
Advances and Challenges in Minimally Invasive Spine Surgery



Abstract
1. Introduction
2. Developmental Milestones
3. Challenges to Adoption
4. Shifting the Paradigm
5. Educating the Future
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guiroy, A.; Sicoli, A.; Masanes, N.G.; Ciancio, A.M.; Gagliardi, M.; Falavigna, A. How to perform the Wiltse posterolateral spinal approach: Technical note. Surg. Neurol. Int. 2018, 9, 38. [Google Scholar] [CrossRef]
- Wiltse, L.L.; Bateman, J.G.; Hutchinson, R.H.; Nelson, W.E. The paraspinal sacrospinalis-splitting approach to the lumbar spine. J. Bone Jt. Surg. Am. 1968, 50, 919–926. [Google Scholar] [CrossRef]
- Park, J.W.; Nam, H.S.; Cho, S.K.; Jung, H.J.; Lee, B.J.; Park, Y. Kambin’s Triangle Approach of Lumbar Transforaminal Epidural Injection with Spinal Stenosis. Ann. Rehabil. Med. 2011, 35, 833–843. [Google Scholar] [CrossRef]
- Kambin, P.; Brager, M.D. Percutaneous posterolateral discectomy. Anatomy and mechanism. Clin. Orthop. Relat. Res. 1987, 223, 145–154. [Google Scholar] [CrossRef]
- Kambin, P.; Sampson, S. Posterolateral percutaneous suction-excision of herniated lumbar intervertebral discs. Report of interim results. Clin. Orthop. Relat. Res. 1986, 207, 37–43. [Google Scholar] [CrossRef]
- Wang, T.Y.; Mehta, V.A.; Gabr, M.; Sankey, E.W.; Bwensa, A.; Goodwin, C.R.; Karikari, I.O.; Chi, J.H.; Abd-El-Barr, M.M. Percutaneous Lumbar Interbody Fusion With an Expandable Titanium Cage Through Kambin’s Triangle: A Case Series With Initial Clinical and Radiographic Results. Int. J. Spine Surg. 2021, 15, 1133–1141. [Google Scholar] [CrossRef]
- Williams, R.W. Microlumbar discectomy: A conservative surgical approach to the virgin herniated lumbar disc. Spine 1978, 3, 175–182. [Google Scholar] [CrossRef]
- Foley, K.T.; Smith, M.M.; Rampersaud, Y.R. Microendoscopic approach to far-lateral lumbar disc herniation. Neurosurg. Focus 1999, 7, e5. [Google Scholar] [CrossRef]
- Fessler, R.G.; Khoo, L.T. Minimally invasive cervical microendoscopic foraminotomy: An initial clinical experience. Neurosurgery 2002, 51 (Suppl. 5), S37–S45. [Google Scholar] [CrossRef] [PubMed]
- Weiner, B.K.; Walker, M.; Brower, R.S.; McCulloch, J.A. Microdecompression for lumbar spinal canal stenosis. Spine 1999, 24, 2268–2272. [Google Scholar] [CrossRef] [PubMed]
- Haaker, R.G.; Senkal, M.; Kielich, T.; Kramer, J. Percutaneous lumbar discectomy in the treatment of lumbar discitis. Eur. Spine J. 1997, 6, 98–101. [Google Scholar] [CrossRef] [PubMed]
- Haji, F.A.; Cenic, A.; Crevier, L.; Murty, N.; Reddy, K. Minimally invasive approach for the resection of spinal neoplasm. Spine 2011, 36, E1018–E1026. [Google Scholar] [CrossRef] [PubMed]
- Holly, L.T.; Schwender, J.D.; Rouben, D.P.; Foley, K.T. Minimally invasive transforaminal lumbar interbody fusion: Indications, technique, and complications. Neurosurg. Focus 2006, 20, E6. [Google Scholar] [CrossRef] [PubMed]
- Forst, R.; Hausmann, B. Nucleoscopy—A new examination technique. Arch. Orthop. Trauma. Surg. 1983, 101, 219–221. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, A.; Suezawa, Y.; Leu, H. Does percutaneous nucleotomy with discoscopy replace conventional discectomy? Eight years of experience and results in treatment of herniated lumbar disc. Clin. Orthop. Relat. Res. 1989, 238, 35–42. [Google Scholar] [CrossRef]
