
Agreement and Associations between Countermovement Jump, 5-Time Sit-To-Stand, Lower-Limb Muscle Power Equations, and Physical Performance Tests in Community-Dwelling Older Adults

 ,
,  , , ,
, , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participant Recruitment
2.2. Anthropometry and Disease Conditions
2.3. Countermovement Jump
2.4. 5-Time Sit-To-Stand Test and Muscle Power Measures
2.5. Physical Performance Tests
2.6. Statistical Analysis
3. Results
3.1. Participants Characteristics
3.2. Pearson’s Correlation
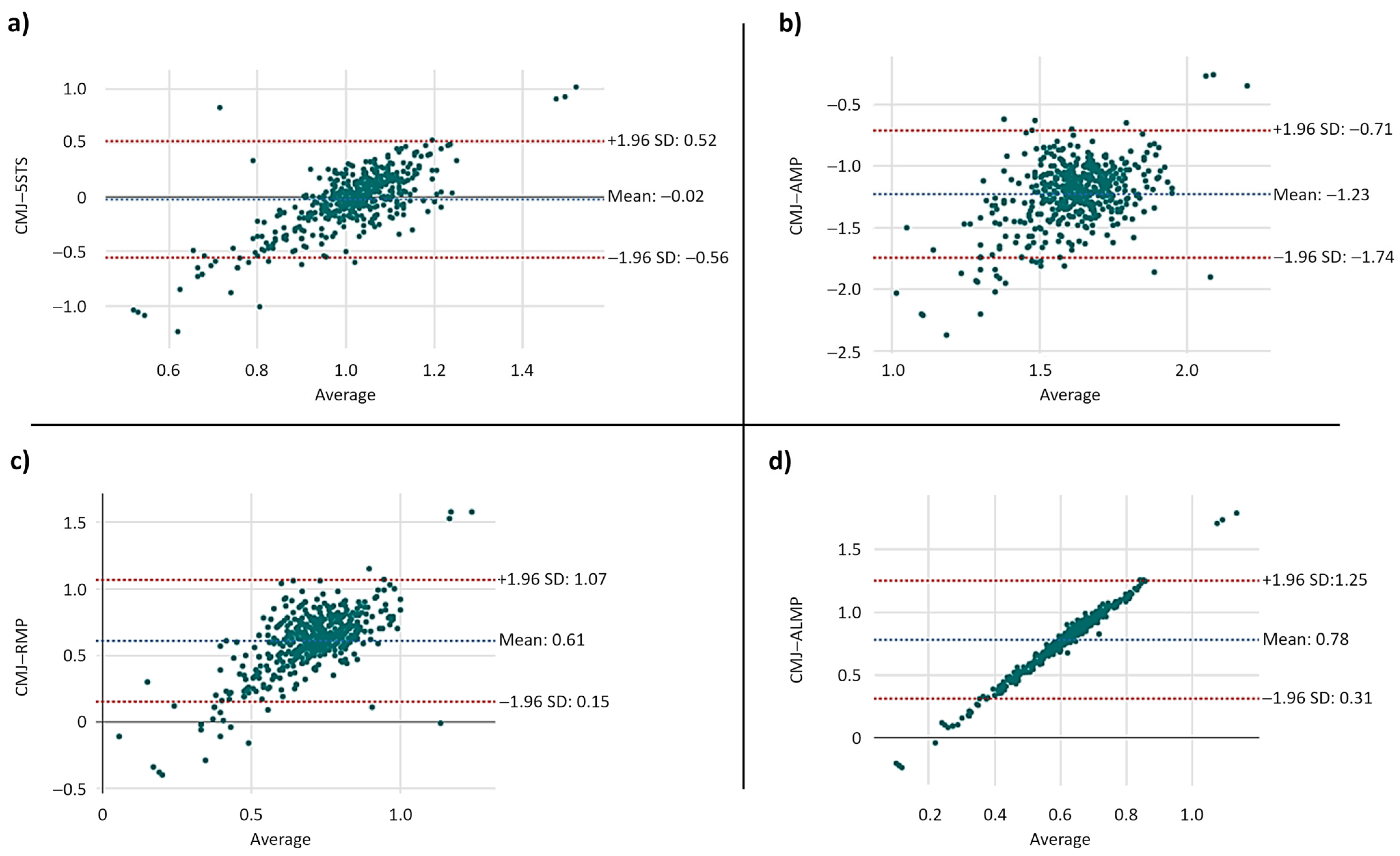
3.3. Bland–Altman Results
3.4. Linear and Multiple Regression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cadore, E.L.; Izquierdo, M. Muscle power training: A hallmark for muscle function retaining in frail clinical setting. J. Am. Med. Dir. Assoc. 2018, 19, 190–192. [Google Scholar] [CrossRef]
- Izquierdo, M.; Cadore, E.L. Muscle Power training in the institutionalized frail: A new approach to counteracting functional declines and very late-life disability. Curr. Med. Res. Opin. 2014, 30, 1385–1390. [Google Scholar] [CrossRef] [PubMed]
- Lauretani, F.; Russo, C.R.; Bandinelli, S.; Bartali, B.; Cavazzini, C.; Di Iorio, A.; Corsi, A.M.; Rantanen, T.; Guralnik, J.M.; Ferrucci, L. Age-associated changes in skeletal muscles and their effect on mobility: An operational diagnosis of sarcopenia. J. Appl. Physiol. 2003, 95, 1851–1860. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Bean, J.F.; Fielding, R.A. Muscle power of the ankle flexors predicts functional performance in community-dwelling older women. J. Am. Geriatr. Soc. 2001, 49, 1161–1167. [Google Scholar] [CrossRef] [PubMed]
- Bean, J.F.; Leveille, S.G.; Kiely, D.K.; Bandinelli, S.; Guralnik, J.M.; Ferrucci, L. A comparison of leg power and leg strength within the inchianti study: Which influences mobility more? J. Gerontol. A Biol. Sci. Med. Sci. 2003, 58, 728–733. [Google Scholar] [CrossRef] [PubMed]
- Hetherington-Rauth, M.; Magalhães, J.P.; Alcazar, J.; Rosa, G.B.; Correia, I.R.; Ara, I.; Sardinha, L.B. Relative sit-to-stand muscle power predicts an older adult’s physical independence at age of 90 yrs beyond that of relative handgrip strength, physical activity, and sedentary time: A cross-sectional analysis. Am. J. Phys. Med. Rehabil. 2022, 101, 995–1000. [Google Scholar] [CrossRef] [PubMed]
- Alcazar, J.; Alegre, L.M.; Van Roie, E.; Magalhães, J.P.; Nielsen, B.R.; González-Gross, M.; Júdice, P.B.; Casajús, J.A.; Delecluse, C.; Sardinha, L.B.; et al. Relative sit-to-stand power: Aging trajectories, functionally relevant cut-off points, and normative data in a large European cohort. J. Cachexia Sarcopenia Muscle 2021, 12, 921–932. [Google Scholar] [CrossRef] [PubMed]
