
Aortic Stenosis and the Evolution of Cardiac Damage after Transcatheter Aortic Valve Replacement

 ,
,  , , , , , , and
, , , , , , and
Abstract
1. Introduction
2. Methods
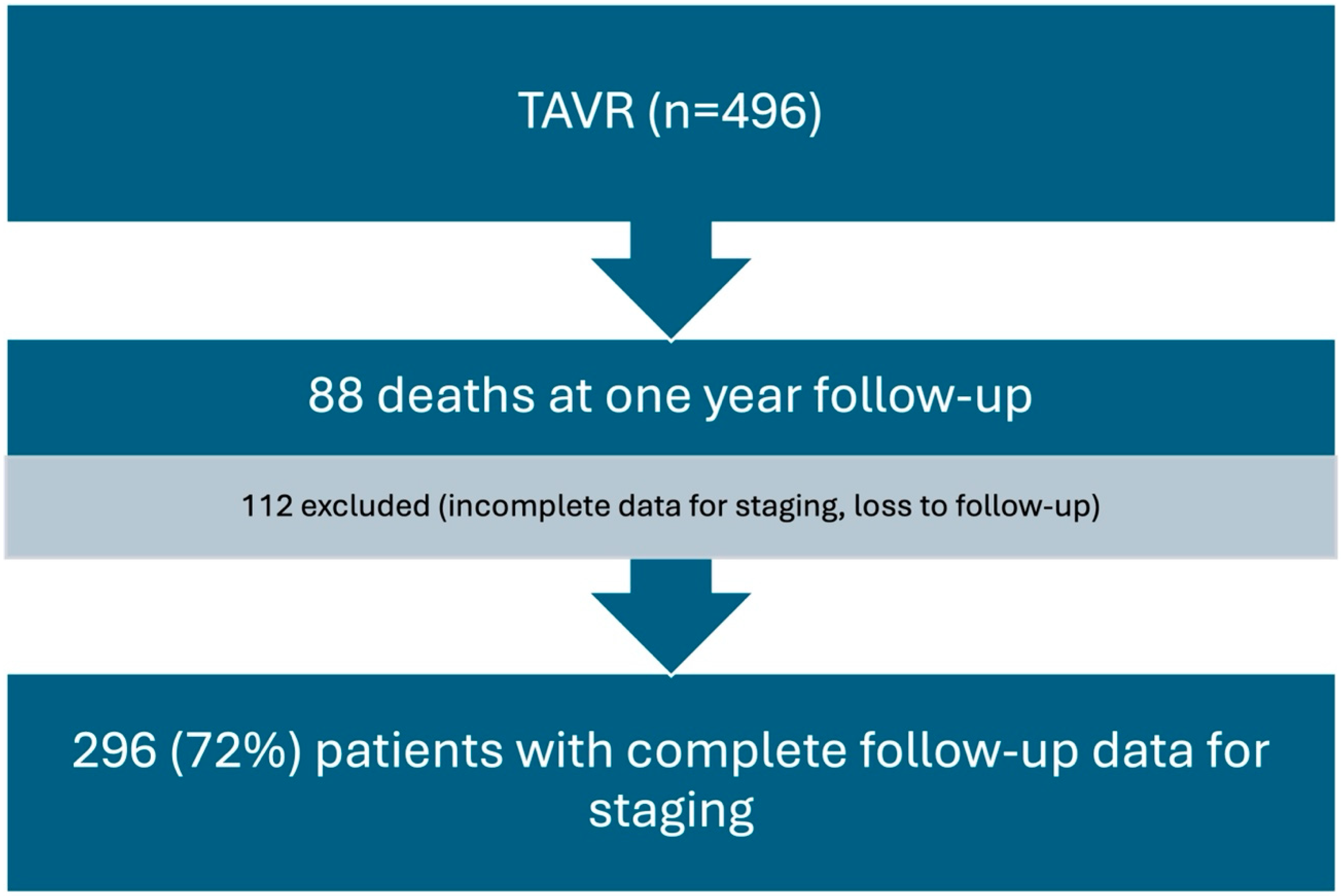
2.1. Design and Setting
2.2. Definitions, Outcome, and Data Collection
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Echocardiographic Characteristics
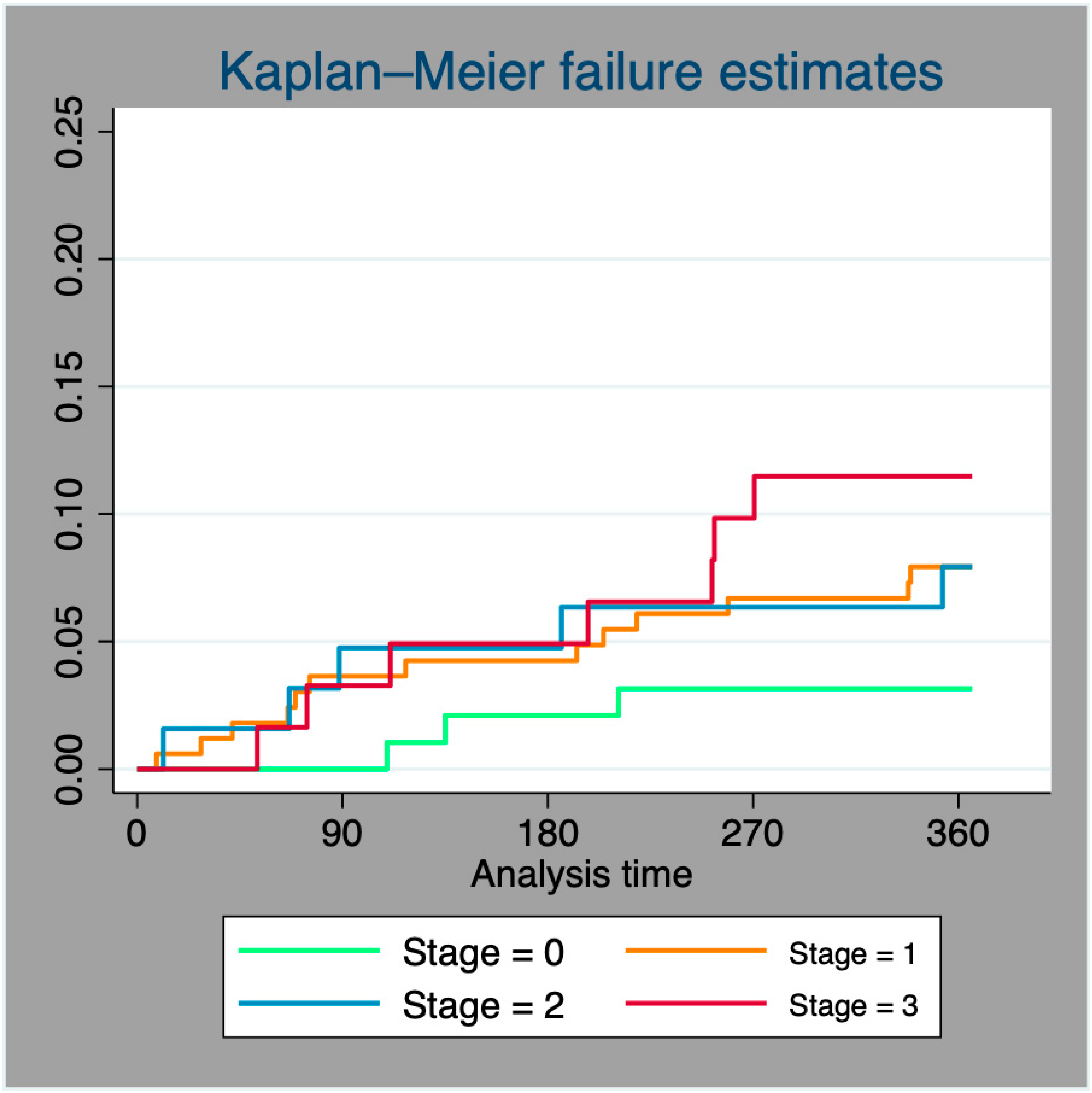
3.3. One-Year Mortality
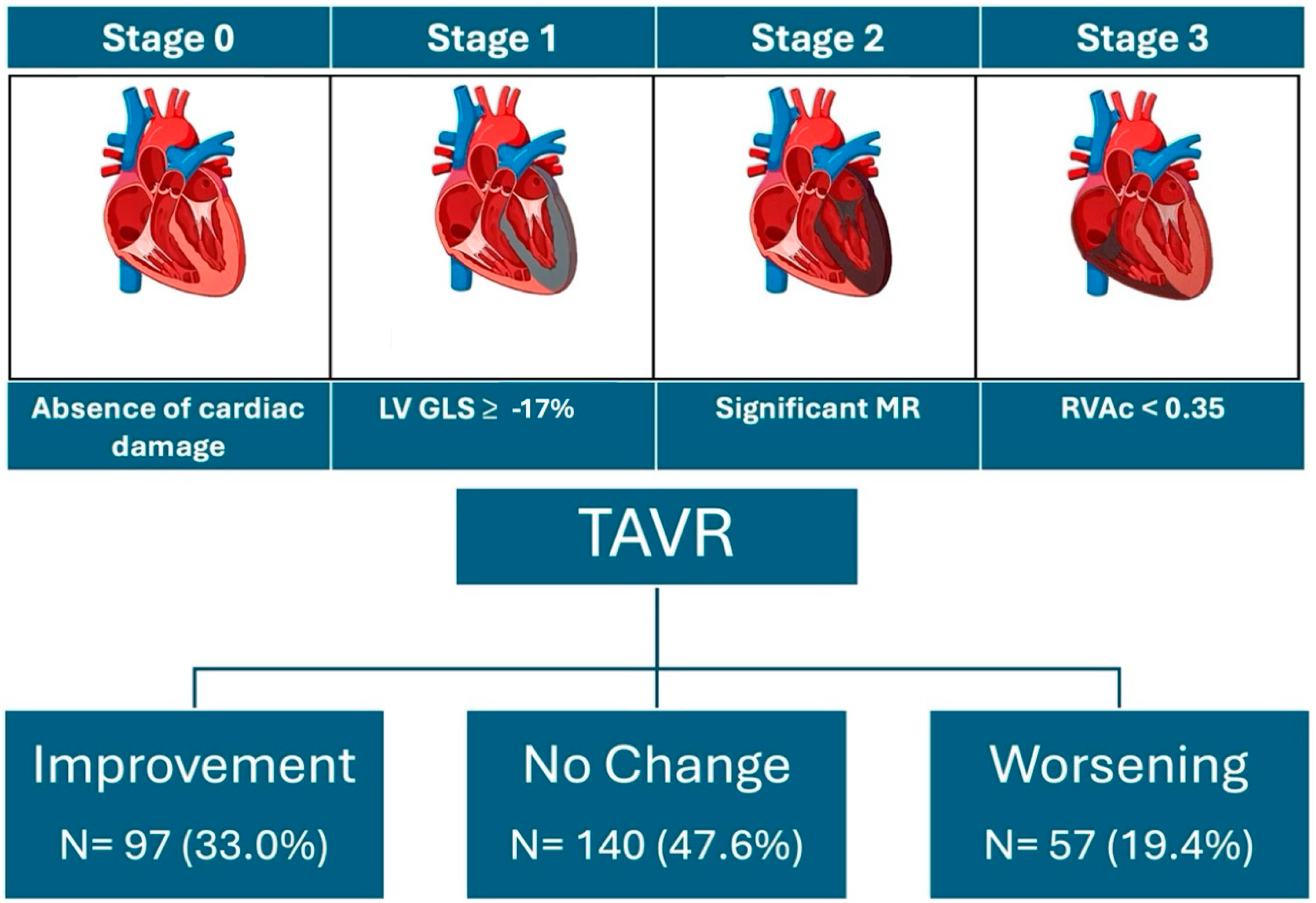
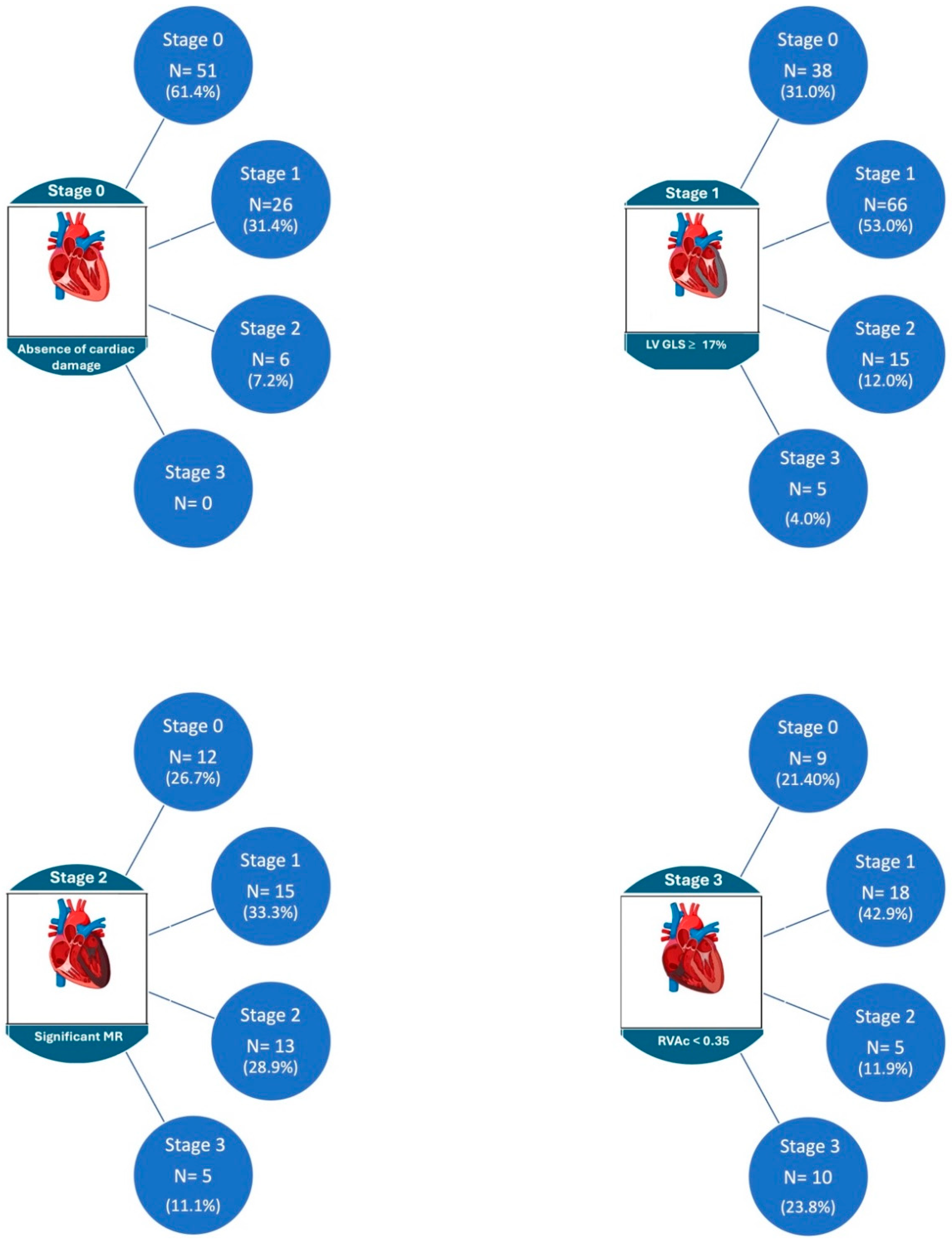
3.4. Evolution of Cardiac Damage at One-Year Follow-Up
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coffey, S.; Cairns, B.J.; Iung, B. The modern epidemiology of heart valve disease. Heart 2016, 102, 75–85. [Google Scholar] [CrossRef]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Généreux, P.; Pibarot, P.; Redfors, B.; Mack, M.J.; Makkar, R.R.; A Jaber, W.; Svensson, L.G.; Kapadia, S.; Tuzcu, E.M.; Thourani, V.H.; et al. Staging classification of aortic stenosis based on the extent of cardiac damage. Eur. Heart J. 2017, 38, 3351–3358. [Google Scholar] [CrossRef] [PubMed]
- Okuno, T.; Heg, D.; Lanz, J.; Praz, F.; Brugger, N.; Stortecky, S.; Windecker, S.; Pilgrim, T. Refined staging classification of cardiac damage associated with aortic stenosis and outcomes after transcatheter aortic valve implantation. Eur. Heart J. Qual. Care Clin. Outcomes 2021, 7, 532–541. