (amnioreduction group) and 72 women did not (no-amnioreduction group). Since there were differences in baseline characteristics and preoperative ultrasound findings between the two groups, we matched 25 women with amnioreduction and 25 women without amnioreduction using a propensity score. In the matched cohort, the amnioreduction group showed a shorter time from operation to delivery than the group without amnioreduction and the hazard ratio of amnioreduction was 2.5 (95% confidence interval; 1.4–4.7). In addition, the preterm birth rate before 28 weeks of gestation and the neonatal composite outcome were higher in the amnioreduction group than that in the group without amnioreduction. Amnioreduction before physical examination-indicated cerclage was associated with poor pregnancy and neonatal outcomes. Therefore, careful consideration is required when performing amnioreduction before cerclage operation.
1. Introduction
Cervical incompetence has been characterized classically by painless cervical dilatation in the mid-trimester, which is a major cause of extremely preterm birth or pregnancy loss. When there is a cervical dilatation with a visible amniotic membrane on physical examination, cerclage placement is necessary to reinforce the cervix. This is called physical examination-indicated cerclage [1,2]. It has been reported that women who have undergone physical examination-indicated cerclage show superior perinatal outcomes than those who are managed expectantly [3,4]. According to a systematic review, neonatal survival improved by 1.6 times and decreased by 0.23 times in delivery at 24–28 weeks when cerclage was performed [4].
However, cerclage operation is technically challenging in cases of cervical dilatation. Intraoperative rupture of membranes and cervical laceration are complications of emergent cerclage operation, having an incidence of 4–8% [4,5,6]. In particular, the difficulty of operation is increased as cervical stitching is performed while replacing the protruding membrane into the cervix.
Several methods have been introduced to reposition the amniotic membrane into the uterus. Pulling the cervix with ring forceps or pushing the bulging bag with saline gauze or foley catheter balloons has been used [2,7,8,9]. Among those methods, amnioreduction facilitates the replacement of the protruding membrane by reducing the hydrostatic force. Through several studies, amnioreduction has been proven to be a feasible method [10,11,12,13,14,15].
Although it is important to evaluate whether this procedure is really beneficial when performing cerclage, there is a paucity of information regarding whether amnioreduction actually improves pregnancy and neonatal outcomes compared to other methods in the context of physical examination-indicated cerclage. Thus, the purpose of this study was to investigate the effect of amnioreduction on pregnancy and neonatal outcomes in women who underwent physical examination-indicated cerclage.
2. Methods
2.1. Study Design and Study Population
This retrospective cohort study was conducted in two centers (Seoul St. Mary’s Hospital and St. Vincent’s Hospital) in South Korea. We collected data of women who underwent physical examination-indicated cerclage due to painless cervical dilatation between 14–28 weeks of gestation from January 2009 to December 2020. Women with ruptured membranes or multiple pregnancies were excluded. To examine the efficacy of amnioreduction, the study population was divided into two groups according to whether or not amnioreduction was performed before surgery. Delivery outcomes of the two groups were then compared using a propensity score matching analysis. We have obtained the approval for this study from the Central Institutional Review Board of the Catholic Medical Center in South Korea.
2.2. Determination of Amnioreduction and Physical Examination-Indicated Cerclage
The examination was performed for women who had symptoms such as vaginal bleeding or discharge and those with amniotic membrane protrusion who were referred from another hospital. If a protruding membrane was confirmed by examination, McDonald operation after replacing the amniotic membrane into the uterus was planned. The decision to carry out amnioreduction was determined based on the severity of the protrusion of the amniotic sac and the doctor’s preference. Amnioreduction was performed using a 20–22-gauge needle under ultrasound-guided conditions. Amniotic fluid was removed as much as possible or until the protruding sac decreased upon cervical examination. In this study, the median amounts of removed amniotic fluid were 175 mL (range: 50–400 mL). Amnioreduction was not performed if amniocentesis was not agreed on or if amniocentesis could not be performed. In most cases, prophylactic tocolytics and antibiotics were used. Regardless of intraoperative amnioreduction, the amnion was replaced by pulling the cervix with sponge forceps and pushing the amniotic membrane gently with a saline gauze during the operation.
