Comparison of Greater Occipital Nerve Blockade and Sphenopalatine Ganglion Blockade in Patients with Episodic Migraine

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
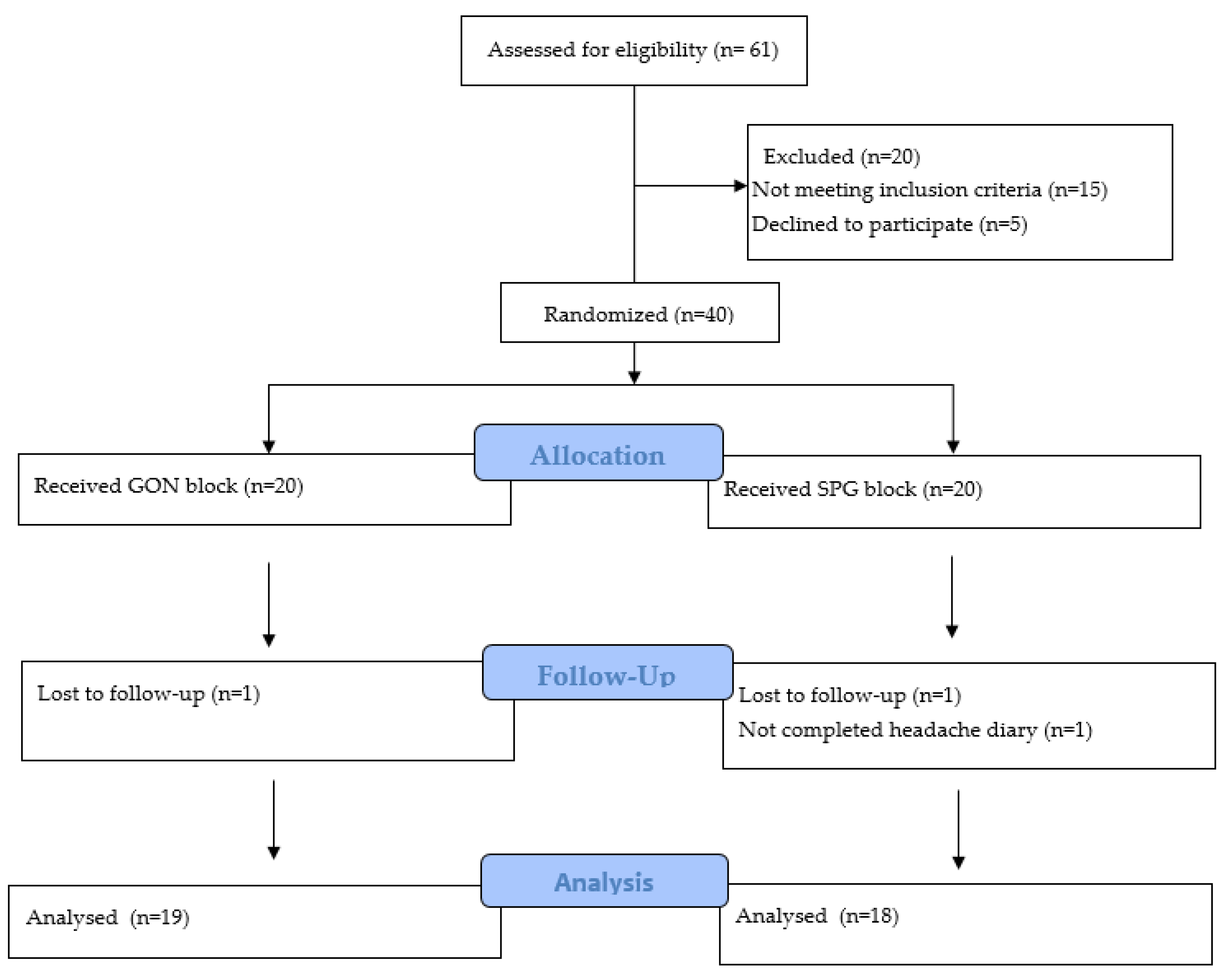
2.2. Sample Size and Randomization
2.3. Procedures and Interventions
2.4. Patient Evaluation and Outcomes
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goadsby, P.J.; Lipton, R.B.; Ferrari, M.D. Migraine—Current Understanding and Treatment. N. Engl. J. Med. 2002, 346, 257–270. [Google Scholar] [CrossRef] [PubMed]
- Headache Classification Committee of the International Headache Society (IHS). Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2019, 39, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Kong, F.; Buse, D.C. Predictors of episodic migraine transformation to chronic migraine: A systematic review and meta-analysis of observational cohort studies. Cephalalgia 2020, 40, 503–516. [Google Scholar] [CrossRef] [PubMed]
- Robbins, M.S. Diagnosis and Management of Headache. JAMA 2021, 325, 1874–1885. [Google Scholar] [CrossRef] [PubMed]
- Warhurst, S.; Rofe, C.J.; Brew, B.J.; Bateson, D.; McGeechan, K.; Merki-Feld, G.S.; Garrick, R.; Tomlinson, S.E. Effectiveness of the progestin-only pill for migraine treatment in women: A systematic review and meta-analysis. Cephalalgia 2018, 38, 754–764. [Google Scholar] [CrossRef] [PubMed]
- Sun-Edelstein, C.; Rapoport, A.M. Update on the Pharmacological Treatment of Chronic Migraine. Curr. Pain Headache Rep. 2016, 20, 6. [Google Scholar] [CrossRef] [PubMed]
- Plato, B.M.; Whitt, M. Interventional Procedures in Episodic Migraine. Curr. Pain Headache Rep. 2020, 24, 75. [Google Scholar] [CrossRef] [PubMed]
- Blumenfeld, A.M.; Bloudek, L.M.; Becker, W.J.; Buse, D.C.; Varon, S.F.; Maglinte, G.A.; Wilcox, T.K.; Kawata, A.K.; Lipton, R.B. Patterns of Use and Reasons for Discontinuation of Prophylactic Medications for Episodic Migraine and Chronic Migraine: Results from the Second International Burden of Migraine Study (IBMS-II). Headache J. Head Face Pain 2013, 53, 644–655. [Google Scholar] [CrossRef] [PubMed]
- Mousa, M.A.; Aria, D.J.; Mousa, A.A.; Schaefer, C.M.; Temkit, M.H.H.; Towbin, R.B. Sphenopalatine ganglion nerve block for the treatment of migraine headaches in the pediatric population. Pain Physician 2021, 24, E111–E116. [Google Scholar]
- Nagib, M.; Hood, P.; Matteo, J. Sphenopalatine Ganglion Block: Treatment of Migraine and Trigeminal Neuralgia Associated with Multiple Sclerosis. Cureus 2020, 12, e8522. [Google Scholar] [CrossRef]