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez-Ortiz, E.; Olmos, C.; Carrión-Sanchez, I.; Jiménez-Quevedo, P.; Nombela-Franco, L.; Párraga, R.; Gil-Abizanda, S.; Mahía, P.; Luaces, M.; de Agustín, J.A.; et al. Redefining cardiac damage staging in aortic stenosis: The value of GLS and RVAc. Eur. Heart J. Cardiovasc. Imaging 2023, 24, 1608–1617. [Google Scholar] [CrossRef] [PubMed]
- Généreux, P.; Pibarot, P.; Redfors, B.; Bax, J.J.; Zhao, Y.; Makkar, R.R.; Kapadia, S.; Thourani, V.H.; Mack, M.J.; Nazif, T.M.; et al. Evolution and Prognostic Impact of Cardiac Damage After Aortic Valve Replacement. J. Am. Coll. Cardiol. 2022, 80, 783–800. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Liu, S.; Han, X.; Chen, Y.; Chen, H.; Dong, S.; Song, B. Impact of Chronic Kidney Disease on the Prognosis of Transcatheter Aortic Valve Replacement in Patients with Aortic Stenosis: A Meta-Analysis of 133624 Patients. Ann. Thorac. Cardiovasc. Surg. 2022, 28, 83–95. [Google Scholar] [CrossRef]
- Gupta, T.; Goel, K.; Kolte, D.; Khera, S.; Villablanca, P.A.; Aronow, W.S.; Bortnick, A.E.; Slovut, D.P.; Taub, C.C.; Kizer, J.R.; et al. Association of Chronic Kidney Disease With In-Hospital Outcomes of Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2017, 10, 2050–2060. [Google Scholar] [CrossRef]
- Allende, R.; Webb, J.G.; Munoz-Garcia, A.J.; de Jaegere, P.; Tamburino, C.; Dager, A.E.; Cheema, A.; Serra, V.; Amat-Santos, I.; Velianou, J.L.; et al. Advanced chronic kidney disease in patients undergoing transcatheter aortic valve implantation: Insights on clinical outcomes and prognostic markers from a large cohort of patients. Eur. Heart J. 2014, 35, 2685–2696. [Google Scholar] [CrossRef]
