
Association of Psoas: Lumbar Vertebral Index (PLVI) with Postherpetic Neuralgia in Patients Aged 60 and Older with Herpes Zoster

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Definition of PHN
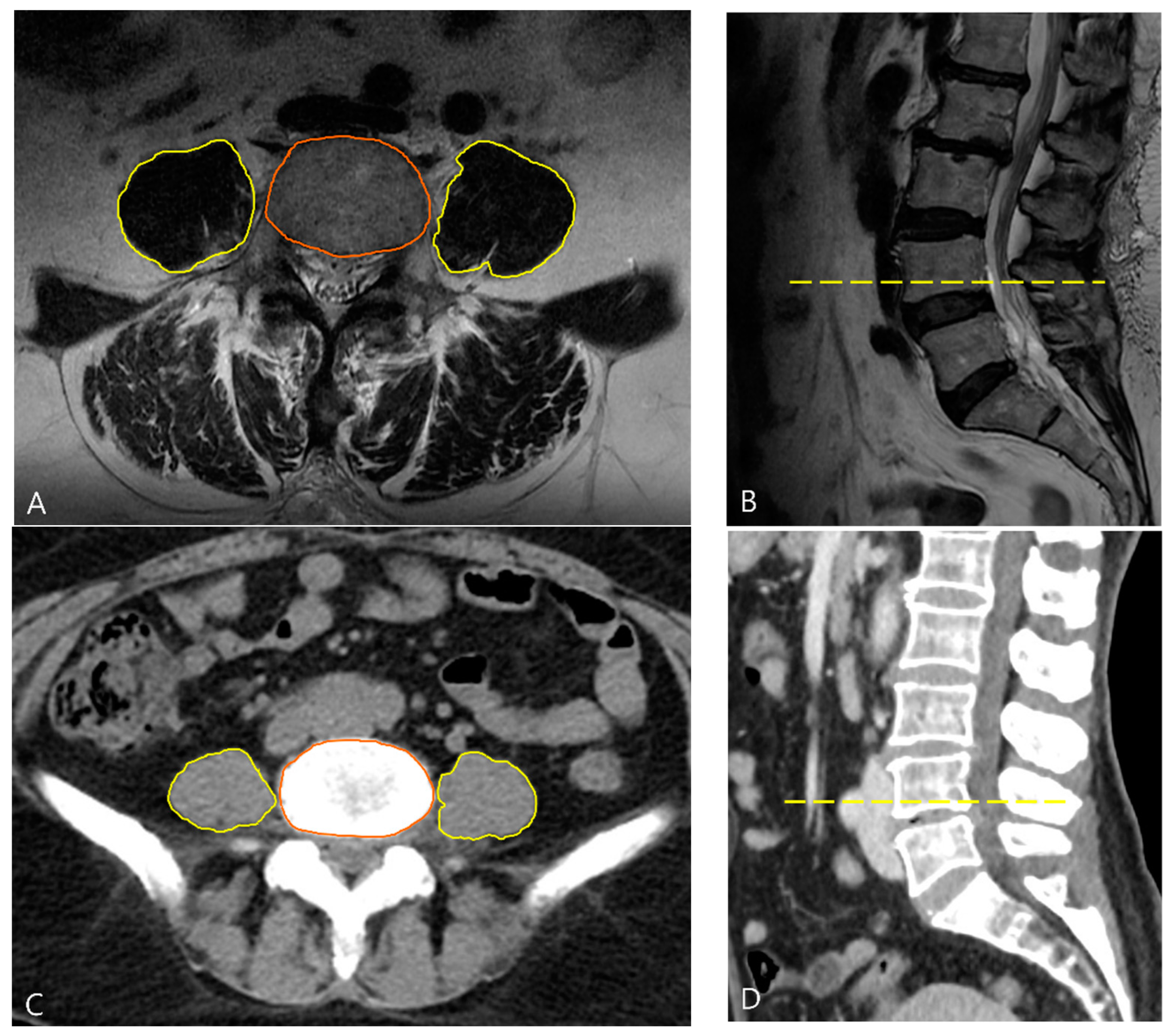
2.3. Measurement of Psoas: Lumbar Vertebral Index (PLVI)
2.4. Assessment of Frailty
2.5. Outcome Measures
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Drolet, M.; Brisson, M.; Schmader, K.; Levin, M.; Johnson, R.; Oxman, M.; Patrick, D.; Camden, S.; Mansi, J.A. Predictors of postherpetic neuralgia among patients with herpes zoster: A prospective study. J. Pain 2010, 11, 1211–1221. [Google Scholar] [CrossRef] [PubMed]
- Bouhassira, D.; Chassany, O.; Gaillat, J.; Hanslik, T.; Launay, O.; Mann, C.; Rabaud, C.; Rogeaux, O.; Strady, C. Patient perspective on herpes zoster and its complications: An observational prospective study in patients aged over 50 years in general practice. Pain 2012, 153, 342–349. [Google Scholar] [CrossRef]
- Kawai, K.; Rampakakis, E.; Tsai, T.F.; Cheong, H.J.; Dhitavat, J.; Covarrubias, A.O.; Yang, L.; Cashat-Cruz, M.; Monsanto, H.; Johnson, K.; et al. Predictors of postherpetic neuralgia in patients with herpes zoster: A pooled analysis of prospective cohort studies from North and Latin America and Asia. Int. J. Infect. Dis. 2015, 34, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Chae, J.S.; Im, J.; Choi, Y.J.; Lee, H.J.; Kim, W.J. Comparison of the Severity of Zoster-Associated Pain and Incidence of Postherpetic Neuralgia in Patients with and without Pre-Existing Spinal Disorders at the Same Spinal Nerve Level: A Retrospective Multicenter Study. J. Pers. Med. 2023, 13, 1286. [Google Scholar] [CrossRef] [PubMed]
