Abstract
Objectives: The aim of the study was to make a preliminary assessment of depression rates and levels of physical activity and the association between physical activity and depression among Polish and Portuguese students in the second year of the COVID-19 pandemic. Methods: A web-based online survey was conducted among students in Poland and Portugal (398 respondents—229 from Poland and 169 from Portugal) aged between 17 and 26 in October 2022. The level of depression was assessed by the Beck Depression Inventory (BDI) in Polish and in Portuguese. The level of physical activity was measured by the International Physical Activity Questionnaire (IPAQ) in Polish and in Portuguese. Results: Overall, 20–35% of respondents suffered from moderate depression, with a lower proportion among men. There were no differences in the percentage distribution of depression classification between Polish and Portuguese students. A decrease in the severity of depression was observed with increasing physical activity. In both countries, walking more often had the strongest effect on reducing depression scores. Conclusions: The continued and alarming prevalence of depressive disorders among university students in the year after the pandemic began had a significant impact on this population—further research on the impact of physical activity on mental health in different populations should be conducted to adjust the optimal level of physical activity for alleviating negative psychiatric symptoms.
1. Introduction
Change in functioning in daily activities related to introduced learning and online work was related to the announcement of the COVID-19 pandemic in 2020. The governments of most countries implemented the measures recommended by the World Health Organization such as social distancing to limit the spread of coronavirus in the population [1,2]. Isolation for several months and staying indoors for most of the day forced not only children and adolescents but also adults to change their lifestyle from active to passive [3]. Restrictions on exercise, and bans on gyms, swimming pools, and health clubs have largely led to a decline in daily physical activity [4].
The World Health Organization defines physical activity as any movement of the human body that is stimulated by skeletal muscles and simultaneously requires an expenditure of energy. To maintain health, 150 min of moderate physical activity or 75 min of vigorous activity per week is recommended [5,6]. Regular moderate physical activity is beneficial for people of all ages, regardless of gender, fitness, and health status, and most importantly improves quality of life [7,8,9].
The positive effects of physical activity on the musculoskeletal, cardiovascular, or neuromuscular systems have been observed. Physical activity is also recognized as a factor that prevents and has a therapeutic effect on mental disorders. In addition, it is one of the ways to deal with anxiety or depression and to strengthen self-esteem [10,11]. Regular physical activity is considered a good way to manage stress and improve mood, and has a positive effect on brain function [12,13]. Even 10 min of physical activity such as walking, jogging, or cycling can improve mood [14]. Limiting physical activity can be one of the risk factors that contribute to diabetes, hypertension, and obesity, or have a negative impact on mental health [15,16,17].
There are numerous studies in the literature confirming the positive effects of physical activity on human mental health [3,18,19]. Even short periods of reduced physical activity require research by multidisciplinary teams into the factors that may cause it and the detrimental effects on the function of numerous systems and organs.
Poland experienced one of the longest lockdowns in education in Europe. In Portugal, lockdowns lasted slightly shorter, placing the country in the middle, albeit among the top countries in Western Europe [20] (Figure 1). Consequently, the researchers decided to compare samples of the student populations from both countries.
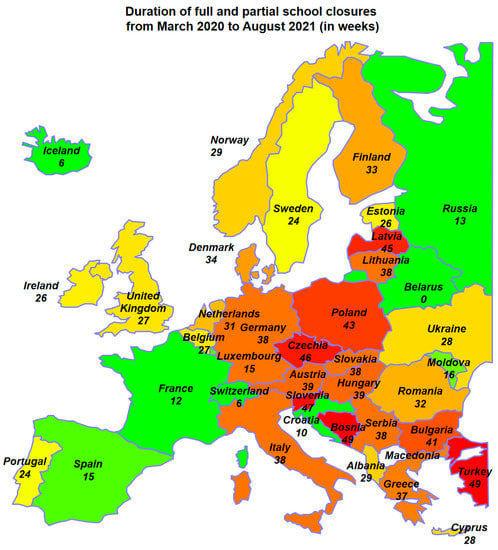
Figure 1.
Duration of full and partial school closures in chosen Europe countries from March 2020 to August 2021 (Countries with a long period of school closures are marked with shades of red, and those with the shortest duration of distance learning are marked with shades of green.) [20].
The aim of the study was to make a preliminary assessment of depression rates and levels of physical activity as well as relationship between physical activity and depression among Polish and Portuguese students in the further year of the COVID-19 pandemic.