- Gracia, E.; Wang, T.Y.; Callahan, S.; Bilfinger, T.; Tannous, H.; Pyo, R.; Kort, S.; Skopicki, H.; Weinstein, J.; Patel, N.; et al. Impact of Severity of Chronic Kidney Disease on Management and Outcomes Following Transcatheter Aortic Valve Replacement With Newer-Generation Transcatheter Valves. J. Invasive Cardiol. 2020, 32, 25–29. [Google Scholar]
- Matsumoto, S.; Ohno, Y.; Miyamoto, J.; Ikari, Y.; Tada, N.; Naganuma, T.; Yamawaki, M.; Yamanaka, F.; Shirai, S.; Mizutani, K.; et al. Impact of diabetes mellitus on outcome after transcatheter aortic valve replacement: Identifying high-risk diabetic population from the OCEAN-TAVI registry. Catheter. Cardiovasc. Interv. 2021, 98, E1058–E1065. [Google Scholar] [CrossRef] [PubMed]
- Abramowitz, Y.; Vemulapalli, S.; Chakravarty, T.; Li, Z.; Kapadia, S.; Holmes, D.; Matsouaka, R.A.; Wang, A.; Cheng, W.; Forrester, J.S.; et al. Clinical Impact of Diabetes Mellitus on Outcomes After Transcatheter Aortic Valve Replacement: Insights From the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Therapy Registry. Circ. Cardiovasc. Interv. 2017, 10, e005417. [Google Scholar] [CrossRef]
- Chorin, E.; Finkelstein, A.; Banai, S.; Aviram, G.; Barkagan, M.; Barak, L.; Keren, G.; Steinvil, A. Impact of Diabetes Mellitus and Hemoglobin A1C on Outcome After Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2015, 116, 1898–1903. [Google Scholar] [CrossRef]