- Losa-Reyna, J.; Alcazar, J.; Carnicero, J.; Alfaro-Acha, A.; Castillo-Gallego, C.; Rosado-Artalejo, C.; Rodríguez-Mañas, L.; Ara, I.; García-García, F.J. Impact of relative muscle power on hospitalization and all-cause mortality in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2022, 77, 781–789. [Google Scholar] [CrossRef] [PubMed]
- Simpkins, C.; Yang, F. Muscle power is more important than strength in preventing falls in community-dwelling older adults. J. Biomech. 2022, 134, 111018. [Google Scholar] [CrossRef]
- Claudino, J.G.; Cronin, J.; Mezêncio, B.; McMaster, D.T.; McGuigan, M.; Tricoli, V.; Amadio, A.C.; Serrão, J.C. The countermovement jump to monitor neuromuscular status: A meta-analysis. J. Sci. Med. Sport 2017, 20, 397–402. [Google Scholar] [CrossRef]
- Hong, N.; Burm, S.W.; Kim, H.C.; Kim, C.O.; Rhee, Y. Jump power predicts fracture risk in older adults independent of sarcopenia and FRAX. J. Bone Miner. Res. 2023, 38, 958–967. [Google Scholar] [CrossRef] [PubMed]
- Marques, D.L.; Neiva, H.P.; Faíl, L.B.; Gil, M.H.; Marques, M.C. Acute effects of low and high-volume resistance training on hemodynamic, metabolic and neuromuscular parameters in older adults. Exp. Gerontol. 2019, 125, 110685. [Google Scholar] [CrossRef]
- Coelho-Junior, H.J.; Rodrigues, B.; de Oliveira Gonçalves, I.; Asano, R.Y.; Uchida, M.C.; Marzetti, E. The physical capabilities underlying timed “up and go” test are time-dependent in community-dwelling older women. Exp. Gerontol. 2018, 104, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Coelho-Júnior, H.J.; de Oliveira Gonçalvez, I.; Sampaio, R.A.C.; Sewo Sampaio, P.Y.; Cadore, E.L.; Izquierdo, M.; Marzetti, E.; Uchida, M.C. Periodized and non-periodized resistance training programs on body composition and physical function of older women. Exp. Gerontol. 2019, 121, 10–18. [Google Scholar] [CrossRef]
- Baltasar-Fernandez, I.; Alcazar, J.; Mañas, A.; Alegre, L.M.; Alfaro-Acha, A.; Rodriguez-Mañas, L.; Ara, I.; García-García, F.J.; Losa-Reyna, J. Relative sit-to-stand power cut-off points and their association with negatives outcomes in older adults. Sci. Rep. 2021, 11, 19460. [Google Scholar] [CrossRef] [PubMed]
- Alcazar, J.; Alegre, L.M.; Suetta, C.; Júdice, P.B.; Van Roie, E.; González-Gross, M.; Rodríguez-Mañas, L.; Casajús, J.A.; Magalhães, J.P.; Nielsen, B.R.; et al. Threshold of relative muscle power required to rise from a chair and mobility limitations and disability in older adults. Med. Sci. Sports Exerc. 2021, 53, 2217–2224. [Google Scholar] [CrossRef] [PubMed]