2.3. Measurement of Protruding Amniotic Sac
Ultrasound parameters in ultrasound scans taken before surgery were measured retrospectively by two physicians (S Hong and YS Jo). Amniotic sludge, the shape of the protruding sac, width and length of the protruding sac, funneling length and width, and width of the narrowest point of the cervix were measured. The measurement method is shown in Supplementary Figure S1. In this figure, A is the maximal width of the protruding sac, B is the maximal length of protruding sac, C is the length of funneling, D is the width of funneling, and E represents the width of the narrowest point of the cervix.
2.4. Definitions of Outcomes
The primary outcome was the interval from operation to delivery. Secondary outcomes were operation failure, preterm birth before 24, 28, and 34 weeks of gestation, and neonatal outcomes. Operation failure was defined as a case when the operation was not possible because the amnion was not replaced during the operation and when the membrane was ruptured at the time of surgery or within 24 h of surgery. Neonatal composite outcomes included respiratory distress syndrome, bronchopulmonary dysplasia, necrotizing enterocolitis, intraventricular hemorrhage, sepsis, and neonatal death.
2.5. Statistical Analysis
For analysis of the total study population, the Student’s t-test or Wilcoxon rank–sum test was used for comparing continuous variables, and the Chi-square test or Fisher’s exact test was used for comparing categorical variables between the two groups. To reduce the influence of potential covariates or selection bias, the independent biostatistician (S Kim) performed propensity score matching to create maximally comparable groups. The possible covariates included for propensity score were the following: maternal demographics (age, parity, pre-pregnancy body mass index, and history of preterm birth), characteristics at admission (gestational age at admission, laboratory findings on admission, symptoms, results of vaginal culture, cervical dilatation, use of tocolytics, and use of antibiotics), and ultrasound parameters (amniotic sludge, appearance of protruding sac, width and length of protruding sac, width and length of funneling, and width of narrowest point of the cervix).
A ‘greedy’-matching algorithm was performed to match subjects using a caliper of 0.2 standard deviations of the logit of the propensity score and the standardized mean difference (SMD) was used for assessing the balance of variables before and after matching. After matching, a paired t-test or Wilcoxon signed–rank test was used to compare continuous variables, and a McNemar’s test was used to compare categorical variables between the two groups. The risk of neonatal outcomes was compared with the use of logistic models using Generalized Estimating Equations (GEE) that accounted for the clustering of matched pairs. It is reported as odds ratios (OR) and 95% confidence intervals (CI). Maternal outcomes and survival outcomes were compared using logistic models and Cox models, respectively, with robust standard errors. They are reported as OR or hazard ratio (HR) and 95% CI, as appropriate. All statistical analyses were performed with SAS version 9.4 (SAS Institute, Cary, NC, USA) or R version 3.6.1. Two-tailed p-values < 0.05 were considered statistically significant.
3. Results
Table 1 shows baseline characteristics and ultrasound parameters of the study population before and after propensity score matching. In the total study population, the amnioreduction group less incidentally found showed more dilated cervix rates upon admission (accidental discovery, p < 0.05; cervical dilatation > 2 cm, p < 0.005). Among ultrasound parameters, hour glassing appearance was observed more in the amnioreduction group (p = 0.001). There were significant differences in the width and length of the protruding sac between the two groups (width of protruding sac: mean 3.1 cm vs. 1.9 cm, p = 0.005; length of protruding sac: mean 2.0 cm vs. 1.0 cm, p < 0.001). After propensity score matching to correct these differences, there were no differences in maternal demographics, characteristics at admission, or ultrasound parameters (all p-value > 0.5, all SMD < 0.2).

Table 1.
Baseline characteristics and ultrasound parameters of the eligible study population and propensity score-matched population.
