The Impact of the Seasonal and Geographical Distribution of Tuberculosis in Sicily: A 6-Year Retrospective Study (2018–2023)

 ,
,  , , ,
, , ,  ,
,  ,
,  and
and 
Abstract
1. Introduction
Objective
2. Materials and Methods
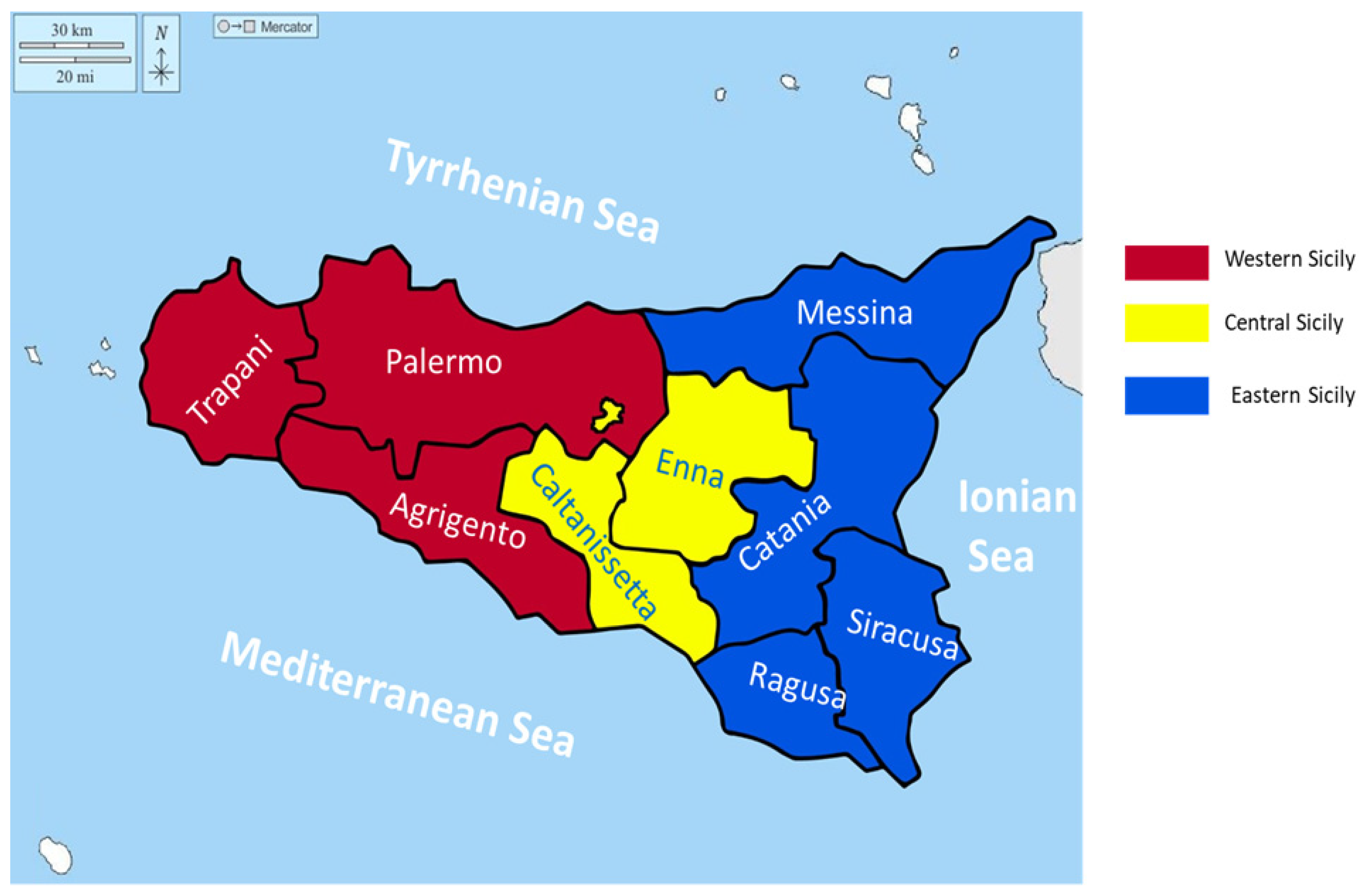
2.1. Geographical Sicilian Area
2.2. Seasonal and Geographical Area Variables
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Control: WHO Report 2022; World Health Organization: Geneva, Switzerland, 2022; Available online: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2022 (accessed on 19 December 2023).
- European Centre for Disease Prevention and Control, WHO Regional Office for Europe. Tuberculosis Surveillance and Monitoring in Europe 2022–2020 Data. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/Tuberculosis-surveillance-monitoring-europe-2022_0.pdf (accessed on 19 December 2023).
- Combating the Global TB Epidemic. U.S. Department of Health & Human Services. Available online: https://www.cdc.gov/globalhivtb/who-we-are/about-us/globaltb/globaltb.html (accessed on 19 December 2023).
- Tuberculosis: Basic TB Facts. Center for Disease Control and Prevention—U.S. Department of Health & Human Services. Available online: http://www.cdc.gov/tb/topic/basics/risk.htm (accessed on 19 December 2023).
- Singh, H.; Rupal, A.; Al Omari, O.; Jani, C.; Ahmed, A.; Khaliqdina, S.; Walker, A.; Shalhoub, J.; Thomson, C.; Marshall, D.C.; et al. Trends in pulmonary tuberculosis mortality between 1985 and 2018: An observational analysis. BMC Pulm. Med. 2023, 23, 184. [Google Scholar] [CrossRef] [PubMed]
- Stop TB Partnership. Global Plan to End TB, 2023–2030 [Internet]. 2022. Available online: https://www.stoptb.org/global-plan-to-end-tb/global-plan-to-end-tb-2023-2030 (accessed on 20 December 2023).
