
Risk Factors and Interventions for Suicide in Huntington’s Disease—A Systematic Review

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. PICO Model
2.3. Study Selection
2.4. Data Extraction and Analysis
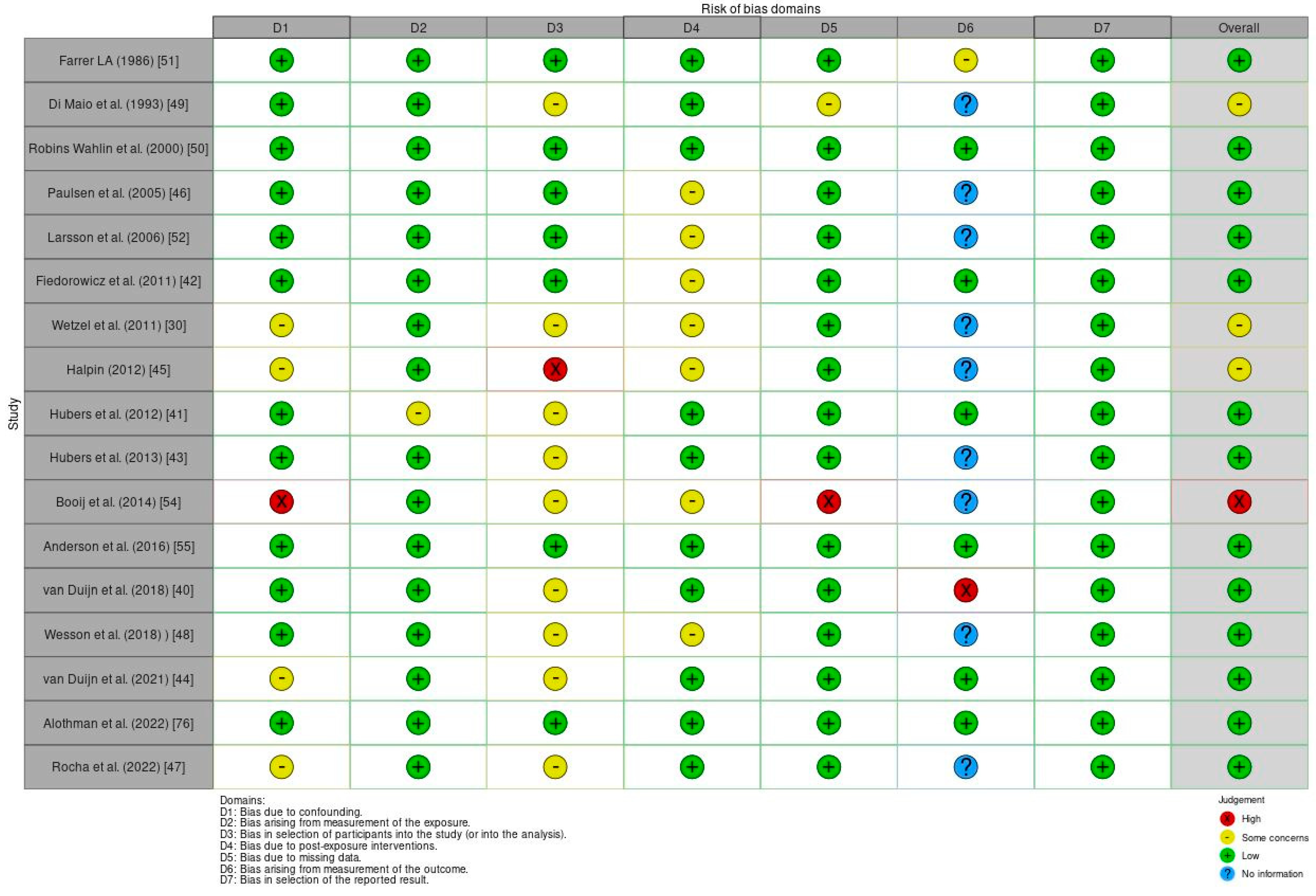
2.5. Risk of Bias within Individual Studies
3. Results
3.1. Synthesis of Evidence

{kind=link}
{kind=link}
| Study | Design | Aims | Patients | Measures | Major Findings |
|---|---|---|---|---|---|
| Farrer LA (1986) [51] | Retrospective Study | Explore the implications for preclinical testing of individuals at risk of HD based on the incidence of suicide and attempted suicide | A total population of 831 HD patients | AQ | The study revealed that 5.7% of fatalities among individuals affected by the condition were due to suicide, and 27.6% of patients made at least one suicide attempt. |
| Di Maio L et al. (1993) [49] | Cross-sectional Study | Assess the risk of suicide in HD | 2793 individuals | Family history and affected questionnaire | Suicide was identified as the reported cause of death in 205 individuals, accounting for 7.3% of the studied subjects. |
| Robins Wahlin TB et al. (2000) [50] | Cross-sectional Study | Assess the possible impacts of presymptomatic testing | 600 patients with HD and 3000 individuals at risk | GHQ-30; LSA; AQ; SIBS; LSI | Both groups showed increased SI. Non-carriers had more suicide attempts, but both groups had significant psychiatric dysfunction. |
| Paulsen JS et al. (2005) [46] | Prospective Longitudinal Study | To identify critical periods of suicide risk in HD | 2835 subjects who received a diagnosis of HD | UHDRS | Suicide is more likely to occur in the early stages of HD and when patients experience the loss of autonomy. |
| Larsson MU et al. (2006) [52] | Prospective Follow-up Study | Reports a two-year follow-up of psychological effects of predictive testing for Huntington’s disease | 35 carriers and 58 non-carriers of the HD gene. | UHDRS; GHQ-30; BDI; SIBS; LSI; LSA | Before predictive testing, both carriers and non-carriers showed elevated SI. Carriers experienced rising depression scores and more frequent suicidal thoughts over time. |
| Fiedorowicz JG et al. (2011) [42] | Prospective Study | Determine risk factors for suicidal behaviour, defined as suicide or attempted suicide, in prodromal HD | 735 cases with HD gene expansion and 194 non-gene-expanded controls. | PSS; LES; and UHDRS | A history of suicide attempts and the existence of depression were associated with suicidal behaviour in the prodromal stage of HD. |
| Wetzel HH et al. (2011) [30] | Cross-sectional Study | Improved understanding of risk factors for suicide in HD | 4000 patients with or at risk of HD | UHDRS | Psychiatric symptoms were linked to elevated rates of SI in HD. |
| Hubers AA et al. (2012) [41] | Cross-sectional Study | Study the prevalence and traits of suicidality, encompassing both thoughts and actions, in individuals with HD | 152 mutation carriers and 56 non-carriers | PBA | A connection has been established between a depressive mood and the potential prediction of suicidality in HD. |