Table 2 demonstrates obstetric outcomes between the amnioreduction group and the no-amnioreduction group after matching. The amnioreduction group showed earlier gestational age at delivery than the no-amnioreduction group, although their difference was not statistically significant (mean: 24.8 weeks vs. 28.5 weeks, p = 0.051). The mean interval from operation to delivery of the amnioreduction group was 3.1 weeks of gestation, which was shorter than that of the no-amnioreduction group (mean: 3.1 weeks vs. 6.8 weeks, p < 0.05). The probability of delivery was significantly higher in the amnioreduction group both before and after matching, as presented in Figure 1 (HR before matching: 3.22, 95% CI: 1.97–5.27, p < 0.001; HR after matching: 2.50, 95% CI: 1.35–4.65, p < 0.005). The rate of operation failure and preterm birth before 24 weeks of gestation were not significantly different between the two groups. However, rates of preterm birth before 28 and 34 weeks of gestation of the amnioreduction group were higher than those of the no-amnioreduction group (preterm birth <28 weeks: 80% vs. 54%, OR: 3.39, 95% CI: 1.05–10.94, p < 0.05; preterm birth <34 weeks: 92% vs. 70%, OR: 5.03, 95% CI: 1.02–24.77, p < 0.05).
Table 2.
Obstetric outcomes of propensity score-matched population.
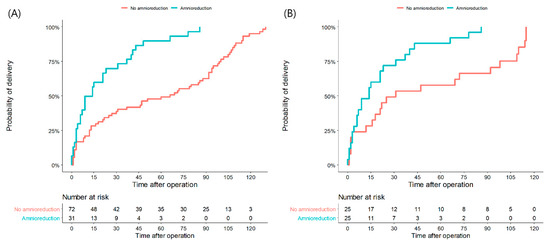
Figure 1.
Kaplan–Meier curves for time to delivery in unmatched(A) and matched patients (B) who underwent amnioreduction or did not. Survival curves show the differences in delivery proportions according to the latency period (days from operation to delivery) between two groups.
Table 3 shows neonatal outcomes of living fetuses of the matched population. NICU admission and composite morbidity of the amnioreduction group were higher than those of the no-amnioreduction group (NICU admission, OR: 5.50, 95% CI: 1.09–27.75, p < 0.05; composite morbidity, OR: 7.33, 95% CI: 1.47–36.67, p < 0.05).
Table 3.
Neonatal outcomes of living fetuses of propensity score-matched population.
4. Discussion
In this study, it was found that amnioreduction was performed in more severe patients. When the two groups were analyzed after propensity score matching, amnioreduction did not show any benefit in pregnancy prolongation. In women who received amnioreduction, the risk of preterm birth <28 weeks and <34 weeks of gestation and composite neonatal outcomes were higher than those who did not.
The protruding membrane in women with cervical incompetence not only suggests a poor prognosis, but also requires complicated surgical techniques to reposition the membrane into the uterus [16]. Although several methods have been introduced to reposition the membrane, there is no evidence that any method is superior [2,17].
Amnioreduction was originally attempted for symptom reduction and better pregnancy outcomes in twin-to-twin transfusion syndrome or idiopathic polyhydramnios. It was introduced as one of facilitating methods of bag repositioning by reducing the intra-amniotic pressure in 1980 [13,18]. Afterwards, several studies reported the feasibility of amnioreduction. They are summarized in Table 4. Interestingly, studies comparing the amnioreduction group and no-amnioreduction group reported to date all showed different results.
Table 4.
Existing studies on amnioreduction before physical examination-indicated cerclage excluding case reports.
Lacatelli et al. reported the superiority of amnioreduction for a better pregnancy outcome [12]. The rate of preterm birth <32 weeks was significantly less (1/7 vs. 6/8) and the duration of neonatal hospital stay was shorter (3 vs. 37 days) in women with amnioreduction compared to those without amnioreduction.
Cakroglu et al. reported no difference in pregnancy or neonatal outcomes according to amnioreduction [11]. The authors argued that amnioreduction was meaningful as a means to determine the presence of chorioamnionitis even though it did not improve the prognosis.
Finally, Makino et al. suggested that amnioreduction was a useful technique for repositioning fetal membranes, although it had the risk of rupture of membranes [10]. In the present study, 3 out of 11 patients who underwent amnioreduction showed rupture at the time of surgery. Except for these cases, there was no significant difference in pregnancy prolongation between the two groups (32.9 days vs. 36.9 days, p = 1.000), although the amnioreduction group had more severe cervical dilation than the no amnioreduction group (6.7 cm vs. 4.1 cm, p < 0.005).