- Coker, R.J.; Atun, R.A.; McKee, M. Health-care system frailties and public health control of communicable disease on the European Union’s new eastern border. Lancet 2004, 363, 1389–1392. [Google Scholar] [CrossRef] [PubMed]
- Pontali, E.; Raviglione, M.C.; Migliori, G.B.; the writing group members of the Global TB Network Clinical Trials Committee. Regimens to treat multidrug-resistant tuberculosis: Past, present, and future perspectives. Eur. Respir. Rev. 2019, 28, 190035. [Google Scholar] [CrossRef] [PubMed]
- Nalunjogi, J.; Mucching-Toscano, S.; Sibomana, J.P.; Centis, R.; D’Ambrosio, L.; Alffenaar, J.-W.; Denholm, J.; Blanc, F.-X.; Borisov, S.; Danila, E.; et al. Impact of COVID-19 on diagnosis of TB, MDR-TB and on mortality in 11 countries in Europe, Northern America, and Australia. A Global Tuberculosis Network study. Int. J. Infect. Dis. 2023, 130, S25–S29. [Google Scholar] [CrossRef]
- Zhou, G.; Luo, S.; He, J.; Chen, N.; Zhang, Y.; Cai, S.; Guo, X.; Chen, H.; Song, C. Effectiveness and safety of tuberculosis preventive treatment for contacts of patients with multidrug-resistant tuberculosis: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2024, 30, 189–196. [Google Scholar] [CrossRef] [PubMed]
- McQuaid, C.F.; Vassall, A.; Cohen, T.; Fiekert, K.; White, R.G. The impact of COVID-19 on TB: A review of the data. Int. J. Tuberc. Lung Dis. 2021, 25, 436–446. [Google Scholar] [CrossRef] [PubMed]
- Migliori, G.B.; Thong, P.M.; Alffenaar, J.-W.; Denholm, J.; Tadolini, M.; Alyaquobi, F.; Blanc, F.-X.; Buonsenso, D.; Cho, J.-G.; Codecasa, L.R.; et al. Gauging the impact of the COVID-19 pandemic on tuberculosis services: A global study. Eur. Respir. J. 2021, 58, 2101786. [Google Scholar] [CrossRef]
- Ministry of Health of 15 December 1990. Available online: https://www.epicentro.iss.it/infettive/pdf/DM_151290.pdf (accessed on 18 December 2023).
- Guidelines for the Control of Tuberculosis (G.U. n°40, 18 febbraio 1999). Available online: https://www.salute.gov.it/imgs/C_17_pubblicazioni_615_allegato.pdf (accessed on 18 December 2023).
- Government Decree July 29, 1998 (G.U. n°200, August 28, 1998). Available online: https://www.gazzettaufficiale.it/gazzetta/serie_generale/caricaDettaglio?dataPubblicazioneGazzetta=1998-08-28&numeroGazzetta=200 (accessed on 5 January 2024).
- Ministry of Health. Guidelines for the Control of Tuberculosis Disease (G.U. n°40, February 18, 1999). Available online: https://www.gazzettaufficiale.it/gazzetta/serie_generale/caricaDettaglio?dataPubblicazioneGazzetta=1999-02-18&numeroGazzetta=40 (accessed on 18 December 2023).
- Infectious Diseases Information System, Simi—epiCentro.iss.it. Available online: https://www.epicentro.iss.it/tubercolosi/ (accessed on 18 December 2023).
- Decree of 7 March 2022 of the Ministry of Health published on Gazzetta Ufficiale Serie Generale n. 82 del 07/04/2022. Review of the Infectious Diseases Reporting System (PREMAL). Available online: https://www.regione.sicilia.it/sites/default/files/2022-02/Assessorato%20Salute%20Regione%20Siciliana%20%20Piano%20Regionale%20Prevenzione%202020-2025.pdf (accessed on 19 December 2023).