| Halpin M (2012) [45] | Qualitative Study | Evaluate if suicide is attributed to mental pathology or the concept of rational suicide | 20 individuals with HD and 10 informal caregivers | Semi-structured interview | Study participants did not link suicide with mental pathology. Instead, they perceived suicide as a response to the reality of living with HD. |
| Hubers AA et al. (2013) [43] | Cross-sectional Study | Investigate correlates and predictors of SI in HD | 2106 HD mutation carriers | PBA-s; HDQLIFE | Depressed mood and benzodiazepine use predicted new-onset SI, while prior suicide attempts did not. |
| Booij SJ et al. (2014) [54] | Cross-sectional Study | Examine the occurrence of suicidal thoughts in individuals diagnosed with HD or identified gene carriers | 134 patients | TFC subscale of the UHDRS; MMSE | From a total of 101 respondents, 75% admitted to end-of-life thoughts, and 11% considered care, while 64% contemplated euthanasia or PAS. |
| Anderson KE et al. (2016) [55] | Cross-sectional Study | Investigate correlations between, mood disorders, CAG expansion status, and motor symptoms with SI in at-risk HD patients | 801 subjects | UHDRS, Barratt Impulsivity Scale | Individuals with suicidal ideation showed higher levels of behavioural symptoms, with feelings of hopelessness and anxiety being strongly associated with this ideation. |
| van Duijn E et al. (2018) [40] | Cross-sectional Study | Examine the complete range of suicidality, encompassing SI, suicidal actions, and self-injurious behaviour | 1451 HD gene expansion carriers | C-SSRS, UHDRS, PBA | Among HD gene expansion carriers, 6.5% reported a lifetime suicide attempt. SI was associated with a depressed mood, with irritability playing a lesser role. |
| Wesson M et al. (2018) [48] | Cross-sectional Study | Examine SI and the impact of assessment modality in HD | 496 participants with premanifest or manifest HD | PBA-s; 16 | Individuals with HD were more likely to endorse suicidal ideation via self-report than via in-person interview |
| van Duijn E et al. (2021) [44] | Prospective Global Study | Investigate the incidence of completed suicide and suicide attempts in HD | 20,912 participants, comprising 15,924 HDGECs and 4988 non-HDGECs | C-SSRS; UHDRS | Suicide rate in HDGEC: 72 per 100,000 person-years, compared to 8 per 100,000 person-years in non-HDGEC settings. Proportionate mortality from suicide in HDGECs: 4.6%. |
| Alothman D et al. (2022) [56] | Retrospective Study | Examine the relative risk of suicide mortality in HD | 594,674 individuals | CPRD; HES; ONS | Risk of death from suicide was markedly elevated in younger individuals with HD compared to HC people. |
| Rocha NP et al. (2022) [47] | Observational Study | Pinpoint clinical factors linked with a past occurrence of depression and suicidal tendencies in individuals carrying the HD gene | Periodic data set 4; N = 11,582 | Binary logistic regression | The prevalence of depression and suicidality were high among HD gene carriers. |
3.2. Risk of Bias
4. Discussion
4.1. Future Directions
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Caron, N.S.; Wright, G.E.B.; Hayden, M.R. Huntington Disease. 23 October 1998 [Updated 11 June 2020]. GeneReviews®. University of Washington, Seattle, WA, USA, 1993–2024. Available online: https://pubmed.ncbi.nlm.nih.gov/20301482/ (accessed on 21 April 2024).