- Schubert, M.; Hoogland, T. Endoscopic transforaminal nucleotomy with foraminoplasty for lumbar disk herniation. Oper. Orthop. Traumatol. 2005, 17, 641–661. [Google Scholar] [CrossRef] [PubMed]
- Jasper, G.P.; Francisco, G.M.; Telfeian, A.E. Clinical success of transforaminal endoscopic discectomy with foraminotomy: A retrospective evaluation. Clin. Neurol. Neurosurg. 2013, 115, 1961–1965. [Google Scholar] [CrossRef] [PubMed]
- Yeung, A.T.; Tsou, P.M. Posterolateral endoscopic excision for lumbar disc herniation: Surgical technique, outcome, and complications in 307 consecutive cases. Spine 2002, 27, 722–731. [Google Scholar] [CrossRef] [PubMed]
- Birjandian, Z.; Emerson, S.; Telfeian, A.E.; Hofstetter, C.P. Interlaminar endoscopic lateral recess decompression-surgical technique and early clinical results. J. Spine Surg. 2017, 3, 123–132. [Google Scholar] [CrossRef]
- Ruetten, S.; Komp, M.; Merk, H.; Godolias, G. Use of newly developed instruments and endoscopes: Full-endoscopic resection of lumbar disc herniations via the interlaminar and lateral transforaminal approach. J. Neurosurg. Spine 2007, 6, 521–530. [Google Scholar] [CrossRef]
- Perez, E.G.; Santander, X.A.; Llinas Amengual, P.; Choi, D.J. Biportal Endoscopic Spine Surgery: Clinical Results for 163 Patients. World Neurosurg. 2023, 180, e676–e685. [Google Scholar] [CrossRef] [PubMed]
- Gatam, A.R.; Gatam, L.; Phedy; Mahadhipta, H.; Luthfi, O.; Ajiantoro; Husin, S.; Aprilya, D. Full Endoscopic Posterior Cervical Foraminotomy in Management of Foraminal Disc Herniation and Foraminal Stenosis. Orthop. Res. Rev. 2022, 14, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ahn, Y. Anterior Endoscopic Cervical Discectomy: Surgical Technique and Literature Review. Neurospine 2023, 20, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Telfeian, A.E.; Wagner, R. Transforaminal endoscopic thoracic discectomy: Surgical technique. J. Spine Surg. 2023, 9, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Simpson, A.K.; Lightsey, H.M.t.; Xiong, G.X.; Crawford, A.M.; Minamide, A.; Schoenfeld, A.J. Spinal endoscopy: Evidence, techniques, global trends, and future projections. Spine J. 2022, 22, 64–74. [Google Scholar] [CrossRef] [PubMed]
- Ditzler, J.W.; Dumke, P.R.; Harrington, J.J.; Fox, J.D. Should spinal anesthesia be used in surgery for herniated intervertebral disk. Anesth. Analg. 1959, 38, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Jellish, W.S.; Thalji, Z.; Stevenson, K.; Shea, J. A prospective randomized study comparing short- and intermediate-term perioperative outcome variables after spinal or general anesthesia for lumbar disk and laminectomy surgery. Anesth. Analg. 1996, 83, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.Y.; Grossman, J. Endoscopic minimally invasive transforaminal interbody fusion without general anesthesia: Initial clinical experience with 1-year follow-up. Neurosurg. Focus 2016, 40, E13. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.W.W.; Michael, Y. The evolution of minimally invasive spine surgery. J. Neurosurg. 2019, 30, 149–158. [Google Scholar] [CrossRef]
- Kolcun, J.P.G.; Brusko, G.D.; Basil, G.W.; Epstein, R.; Wang, M.Y. Endoscopic transforaminal lumbar interbody fusion without general anesthesia: Operative and clinical outcomes in 100 consecutive patients with a minimum 1-year follow-up. Neurosurg. Focus 2019, 46, E14. [Google Scholar] [CrossRef]