2. Materials and Methods
2.1. Participants and Procedure
In October 2022, students from Poland and Portugal participated in an online cross-sectional survey. The researchers distributed the survey by providing links to a Google form that asked students to participate in the survey on online e-learning platforms and on social media (Facebook) in private groups. The survey was accompanied by information about the study, anonymity, and voluntary consent to participate. In the groups for Polish students, the questionnaire was in Polish and in the groups for Portuguese students, the questionnaire was in Portuguese. Inclusion criteria were: student status, consent to participate in the study, residence in Poland or Portugal, full completion of the survey. Exclusion criteria were: no student status, no consent to participate in the study, no residence in Poland or Portugal, incomplete completion of the survey. A total of 502 responses to the researchers’ request were received. A total of 398 questionnaires were correctly completed and this group was analyzed. The study included 229 questionnaires from Poland and 169 from Portugal. The students polled ranged in age from 17 to 26 years. The study included 247 women and 151 men in total.
The Lomza State University of Applied Sciences Senate Committee on Ethics in Scientific Research gave its approval to the initiative.
In accordance with Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016, on the protection of natural persons with regard to the processing of personal data and on the free movement of such data and repealing Directive 95/46/EC, in the Personal Data Protection Act of 10 May 2018, participation in the study was voluntary, and the findings were published (Journal of Laws 2018, item 1000). GDPR, or the General Data Protection Regulation, the study’s goals, the poll’s methodology, and the relevant data protection rules were explained to the respondents.
2.2. Methods of Assessing the Level of Depression and Physical Activity
2.2.1. Beck Depression Inventory
The level of depression was assessed using the Beck Depression Inventory (BDI) in Polish and in Portuguese. This is a questionnaire that consists of 21 questions and is used for self-assessment of the severity of depressive symptoms on a scale from 0 to 3 (further response options indicate increased symptom intensity). The level of depression is calculated after adding up the number of points. The summed measure of the Beck Depression Inventory can range from 0 to 63 points. Higher values obtained by the respondent indicate higher levels of depression [21]. Measures of depression are also considered on a 4-point scale, where: 0–11 means no depression; 12–26 means mild depression; 27–49 means moderate depression; 50–63 means severe depression [21]. The value for Cronbach’s alpha reported in papers is >0.7 [22,23,24,25].
2.2.2. International Physical Activity Questionnaire
The level of physical activity was assessed using an abbreviated version of the International Physical Activity Questionnaire (IPAQ) in Polish and Portuguese, which is designed for people aged 15–69 years. It consists of 7 questions that cover all daily physical activities at work, in and around the home, and during leisure time. The questionnaire assesses activities that last continuously for at least 10 min. Each activity’s description is given in MET-min/week units, which are calculated by multiplying the activity’s coefficient by the number of days it was conducted throughout the week and by the activity’s duration in minutes per day [26,27]. In publications, Cronbach’s alpha is stated to be >0.7 [28,29,30].
2.3. Statistical Methods
For statistical analysis, Statistica v. 13 software was used (TIBCO Software Inc. (2017). Statistica (data analysis software system), version 13). The Mann–Whitney test was used to determine the significance of differences in depression severity (BDI) and physical activity level (IPAQ) between groups of Portuguese and Polish students, while the chi-square test of independence was used to determine differences in the percentage distribution of depression level classification and activity level. Spearman’s rank correlation coefficient was used to calculate correlations between depression severity and physical activity. The Kruskal–Wallis test was used to determine the significance of differences in depression severity (BDI) versus activity level classification. The non-normality of the distributions of the BDI and IPAQ measures, all of which had very strong right-handed asymmetry, dictated the use of non-parametric methods. A significance level of p < 0.05 (*) was established for all statistical analyses, but additionally denoted results for p < 0.01 (**) and p < 0.001 (***).
3. Results
3.1. General Characteristics
The analysis concerns a 398-member sample of students from Poland and Portugal. Both populations were predominantly female students—Poland 129 women (56.3%), Portugal 118 women (69.8%). The average age of the Polish and Portuguese students surveyed is similar (Table 1), so this is not a differentiating factor between the two study groups. They are comparable in this respect.

Table 1.
Average age of respondents.
3.2. Comparison of Depression among Students in Both Countries by Gender
Depression levels are generally lower among men, while there is no statistically significant difference in BDI values between the two countries—neither for men nor for women (Table 2).
Table 2.
Measures of depression severity in Poland and Portugal by gender.
After categorizing the BDI values into a four-point scale of depression severity (Table 3), it appears that the majority of students were not depressed (approximately 60–70% depending on gender and nationality). Moderate depression affected 20–35% of the respondents, while more severe depressive states occurred sporadically. There were also no differences between Polish and Portuguese students in the percentage distribution of depression classifications.
Table 3.
Level of depression severity in Poland and Portugal according to gender on a four-point scale.
