
Spinal Cord Stimulation Prevents Autonomic Dysreflexia in Individuals with Spinal Cord Injury: A Case Series
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Assessments
2.2. Data Processing and Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Krassioukov, A. Autonomic function following cervical spinal cord injury. Respir. Physiol. Neurobiol. 2009, 169, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Krassioukov, A.; Weaver, L. Physical medicine and rehabilitation: State of the Art reviews. In Anatomy of the Autonomic Nervous System; Teasell, R., Baskerville, V.B., Eds.; Hanley and Belfus, Inc.: Philadelphia, PA, USA, 1996; Volume 10, Chapter 1; pp. 1–14. [Google Scholar]
- Wu, J.C.; Chen, Y.C.; Liu, L.; Chen, T.J.; Huang, W.C.; Cheng, H.; Tung-Ping, S. Increased risk of stroke after spinal cord injury: A nationwide 4-year follow-up cohort study. Neurology 2012, 78, 1051–1057. [Google Scholar] [CrossRef]
- Wan, D.; Krassioukov, A.V. Life-threatening outcomes associated with autonomic dysreflexia: A clinical review. J. Spinal Cord Med. 2014, 37, 2–10. [Google Scholar] [CrossRef]
- Forrest, G.P. Atrial fibrillation associated with autonomic dysreflexia in patients with tetraplegia. Arch. Phys. Med. Rehabil. 1991, 72, 592–594. [Google Scholar]
- Cragg, J.J.; Noonan, V.K.; Krassioukov, A.; Borisoff, J. Cardiovascular disease and spinal cord injury: Results from a national population health survey. Neurology 2013, 81, 723–728. [Google Scholar] [CrossRef]
- Guttmann, L.; Whitteridge, D. Effects of bladder distension on autonomic mechanisms after spinal cord injuries. Brain J. Neurol. 1947, 70, 361–404. [Google Scholar] [CrossRef] [PubMed]
- Mathias, C.J.; Frankel, H.L. Cardiovascular control in spinal man. Annu. Rev. Physiol. 1988, 50, 577–592. [Google Scholar] [CrossRef]
- Curt, A.; Nitsche, B.; Rodic, B.; Schurch, B.; Dietz, V. Assessment of autonomic dysreflexia in patients with spinal cord injury. J. Neurol. Neurosurg. Psychiatry 1997, 62, 473–477. [Google Scholar] [CrossRef] [PubMed]