- Oxman, M.N.; Levin, M.J.; Johnson, G.R.; Schmader, K.E.; Straus, S.E.; Gelb, L.D.; Arbeit, R.D.; Simberkoff, M.S.; Gershon, A.A.; Davis, L.E.; et al. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N. Engl. J. Med. 2005, 352, 2271–2284. [Google Scholar] [CrossRef] [PubMed]
- Opstelten, W.; Zuithoff, N.P.A.; van Essen, G.A.; van Loon, A.M.; van Wijck, A.J.M.; Kalkman, C.J.; Verheij, T.J.M.; Moons, K.G.M. Predicting postherpetic neuralgia in elderly primary care patients with herpes zoster: Prospective prognostic study. Pain 2007, 132 (Suppl. 1), S52–S59. [Google Scholar] [CrossRef]
- Whitley, R.; Weiss, H.L.; Soong, S.J.; Gnann, J.W. Herpes zoster: Risk categories for persistent pain. J. Infect. Dis. 1999, 179, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Varghese, L.; Standaert, B.; Olivieri, A.; Curran, D. The temporal impact of aging on the burden of herpes zoster. BMC Geriatr. 2017, 17, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Wilson, D.; Jackson, T.; Sapey, E.; Lord, J.M. Frailty and sarcopenia: The potential role of an aged immune system. Ageing Res. Rev. 2017, 36, 1–10. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Baylis, D.; Bartlett, D.B.; Syddall, H.E.; Ntani, G.; Gale, C.R.; Cooper, C.; Lord, J.M.; Sayer, A.A. Immune-endocrine biomarkers as predictors of frailty and mortality: A 10-year longitudinal study in community-dwelling older people. Age 2013, 35, 963–971. [Google Scholar] [CrossRef] [PubMed]
- Caruso, C.; Buffa, S.; Candore, G.; Colonna-Romano, G.; Dunn-Walters, D.; Kipling, D.; Pawelec, G. Mechanisms of immunosenescence. Immun. Ageing 2009, 6, 1–4. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 22 April 2023).