- Muratori, M.; Fusini, L.; Tamborini, G.; Ali, S.G.; Gripari, P.; Fabbiocchi, F.; Salvi, L.; Trabattoni, P.; Roberto, M.; Agrifoglio, M.; et al. Mitral valve regurgitation in patients undergoing TAVI: Impact of severity and etiology on clinical outcome. Int. J. Cardiol. 2020, 299, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Kiramijyan, S.; Magalhaes, M.A.; Koifman, E.; Didier, R.; Escarcega, R.O.; Minha, S.; Baker, N.C.; Negi, S.I.; Torguson, R.; Gai, J.; et al. Impact of baseline mitral regurgitation on short- and long-term outcomes following transcatheter aortic valve replacement. Am. Heart J. 2016, 178, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Omar, S.; Aneni, E.; Escolar, E.; Mihos, C.G.; Xydas, S.; LaPietra, A.; Beohar, N.; Arenas, I.A. Tricuspid regurgitation and in-hospital outcomes after transcatheter aortic valve replacement in high-risk patients. J. Thorac. Dis. 2020, 12, 2963–2970. [Google Scholar] [CrossRef]
- Amat-Santos, I.J.; Castrodeza, J.; Nombela-Franco, L.; Muñoz-García, A.J.; Gutiérrez-Ibanes, E.; Hernández, J.M.d.l.T.; Córdoba-Soriano, J.G.; Jiménez-Quevedo, P.; Hernández-García, J.M.; González-Mansilla, A.; et al. Tricuspid but not Mitral Regurgitation Determines Mortality After TAVI in Patients With Nonsevere Mitral Regurgitation. Rev. Esp. Cardiol. 2018, 71, 357–364. [Google Scholar] [CrossRef]