- Stjernberg, L.; Blumberg, H.; Wallin, B.G. Sympathetic activity in man after spinal cord injury. Outflow to muscle below the lesion. Brain J. Neurol. 1986, 109 Pt 4, 695–715. [Google Scholar] [CrossRef]
- Krassioukov, A.V.; Weaver, L.C. Morphological changes in sympathetic preganglionic neurons after spinal cord injury in rats. Neuroscience 1996, 70, 211–225. [Google Scholar] [CrossRef] [PubMed]
- Krenz, N.R.; Weaver, L.C. Changes in the morphology of sympathetic preganglionic neurons parallel the development of autonomic dysreflexia after spinal cord injury in rats. Neurosci. Lett. 1998, 243, 61–64. [Google Scholar] [CrossRef]
- Maiorov, D.N.; Krenz, N.R.; Krassioukov, A.V.; Weaver, L.C. Role of spinal NMDA and AMPA receptors in episodic hypertension in conscious spinal rats. Am. J. Physiol. 1997, 273, H1266–H1274. [Google Scholar] [CrossRef] [PubMed]
- Ueno, M.; Ueno-Nakamura, Y.; Niehaus, J.; Popovich, P.G.; Yoshida, Y. Silencing spinal interneurons inhibits immune suppressive autonomic reflexes caused by spinal cord injury. Nat. Neurosci. 2016, 19, 784–787. [Google Scholar] [CrossRef] [PubMed]
- Sachdeva, R.; Hutton, G.; Marwaha, A.S.; Krassioukov, A.V. Morphological maladaptations in sympathetic preganglionic neurons following an experimental high-thoracic spinal cord injury. Exp. Neurol. 2020, 327, 113235. [Google Scholar] [CrossRef] [PubMed]
- Hou, S.; Duale, H.; Cameron, A.A.; Abshire, S.M.; Lyttle, T.S.; Rabchevsky, A.G. Plasticity of lumbosacral propriospinal neurons is associated with the development of autonomic dysreflexia after thoracic spinal cord transection. J. Comp. Neurol. 2008, 509, 382–399. [Google Scholar] [CrossRef] [PubMed]
- Krenz, N.R.; Weaver, L.C. Sprouting of primary afferent fibers after spinal cord transection in the rat. Neuroscience 1998, 85, 443–458. [Google Scholar] [CrossRef]
- Krassioukov, A.V.; Johns, D.G.; Schramm, L.P. Sensitivity of sympathetically correlated spinal interneurons, renal sympathetic nerve activity, and arterial pressure to somatic and visceral stimuli after chronic spinal injury. J. Neurotrauma 2002, 19, 1521–1529. [Google Scholar] [CrossRef]