- Newman-Norlund, R.D.; Rorden, C.; Maleki, N.; Patel, M.; Cheng, B.; Androulakis, X.M. Cortical and subcortical changes following sphenopalatine ganglion blocks in chronic migraine with medication overuse headache: A preliminary longitudinal study. Women’s Midlife Health 2020, 6, 7. [Google Scholar] [CrossRef]
- Cady, R.K.; Saper, J.; Dexter, K.; Cady, R.J.; Manley, H.R. Long-Term Efficacy of a Double-Blind, Placebo-Controlled, Randomized Study for Repetitive Sphenopalatine Blockade with Bupivacaine vs Saline with the Tx360 Device for Treatment of Chronic Migraine. Headache J. Head Face Pain 2015, 55, 529–542. [Google Scholar] [CrossRef]
- Cady, R.; Saper, J.; Dexter, K.; Manley, H.R. A Double-Blind, Placebo-Controlled Study of Repetitive Transnasal Sphenopalatine Ganglion Blockade with Tx360 as Acute Treatment for Chronic Migraine. Headache J. Head Face Pain 2014, 55, 101–116. [Google Scholar] [CrossRef]
- Hasoon, J.; Berger, A. Sphenopalatine ganglion block for abortive treatment of a migraine headache. Saudi J. Anaesth. 2020, 14, 548–549. [Google Scholar] [CrossRef]
- Binfalah, M.; Alghawi, E.; Shosha, E.; Alhilly, A.; Bakhiet, M. Sphenopalatine Ganglion Block for the Treatment of Acute Migraine Headache. Pain Res. Treat. 2018, 2018, 2516953. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, D.; Tomar, A.; Deorari, V.; Duggal, A.; Krishnan, A.; Koul, A. Greater occipital nerve blockade for the preventive treatment of chronic migraine: A randomized double-blind placebo-controlled study. Cephalalgia 2023, 43, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Ulusoy, E.K.; Bolattürk, F. The effect of greater occipital nerve blockade on the quality of life, disability and comorbid depression, anxiety, and sleep disturbance in patients with chronic migraine. Neurol. Sci. 2020, 41, 1829–1835. [Google Scholar] [CrossRef]
- Inan, L.E.; Inan, N.; Karadaş, Ö.; Gül, H.L.; Erdemoğlu, A.K.; Türkel, Y.; Akyol, A. Greater occipital nerve blockade for the treatment of chronic migraine: A randomized, multicenter, double-blind, and placebo-controlled study. Acta Neurol. Scand. 2015, 132, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Okmen, K.; Dagistan, Y.; Dagistan, E.; Kaplan, N.; Cancan, E. Efficacy of the greater occipital nerve block in recurrent migraine type headaches. Neurol. I Neurochir. Pol. 2016, 50, 151–154. [Google Scholar] [CrossRef]