- Shen, J. Fully Endoscopic Lumbar Laminectomy and Transforaminal Lumbar Interbody Fusion Under Local Anesthesia with Conscious Sedation: A Case Series. World Neurosurg. 2019, 127, e745–e750. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, J.L.; Hussain, I.; Sommer, F.; Hartl, R.; Elowitz, E. The Future of Minimally Invasive Spinal Surgery. World Neurosurg. 2022, 163, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Nolte, L.P.; Zamorano, L.J.; Jiang, Z.; Wang, Q.; Langlotz, F.; Berlemann, U. Image-guided insertion of transpedicular screws. A laboratory set-up. Spine 1995, 20, 497–500. [Google Scholar] [CrossRef] [PubMed]
- Hartl, R.; Lam, K.S.; Wang, J.; Korge, A.; Kandziora, F.; Audige, L. Worldwide survey on the use of navigation in spine surgery. World Neurosurg. 2013, 79, 162–172. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, J.L.; Hartl, R.; Elowitz, E. Challenges Hindering Widespread Adoption of Minimally Invasive Spinal Surgery. World Neurosurg. 2022, 163, 228–232. [Google Scholar] [CrossRef] [PubMed]
- Ozgur, B.M.; Aryan, H.E.; Pimenta, L.; Taylor, W.R. Extreme Lateral Interbody Fusion (XLIF): A novel surgical technique for anterior lumbar interbody fusion. Spine J. 2006, 6, 435–443. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.J.; Safaee, M.M.; Khan, N.R.; Brown, M.T.; Foley, K.T. Tubular microdiscectomy: Techniques, complication avoidance, and review of the literature. Neurosurg. Focus 2017, 43, E7. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, H.; Abbasi, A. Oblique Lateral Lumbar Interbody Fusion (OLLIF): Technical Notes and Early Results of a Single Surgeon Comparative Study. Cureus 2015, 7, e351. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Chaudhari, R.; Wu, C.; Mehbod, A.A.; Erkan, S.; Transfeldt, E.E. Biomechanical evaluation of an expandable meshed bag augmented with pedicle or facet screws for percutaneous lumbar interbody fusion. Spine J. 2010, 10, 987–993. [Google Scholar] [CrossRef]
- Tabarestani, T.Q.; Wang, T.Y.; Sykes, D.A.W.; Mehta, V.A.; Yang, L.Z.; Chow, S.C.; Shaffrey, C.I.; Wiggins, W.F.; Chi, J.H.; Abd-El-Barr, M.M. Two-Year Clinical and Radiographic Outcomes for Percutaneous Lumbar Interbody Fusion With an Expandable Titanium Cage Through Kambin’s Triangle Without Facetectomy. Int. J. Spine Surg. 2023, 17, 760–770. [Google Scholar] [CrossRef]
- Kolcun, J.P.G.; Brusko, G.D.; Wang, M.Y. Endoscopic transforaminal lumbar interbody fusion without general anesthesia: Technical innovations and outcomes. Ann. Transl. Med. 2019, 7 (Suppl. 5), S167. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, T.; Fujibayashi, S.; Otsuki, B.; Murata, K.; Matsuda, S. Indirect decompression with lateral interbody fusion for severe degenerative lumbar spinal stenosis: Minimum 1-year MRI follow-up. J. Neurosurg. Spine 2020, 33, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Hamanaka, H.; Tajima, T.; Kurogi, S.; Higa, K.; Nagai, T.; Kuroki, T.; Takamori, H.; Mukai, S.; Kamoto, T.; Chosa, E. Ureter position and risk of ureteral injury during lateral lumbar interbody fusion. J. Orthop. Sci. 2023, 29, 775–780. [Google Scholar] [CrossRef] [PubMed]
- Januszewski, J.; Vivas, A.C.; Uribe, J.S. Limitations and complications of minimally invasive spinal surgery in adult deformity. Ann. Transl. Med. 2018, 6, 109. [Google Scholar] [CrossRef] [PubMed]
