Abstract
Background: Coronary arteries originate from the first portion of the aorta, emerging from the right and left aortic sinuses. They traverse through the subepicardium and coronary sulcus to supply the myocardium during diastolic function. The objective of this review was to understand how the hypoplasia and agenesis of the coronary arteries are associated with cardiac pathologies. Methods: The databases Medline, Scopus, Web of Science, Google Scholar, CINAHL, and LILACS were researched until January 2024. An assurance tool for anatomical studies (AQUA) was used to evaluate methodological quality. The pooled prevalence was estimated using a random effects model. Results: A total of three studies met the established selection criteria for inclusion in this meta-analysis. The prevalence of coronary artery variants was 3% (CI = 2% to 8%), with a heterogeneity of 77%. The other studies were analyzed descriptively, along with their respective clinical considerations in the presence of the variant. Conclusions: Hypoplasia and the congenital absence of the coronary arteries are often incidental findings and understanding these variants is crucial to prevent misdiagnosis. Additionally, it is essential to exercise caution when considering surgical management for hearts with these variants.
1. Introduction
Coronary arteries originate from the first portion of the aorta, emerging from the right and left aortic sinuses [1]. The right coronary artery (RCA) has an anterior to posterior path through the coronary sulcus, where it originates its branches, highlighting, due to its importance, the sinus node artery, right marginal artery, and the posterior descending artery. Altogether, these branches provide the blood supply to most of the heart tissue [1].
The left main coronary artery (LMCA) has a short path in the coronary sulcus. It originates, almost immediately, the left anterior descending artery (LDA) and the left circumflex artery (LCx). LCx arteries follow the coronary sulcus on the left side and originate the left marginal artery in charge of the blood supply of the left ventricle (Loukas et al., 2013 [1]). However, coronary arteries have normal anatomical variations, especially in the dominance of the heart blood supply. The most common dominance is the RCA (81.6%), followed by LCx (12.2%), and the least common is the co-dominance (6.2%) in heart irrigation [2]. These variations between subjects take relevance when presenting coronary artery disease, where the blood supply can be affected in the dominant vessel.
The embryological development of the coronary system is essential when mentioning anomalies such as hypoplasia and the absence of the coronary arteries, since most of them have their origin in intrauterine life. Prior to coronary embryogenesis, the heart is a thin muscular layer that oxygenates through diffusion. After its thickening, it requires the development of a vascular plexus that will mature through anastomosing with the aorta and provide the myocardial tissue with blood, oxygen, and nutrients. It is imperative to mention the signaling pathways involved in the process of the normal coronary development, such as Tbx5, Tbx18 and Vegf-A/Vegfr2, as some studies show that through the knockout of the cell or molecules involved in the pathways, they can produce relevant anomalies in the coronary arteries such as hypoplasia or congenital absence. Coronary artery development is a complex vasculogenic process that begins shortly after the cardiac loop. Coronary vasculogenesis is regulated by the myocardium but depends spatially and temporally on the epicardium and its precursor, the proepicardial organ, for the supply of coronary vascular progenitor cells. Changes in the disposition of cardiac precursors may be the cause of coronary alterations such as hypoplasia [3,4,5].
The absence of the coronary artery is a rare congenital defect. According to an angiographic imaging study, only 0.056% of the 30,230 subjects presented a single coronary artery, where 65% originated from the right sinus of the Valsalva and 35% from the left side [4]. It can be said that the congenital absence of the LMCA is more common. However, it is worth mentioning that the absence of LMCA branches, such as LCx, is far more common, where the complete congenital absence of the LMCA has a much lower prevalence at 0.024% [5]. In general, the hypoplasia or congenital absence of a coronary artery does not have clinical relevance, being an asymptomatic and incidental finding. The clinical relevance of these anatomical defects manifests when coexisting with coronary artery disease, where the single coronary artery cannot provide the blood supply of its own territory and the territory of the missing artery, resulting in myocardial ischemia due to a lack of oxygen and nutrients. Coronary artery disease can be the cause of different ischemia-like symptoms such as exertion angina, syncope, or episodic tachycardia in patients with congenital coronary artery defects. A study reports that 15% of the patients with the congenital absence of a coronary artery have ischemic damage due to its condition [6]. The most serious consequence of the congenital absence of a coronary artery is sudden death due to the complete occlusion of the super-dominant artery. Coronary anomalies are the second most common cause of sudden death in healthy-looking young people [7].
Therefore, this review aims to analyze and characterize congenital coronary artery diseases such as the hypoplasia and absence of coronary arteries, along with highlighting their importance for differential diagnosis in patients with ischemia-like symptoms and its cardiologic repercussions.
2. Methods
2.1. Protocol and Registration
This systematic review and meta-analysis adhered to the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [8]. The registration number in the International Prospective Register of Systematic Reviews (PROSPERO) is CRD42024520734.
2.2. Eligibility Criteria
Studies included in this review were selected using the following criteria:
(1) Population: Samples from cadaveric dissections and live images of hypoplastic coronary artery diseases (HCAD); (2) Results: Examination of the prevalence of CA variants and their correlation with hearth pathologies, with a specific focus on abnormalities of the CA. In addition, anatomical variants were classified and described based on normal anatomy and classifications and descriptions proposed in the literature; (3) Studies: Research articles and case reports involving only human samples, and original research published in English in peer-reviewed journals and indexed in the reviewed databases. Excluded from consideration were letters to the editor.