- Sergi, C.; Serra, N.; Colomba, C.; Ayanlade, S.; Di Carlo, P. Tuberculosis evolution and climate change: How much work is ahead? Public Health 2019, 15, 350–354. [Google Scholar] [CrossRef]
- Gelaw, Y.; Yu, W.; Magalhães, R.S.; Assefa, Y.; Williams, G. Effect of Temperature and Altitude Difference on Tuberculosis Notification: A Systematic Review. J. Glob. Infect. Dis. 2019, 11, 63–68. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Xu, M.; Li, Y.; Liu, B.; Chen, R.; Sheng, L.; Yan, S.; Chen, H.; Hou, J.; Yuan, L.; Ke, L.; et al. Temperature and humidity associated with increases in tuberculosis notifications: A time-series study in Hong Kong. Epidemiol. Infect. 2020, 149, e8. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Xu, M.; Hu, P.; Chen, R.; Liu, B.; Chen, H.; Hou, J.; Ke, L.; Huang, J.; Ren, H.; Hu, H. Association of long-term exposure to ambient air pollution with the number of tuberculosis cases notified: A time-series study in Hong Kong. Environ. Sci. Pollut. Res. 2021, 29, 21621–21633. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, R.; Thiruvengadam, K.; Jayabal, L.; Selvaraju, S.; Watson, B.; Malaisamy, M.; Nagarajan, K.; Tripathy, S.P.; Chinnaiyan, P.; Chandrasekaran, P. An influence of dew point temperature on the occurrence of Mycobacterium tuberculosis disease in Chennai, India. Sci. Rep. 2022, 12, 6147. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, F.M.d.C.; Martins, E.d.S.; Pedrosa, D.M.A.S.; Evangelista, M.D.S.N. Relationship between climatic factors and air quality with tuberculosis in the Federal District, Brazil, 2003–2012. Braz. J. Infect. Dis. 2017, 21, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Mora, C.; McKenzie, T.; Gaw, I.M.; Dean, J.M.; von Hammerstein, H.; Knudson, T.A.; Setter, R.O.; Smith, C.Z.; Webster, K.M.; Patz, J.A.; et al. Over half of known human pathogenic diseases can be aggravated by climate change. Nat. Clim. Chang. 2022, 12, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Liao, Z.; Zhang, X.; Zhang, Y.; Peng, D. Seasonality and Trend Forecasting of Tuberculosis Incidence in Chongqing, China. Interdiscip. Sci. Comput. Life Sci. 2019, 11, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Azeez, A.; Obaromi, D.; Odeyemi, A.; Ndege, J.; Muntabayi, R. Seasonality and Trend Forecasting of Tuberculosis Prevalence Data in Eastern Cape, South Africa, Using a Hybrid Model. Int. J. Environ. Res. Public Health 2016, 13, 757. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Guida, C.; Gargiulo, C.; Papa, R.; Carpentieri, G. Vulnerability and Exposure of Mediterranean Coastal Cities to Climate Change-Related Phenomena. Environ. Sci. Proc. 2022, 21, 79. [Google Scholar] [CrossRef]
- Commission Decision of 28 April 2008 (2008/426/EC:) Amending Decision 2002/253/EC Laying down Case Definitions for Reporting Communicable Diseases to the Community Network under Decision No 2119/98/EC of the European Parliament and of the Council (Notified under Document Number C(2008) 1589) (Text with EEA Relevance). OJ L 159 18.06.2008, p. 46. Available online: http://data.europa.eu/eli/dec/2008/426/oj (accessed on 21 December 2023).
- Diagnostic Standards and Classification of Tuberculosis in Adults and Children. This official statement of the American Thoracic Society and the Centers for Disease Control and Prevention was adopted by the ATS Board of Directors, July 1999. This statement was endorsed by the Council of the Infectious Disease Society of America, September 1999. Am. J. Respir. Crit. Care Med. 2000, 161 Pt 1, 1376–1395. [Google Scholar] [CrossRef] [PubMed]
- Quattrocchi, A.; Barchitta, M.; Nobile, C.G.A.; Prato, R.; Sotgiu, G.; Casuccio, A.; Vitale, F.; Agodi, A. Determinants of patient and health system delay among Italian and foreign-born patients with pulmonary tuberculosis: A multicentre cross-sectional study. BMJ Open 2018, 8, e019673. [Google Scholar] [CrossRef]
- Surveillance Atlas of Infectious Diseases (ECDC). Available online: https://atlas.ecdc.europa.eu/public/index.aspx (accessed on 20 December 2023).
- Ministry of Health. Tuberculosis cases in Italy—Period 2009–2021. Available online: https://www.salute.gov.it/imgs/C_17_pubblicazioni_3387_allegato.pdf (accessed on 20 December 2023).
- Demographic Trend of the Population Resident in Sicily from 2001 to 2022. Graphs and Statistics Based on ISTAT Data as of 31 December of Each Year. Available online: https://www.tuttitalia.it/sicilia/statistiche/popolazione-andamento-demografico/ (accessed on 20 December 2023).
- Pipitò, L.; Colomba, C.; Mancuso, A.; Catania, B.; Cuccia, A.; Sergio, M.; Iaria, C.; Cascio, A. Hospitalizations for tuberculosis in Sicily over the years 2009–2021: Clinical features, comorbidities, and predictors of mortality. J. Infect. Public Health 2023, 16, 1518–1524. [Google Scholar] [CrossRef] [PubMed]
- Lewinsohn, D.M.; Leonard, M.K.; LoBue, P.A.; Cohn, D.L.; Daley, C.L.; Desmond, E.; Keane, J.; Lewinsohn, D.A.; Loeffler, A.M.; Mazurek, G.H.; et al. Official American Thoracic Society/Infectious Diseases Society of America/Centers for Disease Control and Prevention Clinical Practice Guidelines: Diagnosis of Tuberculosis in Adults and Children. Clin. Infect. Dis. 2016, 64, e1–e33. [Google Scholar] [CrossRef] [PubMed]
- Bruno, F.; Vitale, F.; La Russa, F.; Reale, S.; Späth, G.F.; Oliveri, E.; Gargano, V.; Valenza, V.; Facciponte, F.; Giardina, S.; et al. Retrospective Analysis of Leishmaniasis in Sicily (Italy) from 2013 to 2021: One-Health Impact and Future Control Strategies. Microorganisms 2022, 10, 1704. [Google Scholar] [CrossRef] [PubMed]
- Horton, K.C.; MacPherson, P.; Houben, R.M.G.J.; White, R.G.; Corbett, E.L. Sex differences in tuberculosis burden and notifcations in low- and middle-income countries: A systematic review and meta-analysis. PLoS Med. 2016, 13, e1002119. [Google Scholar] [CrossRef] [PubMed]
- Rhines, A.S. The role of sex differences in the prevalence and transmission of tuberculosis. Tuberculosis 2013, 93, 104–107. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization: Smoking and Tuberculosis: A Dangerous Combination. Published 22 March 2018. Available online: https://www.who.int/europe/news/item/22-03-2018-smoking-and-tuberculosis-a-dangerous-combination#:~:text=Smoking%20increases%20the%20risk%20of,to%20treatment%20of%20the%20disease (accessed on 30 May 2024).