- Zhang, H.; Yang, X.; Lin, Y.; Chen, L.; Ye, H. The efficacy of greater occipital nerve block for the treatment of migraine: A systematic review and meta-analysis. Clin. Neurol. Neurosurg. 2018, 165, 129–133. [Google Scholar] [CrossRef]
- Candido, K.D.; Massey, S.T.; Sauer, R.; Darabad, R.R.; Knezevic, N.N. A novel revision to the classical transnasal topical sphenopalatine ganglion block for the treatment of headache and facial pain. Pain Physician 2013, 16, E769–E778. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, K.; Arvidsson, J. Central distribution of trigeminal and upper cervical primary afferents in the rat studied by anterograde transport of horseradish peroxidase conjugated to wheat germ agglutinin. J. Comp. Neurol. 1988, 268, 91–108. [Google Scholar] [CrossRef] [PubMed]
- Bartsch, T.; Goadsby, P.J. Stimulation of the greater occipital nerve induces increased central excitability of dural afferent input. Brain 2002, 125, 1496–1509. [Google Scholar] [CrossRef]
- Piovesan, E.; Kowacs, P.; Tatsui, C.; Lange, M.; Ribas, L.; Werneck, L. Referred Pain After Painful Stimulation of the Greater Occipital Nerve in Humans: Evidence of Convergence of Cervical Afferences on Trigeminal Nuclei. Cephalalgia 2001, 21, 107–109. [Google Scholar] [CrossRef] [PubMed]
- Kesserwani, H. Migraine Triggers: An Overview of the Pharmacology, Biochemistry, Atmospherics, and Their Effects on Neural Networks. Cureus 2021, 13, e14243. [Google Scholar] [CrossRef] [PubMed]
- Robbins, M.S.; Robertson, C.E.; Kaplan, E.; Ailani, J.; Charleston, L.; Kuruvilla, D.; Blumenfeld, A.; Berliner, R.; Rosen, N.L.; Duarte, R.; et al. The Sphenopalatine Ganglion: Anatomy, Pathophysiology, and Therapeutic Targeting in Headache. Headache J. Head Face Pain 2016, 56, 240–258. [Google Scholar] [CrossRef] [PubMed]
- Yarnitsky, D.; Goor-Aryeh, I.; Bajwa, Z.H.; Ransil, B.I.; Cutrer, F.M.; Sottile, A.; Burstein, R. 2003 Wolff Award: Possible Parasympathetic Contributions to Peripheral and Central Sensitization During Migraine. Headache J. Head Face Pain 2003, 43, 704–714. [Google Scholar] [CrossRef]
- Ho, K.W.D.; Przkora, R.; Kumar, S. Sphenopalatine ganglion: Block, radiofrequency ablation and neurostimulation—A systematic review. J. Headache Pain 2017, 18, 118. [Google Scholar] [CrossRef]