2.3. Electronic Search
The systematic research was performed using the subsequent databases: MEDLINE (via PubMed), Web of Science, Google Scholar, the Cumulative Index to Nursing and Allied Health Literature (CINAHL), Scopus, and the Latin American and the Caribbean Literature in Health Sciences (LILACS) from inception until January 2024. The search strategy involved a combination of the following terms: “Anatomy coronary artery” (no mesh), “Hypoplastic coronary artery” (no mesh), “agenesis coronary artery” (no mesh), “clinical anatomy” (no mesh), “irrigation heart” (no mesh), “congenital absence of coronary arteries” (no mesh), and “variations anatomical” (no mesh), using the Boolean connectors AND, OR, and NOT. The search strategies for each database are available in the Supplementary Material.
2.4. Study Selection
Two authors (CAA and JDV) independently screened the titles and abstracts of references retrieved from the searches. The full text was obtained for references that either author considered potentially relevant. We involved a third reviewer (JV) if consensus could not be reached. The inter-evaluator validity was assessed using the Kappa index, yielding a value of 0.68.
2.5. Data Collection Process
Two authors (MO and AQ) independently extracted data on the outcomes of each study. The following data were extracted from the original reports: (i) Authors and year of publication, (ii) Country, (iii) Age and sex, (iv) Prevalence, (v) Clinical history, (vi) Circumstances, (vii) HCAD (Hypoplasia of the Coronary Artery Disease), (viii) Congenital absence of the Coronary Artery, (ix) Aberrant origin, (x) Other, and (xi) Clinical implications.
2.6. Assessment of the Methodological Quality of the Included Studies
The quality assessment was performed using the methodological quality assurance tool for anatomical studies (AQUA) proposed by the International Evidence-Based Anatomy Working Group (IEBA) [9]. Data extraction and quality assessment were independently performed by two reviewers (JJV and CR). We involved a third reviewer (JSG) if a consensus could not be reached. The agreement rate between the reviewers was calculated using Kappa statistics 0.80.
2.7. Statistical Methods
The data extracted from the meta-analysis were interpreted by calculating the VAH prevalence using JAMOVI software (Version 1.12) [accessed January 2024]. The DerSimonian–Laird model with a Freeman–Tukey double arcsine transformation was used to combine the summary data. In addition, a random effects model was used, because the VAH prevalence data were highly heterogeneous. The degree of heterogeneity between included studies was assessed using the chi2 test and the heterogeneity (I2) statistic. For the chi2 test, the p value proposed by the Cochrane collaboration was considered significant at 0.10. Values of the I2 statistic were interpreted with a 95% confidence interval [CI] in the following way: 0–40% might not be important, 30–60% might indicate moderate heterogeneity, 50–90% might represent substantial heterogeneity, and 75–100% could represent a significant amount of heterogeneity.
3. Results
3.1. Included Articles
A total of 195 articles from different databases met the criteria and search terms established by the research team. The filter was applied to the titles and/or abstracts of the articles in the consulted databases, and the primary criterion for eliminating duplicates was used. Subsequently, 112 full-text articles were evaluated for their eligibility for inclusion in this meta-analysis and systematic review. Eighty-eight studies were excluded due to discrepancies between their primary and secondary results compared to those of this review, or because they failed to meet the established criteria for good data extraction. Therefore, 39 articles [10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48] were selected for this study (n = 140,137) (including patients, images, and cadavers) (Figure 1).
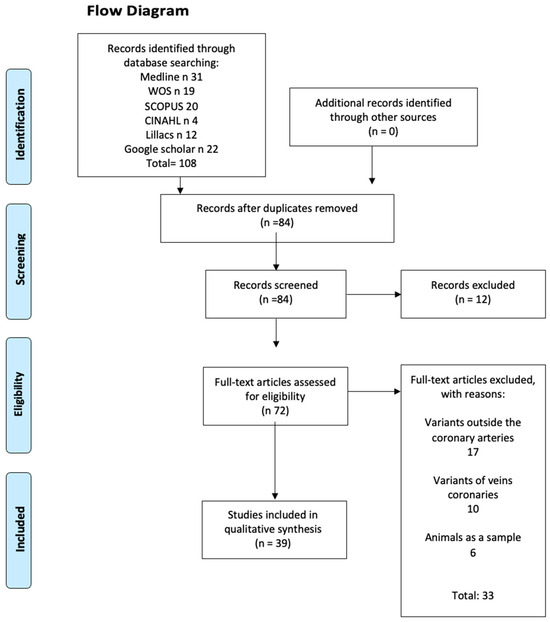
Figure 1.
Flow chart CA.
3.2. Characteristics of the Studies and Population
Of the 39 studies included in this review (as listed in Table 1 and Table 2), 19 articles are from Asia [11,12,13,19,20,21,23,27,33,35,36,37,39,41,43,45,46,47,48], 10 are from Europe [13,16,17,22,26,30,31,32,34,40], 8 are from North America [10,15,18,24,25,29,38,44], 1 is from South America [28], and 1 is from Oceania [42]. Therefore, the total number of subjects is 140,137, among whom 811 presented coronary artery variants, with an average age of diagnosis of 41.4 years.

Table 1.
Geographic distribution with variants of the CA.
Table 2.
Characteristics of the included studies.
3.3. Variant Description
3.3.1. Right Coronary Artery Variants
The right coronary artery (RCA) usually emerges from the first portion of the aorta. The development of the coronary arteries begins between the sixth and seventh weeks of intrauterine life; this period is where congenital anomalies, such as the hypoplasia or absence of coronary arteries occur. The variants and the repercussions they may cause in the function of the heart were analyzed, and featured in 16 articles:
The congenital absence of the RCA was found in nine articles [10,12,16,19,22,26,27,30,45], with a total of ten study subjects, characterizing this abnormality as the complete absence of the RCA or one of its branches. This variation results in insufficient blood supply in the RCA territory of the heart, which may lead to myocardial ischemia during exertion. To compensate for this deficiency, the heart may supply this area by extending the irrigation territory of the left main coronary artery (LMCA) or its branches to ensure proper blood supply to the heart.