3.3. Comparison of Activities by Student Gender
The table (Table 4) provides detailed information on the measure of total physical activity, calculated from the IPAQ questionnaire. As gender is a differentiating factor in physical activity levels, the summary is given by female and male. No statistically significant differences were found in the physical activity levels of young people from the two countries, either for women or for men. For a measure showing a very high asymmetry in the distribution of results, as can be seen by comparing the mean (inflated by a few extremely high observations) and the median, a better measure of the average level is the latter figure.
Table 4.
Measure of total physical activity.
The next table (Table 5) provides summaries for the detailed IPAQ measures and the overall measure in simplified form—the mean, median, and interquartile range (IQR) are provided. As can be seen, although there are no differences between countries on the overall measure, there is a significantly lower level of activity among Portuguese female students on the intensive effort measure (p = 0.0039 *) and to a lesser extent on the moderate effort measure (p = 0.0801).
Table 5.
Summary of IPAQ specific measures.
When comparing the IPAQ measure classifications (Table 6) for the numeric IPAQ measure scores, the differences between the two countries are not statistically significant, while for the classification it seems that the Portuguese female students showed a different profile of physical activity—there were fewer of them with low activity (16% vs. 34%), but also with high activity (27% vs. 43%). Thus, the Polish women showed a more extreme attitude, while more than half of the Portuguese women showed a medium level of activity.
Table 6.
Summary of IPAQ measure classifications.
3.4. Depression and Physical Activity
It was investigated to what extent the level of physical activity was related to the severity of depression, considering different intensities. For this purpose, a correlation analysis was performed between the IPAQ scores and the BDI score. Due to the very pronounced influence of gender on IPAQ measures (they are significantly higher in men), the analysis was performed by gender and separately for both countries (Table 7).
Table 7.
Correlation coefficients between physical activity 19 and the BDI depression index.
In Portuguese women, there was no statistically significant correlation between activity and depression, while in Polish women the only statistically significant (p = 0.0155 *) but very weak correlation (rS = −0.21) was between walking intensity and depression. The negative sign of the correlation means that more walking had a positive effect on the psyche, resulting in a minimal reduction in the severity of depression.
A stronger effect of physical activity on reducing depression was observed in men. The correlations were slightly stronger in the Polish population. In both countries, more frequent walking had the strongest effect on reducing BDI (in Poland, rS = −0.42; in Portugal, rS = −0.28).
Complementary to this analysis, information on the distribution of BDI in groups separated by physical activity level is summarized (Table 8). When the IPAQ is split into groups, some information is lost, and it is therefore more difficult to obtain a statistically significant relationship. In general, however, a weak trend toward a decrease in depression severity with increasing activity can be seen in the Polish group. However, because the differences in depression severity between groups with varying levels of physical activity were not statistically significant, the preceding observation should be regarded as a hypothesis for further research rather than a definitive conclusion. The p-value was less than 0.1 only for male students from Poland, indicating a difference close to statistical significance.
Table 8.
Distribution of BDI in groups separated by physical activity level.
4. Discussion
It has been almost three years since the COVID-19 pandemic hit the world and negatively affected not only people’s physical health, but also their mental health [31]. Depression among university students proved to be one of the most important psychological consequences of the pandemic [32]. At the same time, students suffered at a higher rate compared to the general population [33]. Despite the existing literature on the psychological consequences of the pandemic and the health effects of physical activity, this issue is still relevant.
Results of a systematic review and meta-analysis conducted during the pandemic on the prevalence of depression among students worldwide showed that, on average, it affected 37% (95% CI, 32–42%) of the student population [31]. In a study at the beginning of the pandemic, up to 31% of students in Poland were found to suffer from moderate or severe depression, depending on where the study was conducted [34]. It was also observed that the number of depressions increased significantly as the pandemic progressed [35]. At the same time, data on the prevalence of depression among students in Portugal at the very beginning of the pandemic indicated levels in the range of 17.2% [36], then 24.2% [37]. However, other studies present higher levels of depressive disorders among Portuguese students and also an increased prevalence as the pandemic progressed [38,39]. In addition, 49.2% of Portuguese respondents surveyed by Mauro et al. reported moderate or severe psychological effects of the outbreak [40]. Although our own study found that the majority of students were not depressed, it was alarming that, in the second year of the pandemic, after most sanitary restrictions had been lifted and the vaccine COVID-19 had been released for general use, 20-35% of respondents were still affected by moderate depression.