- Coelho-Júnior, H.J.; Álvarez-Bustos, A.; Rodríguez-Mañas, L.; de Oliveira Gonçalves, I.; Calvani, R.; Picca, A.; Uchida, M.C.; da Silva Aguiar, S.; Marzetti, E. Five-time sit-to-stand-lower limb muscle power in older women: An explorative, descriptive and comparative analysis. J. Frailty Aging 2024, in press. [Google Scholar] [CrossRef]
- Kraemer, W.J.; Newton, R.U. Training for muscular power. Phys. Med. Rehabil. Clin. N. Am. 2000, 11, 341–368. [Google Scholar] [CrossRef] [PubMed]
- Mayson, D.J.; Kiely, D.K.; LaRose, S.I.; Bean, J.F. Leg strength or velocity of movement: Which is more influential on the balance of mobility limited elders? Am. J. Phys. Med. Rehabil. 2008, 87, 969–976. [Google Scholar] [CrossRef]
- Orr, R.; de Vos, N.J.; Singh, N.A.; Ross, D.A.; Stavrinos, T.M.; Fiatarone-Singh, M.A. power training improves balance in healthy older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 78–85. [Google Scholar] [CrossRef]
- Cuoco, A.; Callahan, D.M.; Sayers, S.; Frontera, W.R.; Bean, J.; Fielding, R.A. Impact of muscle power and force on gait speed in disabled older men and women. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, 1200–1206. [Google Scholar] [CrossRef] [PubMed]
- Baltasar-Fernandez, I.; Alcazar, J.; Rodriguez-Lopez, C.; Losa-Reyna, J.; Alonso-Seco, M.; Ara, I.; Alegre, L.M. Sit-to-stand muscle power test: Comparison between estimated and force plate-derived mechanical power and their association with physical function in older adults. Exp. Gerontol. 2021, 145, 111213. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed]
- Roebroeck, M.E.; Doorenbosch, C.A.; Harlaar, J.; Jacobs, R.; Lankhorst, G.J. Biomechanics and muscular activity during sit-to-stand transfer. Clin. Biomech. 1994, 9, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Coelho Junior, H.J.; Rodrigues, B.; da Silva Aguiar, S.; Gonçalves, I.d.O.; Pires, F.d.O.; Asano, R.Y.; Uchida, M.C. Hypertension and functional capacities in community-dwelling older women: A cross-sectional study. Blood Press. 2017, 26, 156–165. [Google Scholar] [CrossRef] [PubMed]
- Coelho-Junior, H.J.; Uchida, M.C.; Gonçalves, I.O.; Calvani, R.; Rodrigues, B.; Picca, A.; Onder, G.; Landi, F.; Bernabei, R.; Marzetti, E. Age- And gender-related changes in physical function in community-dwelling Brazilian adults aged 50 to 102 years. J. Geriatr. Phys. Ther. 2021, 44, E123–E131. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Coelho-Júnior, H.J.; de Oliveira Gonçalves, I.; Landi, F.; Calvani, R.; Tosato, M.; Picca, A.; Marzetti, E. muscle power-related parameters in middle-aged and older Brazilian women: A cross-sectional study. Sci. Rep. 2023, 13, 13186. [Google Scholar] [CrossRef] [PubMed]