- Dakwar, E.; Le, T.V.; Baaj, A.A.; Le, A.X.; Smith, W.D.; Akbarnia, B.A.; Uribe, J.S. Abdominal wall paresis as a complication of minimally invasive lateral transpsoas interbody fusion. Neurosurg. Focus 2011, 31, E18. [Google Scholar] [CrossRef] [PubMed]
- Beckman, J.M.; Vincent, B.; Park, M.S.; Billys, J.B.; Isaacs, R.E.; Pimenta, L.; Uribe, J.S. Contralateral psoas hematoma after minimally invasive, lateral retroperitoneal transpsoas lumbar interbody fusion: A multicenter review of 3950 lumbar levels. J. Neurosurg. Spine 2017, 26, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Cummock, M.D.; Vanni, S.; Levi, A.D.; Yu, Y.; Wang, M.Y. An analysis of postoperative thigh symptoms after minimally invasive transpsoas lumbar interbody fusion. J. Neurosurg. Spine 2011, 15, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Epstein, N.E. Incidence of Major Vascular Injuries with Extreme Lateral Interbody Fusion (XLIF). Surg. Neurol. Int. 2020, 11, 70. [Google Scholar] [CrossRef] [PubMed]
- Kueper, J.; Fantini, G.A.; Walker, B.R.; Aichmair, A.; Hughes, A.P. Incidence of vascular complications during lateral lumbar interbody fusion: An examination of the mini-open access technique. Eur. Spine J. 2015, 24, 800–809. [Google Scholar] [CrossRef]
- Elowitz, E.H.; Yanni, D.S.; Chwajol, M.; Starke, R.M.; Perin, N.I. Evaluation of indirect decompression of the lumbar spinal canal following minimally invasive lateral transpsoas interbody fusion: Radiographic and outcome analysis. Minim. Invasive Neurosurg. 2011, 54, 201–206. [Google Scholar] [CrossRef]
- Hiyama, A.; Sakai, D.; Katoh, H.; Sato, M.; Watanabe, M. Postoperative Radiological Improvement after Staged Surgery Using Lateral Lumbar Interbody Fusion for Preoperative Coronal Malalignment in Patients with Adult Spinal Deformity. J. Clin. Med. 2023, 12, 2389. [Google Scholar] [CrossRef] [PubMed]
- Marotta, N.; Cosar, M.; Pimenta, L.; Khoo, L.T. A novel minimally invasive presacral approach and instrumentation technique for anterior L5-S1 intervertebral discectomy and fusion: Technical description and case presentations. Neurosurg. Focus 2006, 20, E9. [Google Scholar] [CrossRef] [PubMed]
- Gundanna, M.I.; Miller, L.E.; Block, J.E. Complications with axial presacral lumbar interbody fusion: A 5-year postmarketing surveillance experience. SAS J. 2011, 5, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Lindley, E.M.; McCullough, M.A.; Burger, E.L.; Brown, C.W.; Patel, V.V. Complications of axial lumbar interbody fusion. J. Neurosurg. Spine 2011, 15, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Marchi, L.; Oliveira, L.; Coutinho, E.; Pimenta, L. Results and complications after 2-level axial lumbar interbody fusion with a minimum 2-year follow-up. J. Neurosurg. Spine 2012, 17, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Hofstetter, C.P.; Shin, B.; Tsiouris, A.J.; Elowitz, E.; Hartl, R. Radiographic and clinical outcome after 1- and 2-level transsacral axial interbody fusion: Clinical article. J. Neurosurg. Spine 2013, 19, 454–463. [Google Scholar] [CrossRef] [PubMed]
- Bardeesi, A.; Tabarestani, T.Q.; Bergin, S.M.; Huang, C.C.; Shaffrey, C.I.; Wiggins, W.F.; Abd-El-Barr, M.M. Using Augmented Reality Technology to Optimize Transfacet Lumbar Interbody Fusion: A Case Report. J. Clin. Med. 2024, 13, 1513. [Google Scholar] [CrossRef] [PubMed]