In meta-analyses available in the literature, the most significant difference in levels of depression during the pandemic was found between geographical regions. Researchers conducting a review and meta-analysis of studies reporting levels of depression among dental students during the COVID-19 found a significantly higher prevalence of depression in studies from Asia compared to Europe and the Americas [32], which is confirmed by other meta-analyses [41,42]. Differences in levels of depression between different countries may be due to a number of factors, e.g., tools used to measure variables, sample size, the curricular load, and existing socio-cultural differences between countries [36]. Studies conducted at the very beginning of the pandemic on levels of depression in Switzerland and Portugal showed disadvantage of the Portuguese population, which has been linked, among other things, to cultural differences between countries [43].
At the same time, cumulative evidence from a meta-analysis on depression in Eastern Europe during the COVID-19 reveals high prevalence rates of clinically significant symptoms during the pandemic in Eastern Europe [44]. Psychiatric care in Eastern Europe depends on large psychiatric institutions with a focus on inpatient psychiatry, which is not effective in treating depression [45]. In Poland, lack of funding and easy and general access to specialized psychiatric and psychological care also contribute to poor mental health [46]. In Portugal, despite the high prevalence of mental disorders, available data suggest that a significant proportion of people do not receive adequate mental health care [47]. Despite the geographical location, there are no differences in the percentage distribution of depression classifications between Polish and Portuguese students, which may be related to similar problems in accessing mental health care in both countries.
Previous long-term studies, conducted before the pandemic, had already found that women were more likely to develop depression, which is related to gender characteristics [48]. These findings are consistent with other studies conducted in the general population, which found higher rates of depression in women compared to men during the pandemic COVID-19 [49], as well as results from studies conducted in university students [50,51]. In our study, we found that depression rates were generally lower in men, while there was no statistically significant difference in BDI scores between the two countries.
Physical activity can effectively stimulate specific brain regions, thereby improving emotion and behavior regulation, promoting self-regulation of emotions, and helping to apply more adaptive emotion regulation strategies to better cope with stress during a pandemic [52,53]. Physical exertion also leads to a marked increase in sympathetic nervous system activity and catecholamine release. As a result, it may be able to regulate the secretion of melatonin, which significantly improves cardiovascular function, increases skeletal muscle adaptability, and protects body health [54]. Early in the pandemic, it was clear that increased physical activity had a positive effect on mental health in non-students, and regular maintenance of physical activity during the COVID-19 pandemic was associated with lower levels of anxiety and depression in subjects [2,18]. Our study also shows a tendency for depression severity to decrease with increased physical activity. A stronger effect of physical activity on reducing depression was observed in men. The correlations are slightly stronger in the Polish population, but it is difficult to clearly explain this difference.
Ongoing meta-analyses have shown that physical activity of different intensity significantly improves depressiveness and anxiety in university students [55,56]. In our study, a subgroup analysis showed that physical activity at a certain intensity could reduce students’ depressiveness. In both countries, more frequent walking had the strongest effect on reducing depression scores (in Poland, rS = −0.42; in Portugal, rS = −0.28). These results are consistent with the conclusions drawn on the basis of studies conducted during the pandemic. It was concluded that moderate-intensity training may be the optimal training intensity for promoting mental health by reducing TNF-α. This has important implications for dosing recommendations for physical activity for the treatment of mental illness [57]. However, there is no definitive consensus in the literature on the optimal level of physical activity to alleviate negative psychiatric symptoms [11]. There are other studies, indicating that it is, for example, intensive (6 < 9 Mets) physical activity that should be superior to moderate (3 < 6 Mets) physical activity in the treatment of people with depressive disorders [55].
There were no statistically significant differences in physical activity levels among adolescents from the two countries, either in women or men. Portuguese female students showed a different physical activity profile, with fewer low-activity (16% vs. 34%) but also high-activity (27% vs. 43%) students. There were more extreme attitudes among Polish women, while more than half of Portuguese women were active at an intermediate level. Similar results were obtained by Król et al. who studied physical activity levels among students in Poland, Portugal, and Belarus [58].
The present study has several limitations that should be noted. First, the cross-sectional nature of the study does not provide robust and causal evidence for the observed associations. The second limitation was the small sample group and preliminary findings. The study was also conducted in an online survey format and the identity of those who responded is not known [59]. Social media particularly attracts stressed individuals looking for support, which may distort the data and affect the representativeness of the sample. All data were collected using self-report questionnaires, which may bias responses [60]. Despite these limitations, the current study has a number of strengths, such as its potential contribution to the field of mental health, as it presents mental health and physical activity outcomes for the second year of the pandemic. The use of standardized and validated instruments was also a strength of the present study, as well as the easy access to the study group, low cost, and small amount of time spent on the project. Future studies should target a larger sample and use more objective methods to assess the parameters studied.