- Haff, G.G.; Carlock, J.M.; Hartman, M.J.; Kilgore, J.L.; Kawamori, N.; Jackson, J.R.; Morris, R.T.; Sands, W.A.; Stone, M.H. Force-time curve characteristics of dynamic and isometric muscle actions of elite women olympic weightlifters. J. Strength Cond. Res. 2005, 19, 741–748. [Google Scholar] [CrossRef]
- Young, W.; Wilson, G.; Byrne, C. Relationship between strength qualities and performance in standing and run-up vertical jumps. J. Sports Med. Phys. Fitness 1999, 39, 285–293. [Google Scholar]
- Nuzzo, J.L.; Mcbride, J.M.; Cormie, P.; Mccaulley, G.O. Relationship between countermovement jump performance and multijoint isometric and dynamic tests of strength. J. Strength Cond. Res. 2008, 22, 699–707. [Google Scholar] [CrossRef] [PubMed]
- McMahon, J.J.; Suchomel, T.J.; Lake, J.P.; Comfort, P. Understanding the key phases of the countermovement jump force-time curve. Strength Cond. J. 2018, 40, 96–106. [Google Scholar] [CrossRef]
- Van Hooren, B.; Zolotarjova, J. The difference between countermovement and squat jump performances: A review of underlying mechanisms with practical applications. J. Strength Cond. Res. 2017, 31, 2011–2020. [Google Scholar] [CrossRef]
- Roberts, T.J. Contribution of elastic tissues to the mechanics and energetics of muscle function during movement. J. Exp. Biol. 2016, 219, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Newton, R.U.; Murphy, A.J.; Humphries, B.J.; Wilson, G.J.; Kraemer, W.J.; Häkkinen, K. Influence of load and stretch shortening cycle on the kinematics, kinetics and muscle activation that occurs during explosive upper-body movements. Eur. J. Appl. Physiol. Occup. Physiol. 1997, 75, 333–342. [Google Scholar] [CrossRef]
- Dehail, P.; Bestaven, E.; Muller, F.; Mallet, A.; Robert, B.; Bourdel-Marchasson, I.; Petit, J. Kinematic and electromyographic analysis of rising from a chair during a “sit-to-walk” task in elderly subjects: Role of strength. Clin. Biomech. 2007, 22, 1096–1103. [Google Scholar] [CrossRef]
- Sibella, F.; Galli, M.; Romei, M.; Montesano, A.; Crivellini, M. Biomechanical analysis of sit-to-stand movement in normal and obese subjects. Clin. Biomech. 2003, 18, 745–750. [Google Scholar] [CrossRef]
- Bouchouras, G.; Patsika, G.; Hatzitaki, V.; Kellis, E. Kinematics and knee muscle activation during sit-to-stand movement in women with knee osteoarthritis. Clin. Biomech. 2015, 30, 599–607. [Google Scholar] [CrossRef]
- Radaelli, R.; Trajano, G.S.; Freitas, S.R.; Izquierdo, M.; Cadore, E.L.; Pinto, R.S. Power training prescription in older individuals: Is it safe and effective to promote neuromuscular functional improvements? Sports Med. 2023, 53, 569–576. [Google Scholar] [CrossRef]