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.Y.; Woo, J.H.; Yoon, I.Y.; Lee, H.J.; Ahn, S.M.; Chae, J.S.; Kim, Y.J. Predictability of Radiologically Measured Psoas Muscle Area for Intraoperative Hypotension in Older Adult Patients Undergoing Femur Fracture Surgery. J. Clin. Med. 2023, 12, 1691. [Google Scholar] [CrossRef] [PubMed]
- Sim, J.H.; Lee, S.H.; Kim, J.W.; Koh, W.U.; Kim, H.T.; Ro, Y.J.; Kim, H.J. Low psoas lumbar vertebral index is associated with mortality after hip fracture surgery in elderly patients: A retrospective analysis. J. Pers. Med. 2021, 11, 673. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.; Iqbal, S.; Rafatzand, K.; Scheede-Bergdahl, C. Psoas muscle measurement as a marker of sarcopenia predicts risk of Grade 4 or 5 baseline chronic kidney disease and its progression. JCSM Rapid Commun. 2022, 5, 182–193. [Google Scholar] [CrossRef]
- Ebbeling, L.; Grabo, D.J.; Shashaty, M.; Dua, R.; Sonnad, S.S.; Sims, C.A.; Pascual, J.L.; Schwab, C.W.; Holena, D.N. Psoas: Lumbar vertebra index: Central sarcopenia independently predicts morbidity in elderly trauma patients. Eur. J. Trauma Emerg. Surg. 2014, 40, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Xing, X.F.; Zhou, Z.F.; Zhang, F.J.; Yan, M. The effect of early use of supplemental therapy on preventing postherpetic neuralgia: A systematic review and meta-analysis. Pain Physician 2017, 20, 471–486. [Google Scholar] [PubMed]
- Okamura, H.; Kimura, N.; Tanno, K.; Mieno, M.; Matsumoto, H.; Yamaguchi, A.; Adachi, H. The impact of preoperative sarcopenia, defined based on psoas muscle area, on long-term outcomes of heart valve surgery. J. Thorac. Cardiovasc. Surg. 2019, 157, 1071–1079.e3. [Google Scholar] [CrossRef]
- Koizia, L.; Naik, M.; Peck, G.; Mikhail, G.W.; Sen, S.; Malik, I.S.; Ariff, B.; Fertleman, M.B. The utility of psoas muscle assessment in predicting frailty in patients undergoing transcatheter aortic valve replacement. Curr. Gerontol. Geriatr. Res. 2020, 2020, 5783107. [Google Scholar] [CrossRef]
- Okada, Y.; Kiguchi, T.; Okada, A.; Iizuka, R.; Iwami, T.; Ohtsuru, S. Predictive value of sarcopenic findings in the psoas muscle on CT imaging among patients with sepsis. Am. J. Emerg. Med. 2021, 47, 180–186. [Google Scholar] [CrossRef]
- Yawn, B.P.; Wollan, P.; St. Sauver, J. Comparing shingles incidence and complication rates from medical record review and administrative database estimates: How close are they? Am. J. Epidemiol. 2011, 174, 1054–1061. [Google Scholar] [CrossRef]
- Yang, Y.W.; Chen, Y.H.; Wang, K.H.; Wang, C.Y.; Lin, H.W. Risk of herpes zoster among patients with chronic obstructive pulmonary disease: A population-based study. CMAJ 2011, 183, E275–E280. [Google Scholar] [CrossRef]
- Coplan, P.M.; Schmader, K.; Nikas, A.; Chan, I.S.; Choo, P.; Levin, M.J.; Johnson, G.; Bauer, M.; Williams, H.M.; Kaplan, K.M.; et al. Development of a measure of the burden of pain due to herpes zoster and postherpetic neuralgia for prevention trials: Adaptation of the brief pain inventory. J. Pain 2004, 5, 344–356. [Google Scholar] [CrossRef]
- Xu, Z.Y.; Hao, X.Y.; Wu, D.; Song, Q.Y.; Wang, X.X. Prognostic value of 11-factor modified frailty index in postoperative adverse outcomes of elderly gastric cancer patients in China. World J. Gastrointest. Surg. 2023, 15, 1093–1103. [Google Scholar] [CrossRef]
- McQuoid, P. Switching from gabapentin to pregabalin. N. Z. Med. J. 2019, 132, 101–103. [Google Scholar]