- Donfrancesco, C.; Buttari, B.; Marcozzi, B.; Sieri, S.; Di Lonardo, A.; Noce, C.L.; Profumo, E.; Vespasiano, F.; Agnoli, C.; Vannucchi, S.; et al. Nutrition, Physical Activity and Smoking Habit in the Italian General Adult Population: CUORE Project Health Examination Survey 2018–2019. Healthcare 2024, 12, 475. [Google Scholar] [CrossRef] [PubMed]
- Veldhuizen, S.; Zawertailo, L.; Ivanova, A.; Hussain, S.; Selby, P. Seasonal Variation in Demand for Smoking Cessation Treatment and Clinical Outcomes. Nicotine Tob. Res. 2020, 23, 976–982. [Google Scholar] [CrossRef] [PubMed]
- Arku, R.E.; Adamkiewicz, G.; Vallarino, J.; Spengler, J.D.; Levy, D.E. Seasonal variability in environmental tobacco smoke exposure in public housing developments. Indoor Air 2014, 25, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Shaweno, D.; Horton, K.C.; Hayes, R.J.; Dodd, P.J. Assortative social mixing and sex disparities in tuberculosis burden. Sci. Rep. 2021, 11, 7530. [Google Scholar] [CrossRef]
- Rossitto, S.; Gagliardi, M.C.; Ortona, E. Tuberculosis control in Italy and gender phthisiology. Ital. J. Gend.-Specif. Med. 2017, 3, 29–35. [Google Scholar] [CrossRef]
- Beiranvand, R.; Karimi, A.; Delpisheh, A.; Sayehmiri, K.; Soleimani, S.; Ghalavandi, S. Correlation Assessment of Climate and Geographic Distribution of Tuberculosis Using Geographical Information System (GIS). Iran. J. Public Health 2016, 45, 86–93. [Google Scholar] [PubMed] [PubMed Central]
- Elliott, P.; Cuzick, J.; English, D.; Stern, R. Geographical and Environmental Epidemiology: Methods for Small Area Studies, 1st ed.; Oxford Uni Press: Oxford, UK, 1996. [Google Scholar] [CrossRef]
- Rezaeian, M.; Dunn, G.; Leger, S.S.; Appleby, L. Geographical epidemiology, spatial analysis & geographical information system: A multidisciplinary glossary. J. Epidemiol. Community Health 2007, 61, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Martellucci, C.A.; Sah, R.; Rabaan, A.A.; Dhama, K.; Casalone, C.; Arteaga-Livias, K.; Sawano, T.; Ozaki, A.; Bhandari, D.; Higuchi, A.; et al. Changes in the spatial distribution of COVID-19 incidence in Italy using GIS-based maps. Ann. Clin. Microbiol. Antimicrob. 2020, 19, 30. [Google Scholar] [CrossRef] [PubMed]
- Teibo, T.K.A.; Andrade, R.L.d.P.; Rosa, R.J.; Tavares, R.B.V.; Berra, T.Z.; Arcêncio, R.A. Geo-spatial high-risk clusters of Tuberculosis in the global general population: A systematic review. BMC Public Heal. 2023, 23, 1586. [Google Scholar] [CrossRef] [PubMed]
- Pusch, L.-M.; Funke, N.; Wiesmüller, G.; Kistemann, T.; Neuhann, F. Spatio-temporal distribution of tuberculosis in an urban setting in Germany [Räumlich-zeitliche Analyse der Tuberkuloseverteilung in der Stadt Köln 2006–2015—Eine 10-Jahres-Analyse]. Pneumologie 2019, 73, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Classen, C.N.; Warren, R.; Richardson, M.; Hauman, J.H.; Gie, R.P.; Ellis, J.H.P.; van Helden, P.D.; Beyers, N. Impact of social interactions in the community on the transmission of tuberculosis in a high incidence area. Thorax 1999, 54, 136–140. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Duarte, R.; Lönnroth, K.; Carvalho, C.; Lima, F.; Carvalho, A.; Muñoz-Torrico, M.; Centis, R. Tuberculosis, social determinants and co-morbidities (including HIV). Pulmonology 2018, 24, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Clayson, C. Seasonal trends in pulmonary tuberculosis. Br. J. Tuberc. 1939, 33, 187–196. [Google Scholar] [CrossRef]
- Douglas, A.S.; Strachan, D.P.; Maxwell, J.D. Seasonality of tuberculosis: The reverse of other respiratory diseases in the UK. Thorax 1996, 51, 944–946. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Butt, M.F.; Younis, S.; Wu, Z.; Hadi, S.H.; Latif, A.; Martineau, A.R. The relationship between seasonality, latitude and tuberculosis notifications in Pakistan. BMC Infect. Dis. 2021, 21, 210. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fares, A. Seasonality of Tuberculosis. J. Glob. Infect. Dis. 2011, 3, 46–55. [Google Scholar] [CrossRef]
- Sumi, A.; Kobayashi, N. Time-series analysis of geographically specific monthly number of newly registered cases of active tuberculosis in Japan. PLoS ONE 2019, 14, e0213856. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Reichert, T.A.; Simonsen, L.; Sharma, A.; Pardo, S.A.; Fedson, D.S.; Miller, M.A. Influenza and the Winter Increase in Mortality in the United States, 1959–1999. Am. J. Epidemiol. 2004, 160, 492–502. [Google Scholar] [CrossRef] [PubMed]
- Manabe, T.; Takasaki, J.; Kudo, K. Seasonality of newly notified pulmonary tuberculosis in Japan, 2007–2015. BMC Infect. Dis. 2019, 19, 497. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sicily Region Report Year 2022. Tourist Movements in the Region—Provincial Data. Available online: https://www.regione.sicilia.it/sites/default/files/2023-07/prov_mensili_21-22_0.xls (accessed on 17 May 2023).
