
Atypical Presentations of Hydroxychloroquine Retinopathy: A Case Series Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Evaluation
2.3. Definitions and Analysis
3. Results
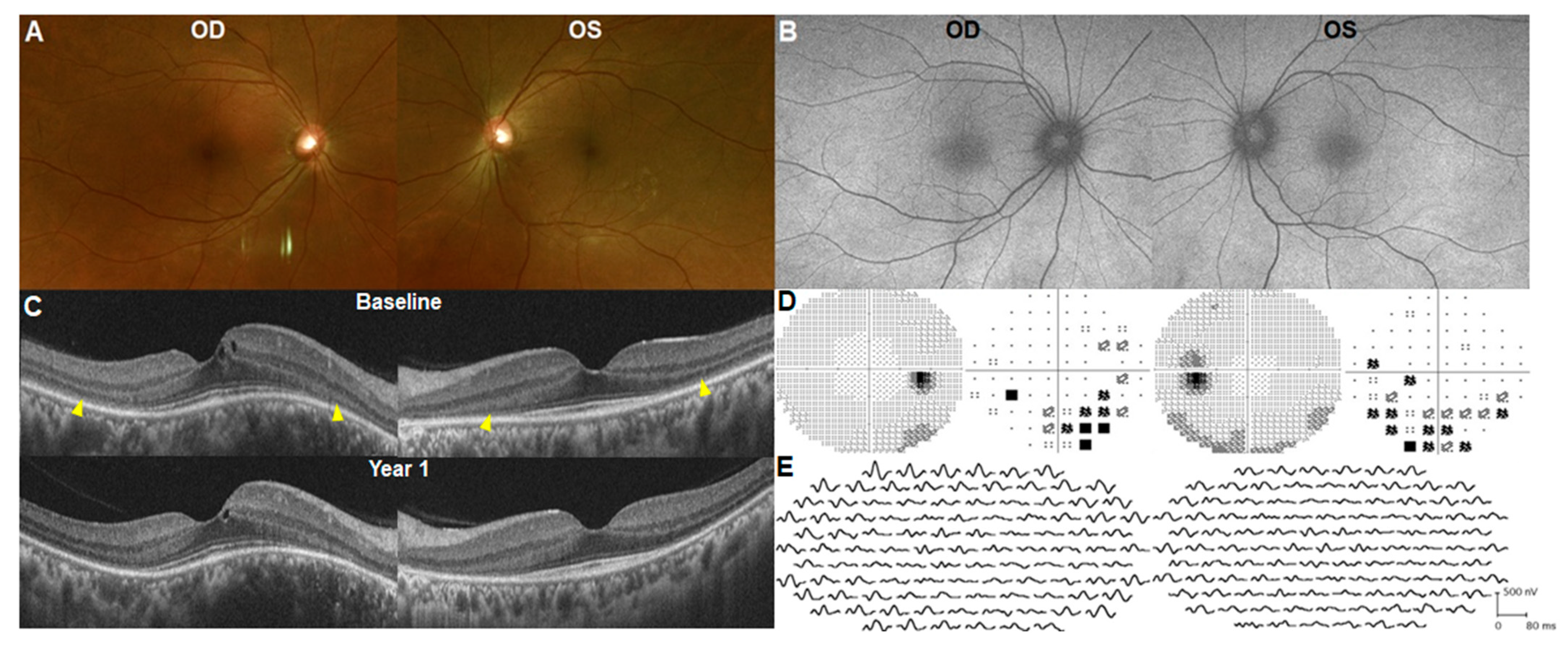
3.1. Early Presentation/Onset (within 1 Year)
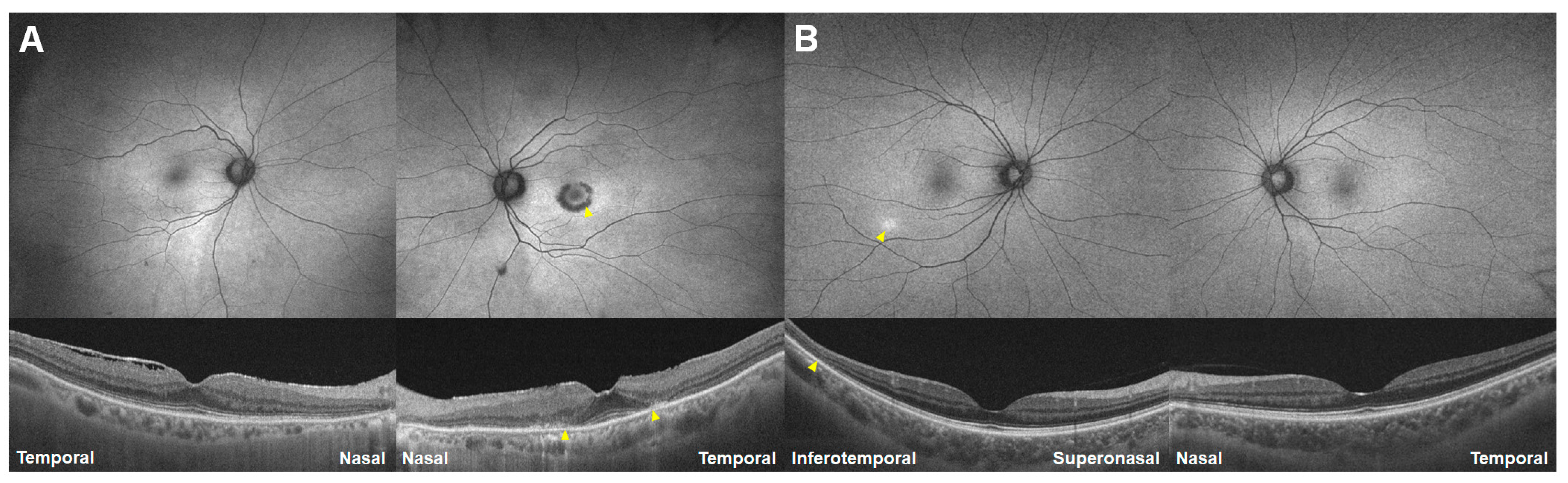
3.2. Nasal Peripheral Involvement
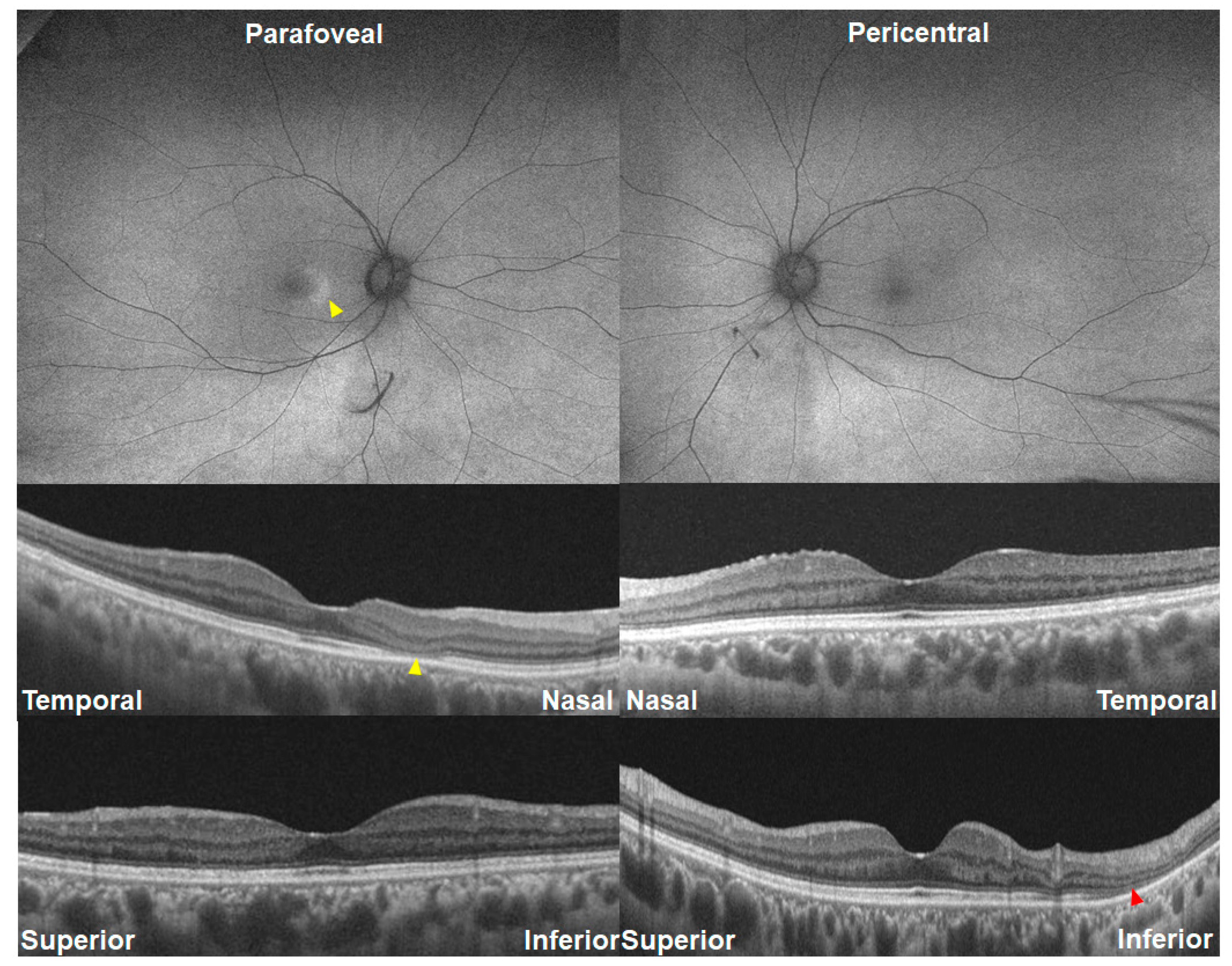
3.3. Perivascular Involvement
3.4. Bitemporal Hemianopsia Due to Nasal Extensive Lesion
3.5. Unilateral Involvement
3.6. Asymmetric Involvement in Retinopathy Severity/Pattern
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marmor, M.F.; Kellner, U.; Lai, T.Y.; Melles, R.B.; Mieler, W.F.; American Academy of Ophthalmology. Recommendations on Screening for Chloroquine and Hydroxychloroquine Retinopathy (2016 Revision). Ophthalmology 2016, 123, 1386–1394. [Google Scholar] [CrossRef] [PubMed]
- Pham, B.H.; Marmor, M.F. Sequential Changes in Hydroxychloroquine Retinopathy up to 20 Years after Stopping the Drug: Implications for Mild versus Severe Toxicity. Retina 2019, 39, 492–501. [Google Scholar] [CrossRef] [PubMed]
- Melles, R.B.; Marmor, M.F. Pericentral retinopathy and racial differences in hydroxychloroquine toxicity. Ophthalmology 2015, 122, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Marmor, M.F.; Melles, R.B. Hydroxychloroquine and the retina. JAMA 2015, 313, 847–848. [Google Scholar] [CrossRef] [PubMed]
- Marmor, M.F.; Kellner, U.; Lai, T.Y.; Lyons, J.S.; Mieler, W.F. Revised recommendations on screening for chloroquine and hydroxychloroquine retinopathy. Ophthalmology 2011, 118, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, I.H.; Sharma, S.; Luqmani, R.; Downes, S.M. Hydroxychloroquine retinopathy. Eye 2017, 31, 828–845. [Google Scholar] [CrossRef] [PubMed]