- Faaborg, P.M.; Christensen, P.; Krassioukov, A.; Laurberg, S.; Frandsen, E.; Krogh, K. Autonomic dysreflexia during bowel evacuation procedures and bladder filling in subjects with spinal cord injury. Spinal Cord 2014, 52, 494–498. [Google Scholar] [CrossRef]
- Pan, S.L.; Wang, Y.H.; Lin, H.L.; Chang, C.W.; Wu, T.Y.; Hsieh, E.T. Intracerebral hemorrhage secondary to autonomic dysreflexia in a young person with incomplete C8 tetraplegia: A case report. Arch. Phys. Med. Rehabil. 2005, 86, 591–593. [Google Scholar] [CrossRef]
- Simpson, L.A.; Eng, J.J.; Hsieh, J.T.; Wolfe, D.L. The health and life priorities of individuals with spinal cord injury: A systematic review. J. Neurotrauma 2012, 29, 1548–1555. [Google Scholar] [CrossRef]
- Anderson, K.D. Targeting recovery: Priorities of the spinal cord-injured population. J. Neurotrauma 2004, 21, 1371–1383. [Google Scholar] [CrossRef] [PubMed]
- Krassioukov, A.; Warburton, D.E.; Teasell, R.; Eng, J.J. A systematic review of the management of autonomic dysreflexia after spinal cord injury. Arch. Phys. Med. Rehabil. 2009, 90, 682–695. [Google Scholar] [CrossRef] [PubMed]
- Krassioukov, A.; Linsenmeyer, T.A.; Beck, L.A.; Elliott, S.; Gorman, P.; Kirshblum, S.; Vogel, L.; Wecht, J.; Clay, S. Evaluation and Management of Autonomic Dysreflexia and Other Autonomic Dysfunctions: Preventing the Highs and Lows: Management of Blood Pressure, Sweating, and Temperature Dysfunction. Top. Spinal Cord Inj. Rehabil. 2021, 27, 225–290. [Google Scholar] [CrossRef]
- Grossman, E.; Messerli, F.H.; Grodzicki, T.; Kowey, P. Should a moratorium be placed on sublingual nifedipine capsules given for hypertensive emergencies and pseudoemergencies? JAMA 1996, 276, 1328–1331. [Google Scholar] [CrossRef]
- Shealy, C.N.; Mortimer, J.T.; Reswick, J.B. Electrical inhibition of pain by stimulation of the dorsal columns: Preliminary clinical report. Anesth. Analg. 1967, 46, 489–491. [Google Scholar] [CrossRef] [PubMed]
- Cameron, T. Safety and efficacy of spinal cord stimulation for the treatment of chronic pain: A 20-year literature review. J Neurosurg. 2004, 100, 254–267. [Google Scholar] [CrossRef] [PubMed]