- ISTAT Report, The Permanent Census of the Population in Sicily. 16 March 2022. Available online: https://www.istat.it/it/files//2022/03/Il-Censimento-della-popolazione-in-Sicilia_focus.pdf (accessed on 17 May 2023).
- Tedijanto, C.; Hermans, S.; Cobelens, F.; Wood, R.; Andrews, J.R. Drivers of seasonal variation in tuberculosis incidence: Insights from a systematic review and mathematical model. Epidemiology 2018, 29, 857–866. [Google Scholar] [CrossRef] [PubMed]
- Perrino, C.; Gilardoni, S.; Landi, T.; Abita, A.; Ferrara, I.; Oliverio, S.; Busetto, M.; Calzolari, F.; Catrambone, M.; Cristofanelli, P.; et al. Air Quality Characterization at Three Industrial Areas in Southern Italy. Front. Environ. Sci. 2020, 7, 196. [Google Scholar] [CrossRef]
- Tran, H.M.; Tsai, F.-J.; Lee, Y.-L.; Chang, J.-H.; Chang, L.-T.; Chang, T.-Y.; Chung, K.F.; Kuo, H.-P.; Lee, K.-Y.; Chuang, K.-J.; et al. The impact of air pollution on respiratory diseases in an era of climate change: A review of the current evidence. Sci. Total. Environ. 2023, 898, 166340. [Google Scholar] [CrossRef] [PubMed]
- Maharjan, B.; Gopali, R.S.; Zhang, Y. A scoping review on climate change and tuberculosis. Int. J. Biometeorol. 2021, 65, 1579–1595. [Google Scholar] [CrossRef] [PubMed]
- Giammanco, S.; Bonfanti, P.; Neri, M. Radon on Mt. Etna (Italy): A useful tracer of geodynamic processes and a potential health hazard to populations. Front. Earth Sci. 2023, 11, 1176051. [Google Scholar] [CrossRef]
- Sahoo, S.; Tiwari, D.K.; Panda, D.; Kundu, B. Eruption cycles of Mount Etna triggered by seasonal climatic rainfall. J. Geodyn. 2022, 149, 101896. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | % (n) |
|---|---|
| Italian patients with active TB | 467 |
| Age at admission | |