- Alushi, B.; Beckhoff, F.; Leistner, D.; Franz, M.; Reinthaler, M.; Stähli, B.E.; Morguet, A.; Figulla, H.R.; Doenst, T.; Maisano, F.; et al. Pulmonary Hypertension in Patients With Severe Aortic Stenosis: Prognostic Impact After Transcatheter Aortic Valve Replacement: Pulmonary Hypertension in Patients Undergoing TAVR. JACC Cardiovasc. Imaging 2019, 12, 591–601. [Google Scholar] [CrossRef]
- Puehler, T.; Pommert, N.S.; Freitag-Wolf, S.; Seoudy, H.; Ernst, M.; Haneya, A.; Sathananthan, J.; Sellers, S.L.; Meier, D.; Schöttler, J.; et al. Tricuspid Regurgitation and TAVR: Outcomes, Risk Factors and Biomarkers. J. Clin. Med. 2024, 13, 1474. [Google Scholar] [CrossRef]
- Ito, S.; Pislaru, S.V.; Soo, W.M.; Huang, R.; Greason, K.L.; Mathew, V.; Sandhu, G.S.; Eleid, M.F.; Suri, R.M.; Oh, J.K.; et al. Impact of right ventricular size and function on survival following transcatheter aortic valve replacement. Int. J. Cardiol. 2016, 221, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Grevious, S.N.; Fernandes, M.F.; Annor, A.K.; Ibrahim, M.; Croix, G.R.S.; de Marchena, E.; Cohen, M.G.; Alfonso, C.E. Prognostic Assessment of Right Ventricular Systolic Dysfunction on Post-Transcatheter Aortic Valve Replacement Short-Term Outcomes: Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2020, 9, e014463. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.; Liu, X.; Yu, L.; Sun, Y.; Jaiswal, S.; Zhu, Q.; Chen, H.; He, Y.; Wang, L.; Ren, K.; et al. Impact of tricuspid regurgitation and right ventricular dysfunction on outcomes after transcatheter aortic valve replacement: A systematic review and meta-analysis. Clin. Cardiol. 