5. Conclusions
Considering the persistent and alarming prevalence of depressive disorders among students in the next year of exposure to the SARS-CoV-2 virus, this situation can be expected to have a significant impact on this population. Understanding the prevalence of mental disorders in specific regions of Europe and the factors that have a positive impact on them can help to create targeted health policies. Further research should be conducted on the impact of physical activity on mental health in different populations, with the aim of adjusting the optimal level of physical activity for the alleviation of negative mental symptoms. Pilot studies have shown that there are not many statistically significant differences in depression and physical activity levels between students in Poland and Portugal.
Author Contributions
Conceptualization, A.Z. and M.G.; methodology, A.Z. and M.G.; formal analysis, M.S.; investigation, A.Z. and M.G.; data curation, A.Z., M.G. and H.F.; writing—original draft preparation, A.Z., M.G. and M.S.; visualization, A.Z. and M.G. All authors have read and agreed to the published version of the manuscript.
Funding
This work received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Senate Commission for Ethics in Scientific Research of the Lomza State University of Applied Sciences (4907500).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are openly available in RepOD at https://doi.org/10.18150/0J3FKR (accessed on 14 February 2023).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hemphill, N.M.; Kuan, M.T.Y.; Harris, K.C. Reduced physical activity during COVID-19 pandemic in children with congenital heart disease. Can. J. Cardiol. 2020, 36, 1130–1134. [Google Scholar] [CrossRef] [PubMed]
- Wolf, S.; Seiffer, B.; Zeibig, J.-M.; Welkerling, J.; Brokmeier, L.; Atrott, B.; Ehring, T.; Schuch, F.B. Is Physical Activity Associated with Less Depression and Anxiety During the COVID-19 Pandemic? A Rapid Systematic Review. Sports Med. 2021, 51, 1771–1783. [Google Scholar] [CrossRef] [PubMed]
- Xiang, M.-Q.; Tan, X.-M.; Sun, J.; Yang, H.-Y.; Zhao, X.-P.; Liu, L.; Hou, X.-H.; Hu, M. Relationship of physical activity with anxiety and depression symptoms in Chinese college students during the COVID-19 outbreak. Front. Psychol. 2020, 11, 582436. [Google Scholar] [CrossRef] [PubMed]
- Websret, C.A.; D’Agostino, E.; Urtel, M.; McMullen, J.; Culp, B.; Ergan Lolacono Cate, A.; Killan, C. Physical education in the COVID era: Considerations for online program delivery using the comprehensive school physical activity program framework. J. Teach. Phys. Educ. 2021, 41, 327–330. [Google Scholar] [CrossRef]
- Wardoku, R.; Blair, C.; Demmer, R.; Prizment, A. Association between physical inactivity and health-related quality of life in adults with coronary heart disease. Maturitas 2019, 128, 36–42. [Google Scholar] [CrossRef]
- Parra-Rizo, M.A.; Sanchis-Soler, G. Satisfaction with Life, Subjective Well-Being and Functional Skills in Active Older Adults Based on Their Level of Physical Activity Practice. Int. J. Environ. Res. Public Health 2020, 17, 1299. [Google Scholar] [CrossRef]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The physical activity guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef]
- Shigdel, R.; Dalen, H.; Sui, X.; Lavie, C.J.; Wisløff, U.; Ernstsen, L. Cardiorespiratory fitness and the risk of first acute myocardial infarction: The HUNT study. J. Am. Heart Assoc. 2019, 8, e010293. [Google Scholar] [CrossRef]
- Hooker, S.P.; Sui, X.; Colabianchi, N.; Vena, J.; Laditka, J.; LaMonte, M.J.; Blair, S.N. Cardiorespiratory fitness as a predictor of fatal and nonfatal stroke in asymptomatic women and men. Stroke 2008, 39, 2950–2957. [Google Scholar] [CrossRef]
- Shahidi, S.H.; Stewart Williams, J.; Hassani, F. Physical activity during COVID-19 quarantine. Acta Paediatr. 2020, 109, 2147–2148. [Google Scholar] [CrossRef]