- Olexa, J.; Shear, B.; Han, N.; Sharma, A.; Trang, A.; Kim, K.; Schwartzbauer, G.; Ludwig, S.; Sansur, C. Feasibility of a novel augmented reality overlay for cervical screw placement in phantom spine models. Asian Spine J. 2024. [Google Scholar] [CrossRef] [PubMed]
- Urakov, T.M. Augmented Reality-assisted Pedicle Instrumentation: Versatility Across Major Instrumentation Sets. Spine 2020, 45, E1622–E1626. [Google Scholar] [CrossRef]
- Bui, T.; Ruiz-Cardozo, M.A.; Dave, H.S.; Barot, K.; Kann, M.R.; Joseph, K.; Lopez-Alviar, S.; Trevino, G.; Brehm, S.; Yahanda, A.T.; et al. Virtual, Augmented, and Mixed Reality Applications for Surgical Rehearsal, Operative Execution, and Patient Education in Spine Surgery: A Scoping Review. Medicina 2024, 60, 332. [Google Scholar] [CrossRef]
- Mummaneni, P.V.; Shaffrey, C.I.; Lenke, L.G.; Park, P.; Wang, M.Y.; La Marca, F.; Smith, J.S.; Mundis, G.M., Jr.; Okonkwo, D.O.; Moal, B.; et al. The minimally invasive spinal deformity surgery algorithm: A reproducible rational framework for decision making in minimally invasive spinal deformity surgery. Neurosurg. Focus 2014, 36, E6. [Google Scholar] [CrossRef] [PubMed]
- Mummaneni, P.V.; Park, P.; Shaffrey, C.I.; Wang, M.Y.; Uribe, J.S.; Fessler, R.G.; Chou, D.; Kanter, A.S.; Okonkwo, D.O.; Mundis, G.M.; et al. The MISDEF2 algorithm: An updated algorithm for patient selection in minimally invasive deformity surgery. J. Neurosurg. Spine 2019, 32, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Sandhu, F.V.; Marc, J. Decision Making for Minimally Invasive Spine Surgery, 1st ed.; Thieme Medical Publishers: New York, NY, USA, 2011. [Google Scholar]
- Fokter, S.K.; Yerby, S.A. Patient-based outcomes for the operative treatment of degenerative lumbar spinal stenosis. Eur. Spine J. 2006, 15, 1661–1669. [Google Scholar] [CrossRef]
- Lucio, J.C.; Vanconia, R.B.; Deluzio, K.J.; Lehmen, J.A.; Rodgers, J.A.; Rodgers, W. Economics of less invasive spinal surgery: An analysis of hospital cost differences between open and minimally invasive instrumented spinal fusion procedures during the perioperative period. Risk Manag. Healthc. Policy 2012, 5, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Chou, D.; Mundis, G.; Wang, M.; Fu, K.M.; Shaffrey, C.; Okonkwo, D.; Kanter, A.; Eastlack, R.; Nguyen, S.; Deviren, V.; et al. Minimally Invasive Surgery for Mild-to-Moderate Adult Spinal Deformities: Impact on Intensive Care Unit and Hospital Stay. World Neurosurg. 2019, 127, e649–e655. [Google Scholar] [CrossRef] [PubMed]
- Lewandrowski, K.U.; Soriano-Sanchez, J.A.; Zhang, X.; Ramirez Leon, J.F.; Soriano Solis, S.; Rugeles Ortiz, J.G.; Martinez, C.R.; Alonso Cuellar, G.O.; Liu, K.; Fu, Q.; et al. Surgeon motivation, and obstacles to the implementation of minimally invasive spinal surgery techniques. J. Spine Surg. 2020, 6 (Suppl. 1), S249–S259. [Google Scholar] [CrossRef]
- Smith, Z.A.; Fessler, R.G. Paradigm changes in spine surgery: Evolution of minimally invasive techniques. Nat. Rev. Neurol. 2012, 8, 443–450. [Google Scholar] [CrossRef]
- Minimally Invasive Spine Surgery Market Size, Share, Industry, Forecast and Outlook (2024–2031). Available online: https://www.datamintelligence.com/research-report/minimally-invasive-spine-surgery-market (accessed on 15 February 2024).