- Chincholkar, M. Gabapentinoids: Pharmacokinetics, pharmacodynamics and considerations for clinical practice. Br. J. Pain 2020, 14, 104–114. [Google Scholar] [CrossRef]
- Heins, S.E.; Frey, K.P.; Alexander, G.C.; Castillo, R.C. Reducing high-dose opioid prescribing: State-level morphine equivalent daily dose policies, 2007–2017. Pain Med. 2020, 21, 308–316. [Google Scholar] [CrossRef]
- Chen, J.Y.; Lan, K.M.; Sheu, M.J.; Tseng, S.F.; Weng, S.F.; Hu, M.L. Peptic ulcer as a risk factor for postherpetic neuralgia in adult patients with herpes zoster. J. Med. Virol. 2015, 87, 222–229. [Google Scholar] [CrossRef]
- Payette, H.; Roubenoff, R.; Jacques, P.F.; Dinarello, C.A.; Wilson, P.W.; Abad, L.W.; Harris, T. Insulin-like growth factor-1 and interleukin 6 predict sarcopenia in very old community-living men and women: The Framingham Heart Study. J. Am. Geriatr. Soc. 2003, 51, 1237–1243. [Google Scholar] [CrossRef]
- Schaap, L.A.; Pluijm, S.M.; Deeg, D.J.; Visser, M. Inflammatory markers and loss of muscle mass (sarcopenia) and strength. Am. J. Med. 2006, 119, 526.e9–526.e17. [Google Scholar] [CrossRef]
- Murton, A.J.; Maddocks, M.; Stephens, F.B.; Marimuthu, K.; England, R.; Wilcock, A. Consequences of late-stage non–small-cell lung cancer cachexia on muscle metabolic processes. Clin. Lung Cancer 2017, 18, e1–e11. [Google Scholar] [CrossRef]
- Ebisui, C.; Tsujinaka, T.; Morimoto, T.; Kan, K.; Iijima, S.; Yano, M.; Kominami, E.; Tanaka, K.; Monden, M. Interleukin-6 induces proteolysis by activating intracellular proteases (cathepsins B and L, proteasome) in C2C12 myotubes. Clin. Sci. 1995, 89, 431–439. [Google Scholar] [CrossRef]
- Franckhauser, S.; Elias, I.; Rotter Sopasakis, V.; Ferré, T.; Nagaev, I.; Andersson, C.X.; Agudo, J.; Ruberte, J.; Bosch, F.; Smith, U. Overexpression of Il6 leads to hyperinsulinaemia, liver inflammation and reduced body weight in mice. Diabetologia 2008, 51, 1306–1316. [Google Scholar] [CrossRef]
- Zhu, S.M.; Liu, Y.M.; An, E.D.; Chen, Q.L. Influence of systemic immune and cytokine responses during the acute phase of zoster on the development of postherpetic neuralgia. J. Zhejiang Univ. Sci. B 2009, 10, 625–630. [Google Scholar] [CrossRef]
- Lin, D.; Zhong, C.; Jiang, Q.; Huang, A.; Liu, Y. Serum interleukin-6 levels are increased in post-herpetic neuralgia: A single-center retrospective study. An. Bras. Dermatol. 2023, 98, 202–207. [Google Scholar] [CrossRef]
- Shi, H.J.; Cui, Z.Q. Correlation of serum inflammatory cytokine and immunoglobulin content with post-herpetic neuralgia in patients with acute herpes zoster. J. Hainan Med. Univ. 2017, 23, 97–100. [Google Scholar]
- Wu, C.L.; Marsh, A.; Dworkin, R.H. The role of sympathetic nerve blocks in herpes zoster and postherpetic neuralgia. Pain 2000, 87, 121–129. [Google Scholar] [CrossRef]
- Chucair-Elliott, A.J.; Jinkins, J.; Carr, M.M.; Carr, D.J. IL-6 contributes to corneal nerve degeneration after herpes simplex virus type I infection. Am. J. Pathol. 2016, 186, 2665–2678. [Google Scholar] [CrossRef] [PubMed]
- Forstenpointner, J.; Rice, A.S.C.; Finnerup, N.B.; Baron, R. Up-date on clinical management of postherpetic neuralgia and mechanism-based treatment: New options in therapy. J. Infect. Dis. 2018, 218 (Suppl. 2), S120–S126. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non-PHN (n = 287) | PHN (n = 64) | p-Value | |
|---|---|---|---|
| Age, year | 72.06 ± 8.206 | 73.98 ± 8.638 | 0.094 a |
| Sex, female | 59.2% (170/287) | 67.2% (43/64) | 0.260 b |
| BMI, kg/m2 | 23.551 ± 3.156 | 22.740 ± 2.466 | 0.055 a |
| Hypertension | 35.2% (101/287) | 46.9% (30/64) | 0.088 b |