- Fragala, M.S.; Cadore, E.L.; Dorgo, S.; Izquierdo, M.; Kraemer, W.J.; Peterson, M.D.; Ryan, E.D. Resistance training for older adults. J. Strength Cond. Res. 2019, 33, 2019–2052. [Google Scholar] [CrossRef]
- American College of Sports Medicine; Chodzko-Zajko, W.J.; Proctor, D.N.; Fiatarone Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef] [PubMed]
- Kuo, H.K.; Leveille, S.G.; Yen, C.J.; Chai, H.M.; Chang, C.H.; Yeh, Y.C.; Yu, Y.H.; Bean, J.F. Exploring how peak leg power and usual gait speed are linked to late-life disability: Data from the National Health and Nutrition Examination Survey (NHANES), 1999–2002. Am. J. Phys. Med. Rehabil. 2006, 85, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Porto, J.M.; Nakaishi, A.P.M.; Cangussu-Oliveira, L.M.; Freire Júnior, R.C.; Spilla, S.B.; Abreu, D.C.C. relationship between grip strength and global muscle strength in community-dwelling older people. Arch. Gerontol. Geriatr. 2019, 82, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Louder, T.; Dolny, D.; Bressel, E. Biomechanical comparison of countermovement jumps performed on land and in water: Age effects. J. Sport Rehabil. 2018, 27, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Lord, S.R.; Murray, S.M.; Chapman, K.; Munro, B.; Tiedemann, A. Sit-to-stand performance depends on sensation, speed, balance, and psychological status in addition to strength in older people. J. Gerontol. A Biol. Sci. Med. Sci. 2002, 57, M539–M543. [Google Scholar] [CrossRef] [PubMed]
- Fabrica, G.; Biancardi, C.M. Commentary: The sit-to-stand muscle power test: An easy, inexpensive and portable procedure to assess muscle power in older people. Exp. Gerontol. 2022, 158, 111652. [Google Scholar] [CrossRef]
- Rosário, J.L.P. A Review of the utilization of baropodometry in postural assessment. J. Bodyw. Mov. Ther. 2014, 18, 215–219. [Google Scholar] [CrossRef]

{kind=link}
| Age, years | 67.6 ± 6.3 |
| Women (%) | 472 (88.4) |
| Body mass, kg | 75.3, 35.3–99.7 |
| Height, m | 1.65, 1.37–1.93 |
| Body mass index, kg/m2 | 27.7 ± 5.3 |
| 5-time sit-to-stand, s | 10.8 ± 2.1 |
| Absolute muscle power, W | 177.3 ± 61.6 |
| Relative muscle power, W/kg | 2.5 ± 0.7 |
| Allometric muscle power, W/m2 | 70.2 ± 26.5 |
| Countermovement jump, cm | 11.5 ± 8.1 |
| Handgrip strength, kg | 24.2 ± 6.8 |
| One-leg stand, s | 15.4 ± 11.9 |
| Timed “up-and-go!”, s | 7.5 ± 2.0 |
| 6 min walking test, m | 568.4 ± 152.3 |
| Walking speed at normal pace, m/s | 1.0 ± 2.7 |
| Walking speed at fast pace, m/s | 1.0 ± 1.0 |
| Hypertension (%) | 351 (65.7) |
| Cardiovascular disease (%) | 48 (9.0) |
| Diabetes mellitus (%) | 92 (17.2) |
| Osteoarthritis (%) | 229 (43.0) |
| Univariate β (95% CI) | p | Adjusted β 1 (95% CI) | p | Adjusted β 2 (95% CI) | p | |