The super dominance of the circumflex artery (LCx) was found, mentioned in three studies featuring three subjects [10,22,27], followed by LMCA super dominance in two studies with two subjects [22,45]. For this reason, this variant is mainly asymptomatic and only exhibits symptoms during exertion.
Another coronary variant found was hypoplastic RCA, with five studies showing that 563 subjects out of a total of 5957 have this anomaly [17,24,38,39,42]. Right hypoplastic coronary artery disease refers to the partial absence or incomplete development of the RCA or its branches. This anomaly has the same consequences as the absence of the vessel, such as ischemia due to insufficient blood supply to the heart during exertion. In one study, hypoplastic RCA was found along with other anatomical pathologies such as single RCA, split RCA, and the abnormal origin of the RCA [11]. Although hypoplasia is believed to be a congenital disorder, we found one study that identified, through genomic sequencing, a NOTCH1 c.1023CA mutation that can cause H-RCA [37].
3.3.2. Left Coronary Artery Variants
The left main coronary artery (LMCA) also arises from the aorta, having a short course before the circumflex artery (LCx) and the left anterior descending artery (LAD) emerge. The congenital anomalies, such as congenital absence and hypoplastic LMCA or its branches, occur during the gestation period, and their effects on blood supply and the function of the heart were analyzed.
The complete absence of the LMCA was found in eight studies with 632 subjects out of a total of 7507 [11,15,26,30,33,40,46,48]. The authors concluded that the congenital absence of the LMCA tends to be asymptomatic and its finding is often incidental. To compensate for the deficiency it may cause, the heart can supply this area through the overdevelopment of the RCA, causing dominancy found in four articles [13,15,18,23], the super dominance of RCA, found in seven articles [20,28,31,34,36,40,43,47], and/or the aberrant origin of LAD or LCx from the RCA found in four articles [11,15,28,44]. These anatomical changes may ensure the correct blood supply to the myocardium. However, one study highlights the relationship between the congenital absence of the LMCA and H-RCA [11]. In both cases, the symptoms manifest when the heart is overloaded and the blood supply is insufficient, ranging from ischemia to myocardial infarction, ventricular fibrillation, or even death [33,40,48]. The congenital absence of the LMCA can also be related to the congenital absence of LAD, a correlation that can also cause ischemia-like symptoms during exertion [15].
The hypoplasia of the LMCA presented fewer incidences, being studied in only four studies with four subjects [14,17,25,35]. Hypoplastic left coronary artery (H-LMCA) refers to the underdevelopment of the LMCA, causing an insufficient blood supply to the heart that can or cannot be compensated by the right coronary system or the aberrant origin of the LCx or LAD. This condition may have symptoms like acute myocarditis, cardiomyopathy, myocardial ischemia, or cardiac failure. Thus, it becomes important to consider these variants when dealing with patients having cardiovascular complications [15].
The most common vessel with these anomalies is the circumflex artery (LCx), found in eleven studies with 62 subjects [18,20,21,23,28,31,34,36,41,47].
The congenital absence of LCx is often an incidental finding [31] and may even be benign [18], sometimes being discovered post-mortem [34]. The absence itself usually lacks major significance due to the compensatory blood supply provided by the overdevelopment of the RCA, LMCA, or LAD, which can adequately irrigate the affected area up to a certain extent. Its clinical importance lies in its association with other pathologies such as atherosclerosis [36], which can lead to ischemic-like symptoms during exertion [23,31], syncope, or even sudden death (Oliveira, 2015 [28]). Additionally, we found two studies featuring two subjects with situs inversus and a congenital absence of the LCx [41,43]. In one case, the patient was asymptomatic, and the absence was incidental [41], while in the other case, the patient experienced angina-like symptoms due to ischemia caused by the congenital absence of the LCx, along with significant stenosis on the LAD [43]. This situation compromises the anatomical compensation of the heart vessels in providing adequate blood supply.
Furthermore, LMCA branches such as LCx and LAD can also be hypoplastic. This anatomical variation was found in four studies with a total of five subjects [13,24,32,35]. The underdevelopment of these vessels may or may not be compensated by the right coronary system. When there is no compensation, the blood supply is insufficient during exertion, leading to symptoms such as dyspnea, palpitations, syncope [24], myocardial ischemia, or even sudden death [13]. A hypoplastic LCx artery may be due to a deficiency of NOS3 during intrauterine life according to Riede et al., 2013 [32].
One of the most common classifications is that of Yamanaka et al., which is characterized below. This classification is based on the location of the coronary artery ostium (right or left) and its direction, and its relationship with other vessels. In single-vessel coronary artery type I, the single artery has a normal course, and collateral vessels compensate for the absent coronary artery. In type II, the anomalous coronary artery arises near the opposite coronary artery, passes through the heart base, and its relation to large vessels may vary: anterior course in relation to pulmonary and aortic arteries (subtype A), between large vessels of the base (subtype B), posterior to the large vessels of the base (subtype P), and combinations of these (C). In type III, the proximal segment of the right coronary artery originates the anterior descending artery and the circumflex branch separately (refer to Figure 2 and Figure 3).
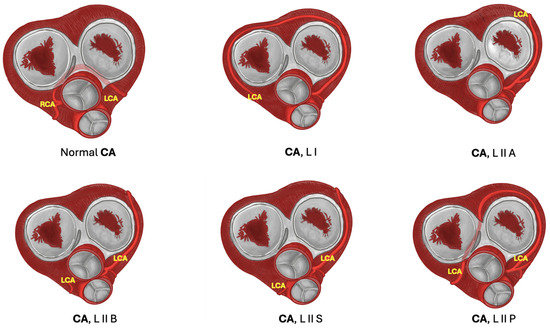
Figure 2.