- Samejima, S.; Henderson, R.; Pradarelli, J.; Mondello, S.E.; Moritz, C.T. Activity-dependent plasticity and spinal cord stimulation for motor recovery following spinal cord injury. Exp. Neurol. 2022, 357, 114178. [Google Scholar] [CrossRef]
- Rowald, A.; Komi, S.; Demesmaeker, R.; Baaklini, E.; Hernandez-Charpak, S.D.; Paoles, E.; Montanaro, H.; Cassara, A.; Becce, F.; Lloyd, B.; et al. Activity-dependent spinal cord neuromodulation rapidly restores trunk and leg motor functions after complete paralysis. Nat. Med. 2022, 28, 260–271. [Google Scholar] [CrossRef]
- Angeli, C.A.; Boakye, M.; Morton, R.A.; Vogt, J.; Benton, K.; Chen, Y.; Ferreira, C.K.; Harkema, S.J. Recovery of Over-Ground Walking after Chronic Motor Complete Spinal Cord Injury. N. Engl. J. Med. 2018, 379, 1244–1250. [Google Scholar] [CrossRef]
- Gill, M.L.; Grahn, P.J.; Calvert, J.S.; Linde, M.B.; Lavrov, I.A.; Strommen, J.A.; Beck, L.A.; Sayenko, D.G.; Van Straaten, M.G.; Drubach, D.I.; et al. Neuromodulation of lumbosacral spinal networks enables independent stepping after complete paraplegia. Nat. Med. 2018, 24, 1677–1682. [Google Scholar] [CrossRef]
- Samejima, S.; Shackleton, C.; Miller, T.; Moritz, C.T.; Kessler, T.M.; Krogh, K.; Sachdeva, R.; Krassioukov, A.V. Mapping the Iceberg of Autonomic Recovery: Mechanistic Underpinnings of Neuromodulation following Spinal Cord Injury. Neurosci. Rev. J. Bringing Neurobiol. Neurol. Psychiatry 2023. [Google Scholar] [CrossRef] [PubMed]
- Squair, J.W.; Gautier, M.; Mahe, L.; Soriano, J.E.; Rowald, A.; Bichat, A.; Cho, N.; Anderson, M.A.; James, N.D.; Gandar, J.; et al. Neuroprosthetic baroreflex controls haemodynamics after spinal cord injury. Nature 2021, 590, 308–314. [Google Scholar] [CrossRef]
- Herrity, A.N.; Aslan, S.C.; Mesbah, S.; Siu, R.; Kalvakuri, K.; Ugiliweneza, B.; Mohamed, A.; Hubscher, C.H.; Harkema, S.J. Targeting bladder function with network-specific epidural stimulation after chronic spinal cord injury. Sci. Rep. 2022, 12, 11179. [Google Scholar] [CrossRef] [PubMed]