- Krebs, K.; Rorden, C.; Androulakis, X.M. Resting State Functional Connectivity After Sphenopalatine Ganglion Blocks in Chronic Migraine with Medication Overuse Headache: A Pilot Longitudinal fMRI Study. Headache J. Head Face Pain 2018, 58, 732–743. [Google Scholar] [CrossRef]
- Piagkou, M.; Demesticha, T.; Troupis, T.; Vlasis, K.; Skandalakis, P.; Makri, A.; Mazarakis, A.; Lappas, D.; Piagkos, G.; Johnson, E.O. The Pterygopalatine Ganglion and its Role in Various Pain Syndromes: From Anatomy to Clinical Practice. Pain Pract. 2011, 12, 399–412. [Google Scholar] [CrossRef]
- Felisati, G.; Arnone, F.; Lozza, P.; Leone, M.; Curone, M.; Bussone, G. Sphenopalatine Endoscopic Ganglion Block: A Revision of a Traditional Technique for Cluster Headache. Laryngoscope 2006, 116, 1447–1450. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.E.; Kim, J.E.; Lee, S.Y.; Gil, H.Y.; Min, S.K.; Park, B.; Kim, S.I.; Cho, R.Y.; Koh, J.C.; Choi, Y.H.; et al. Comparison of Temperature and Pain Changes between the Drip and Topical Methods of Administering the Transnasal Sphenopalatine Ganglion Block. J. Pers. Med. 2022, 12, 830. [Google Scholar] [CrossRef] [PubMed]
- Rapoport, A.M.; Edvinsson, L. Some aspects on the pathophysiology of migraine and a review of device therapies for migraine and cluster headache. Neurol. Sci. 2019, 40, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Kang, J.; Zhang, Y.; Zhang, X. Influence of greater occipital nerve block on pain severity in migraine patients: A systematic review and meta-analysis. Am. J. Emerg. Med. 2017, 35, 1750–1754. [Google Scholar] [CrossRef] [PubMed]
- Karaoğlan, M.; İnan, L.E. A comparison of the clinical efficacy of GON block at the C2 level and GON block at the classical distal occipital level in the treatment of migraine. Clin. Neurol. Neurosurg. 2022, 215, 107190. [Google Scholar] [CrossRef] [PubMed]
- Guner, D.; Bilgin, S. Efficacy of Adding a Distal Level Block to a C2 Level Greater Occipital Nerve Block under Ultrasound Guidance in Chronic Migraine. Ann. Indian Acad. Neurol. 2023, 26, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Emadi, F.; Sharif, F.; Shaygan, M.; Sharifi, N.; Ashjazadeh, N. Comparison of Pain-Related and Psychological Variables between Acute and Chronic Migraine Patients, and Factors Affecting Headache Chronicity. Int. J. Community Based Nurs. Midwifery 2019, 7, 192–200. [Google Scholar] [CrossRef]