|---|---|---|---|---|---|---|
| Handgrip strength | ||||||
| Countermovement jump | 0.01 (0.08, 0.29) | 0.000 | 0.12 (0.06, 0.18) | 0.000 | 0.19 (0.08, 0.29) | 0.000 |
| 5-time sit-to-stand | −0.46 (−0.74, −0.19) | 0.000 | −0.36 (−0.59, −0.12) | 0.003 | −0.35 (−0.64, −0.05) | 0.019 |
| Absolute muscle power | 0.03 (0.02, 0.04) | 0.000 | 0.02 (0.01, 0.03) | 0.000 | 0.02 (0.01, 0.03) | 0.000 |
| Relative muscle power | 2.58 (1.83, 3.34) | 0.000 | 1.52 (0.85, 2.19) | 0.000 | 1.25 (0.46, 2.03) | 0.002 |
| Allometric muscle power | 0.06 (0.03, 0.08) | 0.000 | 0.05 (0.02, 0.07) | 0.000 | 0.04 (0.01, 0.06) | 0.003 |
| One-leg stand | ||||||
| Countermovement jump | 0.26 (0.13, 0.38) | 0.000 | 0.18 (0.05, 0.31) | 0.005 | 0.07 (−0.13, 0.28) | 0.491 |
| 5-time sit-to-stand | −1.67 (−2.18, −1.15) | 0.000 | −1.54 (−2.04, −1.04) | 0.000 | −1.29 (−1.92, −0.66) | 0.000 |
| Absolute muscle power | 0.01 (−0.00, 0.03) | 0.146 | 0.02 (0.00, 0.04) | 0.007 | 0.01 (−0.01, 0.03) | 0.297 |
| Relative muscle power | 2.78 (1.31, 4.25) | 0.000 | 2.11 (0.65, 3.57) | 0.005 | 1.02 (−0.61, 2.65) | 0.220 |
| Allometric muscle power | 0.02 (−0.02, 0.06) | 0.397 | 0.06 (0.01, 0.12) | 0.008 | 0.03 (−0.02, 0.08) | 0.266 |
| Timed “up-and-go!” | ||||||
| Countermovement jump | −0.07 (−0.09, −0.05) | 0.000 | −0.05 (−0.08, −0.03) | 0.000 | −0.04 (−0.06, −0.02) | 0.000 |
| 5-time sit-to-stand | 0.33 (0.25, 0.40) | 0.000 | 0.31 (0.23, 0.38) | 0.000 | 0.24 (0.19, 0.29) | 0.000 |
| Absolute muscle power | −0.00 (−0.00, −0.00) | 0.000 | −0.00 (−0.00, −0.00) | 0.000 | −0.00 (−0.00, −0.00) | 0.000 |
| Relative muscle power | −0.74 (−0.97, −0.52) | 0.000 | −0.60 (−0.83, −0.37) | 0.000 | −0.37 (−0.52, −0.22) | 0.000 |
| Allometric muscle power | −0.01 (−0.02, −0.00) | 0.000 | −0.02 (−0.02, −0.01) | 0.000 | −0.01 (−0.01, −0.00) | 0.000 |
| 6 min walking test | ||||||
| Countermovement jump | 2.46 (0.80, 4.12) | 0.000 | 1.55 (−0.14, 3.24) | 0.073 | 3.77 (1.17, 6.37) | 0.005 |
| 5-time sit-to-stand | −16.5 (−22.2, −10.7) | 0.000 | −15.2 (−20.9, −9.6) | 0.000 | −17.1 (−24.2, −10.0) | 0.000 |
| Absolute muscle power | 0.32 (0.14, 0.51) | 0.000 | 0.41 (0.21, 0.61) | 0.000 | 0.44 (0.20, 0.67) | 0.000 |
| Relative muscle power | 42.3 (25.8, 58.8) | 0.000 | 36.0 (19.2, 52.8) | 0.000 | 37.6 (18.1, 57.0) | 0.000 |
| Allometric muscle power | 0.77 (0.26, 1.29) | 0.003 | 1.15 (0.57, 1.72) | 0.000 | 1.16 (0.50, 1.83) | 0.001 |
| Walking speed at usual pace | ||||||
| Countermovement jump | −0.00 (−0.03, 0.02) | 0.000 | −0.00 (−0.03, 0.02) | 0.843 | 0.00 (−0.06, 0.06) | 0.986 |
| 5-time sit-to-stand | −0.07 (−0.18, 0.03) | 0.166 | −0.07 (−0.18, 0.03) | 0.169 | −0.08 (−0.25, 0.08) | 0.320 |