- Lewandrowski, K.U.; Soriano-Sanchez, J.A.; Zhang, X.; Ramirez Leon, J.F.; Soriano Solis, S.; Rugeles Ortiz, J.G.; Martinez, C.R.; Alonso Cuellar, G.O.; Liu, K.; Fu, Q.; et al. Regional variations in acceptance, and utilization of minimally invasive spinal surgery techniques among spine surgeons: Results of a global survey. J. Spine Surg. 2020, 6 (Suppl. 1), S260–S274. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.Y.; Chang, H.K.; Grossman, J. Reduced Acute Care Costs With the ERAS(R) Minimally Invasive Transforaminal Lumbar Interbody Fusion Compared With Conventional Minimally Invasive Transforaminal Lumbar Interbody Fusion. Neurosurgery 2018, 83, 827–834. [Google Scholar] [CrossRef]
- Basil, G.W.; Wang, M.Y. Trends in outpatient minimally invasive spine surgery. J. Spine Surg. 2019, 5 (Suppl. 1), S108–S114. [Google Scholar] [CrossRef]
- Bass, B.L. Presidential Address: The Joy and Privilege of a Surgical Career. Available online: https://www.facs.org/for-medical-professionals/news-publications/news-and-articles/bulletin/2017/12/presidential-address-the-joy-and-privilege-of-a-surgical-career/ (accessed on 15 February 2024).
- Schmidt, F.A.; Wong, T.; Kirnaz, S.; Taboada, N.; Assaker, R.; Hofstetter, C.; Kim, J.S.; Parajon, A.; Taylor, P.; Assous, M.; et al. Development of a Curriculum for Minimally Invasive Spine Surgery (MISS). Glob. Spine J. 2020, 10, 122S–125S. [Google Scholar] [CrossRef] [PubMed]
- Sclafani, J.A.; Kim, C.W. Complications associated with the initial learning curve of minimally invasive spine surgery: A systematic review. Clin. Orthop. Relat. Res. 2014, 472, 1711–1717. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.K.; Kshettry, V.R.; Recinos, P.F.; Kamian, K.; Schlenk, R.P.; Benzel, E.C. Establishing a surgical skills laboratory and dissection curriculum for neurosurgical residency training. J. Neurosurg. 2015, 123, 1331–1338. [Google Scholar] [CrossRef] [PubMed]
- Haglund, M.M.; Cutler, A.B.; Suarez, A.; Dharmapurikar, R.; Lad, S.P.; McDaniel, K.E. The Surgical Autonomy Program: A Pilot Study of Social Learning Theory Applied to Competency-Based Neurosurgical Education. Neurosurgery 2021, 88, E345–E350. [Google Scholar] [CrossRef] [PubMed]
- Kirsch, E.P.; Suarez, A.; McDaniel, K.E.; Dharmapurikar, R.; Dunn, T.; Lad, S.P.; Haglund, M.M. Construct validity of the Surgical Autonomy Program for the training of neurosurgical residents. Neurosurg. Focus 2022, 53, E8. [Google Scholar] [CrossRef] [PubMed]
- Kosmopoulos, V.; Schizas, C. Pedicle screw placement accuracy: A meta-analysis. Spine 2007, 32, E111–E120. [Google Scholar] [CrossRef] [PubMed]