- Marconcin, P.; Werneck, A.O.; Peralta, M.; Ihle, A.; Gouveia, R.; Ferrari, G.; Sarmento, H.; Marques, A. The association between physical activity and mental health during the first year of the COVID-19 pandemic: A systematic review. BMC Public Health 2022, 22, 209. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.S.; Kubzansky, L.D.; Soo, J.; Boehm, J.K. Maintaining Healthy Behavior: A Prospective Study of Psychological Well-Being and Physical Activity. Ann. Behav. Med. 2017, 51, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Füzéki, E.; Groneberg, D.A.; Banzer, W. Physical activity during COVID-19 induced lockdown: Recommendations. J. Occup. Med. Toxicol 2020, 15, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Rogerson, M.; Wood, C.; Pretty, J.; Schoenmakers, P.; Bloomfield, D.; Barton, J. Regular Doses of Nature: The Efficacy of Green Exercise Interventions for Mental Wellbeing. Int. J. Environ. Res. Public Health 2020, 17, 1526. [Google Scholar] [CrossRef]
- Dong, H.; Yang, F.; Lu, X.; Hao, W. Internet Addiction and Related Psychological Factors Among Children and Adolescents in China During the Coronavirus Disease 2019 (COVID-19) Epidemic. Front. Psychiatry 2020, 11, 00751. [Google Scholar] [CrossRef] [PubMed]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, e100213. [Google Scholar] [CrossRef]
- Salman, D.; Vishnubala, D.; Le Feuvre, P.; Beaney, T.; Korgaonkar, J.; Majeed, A.; McGregor, A.H. Returning to physical activity after covid-19. BMJ 2021, 372, m4721. [Google Scholar] [CrossRef]
- Stanton, R.; To, Q.G.; Khalesi, S.; Williams, S.; Alley, S.J.; Thwaite, T.L.; Fenning, A.S.; Vandelanotte, C. Depression, Anxiety and Stress during COVID-19: Associations with Changes in Physical Activity, Sleep, Tobacco and Alcohol Use in Australian Adults. Int. J. Environ. Res. Public Health 2020, 17, 4065. [Google Scholar] [CrossRef]
- Li, M.; Wang, Q.; Shen, J. The impact of physical activity on mental health during COVID-19 pandemic in China: A systematic review. Int. J. Environ. Res. Public Health 2022, 19, 6584. [Google Scholar] [CrossRef]
- Available online: https://en.unesco.org/file/unesco-data-school-closures-february-2020-june-2022csv-zip (accessed on 9 February 2023).
- Fydrich, T.; Dowdall, D.; Chambless, D.L. Reliability and validity of the beck anxiety inventory. J. Anxiety Disord. 1992, 6, 55–61. [Google Scholar] [CrossRef]
- Sorbie, G.G.; Beaumont, A.J.; Williams, A.K.; Glen, J.; Hardie, S.M.; Lavallee, D. The Impact of the Closure and Reopening of Golf Courses in the United Kingdom on Wellbeing During the COVID-19 Pandemic: A Multi-Study Approach. Front. Sports Act. Living 2021, 3, 622171. [Google Scholar] [CrossRef] [PubMed]
- Brochado, F.J.D.A.O. Inventário de depressão de Beck II (BDI-II): Estudo de Validação e Dados Normativos para a População Portuguesa. Ph.D. Thesis, Universidade do Porto, Porto, Portugal, 2013. Available online: https://hdl.handle.net/10216/94627 (accessed on 25 February 2023).
- Kojima, M.; Furukawa, T.A.; Takahashi, H.; Kawai, M.; Nagaya, T.; Tokudome, S. Cross-cultural validation of the Beck Depression Inventory-II in Japan. Psychiatry Res. 2002, 110, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.P.; Andrade, L.H.; Gorenstein, C. Validation of the Beck Depression Inventory for a Portugese-speaking Chinese community in Brazil. Braz. J. Med Biol. Res. 2005, 38, 399–408. [Google Scholar] [CrossRef] [PubMed]
- Biernat, E.; Stupnicki, R.; Gajewski, A.K. International Physical Activity Questionnaire (IPAQ)-Polish version. Wych. Fiz. Sport 2007, 51, 47–54. [Google Scholar]
- Campaniço, H.M.P.G. Validade Simultanea do Questionario Internacional de Actividade Fisica Atraves de Medição Objetiva da Actividade Fisica por Actigrafia Proporcional. Master’s Thesis, Universidade de Lisboa, Lisbon, Portugal, 2016. Available online: http://hdl.handle.net/10400.5/11866 (accessed on 26 February 2023).