2019, 42, 206–212. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Stage | Stage 0 | Stage 1 | Stage 2 | Stage 3 | p Value |
|---|---|---|---|---|---|
| Age, years | 81.8 ± 6.4 | 81.7 ± 5.8 | 82.2 ± 5.5 | 83.3 ± 5.6 | 0.301 |
| BMI (kg/m2) | 27.9 ± 4.7 | 28.0 ± 5.9 | 28.7 ± 7.1 | 28.0 ± 5.2 | 0.780 |
| HTA (%) | 24.0 | 42.6 | 17.3 | 16.0 | 0.836 |
| DM (%) | 27.3 | 41.7 | 16.6 | 14.4 | 0.738 |
| DLP (%) | 25.4 | 39.6 | 17.1 | 17.9 | 0.364 |
| CKD (%) | 17.6 | 37.2 | 21.6 | 23.5 | 0.017 |
| CAD (%) | 22.6 | 45.3 | 16.8 | 15.3 | 0.900 |
| Logistic EuroSCORE | 11.9 ± 7.2 | 17.5 ± 12.7 | 19.0 ± 14.9 | 26.4 ± 15.0 | <0.001 |
| LVEF % | 64.1 ± 5.1 | 55.4 ± 9.4 | 54.5 ± 13.2 | 53.1 ± 12.5 | <0.001 |
| LVEDV, mL/m2 | 51.3 ± 13.3 | 53.3 ± 22.9 | 58.0 ± 18.9 | 62.1 ± 24.3 | 0.003 |
| LVGLS, % | −17.8 ± 2.8 | −15.4 ± 4.2 | −15.3 ± 4.6 | −15.1 ± 42 | <0.001 |
| LV mass, g/m2 | 116.2 ± 25.0 | 127.2 ± 28.9 | 132.6 ± 34.5 | 140.7 ± 38.9 | <0.001 |
| LAVI, mL/m2 | 42.7 ± 16.3 | 46.1 ± 16.7 | 57.5 ± 20.4 | 66.5 ± 76.6 | <0.001 |
| E/e’ ratio | 13.8 ± 4.7 | 14.7 ± 6.3 | 17.3 ± 6.1 | 19.5 ± 6.5 | <0.001 |
| PASP, mmHg | 31.0 ± 10.3 | 31.9 ± 10.7 | 37.5 ± 12.5 | 57.2 ± 14.3 | <0.001 |
| TAPSE, mm | 22.5 ± 4.2 | 20.9 ± 4.0 | 20.6 ± 4.1 | 15.8 ± 3.8 | <0.001 |
| RVAc | 0.81 ± 0.3 | 0.74 ± 0.3 | 0.69 ± 0.3 | 0.28 ± 0.5 | <0.001 |