- Reiner, A.; Dragatsis, I.; Dietrich, P. Genetics and neuropathology of Huntington’s disease. Int. Rev. Neurobiol. 2011, 98, 325–372. [Google Scholar] [CrossRef] [PubMed]
- Albin, R.L.; Tagle, D.A. Genetics and molecular biology of Huntington’s disease. Trends Neurosci. 1995, 18, 11–14. [Google Scholar] [CrossRef] [PubMed]
- Medina, A.; Mahjoub, Y.; Shaver, L.; Pringsheim, T. Prevalence and Incidence of Huntington’s Disease: An Updated Systematic Review and Meta-Analysis. Mov. Disord. 2022, 37, 2327–2335. [Google Scholar] [CrossRef] [PubMed]
- Kay, C.; Collins, J.A.; Wright, G.E.B.; Baine, F.; Miedzybrodzka, Z.; Aminkeng, F.; Semaka, A.J.; McDonald, C.; Davidson, M.; Madore, S.J.; et al. The molecular epidemiology of Huntington disease is related to intermediate allele frequency and haplotype in the general population. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2018, 177, 346–357. [Google Scholar] [CrossRef] [PubMed]
- Bruzelius, E.; Scarpa, J.; Zhao, Y.; Basu, S.; Faghmous, J.H.; Baum, A. Huntington’s disease in the United States: Variation by demographic and socioeconomic factors. Mov. Disord. 2019, 34, 858–865. [Google Scholar] [CrossRef] [PubMed]
- De Agostinho, L.A.; dos Santos da Silva, I.; de Maia, L.A.; Azevedo, M.A.; Faria, T.M.; Apolinario, T.A.; Pereira, S.P.; de Reis, R.L.; Dos Santos, S.R.; Paiva, C.L. A Study of a Geographical Cluster of Huntington’s Disease in a Brazilian Town of Zona da Mata, Minas Gerais State. Eur. Neurol. 2015, 74, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Squitieri, F.; Mazza, T.; Maffi, S.; De Luca, A.; AlSalmi, Q.; AlHarasi, S.; Collins, J.A.; Kay, C.; Baine-Savanhu, F.; Landwhermeyer, B.G.; et al. Tracing the mutated HTT and haplotype of the African ancestor who spread Huntington disease into the Middle East. Genet. Med. 2020, 22, 1903–1908. [Google Scholar] [CrossRef] [PubMed]
- Baine, F.K.; Kay, C.; Ketelaar, M.E.; Collins, J.A.; Semaka, A.; Doty, C.N.; Krause, A.; Greenberg, L.J.; Hayden, M.R. Huntington disease in the South African population occurs on diverse and ethnically distinct genetic haplotypes. Eur. J. Hum. Genet. 2013, 21, 1120–1127. [Google Scholar] [CrossRef] [PubMed]
- Schulte, J.; Littleton, J.T. The biological function of the Huntingtin protein and its relevance to Huntington’s Disease pathology. Curr. Trends Neurol. 2011, 5, 65–78. [Google Scholar]
- Ajitkumar, A.; De Jesus, O. Huntington Disease. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Rangel-Barajas, C.; Rebec, G.V. Dysregulation of Corticostriatal Connectivity in Huntington’s Disease: A Role for Dopamine Modulation. J. Huntington’s Dis. 2016, 5, 303–331. [Google Scholar] [CrossRef]
- Rüb, U.; Vonsattel, J.P.; Heinsen, H.; Korf, H.W. The Neuropathology of Huntington’s disease: Classical findings, recent developments and correlation to functional neuroanatomy. Adv. Anat. Embryol. Cell Biol. 2015, 217, 1–146. [Google Scholar]