- Harkema, S.J.; Ditterline, B.L.; Wang, S.; Aslan, S.; Angeli, C.A.; Ovechkin, A.; Hirsch, G.A. Epidural spinal cord stimulation training and sustained recovery of cardiovascular function in individuals with chronic cervical spinal cord injury. JAMA Neurol. 2018, 75, 1569–1571. [Google Scholar] [CrossRef]
- Darrow, D.; Balser, D.; Netoff, T.I.; Krassioukov, A.; Phillips, A.; Parr, A.; Samadani, U. Epidural Spinal Cord Stimulation Facilitates Immediate Restoration of Dormant Motor and Autonomic Supraspinal Pathways after Chronic Neurologically Complete Spinal Cord Injury. J. Neurotrauma 2019, 36, 2325–2336. [Google Scholar] [CrossRef] [PubMed]
- DiMarco, A.F.; Geertman, R.T.; Tabbaa, K.; Nemunaitis, G.A.; Kowalski, K.E. Effects of Lower Thoracic Spinal Cord Stimulation on Bowel Management in Individuals With Spinal Cord Injury. Arch. Phys. Med. Rehabil. 2021, 102, 1155–1164. [Google Scholar] [CrossRef]
- Walter, M.; Lee, A.H.X.; Kavanagh, A.; Phillips, A.A.; Krassioukov, A.V. Epidural Spinal Cord Stimulation Acutely Modulates Lower Urinary Tract and Bowel Function Following Spinal Cord Injury: A Case Report. Front. Physiol. 2018, 9, 1816. [Google Scholar] [CrossRef]
- Richardson, R.R.; Cerullo, L.J.; Meyer, P.R. Autonomic hyper-reflexia modulated by percutaneous epidural neurostimulation: A preliminary report. Neurosurgery 1979, 4, 517–520. [Google Scholar] [CrossRef] [PubMed]
- Rupp, R.; Biering-Sørensen, F.; Burns, S.P.; Graves, D.E.; Guest, J.; Jones, L.; Read, M.S.; Rodriguez, G.M.; Schuld, C.; Tansey-Md, K.E.; et al. International Standards for Neurological Classification of Spinal Cord Injury: Revised 2019. Top. Spinal Cord Inj. Rehabil. 2021, 27, 1–22. [Google Scholar] [CrossRef]
- Hubli, M.; Gee, C.M.; Krassioukov, A.V. Refined assessment of blood pressure instability after spinal cord injury. Am. J. Hypertens. 2015, 28, 173–181. [Google Scholar] [CrossRef]
- Sachdeva, R.; Nightingale, T.E.; Pawar, K.; Kalimullina, T.; Mesa, A.; Marwaha, A.; Williams, A.M.M.; Lam, T.; Krassioukov, A.V. Noninvasive Neuroprosthesis Promotes Cardiovascular Recovery After Spinal Cord Injury. Neurotherapeutics 2021, 18, 1244–1256. [Google Scholar] [CrossRef] [PubMed]