| Mean (SD) | Total: 49.5 (22.7); M:52.5 (21.7); F: 44.0 (23.6) |
| Median (IQR) | Total: 52 (31.25–69); M: 55 (37–71); F:44 (25–63) |
| Gender | |
| Male | 65.3% (305) |
| Female | 34.7% (162) |
| Sicilian geographical area | |
| Eastern Sicily * | 52.2% (244) |
| Western Sicily # | 42.6% (199) |
| Central Sicily § | 5.2% (24) |
| Season | |
| Autumn | 28.9% (135) |
| Summer | 26.3% (123) |
| Winter | 25.1% (117) |
| Spring | 19.7% (92) |
| Summer (Su) % (n) | Autumn (Au) % (n) | Winter (Wi) % (n) | Spring (Sp) % (n) | Analysis across Seasons p-Value (Test) | |
|---|---|---|---|---|---|
| Patients (n = 467) | 26.3% | 28.9% | 25.1% | 19.7% | p = 0.0378 * (Cgf) |
| (123) | (135) | (117) | (92) | Au: 28.9% **, p = 0.0449 (Z) | |
| Sp: 19.7% ***, p = 0.0105 (Z) | |||||
| Age at admission | |||||
| Mean (SD) | 53.7(20.1) | 49.7(23.4) | 47.1(23.1) | 46.8 (24.0) | |
| Median (IQR) | 57 (40–71) | 52(28.5–70.75) | 50 (27–66.5) | 50(25–66) | p = 0.10 (KW) |
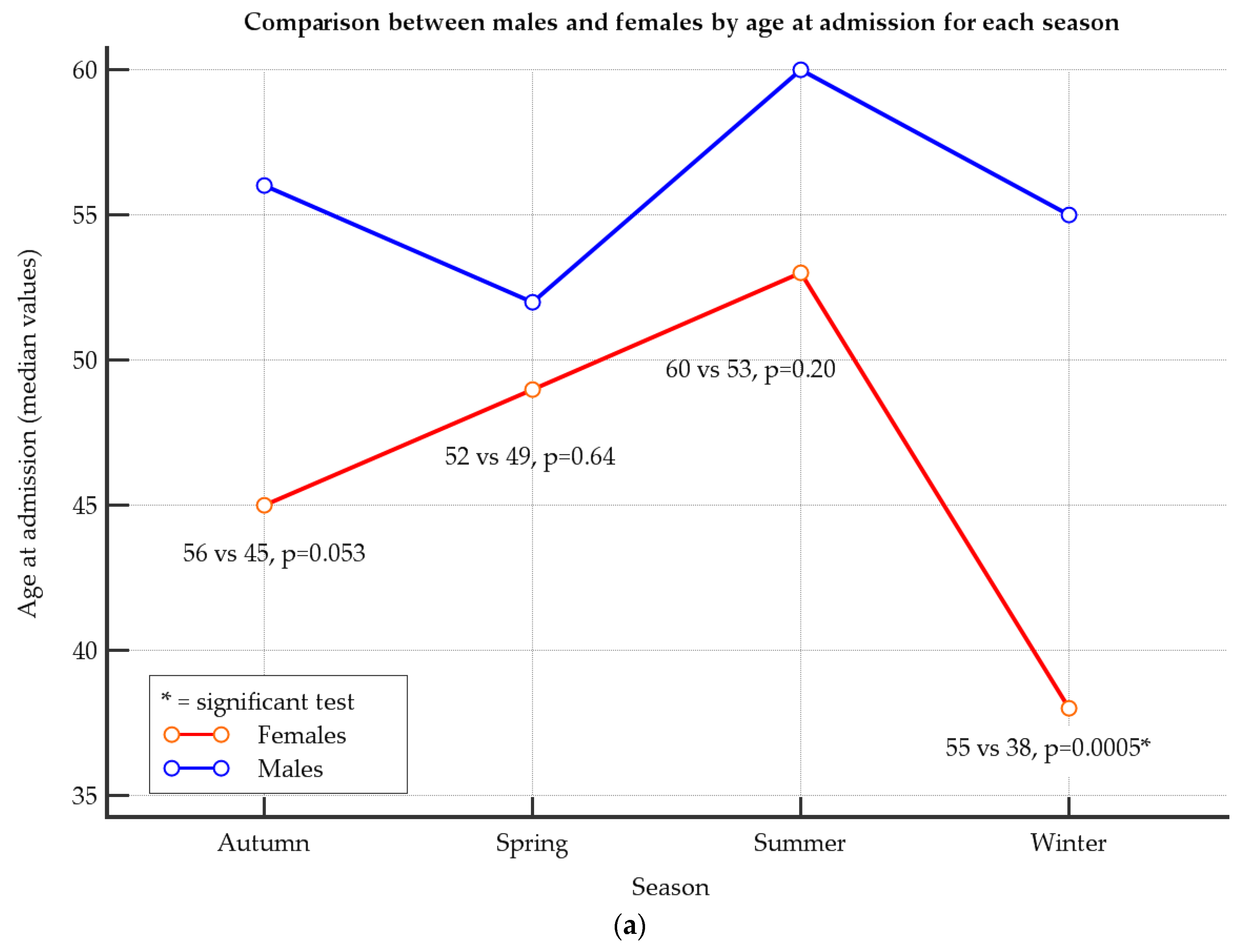
| Age at admission for males | |||||
| Mean (SD) | 55.4 (19.3) | 52.7 (23.2) | 52.1 (21.4) | 47.8 (23.2) | |
| Median (IQR) | 60.0 (41.5–71.8) | 56.0 (36.5–74.0) | 55.0 (39.0–68.5) | 52.0 (27.3–65.3) | p = 0.28 (KW) |
| Age at admission for females | |||||
| Mean (SD) | 49.7 (21.7) | 44.7 (23.1) | 36.2 (23.3) | 45.4 (25.2) | |
| Median (IQR) | 53.0 (30.5–67.5) | 45.0 (26.0–63.0) | 38.0 (16.0–54.0) | 49.0 (25.0–70.8) | p = 0.17 (KW) |
| Gender | p = 0.19 (C) | ||||
| Male | 70.7% (87) ** | 63.0% (85) ** | 68.4% (80) ** | 57.6% (53) | |
| Female | 29.3% (36) | 37.0% (50) | 31.6% (37) | 42.4% (39) | |
| p < 0.0001 * (F) | |||||
| Geographical area | |||||
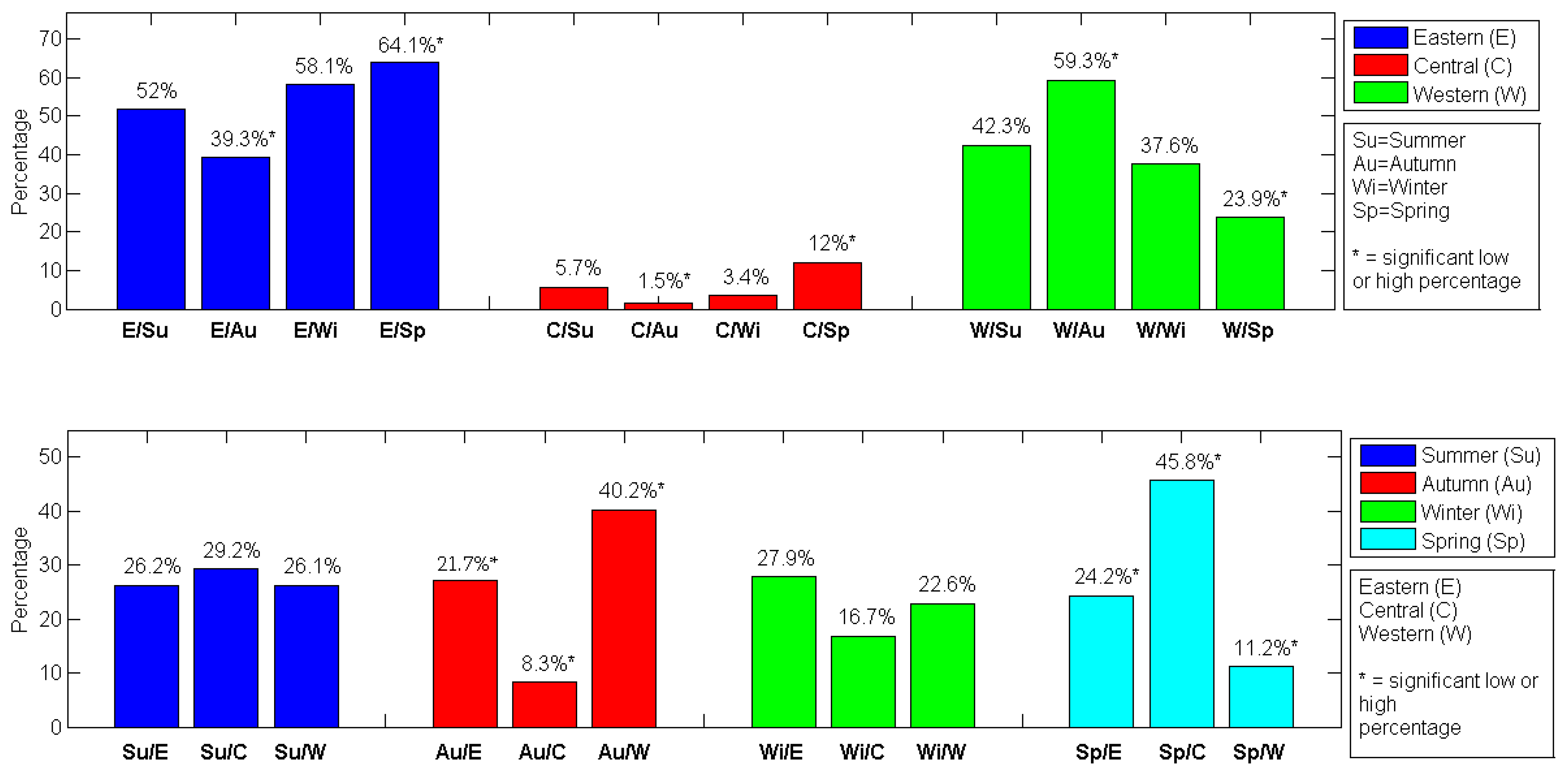
| Eastern Sicily | 52.0% (64) ** | 39.3% (53) | 58.1% (68) ** | 64.1% (59) ** | Au–Western: 59.3% **, p < 0.0001 (Z) |