- Browning, D.J.; Lee, C. Scotoma analysis of 10-2 visual field testing with a white target in screening for hydroxychloroquine retinopathy. Clin. Ophthalmol. 2015, 9, 943–952. [Google Scholar] [CrossRef] [PubMed]
- Browning, D.J.; Lee, C. Test-retest variability of multifocal electroretinography in normal volunteers and short-term variability in hydroxychloroquine users. Clin. Ophthalmol. 2014, 8, 1467–1473. [Google Scholar] [CrossRef] [PubMed]
- Browning, D.J.; Lee, C. Relative sensitivity and specificity of 10-2 visual fields, multifocal electroretinography, and spectral domain optical coherence tomography in detecting hydroxychloroquine and chloroquine retinopathy. Clin. Ophthalmol. 2014, 8, 1389–1399. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.; Blaha, G.R.; Marx, J.L. Humphrey visual field findings in hydroxychloroquine toxicity. Eye 2011, 25, 1535–1545. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, I.H.; Latheef, F.; Ardern-Jones, M.; Lotery, A.J. New recommendations for retinal monitoring in hydroxychloroquine users: Baseline testing is no longer supported. Br. J. Dermatol. 2021, 185, 435–438. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, I.H.; Bukhari, M.; Galloway, J.; Lotery, A.J. Baseline retinal testing is no longer recommended for hydroxychloroquine users in the United Kingdom. Rheumatology 2021, 60, 2037–2039. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, I.H.; Foot, B.; Lotery, A.J. The Royal College of Ophthalmologists recommendations on monitoring for hydroxychloroquine and chloroquine users in the United Kingdom (2020 revision): Executive summary. Eye 2021, 35, 1532–1537. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.J.; Joung, J.; Lee, B.R. Evaluation of Hydroxychloroquine Retinopathy Using Ultra-Widefield Fundus Autofluorescence: Peripheral Findings in the Retinopathy. Am. J. Ophthalmol. 2020, 209, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, J.T.; Costenbader, K.H.; Desmarais, J.; Ginzler, E.M.; Fett, N.; Goodman, S.M.; O’Dell, J.R.; Schmajuk, G.; Werth, V.P.; Melles, R.B.; et al. American College of Rheumatology, American Academy of Dermatology, Rheumatologic Dermatology Society, and American Academy of Ophthalmology 2020 Joint Statement on Hydroxychloroquine Use with Respect to Retinal Toxicity. Arthritis Rheumatol. 2021, 73, 908–911. [Google Scholar] [CrossRef] [PubMed]
- Melles, R.B.; Marmor, M.F. The risk of toxic retinopathy in patients on long-term hydroxychloroquine therapy. JAMA Ophthalmol. 2014, 132, 1453–1460. [Google Scholar] [CrossRef] [PubMed]
- Ozawa, H.; Ueno, S.; Ohno-Tanaka, A.; Sakai, T.; Hashiguchi, M.; Shimizu, M.; Fujinami, K.; Ahn, S.J.; Kondo, M.; Browning, D.J.; et al. Ocular findings in Japanese patients with hydroxychloroquine retinopathy developing within 3 years of treatment. Jpn. J. Ophthalmol. 2021, 65, 472–481. [Google Scholar] [CrossRef] [PubMed]
- Jeltsch, B.M.; Sarraf, D.; Madjdpour, D.; Hanson, J.V.M.; Pfiffner, F.K.; Koller, S.; Berger, W.; Barthelmes, D.; Al-Sheikh, M. Rapid onset hydroxychloroquine toxicity. Retin. Cases Brief Rep. 2024, 18, 351–354. [Google Scholar] [CrossRef] [PubMed]
- Marmor, M.F.; Durbin, M.; de Sisternes, L.; Pham, B.H. Sequential Retinal Thickness Analysis Shows Hydroxychloroquine Damage before Other Screening Techniques. Retin. Cases Brief Rep. 2021, 15, 185–196. [Google Scholar] [CrossRef] [PubMed]