Variants of left coronary artery. In the diagram, LCA variants are shown. Normal CA: Normal anatomical course of both CA. L I: Single LCA passes slightly superior to its normal course and extends its territory to compensate RCA absence. L II A: LCA passes superior to its normal course, laterally to the ascending aorta and pulmonary trunk, and surrounding left atrioventricular valve. L II B: LCA passes between the ascending aorta and pulmonary trunk. L II S: LCA crosses the pulmonary trunk to the right portion of the heart. L II P: LCA passes across the right atrioventricular valve in order to move to the right side of the heart. Abbreviations: RCA: right coronary artery, LCA left coronary artery.
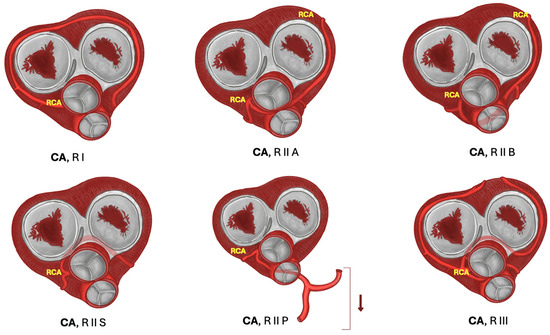
Figure 3.
Variants of right coronary artery. In the diagram, single right coronary artery variants are shown; RCA courses slightly superior to its normal course to compensate LCA absence. R I: Single RCA variant passes superior to the normal course, and extends its territory in order to compensate LCA absence. R II A: RCA passes between the pulmonary trunk and the ascending aorta. R II B: RCA courses anterior to the pulmonary trunk and ascending aorta. R II S: RCA passes behind the ascending aorta, in close relation to right and left atrioventricular valves. R II P: RCA courses behind the pulmonary trunk and descends to the inferior portion of the heart. R III: LAD and LCx are arising separately from RCA. Abbreviations: RCA: right coronary artery.
3.4. Prevalence
To calculate the prevalence of variant coronary arteries in the studies included in this review, four proportion forest plots were created. Three studies [11,39,44] were included for the prevalence of congenital absence or hypoplastic coronary artery, presenting a prevalence of 3% (CI from 2% to 8%). The heterogeneity for the included sample was 94% (Figure 4). However, the funnel plot did not apply to this sample due to the low number of studies included.
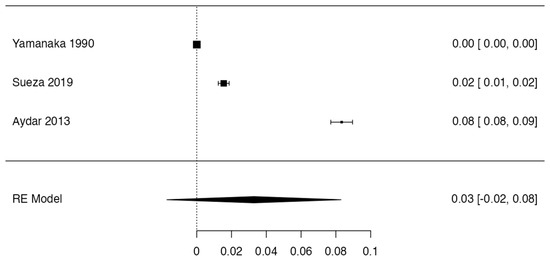
Figure 4.
Forest plot prevalence CA.
3.5. Risk of Bias of Included Articles
Three studies met the criteria for evaluation using the AQUA Checklist for Anatomical Studies tool, which analyzes bias in five domains. In all five domains provided by the AQUA table, the three included studies demonstrated a low risk of bias and were analyzed comprehensively (refer to Figure 5).
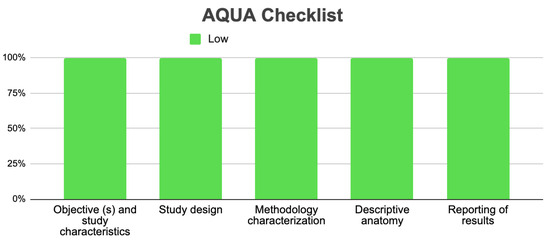
Figure 5.
Risk of bias included studies.
For the analysis of studies with case report methodology, the JBI tool was utilized to evaluate the risk of bias in this type of study. A total of 36 studies [10,12,38,40,41,42,43,45,46,47,48] were analyzed across the eight domains of this bias assessment tool (refer to Figure 6). The majority exhibited a low risk of bias. Specifically, eleven studies showed a high risk of bias in Domain 7, nine studies presented a high risk of bias in Domain 8, and ten studies demonstrated a high risk of bias in Domain 8.
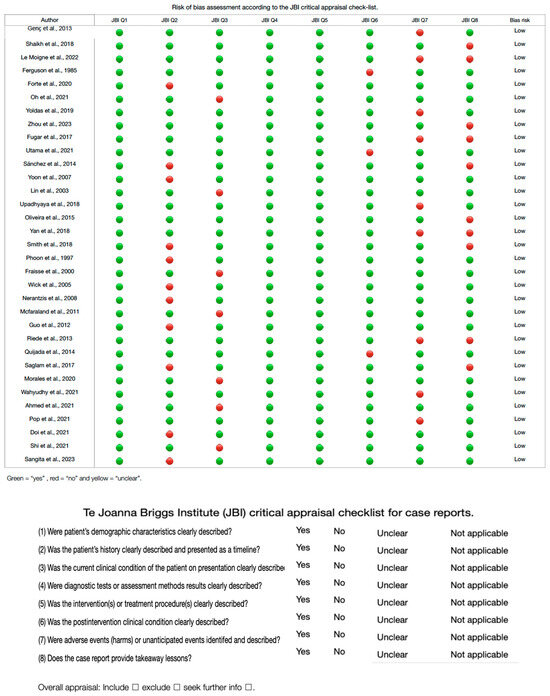
Figure 6.
Risk of bias study of case.
3.6. Clinical Considerations
For the reported clinical correlation, we have found some clinical presentations reported by the articles included in the review.