- Coggrave, M.J.; Norton, C. The need for manual evacuation and oral laxatives in the management of neurogenic bowel dysfunction after spinal cord injury: A randomized controlled trial of a stepwise protocol. Spinal Cord 2010, 48, 504–510. [Google Scholar] [CrossRef] [PubMed]
- Wecht, J.M.; Krassioukov, A.V.; Alexander, M.; Handrakis, J.P.; McKenna, S.L.; Kennelly, M.; Trbovich, M.; Biering-Sorensen, F.; Burns, S.; Elliott, S.L.; et al. International Standards to document Autonomic Function following SCI (ISAFSCI): Second Edition. Top. Spinal Cord Inj. Rehabil. 2021, 27, 23–49. [Google Scholar] [CrossRef]
- Ducla-Soares, J.L.; Santos-Bento, M.; Laranjo, S.; Andrade, A.; Ducla-Soares, E.; Boto, J.P.; Silva-Carvalho, L.; Rocha, I. Wavelet analysis of autonomic outflow of normal subjects on head-up tilt, cold pressor test, Valsalva manoeuvre and deep breathing. Exp. Physiol. 2007, 92, 677–686. [Google Scholar] [CrossRef] [PubMed]
- Pagani, M.; Lombardi, F.; Guzzetti, S.; Rimoldi, O.; Furlan, R.; Pizzinelli, P.; Sandrone, G.; Malfatto, G.; Dell’Orto, S.; Piccaluga, E.; et al. Power spectral analysis of heart rate and arterial pressure variabilities as a marker of sympatho-vagal interaction in man and conscious dog. Circ. Res. 1986, 59, 178–193. [Google Scholar] [CrossRef]
- Claydon, V.E.; Krassioukov, A.V. Clinical correlates of frequency analyses of cardiovascular control after spinal cord injury. Am. J. Physiol. Heart Circ. Physiol. 2008, 294, H668–H678. [Google Scholar] [CrossRef]
- Inskip, J.A.; Lucci, V.M.; McGrath, M.S.; Willms, R.; Claydon, V.E. A Community Perspective on Bowel Management and Quality of Life after Spinal Cord Injury: The Influence of Autonomic Dysreflexia. J. Neurotrauma 2018, 35, 1091–1105. [Google Scholar] [CrossRef]
- Pardee, C.; Bricker, D.; Rundquist, J.; MacRae, C.; Tebben, C. Characteristics of neurogenic bowel in spinal cord injury and perceived quality of life. Rehabil. Nurs. 2012, 37, 128–135. [Google Scholar] [CrossRef]