- Sielatycki, J.A.; Mitchell, K.; Leung, E.; Lehman, R.A. State of the art review of new technologies in spine deformity surgery-robotics and navigation. Spine Deform. 2022, 10, 5–17. [Google Scholar] [CrossRef]
- Urakov, T.M.; Chang, K.H.; Burks, S.S.; Wang, M.Y. Initial academic experience and learning curve with robotic spine instrumentation. Neurosurg. Focus 2017, 42, E4. [Google Scholar] [CrossRef] [PubMed]
- Massaad, E.; Shankar, G.M.; Shin, J.H. Novel Applications of Spinal Navigation in Deformity and Oncology Surgery-Beyond Screw Placement. Oper. Neurosurg. 2021, 21 (Suppl. 1), S23–S38. [Google Scholar] [CrossRef]
- Hartl, R. The 6 T‘s of Minimally Invasive Spine Surgery. Glob. Spine J. 2020, 10 (Suppl. 2), 5S–7S. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time | Advancement | Advantages | Disadvantages |
|---|---|---|---|
| 1968 | Wiltse Approach | Intramuscular dissection, pioneering, tissue-preserving | Poor cosmesis, limited exposure |
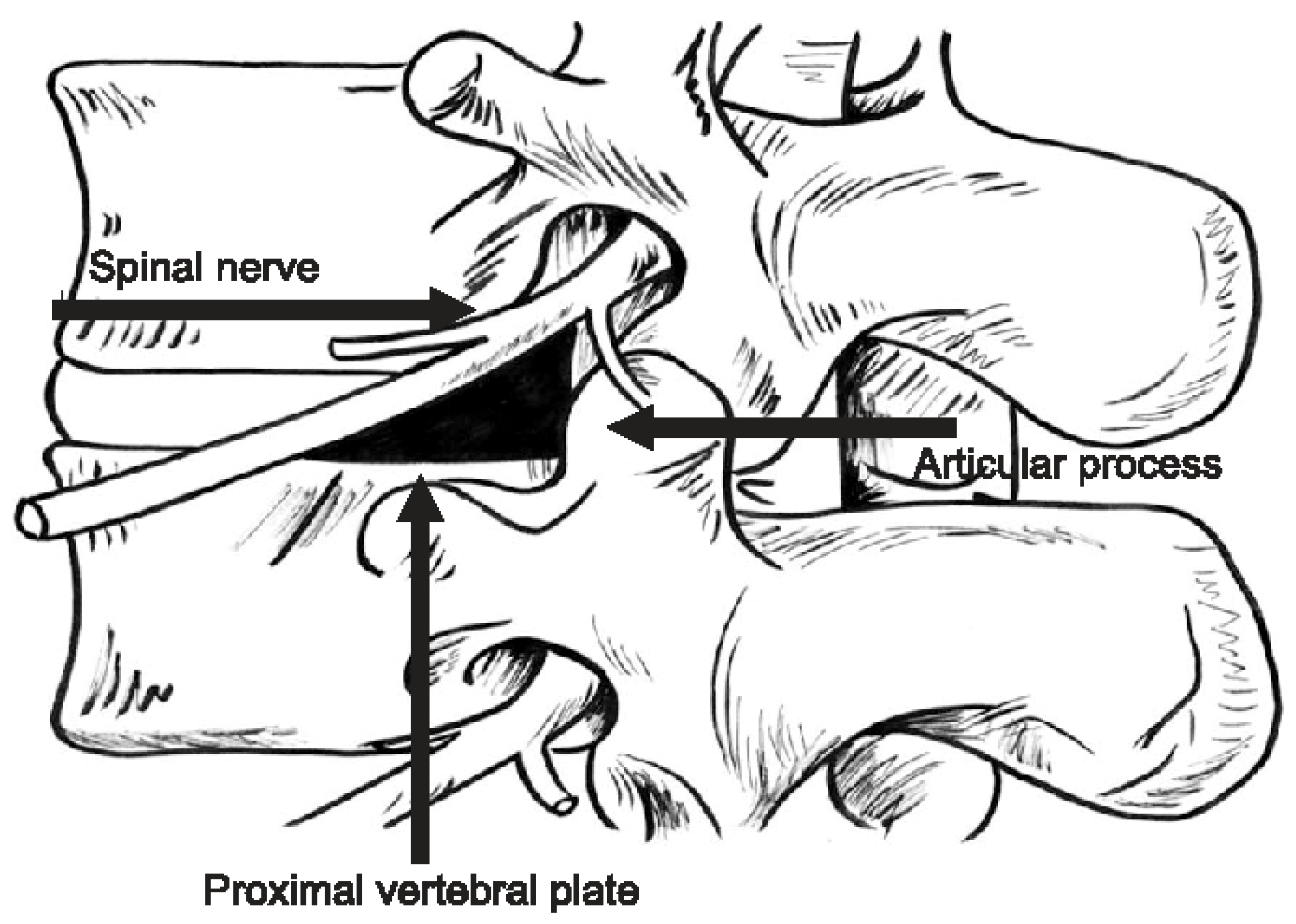
| 1980s | Trans–Kambin Approach | Percutaneous discectomy, ultra-minimally invasive | Possible injury to dorsal root ganglion, reliant on fluoroscopy |
| 1990s–early 2000s | Tubular approaches | Allows direct decompression, minimal tissue disruption, easily adaptible | Unfamiliar visualization, limited exposure |
| Early 2000s | CT-navigation | Accurate, widely available, reduces occupational radiation | Costly, increased radiation for patient, space-occupying |
| 2006 | Lateral-access | Indirect decompression, minimal blood loss, deformity correction | Femoral nerve palsy, possible peritoneal injury, psoas hematoma |
| Mid–2000s | Robotics | Reproducible, minimizes learning curve, indications expanding | Expensive, limited indications, potentially increases operating room time |
| 2000s | Endoscopy | Ultra-minimally invasive, allows for awake surgery | Steep learning curve, equipment and capital investment, limited instrumentation |
| 2010s | Augmented Reality | Familiar anatomic visualization, integrates with existing instrumentation | Accuracy, increased operative time, bulky headset |
| AOSpine Competencies for Minimally Invasive Spine Surgery |
|---|
| 1. Diagnose the patient problem by correlating the clinical finding with imaging and workup |
| 2. Recognize appropriate indications based on your skill set, case experience, and outcomes |
| 3. Select the appropriate MISS procedure for the pathology and indication, and recognize when MISS is not the appropriate option |
| 4. Correctly set up the technology, operating room, and the team of the procedure |