- Moghaddam, M.H.B.; Aghdam, F.; Asghari Jafarabadi, M.; Allahverdipour, H.; Nikookheslat, S.; Safarpour, S. The Iranian Version of International Physical Activity Questionnaire (IPAQ) in Iran: Content and Construct Validity, Factor Structure, Internal Consistency and Stability. World Appl. Sci. J. 2012, 18, 1073–1080. [Google Scholar]
- Mannocci, A.; Masala, D.; Mei, D.; Tribuzio, A.M.; Villari, P. International Physical Activity Questionnaire for Adolescents (IPAQ A): Reliability of an Italian version. Minerva Pediatr. 2021, 73, 383–390. [Google Scholar] [CrossRef]
- Cardol, M.; de Haan, R.J.; de Jong, B.A.; van den Bos, G.A.; de Groot, I.J. Psychometric properties of the Impact on Participation and Autonomy Questionnaire. Arch. Phys. Med. Rehabil. 2001, 82, 210–216. [Google Scholar] [CrossRef]
- Wang, C.; Wen, W.; Zhang, H.; Ni, J.; Jiang, J.; Cheng, Y.; Zhou, M.; Ye, L.; Feng, Z.; Ge, Z.; et al. Anxiety, depression, and stress prevalence among college students during the COVID-19 pandemic: A systematic review and meta-analysis. J. Am. Coll. Health 2021, 1–8. [Google Scholar] [CrossRef]
- Santabárbara, J.; Ozamiz-Etxebarria, N.; Idoiaga, N.; Olaya, B.; Bueno-Novitol, J. Meta-Analysis of Prevalence of Depression in Dental Students during COVID-19 Pandemic. Medicina 2021, 57, 1278. [Google Scholar] [CrossRef]
- Shah, S.M.A.; Mohammad, D.; Qureshi, M.F.H.; Abbas, M.Z.; Aleem, S. Prevalence, Psychological Responses and Associated Correlates of Depression, Anxiety and Stress in a Global Population, During the Coronavirus Disease (COVID-19) Pandemic. Community Ment. Health J. 2020, 57, 101–110. [Google Scholar] [CrossRef]
- Zalewska, A.; Gałczyk, M.; Sobolewski, M.; Białokoz-Kalinowska, I. Depression as Compared to Level of Physical Activity and Internet Addiction among Polish Physiotherapy Students during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 10072. [Google Scholar] [CrossRef] [PubMed]
- Debowska, A.; Horeczy, B.; Boduszek, D.; Dolinski, D. A repeated cross-sectional survey assessing university students’ stress, depression, anxiety, and suicidality in the early stages of the COVID-19 pandemic in Poland. Psychol. Med. 2022, 52, 3744–3747. [Google Scholar] [CrossRef]
- Laranjeira, C.; Dixe, M.A.; Valentim, O.; Charepe, Z.; Querido, A. Mental Health and Psychological Impact during COVID-19 Pandemic: An Online Survey of Portuguese Higher Education Students. Int. J. Environ. Res. Public Health 2022, 19, 337. [Google Scholar] [CrossRef] [PubMed]
- Laranjeira, C.; Dixe, M.A.; Querido, A. Mental Health Status and Coping among Portuguese Higher Education Students in the Early Phase of the COVID-19 Pandemic. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 429–439. [Google Scholar] [CrossRef]
- Ferreira, M.; Sofia, R.; Carreno, D.; Eisenbeck, N.; Jongenelen, I.; Cruz, J. Dealing with the Pandemic of COVID-19 in Portugal: On the Important Role of Positivity, Experiential Avoidance, and Coping Strategies. Front. Psychol. 2021, 12, 647984. [Google Scholar] [CrossRef] [PubMed]
- Moreira, P.; Ferreira, S.; Couto, B.; Machado-Sousa, M.; Fernández, M.; Raposo-Lima, C.; Sousa, N.; Picó-Pérez, M.; Morgado, P. Protective Elements of Mental Health Status during the COVID-19 Outbreak in the Portuguese Population. Int. J. Environ. Res. Public Health 2021, 18, 1910. [Google Scholar] [CrossRef] [PubMed]
- Silva Paulino, M.; Dumas-Diniz, R.; Brissos, S.; Brites, R.; Alho, L.; Simões, M.R.; Silva, C.F. COVID-19 in Portugal: Exploring the immediate psychological impact on the general population. Psychol. Health Med. 2021, 26, 44–55. [Google Scholar] [CrossRef] [PubMed]
- Luo, M.; Guo, L.; Yu, M.; Jiang, W.; Wang, H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public—A systematic review and meta-analysis. Psychiatry Res. 2020, 291, 113190. [Google Scholar] [CrossRef]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef]
- Schwander-Maire, F.; Querido, A.; Cara-Nova, T.; Dixe, M.A.; Aissaoui, D.; Charepe, Z.; Christie, D.; Laranjeira, C. Psychological Responses and Strategies Towards the COVID-19 Pandemic Among Higher Education Students in Portugal and Switzerland: A Mixed-Methods Study. Front. Psychiatry 2022, 13, 903946. [Google Scholar] [CrossRef]