In this study, there were differences in the severity of cervical incompetence between the group with and without amnioreduction. Thus, a propensity score match was performed to eliminate selection bias. As a result, the time from surgery to delivery was shorter and the rate of preterm birth and the risk of composite neonatal outcome were higher in women who received amnioreduction than in those who did not. The risk of rupture of the membrane within 24 h or inoperability was higher in the amnioreduction group, although the difference between the two groups was not statistically different.
There are several possibilities for the higher risk of preterm birth in women who have received amnioreduction before physical examination-indicated cerclage.
First, there is potential for triggering preterm parturition by an aggravation of intraamniotic infection and inflammation. In women with cervical incompetence, up to 80% have intraamniotic infection and inflammation [19,20,21]. The amniotic barrier is already weakened under inflammatory cytokines [22,23]. Puncture of membranes can aggravate the weakness of the membrane because it destroys the continuity of membranes and provides a pathway for microorganism entry into the amniotic fluid [24].
Second, iatrogenic disruption or weakening adherence between uterine decidua and fetal membranes may occur by removing a large amount of amniotic fluid. There are some traditional concerns about the rupture of membranes or placenta abruption resulting from amnioreduction, especially through the lower uterine segment [25]. In addition, chorioamnionic separation may occur due to amniotic fluid efflux into the chorioamnionic space after an invasive procedure, which is associated with a poor pregnancy outcome [26,27,28].
To the best of our knowledge, our study included the largest number of patients among studies comparing methods to replace the protruding membranes in the uterus. In addition, to reduce selection bias due to its retrospective nature, the amnioreduction effect was verified through case-control propensity score matching analysis. In particular, ultrasound findings, which were the most important objective findings on prognosis, were reviewed by two physicians and as many variables as possible were matched to make the two groups comparable.
Despite the above efforts, selection bias could exist and the number of patients was too small to evaluate neonatal outcomes. Since amniocentesis was not performed in the control group, we could not compare intraamniotic infection or inflammation. A large-scale prospective study comparing the methods of replacing the membranes is needed. Information on various biological markers as well as ultrasound findings is required in further studies.
In conclusion, amnioreduction as a method of repositioning the protruding membranes did not improve pregnancy prognosis, but rather worsened pregnancy outcomes. Therefore, it is necessary to try other methods first for amnion repositioning. Amnioreduction should be selectively performed for patients who cannot proceed with other methods.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/jcm12072480/s1, Figure S1. The measurement method of protruding sac and funneling of the cervix. (A) width of protruding sac, (B) length of protruding sac, (C) length of funneling, (D) width of funneling, (E) width of the narrowest point of the cervix.
Author Contributions
S.H., H.S.K. and Y.S.J. contributed to the conceptualization, and collected the data. S.K. analyzed the data. Y.S.J. and I.Y.P. assisted in developing the methodology and supervised the study. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by the Research Fund of Seoul St. Mary’s Hospital, The Catholic University of Korea. The authors wish to acknowledge the financial support of the Catholic Medical Center Research Foundation made in the program year of 2021. The funding bodies played no role in the design of the study, collection, analysis, and interpretation of data or in writing the manuscript.
Institutional Review Board Statement
We have obtained the approval of this study and the grantee of an exemption from requiring written informed consent by the Catholic Medical Center Central Institutional Review Board of the School of medicine of the Catholic University of Korea (IRB No. XC21RIDI0161). We followed the ethical standards for human experimentation established in the Declaration of Helsinki.
Informed Consent Statement
Patient consent was waived due to the retrospective design.