- Mehrabi, N.F.; Waldvogel, H.J.; Tippett, L.J.; Hogg, V.M.; Synek, B.J.; Faull, R.L. Symptom heterogeneity in Huntington’s disease correlates with neuronal degeneration in the cerebral cortex. Neurobiol. Dis. 2016, 96, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Kiferle, L.; Mazzucchi, S.; Unti, E.; Pesaresi, I.; Fabbri, S.; Nicoletti, V.; Volterrani, D.; Cosottini, M.; Bonuccelli, U.; Ceravolo, R. Nigral involvement and nigrostriatal dysfunction in Huntington’s disease: Evidences from an MRI and SPECT study. Park. Relat. Disord. 2013, 19, 800–805. [Google Scholar] [CrossRef] [PubMed]
- Nopoulos, P.C. Huntington disease: A single-gene degenerative disorder of the striatum. Dialogues Clin. Neurosci. 2016, 18, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Finkbeiner, S. Huntington’s Disease. Cold Spring Harb. Perspect. Biol. 2011, 3, a007476. [Google Scholar] [CrossRef] [PubMed]
- Mann, R.K.; Edwards, R.; Zhou, J.; Fenney, A.; Jog, M.; Duval, C. Comparing movement patterns associated with Huntington’s chorea and Parkinson’s dyskinesia. Exp. Brain Res. 2012, 218, 639–654. [Google Scholar] [CrossRef] [PubMed]
- Dayalu, P.; Albin, R.L. Huntington disease: Pathogenesis and treatment. Neurol. Clin. 2015, 33, 101–114. [Google Scholar] [CrossRef] [PubMed]
- Farrar, A.M.; Murphy, C.A.; Paterson, N.E.; Oakeshott, S.; He, D.; Alosio, W.; McConnell, K.; Menalled, L.B.; Ramboz, S.; Park, L.C.; et al. Cognitive deficits in transgenic and knock-in HTT mice parallel those in Huntington’s disease. J. Huntington’s Dis. 2014, 3, 145–158. [Google Scholar] [CrossRef]
- Curtin, P.C.; Farrar, A.M.; Oakeshott, S.; Sutphen, J.; Berger, J.; Mazzella, M.; Cox, K.; He, D.; Alosio, W.; Park, L.C.; et al. Cognitive Training at a Young Age Attenuates Deficits in the zQ175 Mouse Model of HD. Front. Behav. Neurosci. 2016, 9, 361. [Google Scholar] [CrossRef]
- Frank, S. Treatment of Huntington’s disease. Neurotherapeutics 2014, 11, 153–160. [Google Scholar] [CrossRef]
- Paulsen, J.S.; Conybeare, R.A. Cognitive changes in Huntington’s disease. Adv. Neurol. 2005, 96, 209–225. [Google Scholar] [PubMed]
- Morris, L.A.; O’Callaghan, C.; Le Heron, C. Disordered Decision Making: A Cognitive Framework for Apathy and Impulsivity in Huntington’s Disease. Mov. Disord. 2022, 37, 1149–1163. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, J.M.; Salmon, D.P.; Corey-Bloom, J.; Gamst, A.; Paulsen, J.S.; Jerkins, S.; Jacobson, M.W.; Peavy, G. Behavioural abnormalities contribute to functional decline in Huntington’s disease. J. Neurol. Neurosurg. Psychiatry 2003, 74, 120–122. [Google Scholar] [CrossRef]
- Rodrigues, F.B.; Abreu, D.; Damásio, J.; Goncalves, N.; Correia-Guedes, L.; Coelho, M.; Ferreira, J.J.; REGISTRY Investigators of the European Huntington’s Disease Network. Survival, Mortality, Causes and Places of Death in a European Huntington’s Disease Prospective Cohort. Mov. Disord. Clin. Pract. 2017, 4, 737–742. [Google Scholar] [CrossRef]
- Kachian, Z.R.; Cohen-Zimerman, S.; Bega, D.; Gordon, B.; Grafman, J. Suicidal ideation and behavior in Huntington’s disease: Systematic review and recommendations. J. Affect. Disord. 2019, 250, 319–329. [Google Scholar] [CrossRef]
- Solberg, O.K.; Filkuková, P.; Frich, J.C.; Feragen, K.J.B. Age at Death and Causes of Death in Patients with Huntington Disease in Norway in 1986–2015. J. Huntington’s Dis. 2018, 7, 77–86. [Google Scholar] [CrossRef]