- Rezaeian, S.; Hamzeh, B.; Darbandi, M.; Najafi, F.; Shakiba, E.; Pasdar, Y. Factors associated with chronic headache among adults: Results from a Ravansar noncommunicable disease cohort study. East. Mediterr. Health J. 2023, 29, 620–629. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, B.K. Migraine and tension-type headache in a general population: Psychosocial factors. Int. J. Epidemiol. 1992, 21, 1138–1143. [Google Scholar] [CrossRef]
- Wilkins, K.; Beaudet, M.P. Work stress and health. Health Rep. 1998, 10, 47–62. [Google Scholar]
- Ha, H.; Gonzalez, A. Migraine Headache Prophylaxis. Am. Fam. Physician 2019, 99, 17–24. [Google Scholar] [PubMed]

{kind=link}
| Variables | Groups | Test Statistics | ||||
|---|---|---|---|---|---|---|
| GON Block n = 19 | SPG Block n = 18 | Test Value | p-Value | |||
| Age | 33.5 ± 7.6 | 35.3 ± 8.5 | 0.680 | 0.501 † | ||
| Gender, n (%) | ||||||
| Female | 13 | 68.4 | 11 | 61.1 | 0.015 | 0.904 Φ |
| Male | 6 | 31.6 | 7 | 38.9 | ||
| Education n (%) | 3.478 | 0.150 ¥ | ||||
| University | 11 | 57.9 | 15 | 83.3 | ||
| High school | 7 | 36.8 | 2 | 11.1 | ||
| Primary school | 1 | 5.3 | 1 | 5.6 | ||
| Marital status, n (%) | 0.948 | 0.746 ¥ | ||||
| Single | 7 | 36.8 | 9 | 50.0 | ||
| Married | 11 | 57.9 | 8 | 44.4 | ||
| Divorced | 1 | 5.3 | 1 | 5.6 | ||
| Prophylactic med, n (%) | 3.975 | 0.614 ¥ | ||||
| Beta-blockers | 5 | 26.3 | 6 | 33.3 | ||
| Ca channel Blockers | 4 | 21.1 | 7 | 38.9 | ||
| TSA | 3 | 15.8 | 3 | 16.7 | ||
| SSNRI | 4 | 21.1 | 1 | 5.6 | ||
| VPA | 2 | 10.5 | 1 | 5.6 | ||
| TPM | 1 | 5.3 | 0 | 0.0 | ||
| Groups | Test Statistics | ||||
|---|---|---|---|---|---|
| GON Block | SPG Block | Test Value | p Value & | ||
| Intensity | Baseline | 7.0 (5.0–8.0) | 6.0 (4.0–8.0) | 1.286 | 0.198 |
| 1st month | 4.0 (2.0–7.0) * | 5.5 (4.0–6.0) | 3.525 | <0.001 | |
| 2nd month | 4.0 (3.0–5.0) * | 5.0 (4.0–6.0) * | 3.847 | <0.001 | |
| 3rd month | 4.0 (2.0–4.0) * | 5.0 (4.0–6.0) * | 5.041 | <0.001 | |
| Difference (baseline-3rd month) | 3.0 (1.0–4.0) | 0.0 (−1.0–3.0) | 4.608 | <0.001 | |
| Test value; p value ‡ | 43.082; <0.001 | 15.270; 0.002 | |||
| Duration | Baseline | 24.0 (6.0–48.0) | 18.0 (4.0–48.0) | 1.972 | 0.049 |
| 1st month | 6.0 (3.0–24.0) * | 4.0 (2.0–24.0) * | 2.397 | 0.017 | |
| 2nd month | 4.0 (1.0–8.0) * | 4.0 (3.0–12.0) * | 1.279 | 0.201 | |
| 3rd month | 3.0 (1.0–6.0) * | 4.0 (2.0–12.0) * | 1.949 | 0.051 | |
| Difference (baseline-3rd month) | 20.0 (2.0–47.0) | 14.0 (0.0–36.0) | 2.297 | 0.022 | |
| Test value; p value ‡ | 47.873; <0.001 | 43.575; <0.001 | |||
| Day | Baseline | 6.0 (4.0–10.0) | 4.0 (3.0–8.0) | 2.398 | 0.016 |