| DM | 12.9% (37/287) | 23.4% (15/64) | 0.035 b |
| CHF | 12.5% (36/287) | 23.4% (15/64) | 0.031 b |
| Cardiac intervention or angina | 8.7% (25/286) | 15.6% (10/64) | 0.107 b |
| MI | 8.7% (25/286) | 15.6% (10/64) | 0.107 b |
| TIA or CVA | 15.7% (45/287) | 25.0% (16/64) | 0.099 b |
| CVA with sequelae | 7.0% (20/286) | 17.5% (11/64) | 0.013 b |
| Dependent functional status | 4.9% (14/286) | 14.1% (9/64) | 0.012 b |
| Peripheral disease | 10.8% (31/287) | 18.8% (12/64) | 0.092 b |
| Pulmonary disease | 9.4% (27/286) | 20.3% (13/64) | 0.018 b |
| Impaired sensory | 10.5% (30/286) | 18.8% (12/64) | 0.086 b |
| Number of SNRBs | 2.86 (2.00) | 3.23 (3.00) | 0.021 c |
| Dermatome affected | 0.997 d | ||
| Facial | 34 (11.8%) | 8 (12.5%) | |
| Cervical | 62 (21.6%) | 13 (20.3%) | |
| Thoracic | 123 (42.9%) | 27 (42.2%) | |
| Lumbar | 58 (20.2%) | 14 (21.9%) | |
| Sacral | 10 (3.5%) | 2 (16.7%) | |
| NRS | 6.66 ± 1.626 | 7.50 ± 1.345 | <0.001 a |
| Pain duration | 20.30 ± 14.189 | 25.61 ± 18.268 | 0.011 a |
| MME | 17.719 ± 17.152 | 18.207 ± 16.583 | 0.836 a |
| Anticonvulsant | 195.96 ± 85.704 | 201.56 ± 90.325 | 0.640 a |
| No-PHN (n = 287) | PHN (n = 64) | p-Value | |
|---|---|---|---|
| PLVI | |||
| High PLVI | 58.9 (169/287) | 20.3 (13/64) | <0.001 |
| Low PLVI | 41.1 (118/287) | 79.7 (51/64) | |
| Frailty | |||
| Not-frail (mFI < 0.27) | 85.4% (245/287) | 51.6% (33/64) | <0.001 |
| Frail (mFI ≥ 0.27) | 14.6% (42/287) | 48.4% (31/64) |
| Variables | Unadjusted Analysis | Adjusted Analysis | ||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p-Value | Odds Ratio (95% CI) | p-Value | |
| Age (for 1 year increase) | 1.027 (0.995, 1.060) | 0.095 | ||
| Sex (female) | 1.409 (0.795, 2.498) | 0.240 | ||
| NRS | 1.409 (1.175, 1.690) | <0.001 | 1.300 (1.071, 1.579) | 0.008 |
| Number of SNRBs | 1.093 (0.961, 1.242) | 0.176 | ||
| Pain duration | 1.021 (1.005, 1.039) | 0.012 | ||
| Low PLVI | 5.619 (2.925, 10.793) | <0.001 | 3.265 (1.523, 7.001) | 0.002 |
| mFI variables (categorical) | 5.480 (3.039, 9.880) | <0.001 | 2.455 (1.211, 4.976) | 0.013 |
| HTN | 1.625 (0.940, 2.809) | 0.082 | ||
| DM | 2.068 (1.055, 4.057) | 0.034 | ||
| CHF | 2.134 (1.086, 4.195) | 0.028 | ||
| Cardiac intervention or angina | 1.941 (0.881, 4.275) | 0.100 | ||
| MI | 1.941 (0.881, 4.275) | 0.100 | ||
| TIA or CVA | 1.793 (0.937, 3.431) | 0.078 | ||
| CVA with sequelae | 2.824 (1.277, 6.244) | 0.010 | ||
| Dependent functional status | 3.191 (1.316, 7.740) | 0.010 | ||
| Peripheral disease | 1.906 (0.918, 3.955) | 0.083 | ||
| Pulmonary disease | 2.455 (1.187, 5.076) | 0.015 | ||
| Sensory impairment | 1.977 (0.950, 4.114) | 0.068 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
An, S.-M.; Chae, J.S.; Lee, H.J.; Cho, S.; Im, J. Association of Psoas: Lumbar Vertebral Index (PLVI) with Postherpetic Neuralgia in Patients Aged 60 and Older with Herpes Zoster. J. Clin. Med. 2024, 13, 3100. https://doi.org/10.3390/jcm13113100
An S-M, Chae JS, Lee HJ, Cho S, Im J. Association of Psoas: Lumbar Vertebral Index (PLVI) with Postherpetic Neuralgia in Patients Aged 60 and Older with Herpes Zoster. Journal of Clinical Medicine. 2024; 13(11):3100. https://doi.org/10.3390/jcm13113100
Chicago/Turabian StyleAn, Sang-Mee, Ji Seon Chae, Hyun Jung Lee, Sooyoung Cho, and Jiwoong Im. 2024. "Association of Psoas: Lumbar Vertebral Index (PLVI) with Postherpetic Neuralgia in Patients Aged 60 and Older with Herpes Zoster" Journal of Clinical Medicine 13, no. 11: 3100. https://doi.org/10.3390/jcm13113100