Most of the articles concluded that the congenital absence or hypoplasia of CA on its own lacks clinical relevance, being a relatively benign and asymptomatic finding [16,18,19,22,26,33,34,48] due to the overdevelopment of the other vessels [22]. However, it can be relevant when the absence/hypoplasia or super dominance of the other coronary arteries (or its branches) coexist with another pathology that exacerbates the insufficient blood supply to the myocardium, or when the lifestyle of the patient requires a high oxygen demand as an athlete [10,26,36]. Eight studies [10,12,17,22,27,36,43,45] reported that the coexistence of these variants and atherosclerotic disease can lead to an insufficient blood supply to the myocardium due to the restriction in the super-dominant vessel that replaces the irrigation, resulting in ischemia-like symptoms in exertion such as angina pectoris or even myocardial infarction with complete (STEMI) [12,27] or incomplete (NSTEMI) [10,17] vessel occlusion.
The most common symptoms that lead the patients to seek medical attention were described in nine studies [15,17,23,24,28,31,38,40,48] which included: ischemia-like symptoms [28,40,48], angina pectoris in exertion [15,17,23,31], syncope [24], dyspnea [38], palpitations [24], and bradycardia [38].
A chronic insufficient blood supply of the myocardium can lead to an ischemic disease, described in four studies [17,24,38,42], characterized by ventricular dysfunction or ventricular dilatation [24], unstable angina [38], acute myocardial infarction, and death [17,38,42].
Other clinical manifestations were less common, but worth mentioning due to their relevance in the prevention or treatment of the patient:
First, one study [10] has proposed the possible early and abnormal degeneration of the sinoatrial nodule or atrioventricular nodule due to the congenital absence of the RCA, which is normally responsible for the blood supply of these structures. This early degeneration can lead to a nodal conduction dysfunction, resulting in arrhythmias or ischemia [10].
A study [11] found that 36 of 46 patients have hypoplastic RCA related to the congenital absence of the LMCA, which can result in an increased risk for myocardial ischemia [11].
On the other hand, another study [10] said that the increased blood flow to the remaining CA, which supplies the missing vessel irrigation territory, can also increase its diameter, causing compression ischemia in nearby structures as well as the endothelial dysfunction and/or atherosclerosis of the CA [10].
Finally, it is critical to be aware of these anatomical variations (congenital absence or hypoplasia) as a patient with ischemia-like symptoms or cardiac failure may have them. Hence, it is important to consider the possible presence of these variants, and to perform a proper diagnosis and treatment [14]. In addition, even myocarditis and cardiomyopathy [14] can manifest when these variants are present, even leading to sudden death [13,28].
It is essential to emphasize that it is possible and common to find more than one coronary variant in the same patient; in fact, the articles that mention a unique variant are fewer [10,11,24]. Considering this, as these anatomical anomalies may mimic many cardiac diseases and CAD, it becomes critical to perform, as mentioned before, a correct and profound analysis of the exams and also to conduct proper tests that allow the medical team to detect these anomalies, such as selective coronary angiography (SCA), coronary angiogram, or computerized tomography coronary angiography (CTA), to avoid overlooking a coronary artery (CA) variant [12,13]. It is also recommended to corroborate the results with MDCT [12].
Many of the reviewed articles recommend treating HCAD by implanting an ICD to improve the quality of life. However, this may not be effective for all patients because its success depends on the severity of the blood supply alteration caused by the variants.
4. Discussion
In this systematic review and meta-analysis, coronary artery variants have been studied, primarily focusing on HCA as well as the congenital absence of the coronary artery and its branches. These variants, uncommon in the population, exhibit considerable variability in their description and regions of occurrence. The severity of this condition is contingent upon several factors, including the degree of narrowing in the HCA, the presence of single or multiple coronary artery variants, compromised areas, the presence of underlying chronic heart disease, and the lifestyle of the individual, regarding its requirement for high oxygen demand. These abnormalities may go unnoticed; therefore, their detection is mostly incidental during surgeries or imaging exams. Furthermore, once HCAD is diagnosed, it needs to be treated as soon as possible, as it can cause severe pathologies leading to death. Previous reviews have not found detailed analyses of these variants or studies that directly associate them with clinical considerations. This study is the first in this line of research and is innovative; it may be important to consider during clinical surgical management.
There is an evident prevalence of studies conducted in Asia and Europe, rather than in the Americas and Oceania. However, among the 140,137 subjects included in the study, 126,602 (90.34%) are from North America, 6019 (4.29%) from Asia, and 7514 (2.30%) from Europe, with only one subject each from South America and Oceania (0.0007%).
Regarding subjects presenting coronary artery abnormalities, there is a clear ethnic prevalence. Out of the 811 subjects with coronary artery variants, the majority (639; 78.79%) are from Europe, followed by Asia with 159 (19.60%), and a minority from North America with 11 (1.35%). On the other hand, South America and Oceania each have one subject (0.12%) with a coronary abnormality [49].
Additionally, sex distribution was examined. Among the subjects, 35,049 were identified as female and 99,135 as male, accounting for 25.01% female and 70.74% male subjects, respectively. However, sex was not specified in 93 articles, encompassing 5953 subjects (4.27%). Therefore, there is a prevalence ratio of 2.8 to 1 between males and females included in the study. Nonetheless, insufficient information about the sex of the patients precludes determining the prevalence of these variants between genders.
Regarding the prevalence of this variant, only three studies met the criteria for random sample analysis, so the prevalence reported may not reflect the true prevalence. It is also important to note that this type of AC variant is most commonly identified symptomatically in patients at various life stages or during surgical procedures on adjacent structures. Despite the majority of the included studies being case studies, the risk of bias was low, indicating methodological rigor.
Understanding these anatomical variations in the coronary arteries is crucial in clinical practice, particularly for the differential diagnosis of cardiovascular diseases and understanding the implications of results and repercussions of procedures and surgeries. The objective is to identify these anomalies to prevent complications and ensure successful recovery or an improved quality of life [50].