- Coggrave, M.; Norton, C.; Wilson-Barnett, J. Management of neurogenic bowel dysfunction in the community after spinal cord injury: A postal survey in the United Kingdom. Spinal Cord 2009, 47, 323–333. [Google Scholar] [CrossRef] [PubMed]
- Garshick, E.; Kelley, A.; Cohen, S.A.; Garrison, A.; Tun, C.G.; Gagnon, D.; Brown, R. A prospective assessment of mortality in chronic spinal cord injury. Spinal Cord 2005, 43, 408–416. [Google Scholar] [CrossRef] [PubMed]
- DeVivo, M.J.; Krause, J.S.; Lammertse, D.P. Recent trends in mortality and causes of death among persons with spinal cord injury. Arch. Phys. Med. Rehabil. 1999, 80, 1411–1419. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.; Lee, M.; Kiratli, J. Cardiovascular disease in spinal cord injury: An overview of prevalence, risk, evaluation, and management. Am. J. Phys. Med. Rehabil. 2007, 86, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Soriano, J.E.; Hudelle, R.; Squair, J.W.; Anderson, M.A.; Gautier, M.; Mahe, L.; Tso, M.; Amir, S.; Courtine, G.; Phillips, A.A. Long-term neuroprosthetic hemotherapy treats autonomic dysreflexia after spinal cord injury. FASEB J. 2022, 36. [Google Scholar] [CrossRef]
- Melzack, R.; Wall, P.D. Pain mechanisms: A new theory. Science 1965, 150, 971–979. [Google Scholar] [CrossRef] [PubMed]
- Daniele, C.A.; MacDermott, A.B. Low-threshold primary afferent drive onto GABAergic interneurons in the superficial dorsal horn of the mouse. J. Neurosci. Off. J. Soc. Neurosci. 2009, 29, 686–695. [Google Scholar] [CrossRef]
- Cui, J.G.; O’Connor, W.T.; Ungerstedt, U.; Linderoth, B.; Meyerson, B.A. Spinal cord stimulation attenuates augmented dorsal horn release of excitatory amino acids in mononeuropathy via a GABAergic mechanism. Pain 1997, 73, 87–95. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
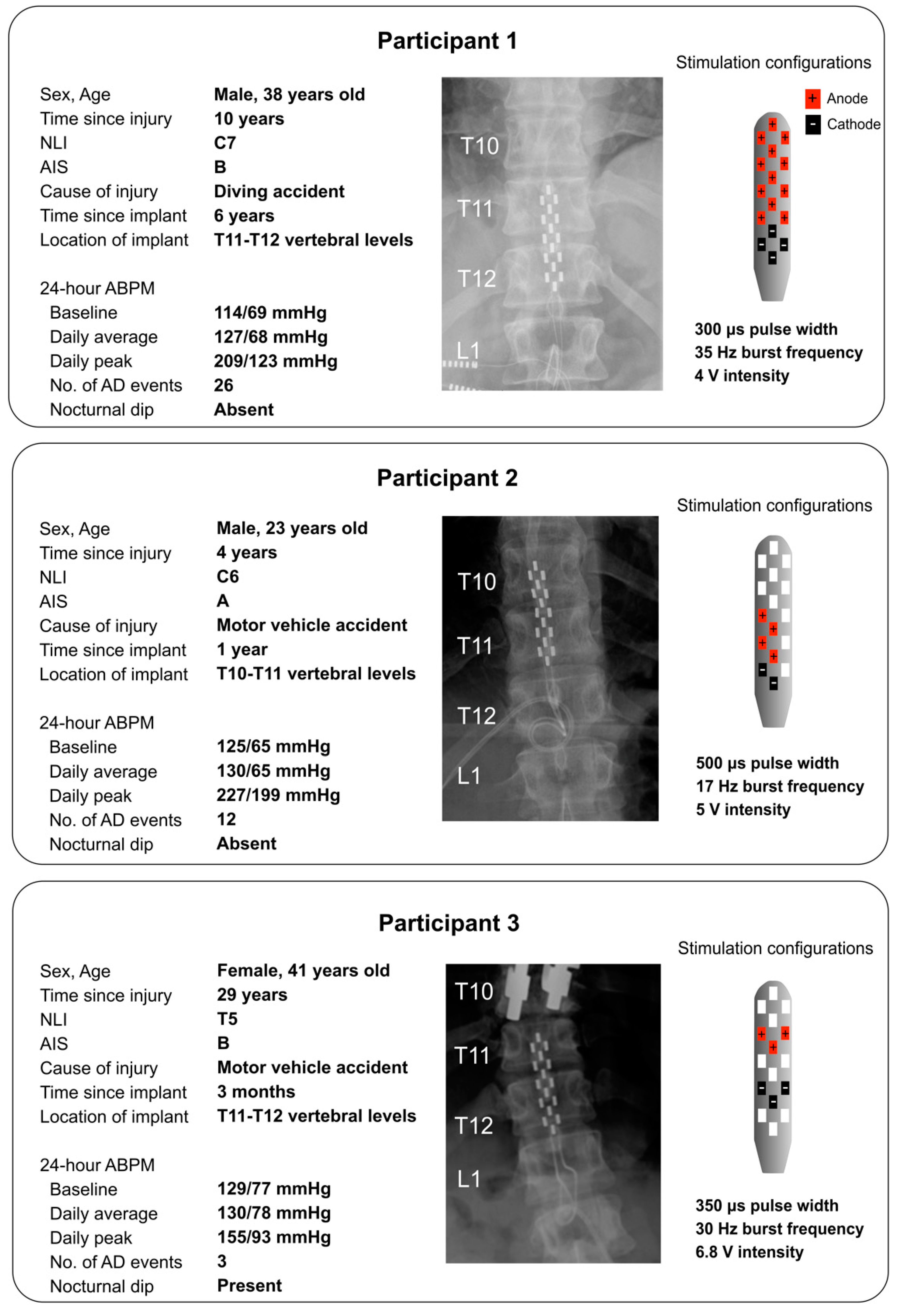
| Participant 1 | Participant 2 | Participant 3 | ||||
|---|---|---|---|---|---|---|
| Without eSCS | With eSCS | Without eSCS | With eSCS | Without eSCS | With eSCS | |
| Baseline SBP (mmHg) | 110 ± 10 | 118 ± 12 | 102 ± 2 | 96 ± 1 | 134 ± 1 | 137 ± 4 |