| Stage 1-Year FU | Stage 0 | Stage 1 | Stage 2 | Stage 3 | p Value |
|---|---|---|---|---|---|
| LVEF % | 61.4 ± 5.5 | 58.2 ± 9.3 | 56.6 ± 9.0 | 57.7 ± 8.9 | <0.001 |
| LVEDV, mL/m2 | 49.6 ± 14.9 | 50.8 ± 15.5 | 52.1 ± 21.1 | 56.0 ± 21.7 | 0.223 |
| LV mass, gr/m2 | 110.7 ± 31.8 | 111.4 ± 31.0 | 113.8 ± 26.6 | 120.6 ± 26.1 | 0.307 |
| LVGLS, % | −17.8 ± 2.8 | −15.4 ± 4.2 | −15.3 ± 4.6 | −15.1 ± 42 | <0.001 |
| LAVI, mL/m2 | 41.4 ± 16.1 | 43.9 ± 17.8 | 55.3 ± 21.7 | 71.0 ± 74.4 | <0.001 |
| E/e’ ratio | 13.8 ± 5.1 | 14.6 ± 5.5 | 15.8 ± 5.4 | 15.9 ± 4.7 | 0.284 |
| PASP, mmHg | 26.9 ± 7.4 | 28.5 ± 11.3 | 31.5 ± 13.3 | 37.3 ± 13.6 | <0.001 |
| TAPSE, mm | 21.8 ± 4.1 | 20.4 ± 3.9 | 20.7 ± 4.6 | 18.4 ± 4.5 | <0.001 |
| RVAc | 0.87 ± 0.3 | 0.81 ± 0.3 | 0.77 ± 0.3 | 0.58 ± 0.3 | <0.001 |
| Univariable Logistic Regression Analysis | Multivariable Logistic Regression Analysis | |||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p Value | Odds Ratio (95% CI) | p Value | |
| HTA | 1.49 (0.76–2.93) | 0.236 | ||
| DM | 1.55 (1.14–2.17) | 0.014 | 1.38 (1.09–2.48) | 0.047 |
| DLP | 1.27 (0.74–2.17) | 0.374 | ||
| CKD | 2.14 (1.20–3.79) | 0.010 | 2.19 (1.15–4.20) | 0.024 |
| CAD | 1.58 (0.93–2.67) | 0.092 | ||
| EuroSCORE | 1.00 (0.99–1.02) | 0.599 | ||
| LVEF | 1.02 (1.00–1.06) | 0.029 | ||
| GLS | 0.92 (0.86–0.98) | 0.015 | ||
| MR ≥ 2 | 1.83 (1.01–3.32) | 0.047 | 3.24 (1.07–9.87) | <0.001 |