| Central Sicily | 5.7% (7) *** | 1.5% (2) *** | 3.4% (4) *** | 12.0% (11) *** | Sp–Western: 23.9% ***, p = 0.0001 (Z) |
| Western Sicily | 42.3% (52) ** | 59.3% (80) ** | 37.6% (44) | 23.9% (22) | Sp–Eastern: 64.1% **, p = 0.0116 (Z) |
| Au–Eastern: 39.3% ***, p = 0.0003 (Z) | |||||
| Au–Central: 1.5% ***, p = 0.0221 (Z) | |||||
| Sp–Central: 12% **, p = 0.0010 (Z) |
| Eastern Sicily % (n) | Central Sicily % (n) | Western Sicily % (n) | Analysis across Sicilian Areas p-Value (Test) | |
|---|---|---|---|---|
| p < 0.0001 * (Cgf) | ||||
| Patients (n = 467) | 52.2% (244) ** | 5.2% (24) *** | 42.6% (199) ** | Eastern: 52.2% **, p < 0.0001 (Z) |
| Central: 5.2% ***, p < 0.0001 (Z) | ||||
| Western: 42.6% **, p < 0.0001 (Z) | ||||
| Age at admission | ||||
| Mean (SD) | 48.5(23) | 43.8 (22.6) | 51.5 (22.4) | |
| Median (IQR) | 52 (28–67.5) | 41.5 (21.5–63) | 53 (37–71) | p = 0.18 (KW) |
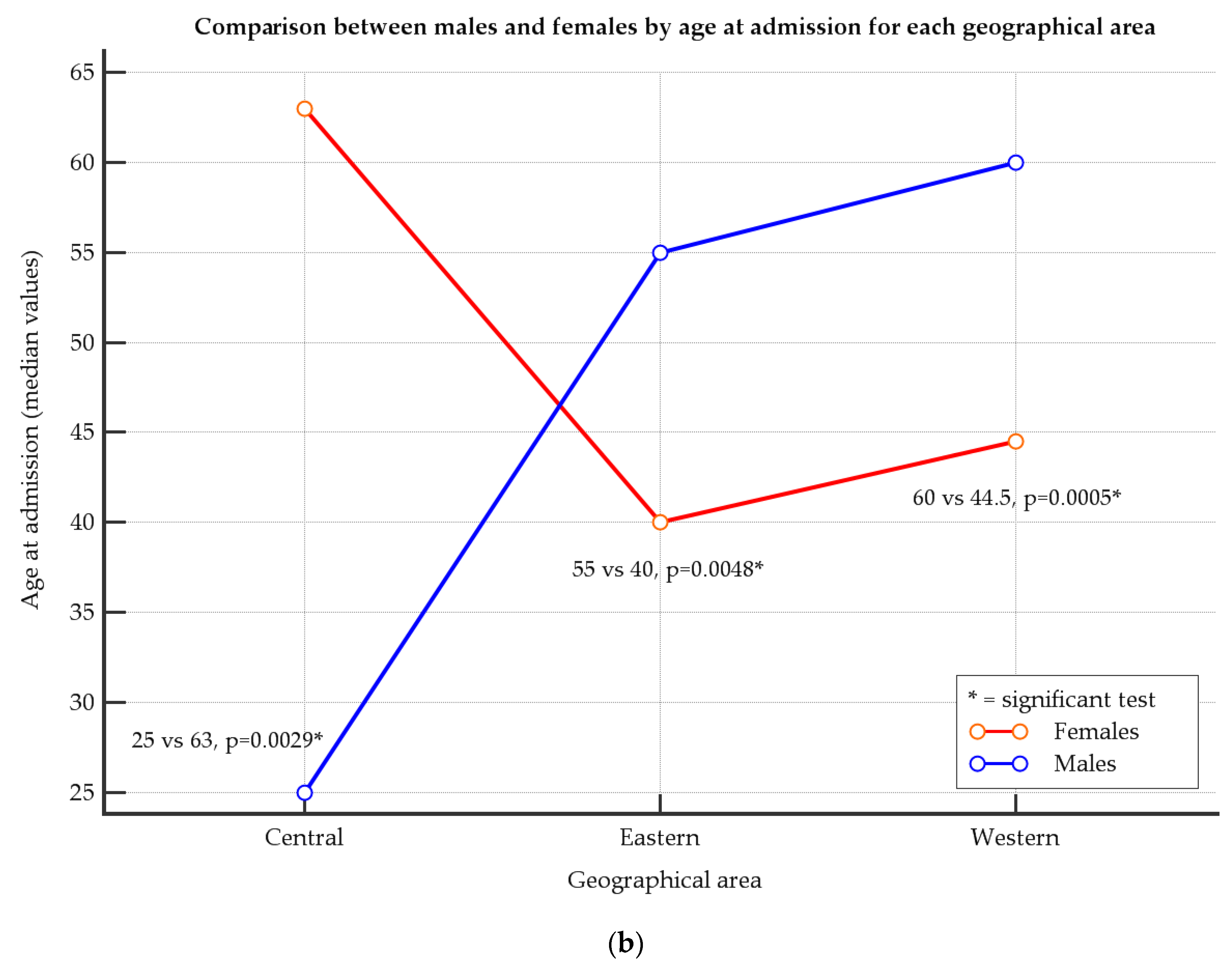
| Age at admission for males | p = 0.0009 * (KW) | |||
| Mean (SD) | 51.8 (21.2) | 33.3 (19.2) | 55.6 (21.5) | Central < Eastern, p < 0.05 (Co) |
| Median (IQR) | 55.0 (38.0–69.0) | 25 (19–49) | 60.0 (41.8–73.3) | Central < Western, p < 0.05 (Co) |
| Age at admission for females | ||||
| Mean (SD) | 42.3 (24.9) | 61.2 (16.3) | 43.9 (22.2) | |
| Median (IQR) | 40.0 (20.0–65.5) | 63 (52.8–71.5) | 44.5 (26.0–60.0) | p = 0.07 (KW) |
| Gender | p = 0.93 I | |||
| Male | 66.0% (161) ** | 62.5% (15) | 64.8% (129) ** | |
| Female | 34.0% (83) | 37.5% (9) | 35.2% (70) | |
| p < 0.0001 * (F) | ||||
| Season | ||||
| Summer (Su) | 26.2% (64) | 29.2% (7) | 26.1% (52) | Eastern–Sp: 24.2% **, p = 0.0109 (Z) |
| Autumn (Au) | 21.7% (53) | 8.3% (2) | 40.2% (80) ** | Eastern–Au: 21.7% ***, p = 0.0003 (Z) |
| Winter (Wi) | 27.9% (68) | 16.7% (4) | 22.6% (45) | Central–Au: 8.3% ***, p = 0.0224 (Z) |