- Turecki, G.; Brent, D.A. Suicide and suicidal behavior. Lancet 2016, 387, 1227–1239. [Google Scholar] [CrossRef] [PubMed]
- Wetzel, H.H.; Gehl, C.R.; Dellefave-Castillo, L.; Schiffman, J.F.; Shannon, K.M.; Paulsen, J.S.; Huntington Study Group. Suicidal ideation in Huntington disease: The role of comorbidity. Psychiatry Res. 2011, 188, 372–376. [Google Scholar] [CrossRef] [PubMed]
- Huntington Study Group. Tetrabenazine as antichorea therapy in Huntington disease: A randomized controlled trial. Neurology 2006, 66, 366–372. [Google Scholar] [CrossRef]
- Dorsey, E.R.; Brocht, A.F.; Nichols, P.E.; Darwin, K.C.; Anderson, K.E.; Beck, C.A.; Singh, S.; Biglan, K.M.; Shoulson, I. Depressed mood and suicidality in individuals exposed to tetrabenazine in a large Huntington disease observational study. J. Huntington’s Dis. 2013, 2, 509–515. [Google Scholar] [CrossRef]
- Sampaio, C.; Ware, J.J.; Macleod, M.; Wagenmakers, E.J.; Munafò, M. Reader response: Evaluating depression and suicidality in tetrabenazine users with Huntington disease. Neurology 2019, 92, 447–448. [Google Scholar] [CrossRef]
- Schultz, J.L.; Killoran, A.; Nopoulos, P.C.; Chabal, C.C.; Moser, D.J.; Kamholz, J.A. Evaluating depression and suicidality in tetrabenazine users with Huntington disease. Neurology 2018, 91, e202–e207. [Google Scholar] [CrossRef]
- Nock, M.K.; Borges, G.; Bromet, E.J.; Cha, C.B.; Kessler, R.C.; Lee, S. Suicide and suicidal behavior. Epidemiol. Rev. 2008, 30, 133–154. [Google Scholar] [CrossRef] [PubMed]
- Harmer, B.; Lee, S.; Duong, T.V.H.; Saadabadi, A. Suicidal Ideation. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Morgan, R.L.; Rooney, A.A.; Taylor, K.W.; Thayer, K.A.; Raquel, A.; Silva, R.A.; Courtney Lemeris, C.; Akl, E.A.; Bateson, T.F.; et al. A tool to assess risk of bias in non-randomized follow-up studies of exposure effects (ROBINS-E). Environ. Int. 2024, 186, 108602. [Google Scholar] [CrossRef]
- Van Duijn, E.; Vrijmoeth, E.M.; Giltay, E.J.; Bernhard Landwehrmeyer, G.; REGISTRY investigators of the European Huntington’s Disease Network. Suicidal ideation and suicidal behavior according to the C-SSRS in a European cohort of Huntington’s disease gene expansion carriers. J. Affect. Disord. 2018, 228, 194–204. [Google Scholar] [CrossRef] [PubMed]
- Hubers, A.A.; Reedeker, N.; Giltay, E.J.; Roos, R.A.; van Duijn, E.; van der Mast, R.C. Suicidality in Huntington’s disease. J. Affect. Disord. 2012, 136, 550–557. [Google Scholar] [CrossRef]
- Fiedorowicz, J.G.; Mills, J.A.; Ruggle, A.; Langbehn, D.; Paulsen, J.S.; PREDICT-HD Investigators of the Huntington Study Group. Suicidal behavior in prodromal Huntington disease. Neurodegener. Dis. 2011, 8, 483–490. [Google Scholar] [CrossRef]
- Hubers, A.A.; van Duijn, E.; Roos, R.A.; Craufurd, D.; Rickards, H.; Bernhard Landwehrmeyer, G.; van der Mast, R.C.; Giltay, E.J.; REGISTRY investigators of the European Huntington’s Disease Network. Suicidal ideation in a European Huntington’s disease population. J. Affect. Disord. 2013, 151, 248–258. [Google Scholar] [CrossRef]
- Van Duijn, E.; Fernandes, A.R.; Abreu, D.; Ware, J.J.; Neacy, E.; Sampaio, C. Incidence of completed suicide and suicide attempts in a global prospective study of Huntington’s disease. BJPsych Open 2021, 7, e158. [Google Scholar] [CrossRef] [PubMed]