| Absolute muscle power | −0.00 (−0.03, 0.04) | 0.825 | −0.01 (−0.00, 0.00) | 0.708 | 0.01 (−0.00, 0.00) | 0.737 |
| Relative muscle power | 0.11 (−0.19, 0.42) | 0.473 | 0.12 (−0.19, 0.44) | 0.428 | 0.16 (−0.29, 0.61) | 0.486 |
| Allometric muscle power | 0.00 (−0.00, 0.01) | 0.549 | 0.00 (−0.00, 0.01) | 0.440 | 0.00 (−0.01, 0.02) | 0.533 |
| Walking speed at fast pace | ||||||
| Countermovement jump | 0.01 (−0.04, 0.07) | 0.004 | 0.00 (−0.05, 0.06) | 0.787 | 0.02 (−0.07, 0.01) | 0.614 |
| 5-time sit-to-stand | −0.09 (−0.30, 0.10) | 0.316 | −0.09 (−0.30, 0.11) | 0.386 | −0.08 (−0.36, 0.20) | 0.572 |
| Absolute muscle power | −0.00 (−0.00, 0.00) | 0.788 | 0.00 (−0.00, 0.00) | 0.923 | 0.00 (−0.00, 0.00) | 0.980 |
| Relative muscle power | 0.14 (−0.44, 0.72) | 0.640 | 0.15 (−0.45, 0.76) | 0.610 | 0.13 (−0.62, 0.90) | 0.727 |
| Allometric muscle power | 0.00 (−0.01, 0.01) | 0.980 | 0.00 (−0.01, 0.02) | 0.683 | 0.00 (−0.02, 0.02) | 0.821 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coelho-Júnior, H.J.; da Silva Aguiar, S.; de Oliveira Gonçalves, I.; Álvarez-Bustos, A.; Rodríguez-Mañas, L.; Uchida, M.C.; Marzetti, E. Agreement and Associations between Countermovement Jump, 5-Time Sit-To-Stand, Lower-Limb Muscle Power Equations, and Physical Performance Tests in Community-Dwelling Older Adults. J. Clin. Med. 2024, 13, 3380. https://doi.org/10.3390/jcm13123380
Coelho-Júnior HJ, da Silva Aguiar S, de Oliveira Gonçalves I, Álvarez-Bustos A, Rodríguez-Mañas L, Uchida MC, Marzetti E. Agreement and Associations between Countermovement Jump, 5-Time Sit-To-Stand, Lower-Limb Muscle Power Equations, and Physical Performance Tests in Community-Dwelling Older Adults. Journal of Clinical Medicine. 2024; 13(12):3380. https://doi.org/10.3390/jcm13123380
Chicago/Turabian StyleCoelho-Júnior, Hélio José, Samuel da Silva Aguiar, Ivan de Oliveira Gonçalves, Alejandro Álvarez-Bustos, Leocadio Rodríguez-Mañas, Marco Carlos Uchida, and Emanuele Marzetti. 2024. "Agreement and Associations between Countermovement Jump, 5-Time Sit-To-Stand, Lower-Limb Muscle Power Equations, and Physical Performance Tests in Community-Dwelling Older Adults" Journal of Clinical Medicine 13, no. 12: 3380. https://doi.org/10.3390/jcm13123380
APA StyleCoelho-Júnior, H. J., da Silva Aguiar, S., de Oliveira Gonçalves, I., Álvarez-Bustos, A., Rodríguez-Mañas, L., Uchida, M. C., & Marzetti, E. (2024). Agreement and Associations between Countermovement Jump, 5-Time Sit-To-Stand, Lower-Limb Muscle Power Equations, and Physical Performance Tests in Community-Dwelling Older Adults. Journal of Clinical Medicine, 13(12), 3380. https://doi.org/10.3390/jcm13123380