Data Availability Statement
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Acknowledgments
We thank the clinicians and staff from Seoul St. Mary’s Hospital and St. Vincent’s Hospital for their assistance in collecting data.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Arnold, K.C.; Flint, C.J. Cerclage for the Management of Cervical Insufficiency. In Obstetrics Essentials; Arnold, K.C., Flint, C.J., Eds.; Springer: Cham, Switzerland, 2017; pp. 173–177. [Google Scholar]
- Naqvi, M.; Barth, W.H., Jr. Emergency Cerclage: Outcomes, Patient Selection, and Operative Considerations. Clin. Obstet. Gynecol. 2016, 59, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Pereira, L.; Cotter, A.; Gómez, R.; Berghella, V.; Prasertcharoensuk, W.; Rasanen, J.; Chaithongwongwatthana, S.; Mittal, S.; Daly, S.; Airoldi, J.; et al. Expectant management compared with physical examination-indicated cerclage (EM-PEC) in selected women with a dilated cervix at 14(0/7)–25(6/7) weeks: Results from the EM-PEC international cohort study. Am. J. Obstet. Gynecol. 2007, 197, 483.e1–483.e8. [Google Scholar] [CrossRef] [PubMed]
- Ehsanipoor, R.M.; Seligman, N.S.; Saccone, G.; Szymanski, L.M.; Wissinger, C.; Werner, E.F.; Berghella, V. Physical examination-indicated cerclage: A systematic review and meta-analysis. Obstet. Gynecol. 2015, 126, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Blikman, M.J.; Le, T.M.; Bruinse, H.W.; van der Heijden, G.J. Ultrasound-predicated versus history-predicated cerclage in women at risk of cervical insufficiency: A systematic review. Obstet. Gynecol. Surv. 2008, 63, 803–812. [Google Scholar] [CrossRef]
- Belej-Rak, T.; Okun, N.; Windrim, R.; Ross, S.; Hannah, M.E. Effectiveness of cervical cerclage for a sonographically shortened cervix: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2003, 189, 1679–1687. [Google Scholar] [CrossRef]
- Ayromlooi, J. Balloon replacement of fetal membranes to facilitate emergency cervical cerclage. Obstet. Gynecol. 2002, 99, 345. [Google Scholar]
- Lv, M.; Zhao, B.; Chen, Y.; Xi, F.; Zhan, Q.; Wang, Y.; Pu, Y.; Luo, Q. Balloon tamponade for successful emergency cervical cerclage. J. Obstet. Gynaecol. Res. 2020, 46, 418–424. [Google Scholar] [CrossRef]
- Son, G.-H.; Chang, K.H.-J.; Song, J.-E.; Lee, K.-Y. Use of a uniconcave balloon in emergency cerclage. Am. J. Obstet. Gynecol. 2015, 212, 114.e1–114.e4. [Google Scholar] [CrossRef]
- Makino, Y.; Makino, I.; Tsujioka, H.; Kawarabayashi, T. Amnioreduction in patients with bulging prolapsed membranes out of the cervix and vaginal orifice in cervical cerclage. J. Perinat. Med. 2004, 32, 140–148. [Google Scholar] [CrossRef]
- Cakiroglu, Y.; Doger, E.; Kopuk, S.Y.; Gunlemez, A.; Oguz, D.; Caliskan, E. Does amnioreduction increase success of emergency cervical cerclage in cases with advanced cervical dilatation and protruding membranes? Clin. Exp. Obstet. Gynecol. 2016, 43, 708–712. [Google Scholar] [CrossRef]
- Locatelli, A.; Vergani, P.; Bellini, P.; Strobelt, N.; Arreghini, A.; Ghidini, A. Amnioreduction in emergency cerclage with prolapsed membranes: Comparison of two methods for reducing the membranes. Am. J. Perinatol. 1999, 16, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Goodlin, R.C. Cervical incompetence, hourglass membranes, and amniocentesis. Obstet. Gynecol. 1979, 54, 748–750. [Google Scholar] [PubMed]
- Zhang, Y.; Han, Z.; Gao, Q.; Bai, X.; Hou, H. Amnioreduction in emergency cervical cerclage: A series of eight cases. Int. J. Gynaecol. Obstet. 2020, 150, 416–417. [Google Scholar] [CrossRef] [PubMed]