Concerning the symptoms, most studies showed that the anatomical anomaly tends to be asymptomatic when there are no other pathologies. This means that it is often an incidental and benign finding in patients with healthy lifestyles. However, it can be symptomatic by itself if the blood supply is insufficient to the heart or the nodules, causing ischemia or arrhythmias.
The real clinical value of knowing if a patient has hypoplasia or a congenital absence of the coronary arteries lies in the coexistence with other diseases, such as atherosclerosis, hypertension, diabetes, metabolic syndrome, or others that are less frequent, like acute cardiac failure or ventricular hypertrophy. This can lead to ischemia-like symptoms, angina pectoris, dyspnea, an increased risk of myocardial infarction, or even sudden death, among other complications. Most of the mentioned complications can be preventable with surgical procedures, lifestyle changes, or through treating the base pathology.
It is also relevant to be aware of the super-dominant vessel and the preventable repercussions of not treating it, as it can increase in diameter and cause the compression of nearby structures, leading to endothelial dysfunction or ischemia in previously healthy tissue.
Finally, it is important to always think of the slight chance of a congenital absence or hypoplasia of the coronary artery when dealing with patients with cardiac failure, myocarditis, or cardiomyopathy, as these conditions are differential diagnoses to a coronary artery variation and must be discarded to treat the patient and their condition in the best way possible, ensuring a correct diagnosis and therefore the corresponding treatment.
5. Limitations
This review was limited by the publication and authorship bias of the included studies. First, studies with different results that were in the non-indexed literature in the selected databases may have been excluded. Second, there could be limitations in the sensitivity and specificity of the searches. Finally, the authors personally selected the articles. All of this increases the probability of excluding potential cases from countries outside of Asia and North America that are not being reported in the scientific community.
6. Conclusions
In this systematic review, we have studied some congenital anomalies that affect CA, which have a low prevalence and are most often asymptomatic. The congenital absence of LMCA plus hypoplastic RCA are associated with an increased risk of ischemia, while myocarditis and cardiomyopathy are more likely to manifest in the presence of congenital coronary arteries and are associated with an increased risk of sudden death. It is important that cardiovascular doctors and surgeons recognize the variants of this anomaly for the adequate management of asymptomatic patients to be diagnosed early to have less probability of future complications. Finally, we believe that new studies could better study the relationship between these conditions and different cardiovascular pathologies.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/jcm13113085/s1, Complementary Table S1: Search details.
Author Contributions
Conceptualization M.O.-D., A.B.-M., J.d.V.-V. and J.J.V.-F.; methodology, C.A.-A., A.S.-S. and P.N.-B.; software, J.J.V.-F.; validation, J.J.V.-F., J.S.-G. and M.O.-D.; formal analysis, W.S.-L.; investigation, J.J.V.-F., C.R. and J.d.V.-V.; resources, J.J.V.-F.; data curation, W.S.-L. and A.B.-M. and C.R; writing—original draft preparation, W.S.-L.; writing—review and editing, J.J.V.-F.; visualization, C.A.-A., A.B.-F. and A.S.-S.; supervision, A.S.-S.; project administration J.J.V.-F. and A.B.-F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy.
Acknowledgments
We thank “Universidad de Playa Ancha, Plan de Fortalecimiento Universidades Estatales–Ministerio de Educación, Convenio UPA 1999” for helping us with the payment of publishing under Open Access.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
EKG/ECG: Electrocardiogram; PVCs: Premature Ventricular Contractions; SCA: Selective Coronary Angiography; IHC: Ischemic Heart Disease; H-RCA: Hypoplastic Right Coronary Artery; MRI: Magnetic Resonance Imaging; MDCT: Multidetector Computerized Tomography; CTA: Computerized Tomography Coronary Angiography; SA: Sinoatrial Node; AV: Atrioventricular Node; CAD: Coronary Artery Disease; HCAD: Hypoplastic Coronary Artery Disease, including hypoplasia and congenital absence; HCA: Hypoplastic Coronary Artery; CA: Coronary Artery; RCA: Right Coronary Artery; LMCA: Left Main Coronary Artery; LCx: Left Circumflex Artery; LAD: Left Anterior Descending Artery; H-RCA: Hypoplastic Right Coronary Artery; H-LMCA: Hypoplastic Left Main Coronary Artery; ICD: Implantable Cardioverter-Defibrillator.