- Halpin, M. Accounts of suicidality in the Huntington disease community. Omega 2012, 65, 317–334. [Google Scholar] [CrossRef] [PubMed]
- Paulsen, J.S.; Hoth, K.F.; Nehl, C.; Stierman, L. Critical periods of suicide risk in Huntington’s disease. Am. J. Psychiatry 2005, 162, 725–731. [Google Scholar] [CrossRef] [PubMed]
- Rocha, N.P.; Tuazon, M.R.; Patino, J.; Furr Stimming, E.; Teixeira, A.L. Clinical Correlates of Depression and Suicidality in Huntington Disease: An Analysis of the Enroll-HD Observational Study. Cogn. Behav. Neurol. 2022, 35, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Wesson, M.; Boileau, N.R.; Perlmutter, J.S.; Paulsen, J.S.; Barton, S.K.; McCormack, M.K.; Carlozzi, N.E. Suicidal Ideation Assessment in Individuals with Premanifest and Manifest Huntington Disease. J. Huntington’s Dis. 2018, 7, 239–249. [Google Scholar] [CrossRef]
- Di Maio, L.; Squitieri, F.; Napolitano, G.; Campanella, G.; Trofatter, J.A.; Conneally, P.M. Suicide risk in Huntington’s disease. J. Med. Genet. 1993, 30, 293–295. [Google Scholar] [CrossRef] [PubMed]
- Robins Wahlin, T.B.; Bäckman, L.; Lundin, A.; Haegermark, A.; Winblad, B.; Anvret, M. High suicidal ideation in persons testing for Huntington’s disease. Acta Neurol. Scand. 2000, 102, 150–161. [Google Scholar] [CrossRef] [PubMed]
- Farrer, L.A. Suicide and attempted suicide in Huntington disease: Implications for preclinical testing of persons at risk. Am. J. Med. Genet. 1986, 24, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Larsson, M.U.; Luszcz, M.A.; Bui, T.H.; Wahlin, T.B. Depression and suicidal ideation after predictive testing for Huntington’s disease: A two-year follow-up study. J. Genet. Couns. 2006, 15, 361–374. [Google Scholar] [CrossRef]
- David Klonsky, E.; Kotov, R.; Bakst, S.; Rabinowitz, J.; Bromet, E.J. Hopelessness as a predictor of attempted suicide among first admission patients with psychosis: A 10-year cohort study. Suicide Life Threat. Behav. 2012, 42, 1–10. [Google Scholar] [CrossRef]
- Booij, S.J.; Tibben, A.; Engberts, D.P.; Marinus, J.; Roos, R.A. Thinking about the end of life: A common issue for patients with Huntington’s disease. J. Neurol. 2014, 261, 2184–2191. [Google Scholar] [CrossRef]
- Anderson, K.E.; Eberly, S.; Groves, M.; Kayson, E.; Marder, K.; Young, A.B.; Shoulson, I.; PHAROS Investigators. Risk Factors for Suicidal Ideation in People at Risk for Huntington’s Disease. J. Huntington’s Dis. 2016, 5, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Alothman, D.; Marshall, C.R.; Tyrrell, E.; Lewis, S.; Card, T.; Fogarty, A. Risk of mortality from suicide in patients with Huntington’s disease is increased compared to the general population in England. J. Neurol. 2022, 269, 4436–4439. [Google Scholar] [CrossRef] [PubMed]
- Alejos, M.; Vázquez-Bourgon, J.; Santurtún, M.; Riancho, J.; Santurtún, A. Do patients diagnosed with a neurological disease present increased risk of suicide? Neurologia 2023, 38, 41–46. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization, Comprehensive Mental Health Action Plan 2013–2030; World Health Organisation: Geneva, Switzerland, 2013.