| TR ≥ 2 | 1.73 (1.36–3.18) | 0.038 | 2.33 (1.01–3.99) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Islas, F.; O’Neill-González, P.; Jiménez-Quevedo, P.; Nombela-Franco, L.; Gil-Abizanda, S.; Mahía-Casado, P.; Rivadeneira-Ruiz, M.; Pozo-Osinalde, E.; Carbone, A.; Olmos, C. Aortic Stenosis and the Evolution of Cardiac Damage after Transcatheter Aortic Valve Replacement. J. Clin. Med. 2024, 13, 3539. https://doi.org/10.3390/jcm13123539
Islas F, O’Neill-González P, Jiménez-Quevedo P, Nombela-Franco L, Gil-Abizanda S, Mahía-Casado P, Rivadeneira-Ruiz M, Pozo-Osinalde E, Carbone A, Olmos C. Aortic Stenosis and the Evolution of Cardiac Damage after Transcatheter Aortic Valve Replacement. Journal of Clinical Medicine. 2024; 13(12):3539. https://doi.org/10.3390/jcm13123539
Chicago/Turabian StyleIslas, Fabián, Patrick O’Neill-González, Pilar Jiménez-Quevedo, Luis Nombela-Franco, Sandra Gil-Abizanda, Patricia Mahía-Casado, María Rivadeneira-Ruiz, Eduardo Pozo-Osinalde, Andreina Carbone, and Carmen Olmos. 2024. "Aortic Stenosis and the Evolution of Cardiac Damage after Transcatheter Aortic Valve Replacement" Journal of Clinical Medicine 13, no. 12: 3539. https://doi.org/10.3390/jcm13123539
APA StyleIslas, F., O’Neill-González, P., Jiménez-Quevedo, P., Nombela-Franco, L., Gil-Abizanda, S., Mahía-Casado, P., Rivadeneira-Ruiz, M., Pozo-Osinalde, E., Carbone, A., & Olmos, C. (2024). Aortic Stenosis and the Evolution of Cardiac Damage after Transcatheter Aortic Valve Replacement. Journal of Clinical Medicine, 13(12), 3539. https://doi.org/10.3390/jcm13123539