References
- Loukas, M.; Sharma, A.; Blaak, C.; Sorenson, E.; Mian, A. The clinical anatomy of the coronary arteries. J. Cardiovasc. Transl. Res. 2013, 6, 197–207. [Google Scholar] [CrossRef] [PubMed]
- Altin, C.; Kanyilmaz, S.; Koc, S.; Gursoy, Y.C.; Bal, U.; Aydinalp, A.; Yildirir, A.; Muderrisoglu, H. Coronary anatomy, anatomic variations and anomalies: A retrospective coronary angiography study. Singap. Med. J. 2015, 56, 339–345. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sharma, B.; Chang, A.; Red-Horse, K. Coronary Artery Development: Progenitor Cells and Differentiation Pathways. Annu. Rev. Physiol. 2017, 79, 1–19. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Michalowska, A.M.; Tyczynski, P.; Pregowski, J.; Skowronski, J.; Mintz, G.S.; Kepka, C.; Kruk, M.; Witkowski, A.; Michalowska, I. Prevalence and Anatomic Characteristics of Single Coronary Artery Diagnosed by Computed Tomography Angiography. Am. J. Cardiol. 2019, 124, 939–946. [Google Scholar] [CrossRef] [PubMed]
- Lipton, M.J.; Barry, W.H.; Obrez, I.; Silverman, J.F.; Wexler, L. Isolated single coronary artery: Diagnosis, angiographic classification, and clinical significance. Radiology 1979, 130, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Shirani, J.; Roberts, W.C. Solitary coronary ostium in the aorta in the absence of other major congenital cardiovascular anomalies. J. Am. Coll. Cardiol. 1993, 21, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Mazine, A.; Fernandes, I.M.; Haller, C.; Hickey, E.J. Anomalous origins of the coronary arteries: Current knowledge and future perspectives. Curr. Opin. Cardiol. 2019, 34, 543–551. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Henry, B.M.; Tomaszewski, K.A.; Walocha, J.A. Methods of Evidence-Based Anatomy: A guide to conducting systematic reviews and meta-analysis of anatomical studies. Ann. Anat. 2016, 205, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Assaf, A.; Mantha, Y.; Small, D.; Zughaib, M. A Rare Anatomical Variant: Congenital Absence of the Right Coronary Artery with Left Circumflex Artery Supplying the Right Coronary Artery (RCA) Territory. Am. J. Case Rep. 2021, 22, e932248. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Aydar, Y.; Yazici, H.U.; Birdane, A.; Ulus, T.; Nadir, A.; Nasifov, M.; Göktekin, O.; Gorenek, B.; Unalir, A. Relationship between hypoplastic right coronary artery and coronary artery anomalies. Eur. Rev. Med. Pharmacol. Sci. 2013, 17, 694–700. [Google Scholar] [PubMed]
- Chen, Z.; Yan, J.; Han, X.; Adhikari, B.K.; Zhang, J.; Zhang, Y.; Sun, J.; Wang, Y. Congenital absence of the right coronary artery with acute myocardial infarction: Report of two cases and review of the literature. J. Int. Med. Res. 2020, 48, 300060520971508. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- De Giorgio, F.; Abbate, A.; Stigliano, E.; Capelli, A.; Arena, V. Hypoplastic coronary artery disease causing sudden death. Report of two cases and review of the literature. Cardiovasc. Pathol. 2010, 19, e107-11. [Google Scholar] [CrossRef] [PubMed]
- Doi, Y.; Waki, K.; Ogino, K.; Hayashi, T. Hypoplastic coronary artery disease and hypertension in a child: A case report. Eur. Heart J. Case Rep. 2021, 6, ytab526. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ferguson, D.W.; Henkle, J.Q.; Haws, C.W. Absence of left anterior descending coronary artery associated with anomalous origin of left circumflex coronary artery from the right coronary artery: A case report and review. Catheter. Cardiovasc. Diagn. 1985, 11, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Forte, E.; Punzo, B.; Agrusta, M.; Salvatore, M.; Spidalieri, G.; Cavaliere, C. A case report of right coronary artery agenesis diagnosed by computed tomography coronary angiography. Medicine 2020, 99, e19176. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fraisse, A.; Quilici, J.; Canavy, I.; Savin, B.; Aubert, F.; Bory, M. Images in cardiovascular medicine. Myocardial infarction in children with hypoplastic coronary arteries. Circulation 2000, 101, 1219–1222. [Google Scholar] [CrossRef] [PubMed]
- Fugar, S.; Issac, L.; Okoh, A.K.; Chedrawy, C.; Hangouche, N.E.; Yadav, N. Congenital Absence of Left Circumflex Artery: A Case Report and Review of the Literature. Case Rep. Cardiol. 2017, 2017, 6579847. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Genç, B.; Solak, A.; Doksöz, O.; Tavlı, V. A patient with ischemic symptoms presents with left coronary artery-to-right ventricle fistula and agenesis of the right coronary artery. Turk Kardiyol Dern Ars. 2013, 41, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Xu, M. Congenital absence of the left circumflex artery associated with inferior myocardial infarction. Intern. Med. 2012, 51, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Jariwala, P.; Jadhav, K.; Kale, S.S. Congenital absence of the left circumflex artery: Case series and review. Asian Cardiovasc Thorac. Ann. 2021, 29, 826–835. [Google Scholar] [CrossRef] [PubMed]
- Le Moigne, F.; Genicon, C. Right Coronary Artery Agenesis with Superdominant Left Circumflex Artery Diagnosed by CT Angiography. Turk Kardiyol. Dern. Ars. 2022, 50, 395–396. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.C.; Lee, W.S.; Kong, C.W.; Chan, W.L. Congenital absence of the left circumflex coronary artery. Jpn. Heart J. 2003, 44, 1015–1020. [Google Scholar] [CrossRef] [PubMed]
- McFarland, C.; Swamy, R.S.; Shah, A. Hypoplastic coronary artery disease: A rare cause of sudden cardiac death and its treatment with an implantable defibrillator. J. Cardiol. Cases 2011, 4, e148–e151. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Morales, R.; Bokowski, J.; Aljemmali, S.; Murphy, J.; Bharati, S.; Abdulla, R.I. A Rare Report of Hypoplastic Coronary Arteries and Pulmonary Veins: A Case Report and Review of the Literature. Pediatr. Cardiol. 2020, 41, 1231–1237. [Google Scholar] [CrossRef] [PubMed]