| 5. Perform microscopic minimally invasive procedures: posterior cervical foraminotomy, interlaminar lumbar discectomy, lumbar extraforaminal discectomy, and unilateral laminotomy for bilateral decompression |
| 6. Perform endoscopic procedures: interlaminar lumbar discectomy, transforaminal lumbar foraminotomy and discectomy, and unilateral laminotomy for bilateral decompression |
| 7. Perform the fusion MISS procedures (percutaneous screws and rod placement, (transforaminal lumbar interbody fusion, TLIF) and lateral lumbar interbody fusion (LLIF)) and apply strategies to optimize arthrodesis |
| 8. Manage complications and apply a backup plan |
| 9. Use MISS techniques for revision surgery |
| AOSpine Foundational Procedures and Skills for Minimally Invasive Spine Surgery |
|---|
| Procedures |
| 1. Interlaminar microscopic tubular lumbar discectomy (IMTLD) |
| 2. Posterior microscopic tubular cervical foraminotomy (PMTCF) |
| 3. Extraforaminal microscopic tubular lumbar discectomy (EMTLD) |
| 4. Interlaminar endoscopic lumbar discectomy (IELD) |
| 5. Transforaminal endoscopic lumbar foraminotomy and discectomy (TELF/TELD) |
| 6. Lumbar endoscopic unilateral laminotomy for bilateral decompression (Endoscopic “over the top” decompression or endoscopic LE–ULBD) |
| 7. Microscopic tubular unilateral laminotomy for bilateral decompression (“over the top” decomp, MT–ULBD) |
| 8. Percutaneous screw and rod placement |
| 9. MIS transforaminal lumbar interbody fusion (TLIF) |
| General Skills |
| 1. Using a microscope |
| 2. Using an endoscope |
| 3. Using a burr with an endoscope |
| 4. Using a drill for minimally invasive spine surgery (MISS) |
| 5. Using 2D and 3D navigation and assistive technologies |
| 6. Managing a dural tear |
| 7. Bleeding control |
| 8. Radiation reduction |
| 9. Placing a tubular retractor (or retractor) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, T.Y.; Wang, M.Y. Advances and Challenges in Minimally Invasive Spine Surgery. J. Clin. Med. 2024, 13, 3329. https://doi.org/10.3390/jcm13113329
Wang TY, Wang MY. Advances and Challenges in Minimally Invasive Spine Surgery. Journal of Clinical Medicine. 2024; 13(11):3329. https://doi.org/10.3390/jcm13113329
Chicago/Turabian StyleWang, Timothy Y., and Michael Y. Wang. 2024. "Advances and Challenges in Minimally Invasive Spine Surgery" Journal of Clinical Medicine 13, no. 11: 3329. https://doi.org/10.3390/jcm13113329
APA StyleWang, T. Y., & Wang, M. Y. (2024). Advances and Challenges in Minimally Invasive Spine Surgery. Journal of Clinical Medicine, 13(11), 3329. https://doi.org/10.3390/jcm13113329