| Spring (Sp) | 24.2% (59) | 45.8% (11) | 11.2% (22) *** | Central–Sp: 45.8% **, p = 0.0010 (Z) |
| Western–Au: 40.2% **, p < 0.0001 (Z) | ||||
| Western–Sp: 11.2% ***, p = 0.0001 (Z) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malta, G.; Serra, N.; Spatola, G.F.; Maida, C.M.; Graziano, G.; Di Raimondo, D.; Fasciana, T.M.A.; Caputo, V.; Giammanco, A.; Capuano, A.; et al. The Impact of the Seasonal and Geographical Distribution of Tuberculosis in Sicily: A 6-Year Retrospective Study (2018–2023). J. Clin. Med. 2024, 13, 3546. https://doi.org/10.3390/jcm13123546
Malta G, Serra N, Spatola GF, Maida CM, Graziano G, Di Raimondo D, Fasciana TMA, Caputo V, Giammanco A, Capuano A, et al. The Impact of the Seasonal and Geographical Distribution of Tuberculosis in Sicily: A 6-Year Retrospective Study (2018–2023). Journal of Clinical Medicine. 2024; 13(12):3546. https://doi.org/10.3390/jcm13123546
Chicago/Turabian StyleMalta, Ginevra, Nicola Serra, Giovanni Francesco Spatola, Carmelo Massimo Maida, Giorgio Graziano, Domenico Di Raimondo, Teresa Maria Assunta Fasciana, Valentina Caputo, Anna Giammanco, Angela Capuano, and et al. 2024. "The Impact of the Seasonal and Geographical Distribution of Tuberculosis in Sicily: A 6-Year Retrospective Study (2018–2023)" Journal of Clinical Medicine 13, no. 12: 3546. https://doi.org/10.3390/jcm13123546
APA StyleMalta, G., Serra, N., Spatola, G. F., Maida, C. M., Graziano, G., Di Raimondo, D., Fasciana, T. M. A., Caputo, V., Giammanco, A., Capuano, A., Sergi, C. M., Cascio, A., & Di Carlo, P. (2024). The Impact of the Seasonal and Geographical Distribution of Tuberculosis in Sicily: A 6-Year Retrospective Study (2018–2023). Journal of Clinical Medicine, 13(12), 3546. https://doi.org/10.3390/jcm13123546