- Rodriguez Santana, I.; Frank, S.; Doherty, M.; Willock, R.; Hamilton, J.; Hubberstey, H.; Stanley, C.; Vetter, L.; Winkelmann, M.; Dolmetsch, R.E.; et al. Humanistic Burden of Huntington Disease: Evidence From the Huntington Disease Burden of Illness Study. Neurol. Clin. Pract. 2022, 12, e172–e180. [Google Scholar] [CrossRef] [PubMed]
- Zarotti, N.; D’Alessio, B.; Scocchia, M.; Casella, M.; Squitieri, F. “I Wouldn’t Even Know What to Ask for”: Patients’ and Caregivers’ Experiences of Psychological Support for Huntington’s Disease in Italy. NeuroSci 2024, 5, 98–113. [Google Scholar] [CrossRef]
- Bonelli, R.M.; Cummings, J.L. Frontal-subcortical circuitry and behavior. Dialogues Clin. Neurosci. 2007, 9, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Dondanville, D.S.; Hanson-Kahn, A.K.; Kavanaugh, M.S.; Siskind, C.E.; Fanos, J.H. “This could be me”: Exploring the impact of genetic risk for Huntington’s disease young caregivers. J. Community Genet. 2019, 10, 291–302. [Google Scholar] [CrossRef]
- Booij, S.J.; Engberts, D.P.; Rödig, V.; Tibben, A.; Roos, R.A. A plea for end-of-life discussions with patients suffering from Huntington’s disease: The role of the physician. J. Med. Ethics 2013, 39, 621–624. [Google Scholar] [CrossRef]
- Zarotti, N.; Dale, M.; Eccles, F.J.R.; Simpson, J. More than Just a Brain Disorder: A Five-Point Manifesto for Psychological Care for People with Huntington’s Disease. J. Pers. Med. 2022, 12, 64. [Google Scholar] [CrossRef]
- Simpson, J.; Eccles, F.J.; Zarotti, N. Extended Evidence-Based Guidance on Psychological Interventions for Psychological Difficulties in Individuals with Huntington’s Disease, Parkinson’s Disease, Motor Neurone Disease, and Multiple Sclerosis; Lancaster University: Lancaster, UK, 2021. [Google Scholar]
- Eccles, F.J.R.; Craufurd, D.; Smith, A.; Davies, R.; Glenny, K.; Homberger, M.; Rose, L.; Theed, R.; Peeren, S.; Rogers, D.; et al. Experiences of Mindfulness-Based Cognitive Therapy for Premanifest Huntington’s Disease. J. Huntingt. Dis. 2021, 10, 277–291. [Google Scholar] [CrossRef] [PubMed]
- A’Campo, L.E.I.; Spliethoff-Kamminga, N.G.A.; Roos, R.A.C. The Patient Education Program for Huntington’s Disease (PEP-HD). J. Huntingt. Dis. 2012, 1, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Eccles, F.J.R.; Craufurd, D.; Smith, A.; Davies, R.; Glenny, K.; Homberger, M.; Peeren, S.; Rogers, D.; Rose, L.; Skitt, Z.; et al. A Feasibility Investigation of Mindfulness-Based Cognitive Therapy for People with Huntington’s Disease. Pilot. Feasibility Stud. 2020, 6, 90. [Google Scholar] [CrossRef] [PubMed]
- Fisher, C.A.; Brown, A. Sensory Modulation Intervention and Behaviour Support Modification for the Treatment of Severe Aggression in Huntington’s Disease. A Single Case Experimental Design. Neuropsychol. Rehabil. 2017, 27, 891–903. [Google Scholar] [CrossRef] [PubMed]
- Zarotti, N.; Dale, M.; Eccles, F.; Simpson, J. Psychological Interventions for People with Huntington’s Disease: A Call to Arms. J. Huntingt. Dis. 2020, 9, 231–243. [Google Scholar] [CrossRef] [PubMed]
- British Psychological Society. Psychological Interventions for People with Huntington’s Disease, Parkinson’s Disease, Motor Neurone Disease, and Multiple Sclerosis: Evidence-Based Guidance; British Psychological Society: Leicester, UK, 2021. [Google Scholar]