- Proctor, L.K.; Ronzoni, S.; Melamed, N.; Nevo, O.; Cohen, H.; Barrett, J. Amnioreduction with rescue cerclage at advanced cervical dilation or gestational age. J. Matern. Fetal Neonatal Med. 2021, 35, 5607–5610. [Google Scholar] [CrossRef]
- Rius, M.; Cobo, T.; Garcia-Posadas, R.; Hernandez, S.; Teixido, I.; Barrau, E.; Abad, C.; Palacio, M. Emergency cerclage: Improvement of outcomes by standardization of management. Fetal Diagn. Ther. 2016, 39, 134–139. [Google Scholar] [CrossRef]
- Hashim, H.A.; Al-Inany, H.; Kilani, Z. A review of the contemporary evidence on rescue cervical cerclage. Int. J. Gynaecol. Obstet. 2014, 124, 198–203. [Google Scholar] [CrossRef]
- Goodlin, R.C. Surgical treatment of patients with hour glass shaped or ruptured membranes prior to the twenty-fifth week of gestation. Surg. Gynecol. Obstet. 1987, 165, 410–412. [Google Scholar]
- Romero, R.; Gonzalez, R.; Sepulveda, W.; Brandt, F.; Ramirez, M.; Sorokin, Y.; Mazor, M.; Treadwell, M.C.; Cotton, D.B. Infection and labor. VIII. Microbial invasion of the amniotic cavity in patients with suspected cervical incompetence: Prevalence and clinical significance. Am. J. Obstet. Gynecol. 1992, 167, 1086–1091. [Google Scholar] [CrossRef]
- Lee, S.E.; Romero, R.; Park, C.W.; Jun, J.K.; Yoon, B.H. The frequency and significance of intraamniotic inflammation in patients with cervical insufficiency. Am. J. Obstet. Gynecol. 2008, 198, 633.e1–633.e8. [Google Scholar] [CrossRef]
- Bujold, E.; Morency, A.M.; Rallu, F.; Ferland, S.; Tétu, A.; Duperron, L.; Audibert, F.; Laferrière, C. Bacteriology of amniotic fluid in women with suspected cervical insufficiency. J. Obstet. Gynaecol. Can. 2008, 30, 882–887. [Google Scholar] [CrossRef]
- Kobayashi, K.; Miwa, H.; Yasui, M. Inflammatory mediators weaken the amniotic membrane barrier through disruption of tight junctions. J. Physiol. 2010, 588, 4859–4869. [Google Scholar] [CrossRef] [PubMed]
- Vrachnis, N.; Karavolos, S.; Iliodromiti, Z.; Sifakis, S.; Siristatidis, C.; Mastorakos, G.; Creatsas, G. Review: Impact of mediators present in amniotic fluid on preterm labour. Vivo 2012, 26, 799–812. [Google Scholar]
- Maggio, L.; Carr, S.R.; Watson-Smith, D.; O’Brien, B.M.; Lopes, V.; Muratore, C.S.; Luks, F.I. Iatrogenic Preterm Premature Rupture of Membranes after Fetoscopic Laser Ablative Surgery. Fetal Diagn. Ther. 2015, 38, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Müngen, E.; Tütüncü, L.; Muhcu, M.; Yergök, Y.Z. Pregnancy outcome following second-trimester amniocentesis: A case-control study. Am. J. Perinatol. 2006, 23, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Bergh, E.P.; Moise, K.J., Jr.; Johnson, A.; Papanna, R. Pregnancy outcomes associated with chorioamnion membrane separation severity following fetoscopic laser surgery for twin-twin transfusion syndrome. Prenat. Diagn. 2020, 40, 1020–1027. [Google Scholar] [CrossRef]
- Krispin, E.; Mustafa, H.J.; Sun, R.C.; Donepudi, R.; Espinoza, J.; Nassr, A.A.; Belfort, M.A.; Sanz Cortes, M.; Mostafaei, S.; Harman, C.; et al. Iatrogenic chorioamniotic separation and septostomy following fetoscopic laser photocoagulation for twin-twin transfusion syndrome. Ultrasound Obstet. Gynecol. 2021, 59, 506–512. [Google Scholar] [CrossRef]
- Takano, M.; Nakata, M.; Murata, S.; Sumie, M.; Morita, M. Chorioamniotic membrane separation after fetoscopic laser photocoagulation. Fetal Diagn. Ther. 2018, 43, 40–44. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).