| Baseline DBP (mmHg) | 63 ± 7 | 66 ± 10 | 62 ± 3 | 53 ± 2 | 93 ± 5 | 91 ± 1 |
| Baseline HR (bpm) | 71 ± 8 | 71 ± 14 | 47 ± 1 | 46 ± 1 | 69 ± 0.1 | 70 ± 1 |
| Baseline LF wavelet power (a.u.) | 0.0047 ± 0.0030 | 0.0051 ± 0.0015 | 0.0050 ± 0.0044 | 0.0050 ± 0.0013 | 0.0058 ± 0.0014 | 0.0052 ± 0.0003 |
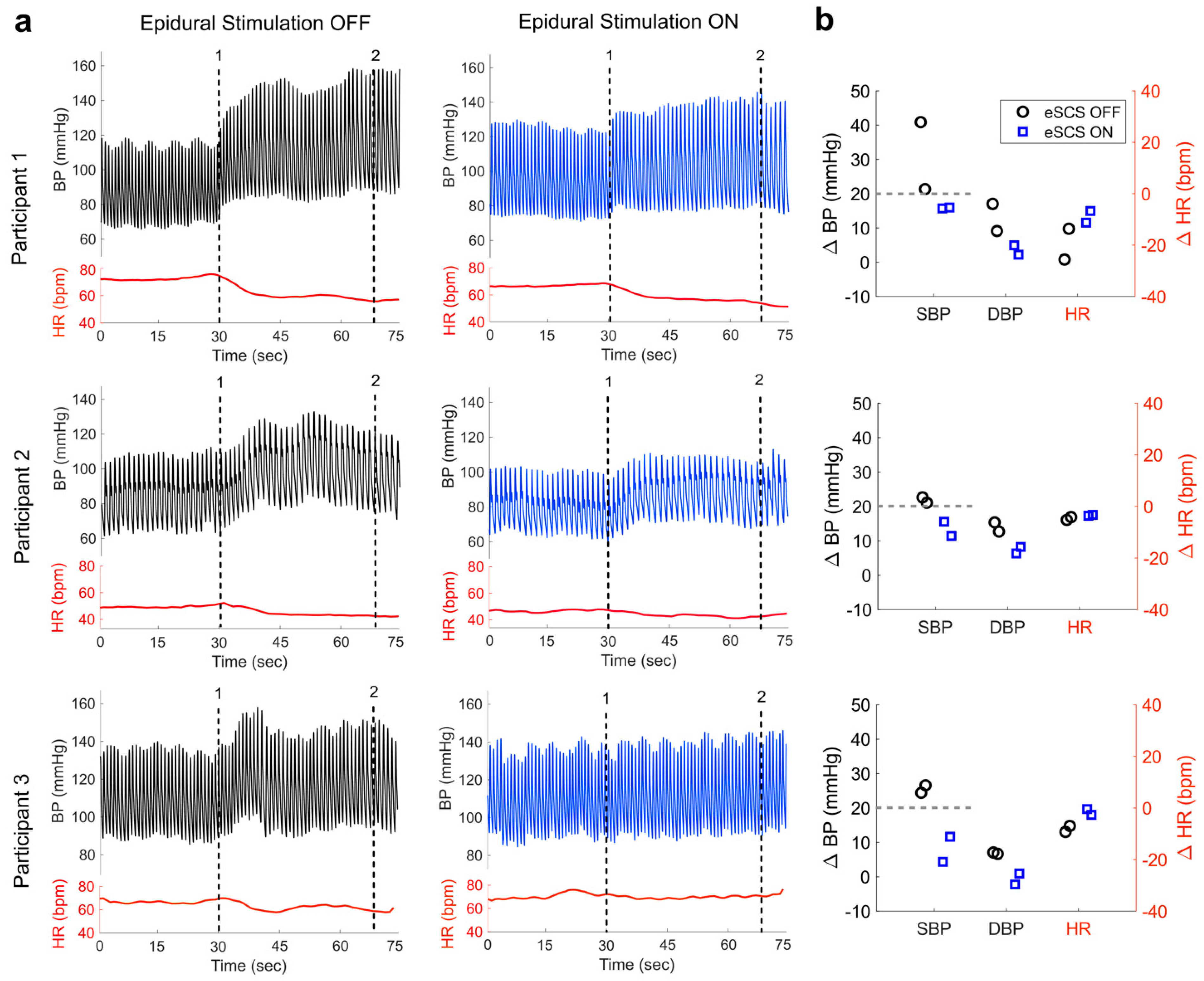
| ∆ SBP during DARS (mmHg) | 31 ± 14 | 16 ± 0.2 | 22 ± 1 | 13 ± 3 | 26 ± 2 | 8 ± 5 |
| ∆ DBP during DARS (mmHg) | 13 ± 6 | 4 ± 2 | 14 ± 2 | 7 ± 1 | 7 ± 0.2 | −1 ± 2 |
| ∆ HR during DARS (bpm) | −20 ± 8 | −9 ± 3 | −5 ± 1 | −3 ± 0.2 | −8 ± 2 | −2 ± 2 |
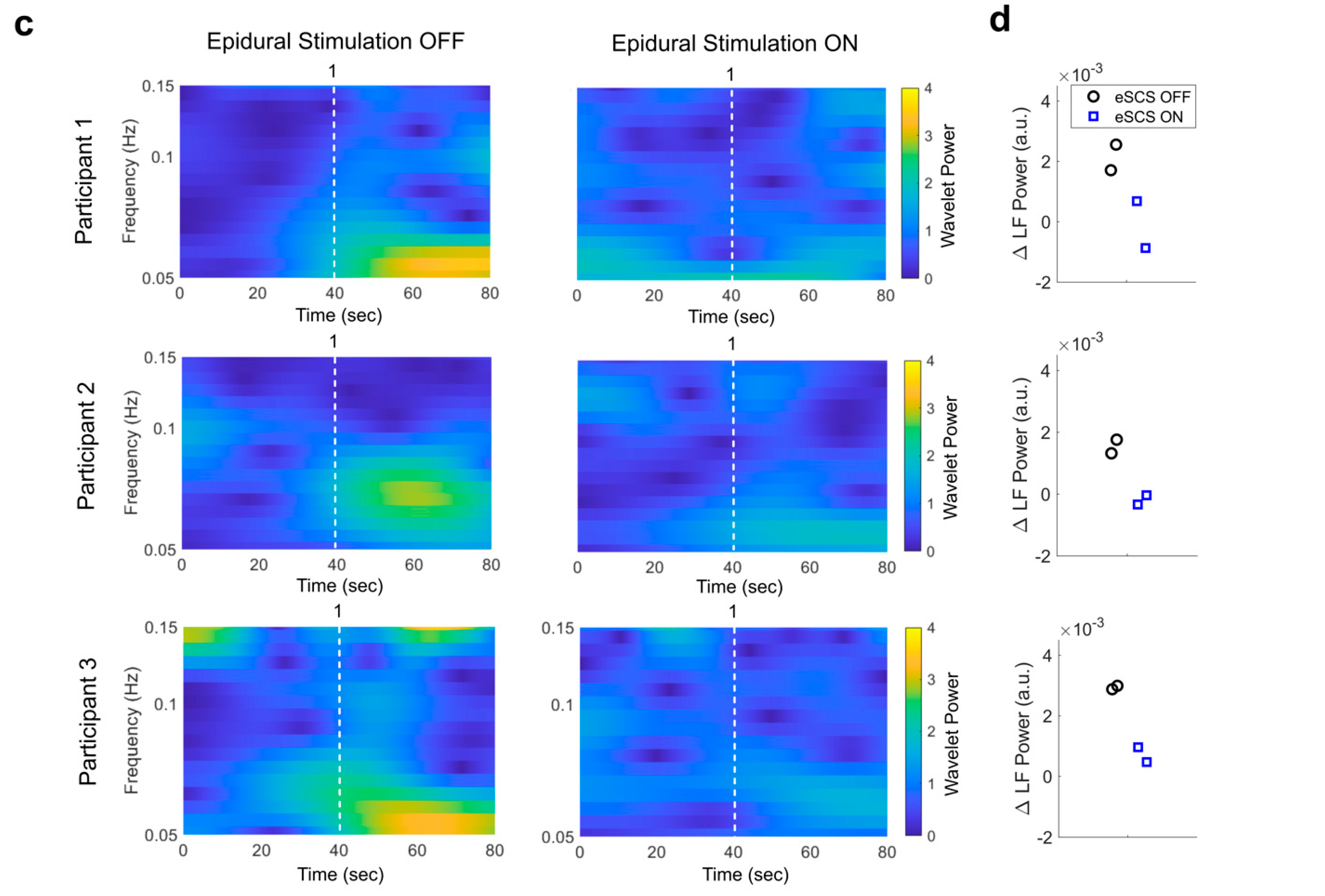
| ∆ LF wavelet power during DARS (a.u.) | 0.0021 ± 0.0006 | −0.0001 ± 0.0011 | 0.0015 ± 0.0003 | −0.0002 ± 0.0002 | 0.0029 ± 0.0001 | 0.0007 ± 0.0003 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Samejima, S.; Shackleton, C.; Malik, R.N.; Cao, K.; Bohorquez, A.; Nightingale, T.E.; Sachdeva, R.; Krassioukov, A.V. Spinal Cord Stimulation Prevents Autonomic Dysreflexia in Individuals with Spinal Cord Injury: A Case Series. J. Clin. Med. 2023, 12, 2897. https://doi.org/10.3390/jcm12082897
Samejima S, Shackleton C, Malik RN, Cao K, Bohorquez A, Nightingale TE, Sachdeva R, Krassioukov AV. Spinal Cord Stimulation Prevents Autonomic Dysreflexia in Individuals with Spinal Cord Injury: A Case Series. Journal of Clinical Medicine. 2023; 12(8):2897. https://doi.org/10.3390/jcm12082897
Chicago/Turabian StyleSamejima, Soshi, Claire Shackleton, Raza N. Malik, Kawami Cao, Anibal Bohorquez, Tom E. Nightingale, Rahul Sachdeva, and Andrei V. Krassioukov. 2023. "Spinal Cord Stimulation Prevents Autonomic Dysreflexia in Individuals with Spinal Cord Injury: A Case Series" Journal of Clinical Medicine 12, no. 8: 2897. https://doi.org/10.3390/jcm12082897
APA StyleSamejima, S., Shackleton, C., Malik, R. N., Cao, K., Bohorquez, A., Nightingale, T. E., Sachdeva, R., & Krassioukov, A. V. (2023). Spinal Cord Stimulation Prevents Autonomic Dysreflexia in Individuals with Spinal Cord Injury: A Case Series. Journal of Clinical Medicine, 12(8), 2897. https://doi.org/10.3390/jcm12082897