- Yoshihara, M.K.; Lui, F. Neuroanatomy, Bitemporal Hemianopsia. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Typical Case |
|---|---|
| Sex | Typically women |
| Duration of hydroxychloroquine use | Typically occur after 5 year’s use |
| Structural findings | Photoreceptor defects and/or retinal pigment epithelium defects on OCT or hyper- or hypoautofluorescence on FAF in the parafoveal or pericentral areas |
| Functional (perimetric) findings | Paracentral patchy/ring scotoma, central island |
| Eye involvement | Bilateral, symmetric |
| Characteristics | Case 1 | Case 2 | Case 3 | Case 4 | Case 5 | Case 6 | Case 7 |
|---|---|---|---|---|---|---|---|
| Age/sex | 44/F | 72/F | 75/F | 60/F | 54/F | 75/F | 39/F |
| Medical diagnosis for HCQ use | RA | RA | SLE | SLE | Sjogren’s syndrome | SLE | SLE |
| Daily dose of hydroxychloroquine/body weight ratio | 5.4 mg/kg | 3.3 mg/kg | 3.0 mg/kg | 5.6 mg/kg | 4.2 mg/kg | 8.0 mg/kg | 4.0 mg/kg |
| Duration of hydroxychloroquine use | 6 months | 25 years | 20 years | 20 years | 6 years | 23 years | 8 years |
| Structural findings | Photoreceptor defects on pericentral areas | Hypo-AF on nasal far periphery and inf. pericentral photoreceptor defect | Hypo-AF on nasal far periphery and posterior pole | Perivascular hypo-AF | Half-ring-shaped nasal peripheral hypo-AF | Ring-shaped parafoveal hypo-AF only in the left eye | Localized pericentral hyper-AF (early stage) in the right and hypo-AF in the left (severe stage) |
| Functional (perimetric) findings | Paracentral scotoma | Patchy scotoma | Central island | Ring scotoma | Bitemporal hemianopsia with central sparing | Ring scotoma only in the left eye | Sup. patchy scotoma |