- Nerantzis, C.E.; Gavrielatos, G. Absence of right coronary artery with separate origin of a dominant left circumflex and left anterior descending branches: A rare postmortem angiographic finding. Clin. Anat. 2008, 21, 777–778. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.; Kim, J.H.; Kim, M.C.; Hong, Y.J.; Ahn, Y.; Jeong, M.H. Posterior myocardial infarction caused by superdominant circumflex occlusion over an absent right coronary artery: Case report and review of literature. Medicine 2021, 100, e26604. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Oliveira, M.D.; de Fazzio, F.R.; Mariani Junior, J.; Campos, C.M.; Kajita, L.J.; Ribeiro, E.E.; Lemos, P.A. Superdominant Right Coronary Artery with Absence of Left Circumflex and Anomalous Origin of the Left Anterior Descending Coronary from the Right Sinus: An Unheard Coronary Anomaly Circulation. Case Rep. Cardiol. 2015, 2015, 721536. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Phoon, C.K.; Van Son, J.; Moore, P.A.; Brook, M.M.; Haas, G.S.; Higgins, C.B. Aberrant left coronary artery arising from the right sinus of Valsalva with a right coronary arteriovenous malformation. Pediatr. Cardiol. 1997, 18, 385–388. [Google Scholar] [CrossRef] [PubMed]
- Pop, M.; Pal, K.; Vaga, D. Absence of Both Right and Left Main Coronary in a COVID Survivor. Diagnostics 2021, 11, 1199. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Quijada-Fumero, A.; Pimienta-González, R.; Rodriguez-Esteban, M. Absence of left circumflex with superdominant right coronary artery. BMJ Case Rep. 2014, 2014, bcr2014206782. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Riede, F.N.; Bulla, S.; Grundmann, S.; Werner, M.; Riede, U.N.; Otto, C. Isolated hypoplastic circumflex coronary artery: A rare cause of haemorrhagic myocardial infarction in a young athlete. Diagn. Pathol. 2013, 8, 91. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Saglam, M.; Dogan, D.; Sahin, S.; Turkkan, C.; Kula, O. Single right coronary artery with absence of the left main coronary artery, left anterior descending artery, and circumflex artery. Echocardiography 2017, 34, 1401–1403. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Zuriaga, D.; Martínez-Soriano, F. Absence of circumflex artery with superdominant right coronary: A classic anatomical dissection study. Surg Radiol Anat. 2015, 37, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Sangita, M.; Yadav, J.; Chaurasia, J.K.; Arora, A.; Jahan, A.; Patnaik, M. Hypoplastic coronary artery disease, as a cause of sudden death. Autops. Case Rep. 2023, 13, e2023440. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Shaikh, S.S.A.; Deshmukh, V.; Patil, V.; Khan, Z.; Singla, R.; Bansal, N.O. Congenital Absence of the Left Circumflex Artery With Super-Dominant Right Coronary Artery: Extremely Rare Coronary Anomaly. Cardiol Res. 2018, 9, 264–267. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Shi, X.; Liu, J.; Wu, J.; Hua, Y.; Zhou, K.; Li, Y. Hypoplastic coronary arteries in a child with a mutation in Notch1: A case report. Medicine 2020, 99, e21355. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Smith, J.C. Hypoplasia of the right and thrombosis of the left coronary artery with rupture of the left ventricle: A case report. Am. Heart J. 1952, 43, 796–799. [Google Scholar] [CrossRef] [PubMed]
- Sueda, S.; Kohno, H. Clinical characteristics in patients with rest angina and hypoplastic right coronary artery. Heart Vessel. 2020, 35, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Upadhyaya, S.G.N.; Mughal, L.H.; Connolly, D.; Lip, G. Single right coronary artery with congenital absence of left coronary system. BMJ Case Rep. 2018, 11, e228296. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Utama, H.W.; Widyoningroem, A. Situs inversus with congenital absence of left circumflex artery and a superdominant left-sided right coronary artery: A case report. Radiol. Case Rep. 2021, 17, 735–739, Erratum in Radiol. Case Rep. 2022, 17, 1034–1036. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wick, R.; Gilbert, J.D.; Byard, R.W. Café coronary syndrome-fatal choking on food: An autopsy approach. J. Clin. Forensic Med. 2006, 13, 135–138. [Google Scholar] [CrossRef] [PubMed]
- Widy, A.; Shalmont, G.; Situmorang, G.R.; Wahyudi, I.; Tanurahardja, B.; Rodjani, A. Abnormal dartos fascia in buried penis and hypospadias: Evidence from histopathology. J. Pediatr. Urol. 2018, 14, 536.e1–536.e7. [Google Scholar] [CrossRef] [PubMed]
- Yamanaka, O.; Hobbs, R.E. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Catheter. Cardiovasc. Diagn. 1990, 21, 28–40. [Google Scholar] [CrossRef] [PubMed]
- Yan, G.W.; Bhetuwal, A.; Yang, G.Q.; Fu, Q.S.; Hu, N.; Zhao, L.W.; Chen, H.; Fan, X.P.; Yan, J.; Zeng, H.; et al. Congenital absence of the right coronary artery: A case report and literature review. Medicine 2018, 97, e0187. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yoldaş, T.; Beyazal, M.; Örün, U.A. Single right coronary artery with right ventricular fistula and congenital absence of left coronary artery: An extremely rare combination. Cardiol. Young 2019, 29, 1402–1403. [Google Scholar] [CrossRef] [PubMed]
- Yoon, Y.K.; Rha, S.W.; Na, J.O.; Suh, S.Y.; Choi, C.U.; Kim, J.W.; Kim, E.J.; Park, C.G.; Seo, H.S.; Oh, D.J. Congenital absence of left circumflex coronary artery presented with vasospastic angina and myocardial bridge in single left coronary artery. Int. J. Cardiol. 2009, 131, e108-11. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.P.; Wang, L.L.; Qiu, Y.G.; Huang, S.W. R-I subtype single right coronary artery with congenital absence of left coronary system: A case report. World J. Cardiol. 2023, 15, 649–654. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Angelini, P. Arterias coronarias normales y anómalas: Definiciones y clasificación. Rev. Am. Corazón 1989, 117, 418–434. [Google Scholar] [CrossRef]
- Marchesi, A.; Tarissi de Jacobis, I.; Rigante, D.; Rimini, A.; Malorni, W.; Corsello, G.; Bossi, G.; Buonuomo, S.; Cardinale, F.; Cortis, E.; et al. Kawasaki disease: Guidelines of the Italian Society of Pediatrics, part I-definition, epidemiology, etiopathogenesis, clinical expression and management of the acute phase. Ital. J. Pediatr. 2018, 44, 102. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).