- Zhang, S.X.; Miller, S.O.; Xu, W.; Yin, A.; Chen, B.Z.; Delios, A.; Dong, R.K.; Chen, R.Z.; McIntyre, R.S.; Wan, X.; et al. Meta-analytic evidence of depression and anxiety in Eastern Europe during the COVID-19 pandemic. Eur. J. Psychotraumatol. 2022, 13, 2000132. [Google Scholar] [CrossRef] [PubMed]
- Krupchanka, D.; Winkler, P. State of mental healthcare systems in Eastern Europe: Do we really understand what is going on? BJPsych. Int. 2016, 13, 96–99. [Google Scholar] [CrossRef] [PubMed]
- Grabowski, J.; Witkowska, N.; Bidzan, L. Letter to the editor: Excess all-cause mortality during second wave of COVID-19—The Polish perspective. Eurosurveillance 2021, 26, 2100117. [Google Scholar] [CrossRef]
- Coelho, A.; de Bienassis, K.; Klazinga, N.; Santo, S.; Frade, P.; Costa, A.; Gaspar, T. Mental Health Patient-Reported Outcomes and Experiences Assessment in Portugal. Int. J. Environ. Res. Public Health 2022, 19, 11153. [Google Scholar] [CrossRef] [PubMed]
- Gao, W.B.; Chen, Z.Y.; Wang, Y.N. Analysis on the influence and change trend of public mentality during Sars epidemic. Community Ment. Health J. 2003, 17, 594–596. [Google Scholar]
- Özdin, S.; Bayrak, Ö.Ş. Levels and predictors of anxiety, depression and health anxiety during COVID-19 pandemic in Turkish society: The importance of gender. Int. J. Soc. Psychiatry 2020, 66, 504–511. [Google Scholar] [CrossRef]
- Huang, L.; Lei, W.; Xu, F.; Liu, H.; Yu, L. Emotional responses and coping strategies in nurses and nursing students during Covid-19 outbreak: A comparative study. PLoS ONE 2020, 15, e0237303. [Google Scholar] [CrossRef]
- Elmer, T.; Mepham, K.; Stadtfeld, C. Students under lockdown: Comparisons of students’ social networks and mental health before and during the COVID-19 crisis in Switzerland. PLoS ONE 2020, 15, e0236337. [Google Scholar] [CrossRef]
- Belcher, B.R.; Zink, J.; Azad, A.; Campbell, C.E.; Chakravartti, S.P.; Herting, M.M. The Roles of Physical Activity, Exercise, and Fitness in Promoting Resilience during Adolescence: Effects on Mental Well-Being and Brain Development. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2021, 6, 225–237. [Google Scholar] [CrossRef]
- Costa, S.; Santi, G.; di Fronso, S.; Montesano, C.; Di Gruttola, F.; Ciofi, E.G.; Morgilli, L.; Bertollo, M. Athletes and adversities: Athletic identity and emotional regulation in time of COVID-19. Sport Sci. Health 2020, 16, 609–618. [Google Scholar] [CrossRef]
- McMurray, R.; Forsythe, W.; Mar, M.; Hardy, C.J. Exercise intensity-related responses of beta-endorphin and catecholamines. Med. Sci. Sports Exerc. 1987, 19, 570–574. [Google Scholar] [CrossRef]
- Luo, Q.; Zhang, P.; Liu, Y.; Ma, X.; Jennings, G. Intervention of Physical Activity for University Students with Anxiety and Depression during the COVID-19 Pandemic Prevention and Control Period: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 15338. [Google Scholar] [CrossRef] [PubMed]
- Bailey, A.P.; Hetrick, S.E.; Rosenbaum, S.; Purcell, R.; Parker, A.G. Treating depression with physical activity in adolescents and young adults: A systematic review and meta-analysis of randomised controlled trials. Psychol. Med. 2018, 48, 1068–1083. [Google Scholar] [CrossRef] [PubMed]
- Paolucci, E.M.; Loukov, D.; Bowdish, D.M.E.; Heisz, J.J. Exercise reduces depression and inflammation but intensity matters. Biol. Psychol. 2018, 133, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Król, M.; Latosiewicz, R.; Brás, R.M.M.; Barkow, W.; Zuzda, J.G. Level of physical activity of students in Poland, Portugal and Belarus. Ann. Agric. Environ. Med. 2022, 29, 126–135. [Google Scholar] [CrossRef]
- Sax, L.; Gilmartin, S.; Bryant, A. Assessing response rate and nonresponse bias in web and paper surveys. Res. High. Ed. 2003, 44, 409–432. [Google Scholar] [CrossRef]
- Gao, J.; Zheng, P.; Jia, Y. Mental health problems and social media exposure during COVID-19 outbreak. PLoS ONE 2020, 15, e0231924. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).