| Symmetricity between the two eyes | Symmetric in both pattern and severity | Symmetric | Symmetric | Symmetric | Symmetric | Asymmetric (unilateral involvement) | Asymmetric in severity |
| Atypical Presentations | Figure No. | Prevalence, n (%) | Methods for Detection |
|---|---|---|---|
| Early disease onset | Figure 2 | 1 (1.1%) | Baseline screening performed using OCT within 1 year of hydroxychloroquine use |
| Far peripheral involvement (dominance) | Figure 3 | 4 (4.3%) | Widefield FAF |
| Perivascular involvement | Figure 4 | 1 (1.1%) | Widefield FAF |
| Bitemporal hemianopsia due to nasal extensive lesion | Figure 5 | 1 (1.1%) | Automated visual field, widefield FAF |
| Unilateral involvement | Figure 6 | 2 (2.1%) | Standard screening modalities * |
| Asymmetric involvement | Figure 7 and Figure 8 | 7 (7.4%) | |
| in pattern of retinopathy | Figure 7 | 6 (6.3%) | Widefield OCT or FAF (for detection of pericentral pattern in one eye) |
| in severity of retinopathy | Figure 8 | 2 (2.1%) | Standard screening modalities * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.M.; Kwon, H.Y.; Ahn, S.J. Atypical Presentations of Hydroxychloroquine Retinopathy: A Case Series Study. J. Clin. Med. 2024, 13, 3411. https://doi.org/10.3390/jcm13123411
Lee JM, Kwon HY, Ahn SJ. Atypical Presentations of Hydroxychloroquine Retinopathy: A Case Series Study. Journal of Clinical Medicine. 2024; 13(12):3411. https://doi.org/10.3390/jcm13123411
Chicago/Turabian StyleLee, Jung Min, Hyeon Yoon Kwon, and Seong Joon Ahn. 2024. "Atypical Presentations of Hydroxychloroquine Retinopathy: A Case Series Study" Journal of Clinical Medicine 13, no. 12: 3411. https://doi.org/10.3390/jcm13123411