- Silver, A. Cognitive-behavioural therapy with a Huntington’s gene positive patient. Patient Educ. Couns. 2003, 49, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Sher, L.; Oquendo, M.A.; Mann, J.J. Risk of suicide in mood disorders. Clin. Neurosci. Res. 2001, 1, 337–344. [Google Scholar] [CrossRef]
- Johansson, L.; Lindqvist, P.; Eriksson, A. Teenage suicide cluster formation and contagion: Implications for primary care. BMC Fam. Pract. 2006, 7, 32. [Google Scholar] [CrossRef] [PubMed]
- Hubers, A.A.; Hamming, A.; Giltay, E.J.; von Faber, M.; Roos, R.A.; van der Mast, R.C.; van Duijn, E. Suicidality in Huntington’s Disease: A Qualitative Study on Coping Styles and Support Strategies. J. Huntingtons Dis. 2016, 5, 185–198. [Google Scholar] [CrossRef]
- Sturrock, A.; Leavitt, B.R. The clinical and genetic features of Huntington disease. J. Geriatr. Psychiatry Neurol. 2010, 23, 243–259. [Google Scholar] [CrossRef]
- Mestre, T.A.; Sampaio, C. Huntington Disease: Linking Pathogenesis to the Development of Experimental Therapeutics. Curr. Neurol. Neurosci. Rep. 2017, 17, 18. [Google Scholar] [CrossRef] [PubMed]
- Wild, E.J.; Tabrizi, S.J. Therapies targeting DNA and RNA in Huntington’s disease. Lancet Neurol. 2017, 16, 837–847. [Google Scholar] [CrossRef] [PubMed]

| Databases | PubMed, Cochrane, and Web of Science |
|---|---|
| Search Terms | (“suicid”[All Fields] OR “suicidal ideation”[MeSH Terms] OR (“suicidal”[All Fields] AND “ideation”[All Fields]) OR “suicidal ideation”[All Fields] OR “suicidality”[All Fields] OR “suicidal”[All Fields] OR “suicidally”[All Fields] OR “suicidals”[All Fields] OR “sui-cide”[MeSH Terms] OR “suicide”[All Fields] OR “suicides”[All Fields] OR “suicide s”[All Fields] OR “suicided”[All Fields] OR “suiciders”[All Fields]) AND (“huntington”[All Fields] OR “huntington s”[All Fields] OR “huntingtons”[All Fields]) |
| Exclusion Criteria | (i) case studies and reviews; (ii) articles with a lack of an assessment of suicide risk; (iii) duplicate studies; (iv) animal studies; (v) non-English studies. |
| Inclusion Criteria | (i) articles that enrolled adult patients with HD; (ii) studies that specifically assessed the relationship between HD and suicide or suicide risk factors; (iii) articles published in the English language only. |
| Review Process | Titles, abstracts, and full texts were reviewed by two investigators (AG and IV) independently. A third researcher (LC) made the final decision in case of disagreement on inclusion/exclusion criteria. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grimaldi, A.; Veneziani, I.; Culicetto, L.; Quartarone, A.; Lo Buono, V. Risk Factors and Interventions for Suicide in Huntington’s Disease—A Systematic Review. J. Clin. Med. 2024, 13, 3437. https://doi.org/10.3390/jcm13123437
Grimaldi A, Veneziani I, Culicetto L, Quartarone A, Lo Buono V. Risk Factors and Interventions for Suicide in Huntington’s Disease—A Systematic Review. Journal of Clinical Medicine. 2024; 13(12):3437. https://doi.org/10.3390/jcm13123437
Chicago/Turabian StyleGrimaldi, Alessandro, Isabella Veneziani, Laura Culicetto, Angelo Quartarone, and Viviana Lo Buono. 2024. "Risk Factors and Interventions for Suicide in Huntington’s Disease—A Systematic Review" Journal of Clinical Medicine 13, no. 12: 3437. https://doi.org/10.3390/jcm13123437
APA StyleGrimaldi, A., Veneziani, I., Culicetto, L., Quartarone, A., & Lo Buono, V. (2024). Risk Factors and Interventions for Suicide in Huntington’s Disease—A Systematic Review. Journal of Clinical Medicine, 13(12), 3437. https://doi.org/10.3390/jcm13123437