| 1st month | 1.0 (0.0–3.0) * | 3.0 (1.0–4.0) * | 4.267 | <0.001 | |
| 2nd month | 1.0 (0.0–3.0) * | 2.0 (1.0–4.0) * | 4.362 | <0.001 | |
| 3rd month | 1.0 (0.0–3.0) * | 3.0 (1.0–4.0) * | 4.691 | <0.001 | |
| Difference (baseline-3rd month) | 5.0 (3.0–9.0) | 2.0 (1.0–4.0) | 5.018 | <0.001 | |
| Test value; p value ‡ | 47.870; <0.001 | 46.467; <0.001 | |||
| MIDAS | Baseline | 16.0 (8.0–42.0) | 15.0 (8.0–24.0) | 1.058 | 0.290 |
| 3rd month | 2.0 (0.0–8.0) | 9.0 (4.0–14.0) | 4.681 | <0.001 | |
| Difference (baseline-3rd month) | 13.0 (4.0–41.0) | 6.0 (4.0–12.0) | 4.369 | <0.001 | |
| Test value; p value † | 3.828; <0.001 | 3.758; <0.001 | |||
| Groups | Test Statistics | ||||
|---|---|---|---|---|---|
| GON Block | SPG Block | Test Value | p Value & | ||
| Number of NSAID days | Baseline | 6.0 (3.0–8.0) | 4.0 (2.0–8.0) | 2.482 | 0.013 |
| 1st month | 2.0 (1.0–4.0) * | 3.0 (1.0–5.0) * | 2.189 | 0.029 | |
| 2nd month | 2.0 (1.0–4.0) * | 2.0 (1.0–4.0) * | 0.117 | 0.907 | |
| 3rd month | 2.0 (1.0–3.0) * | 3.0 (1.0–5.0) * | 2.769 | 0.006 | |
| Difference (baseline-3rd month) | 4.0 (1.0–7.0) | 2.0 (0.0–3.0) | 4.29 | <0.001 | |
| Test value; p value ‡ | 49.336; <0.001 | 46.050; <0.001 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Unal, H.A.; Basarı, A.; Celiker, O.S.; Cakar Turhan, K.S.; Asik, I.; Ozgencil, G.E. Comparison of Greater Occipital Nerve Blockade and Sphenopalatine Ganglion Blockade in Patients with Episodic Migraine. J. Clin. Med. 2024, 13, 3027. https://doi.org/10.3390/jcm13113027
Unal HA, Basarı A, Celiker OS, Cakar Turhan KS, Asik I, Ozgencil GE. Comparison of Greater Occipital Nerve Blockade and Sphenopalatine Ganglion Blockade in Patients with Episodic Migraine. Journal of Clinical Medicine. 2024; 13(11):3027. https://doi.org/10.3390/jcm13113027
Chicago/Turabian StyleUnal, Hanzade Aybuke, Ahmet Basarı, Opal Sezgi Celiker, Keziban Sanem Cakar Turhan, Ibrahim Asik, and Gungor Enver Ozgencil. 2024. "Comparison of Greater Occipital Nerve Blockade and Sphenopalatine Ganglion Blockade in Patients with Episodic Migraine" Journal of Clinical Medicine 13, no. 11: 3027. https://doi.org/10.3390/jcm13113027
APA StyleUnal, H. A., Basarı, A., Celiker, O. S., Cakar Turhan, K. S., Asik, I., & Ozgencil, G. E. (2024). Comparison of Greater Occipital Nerve Blockade and Sphenopalatine Ganglion Blockade in Patients with Episodic Migraine. Journal of Clinical Medicine, 13(11), 3027. https://doi.org/10.3390/jcm13113027