
The Efficacy of CO2 Vaginal Laser in the Treatment of Recurrent, Post-Coital and Interstitial Cystitis: A Multicentric Prospective Study
 , , ,
, , ,  ,
,  and
and
Abstract
1. Introduction
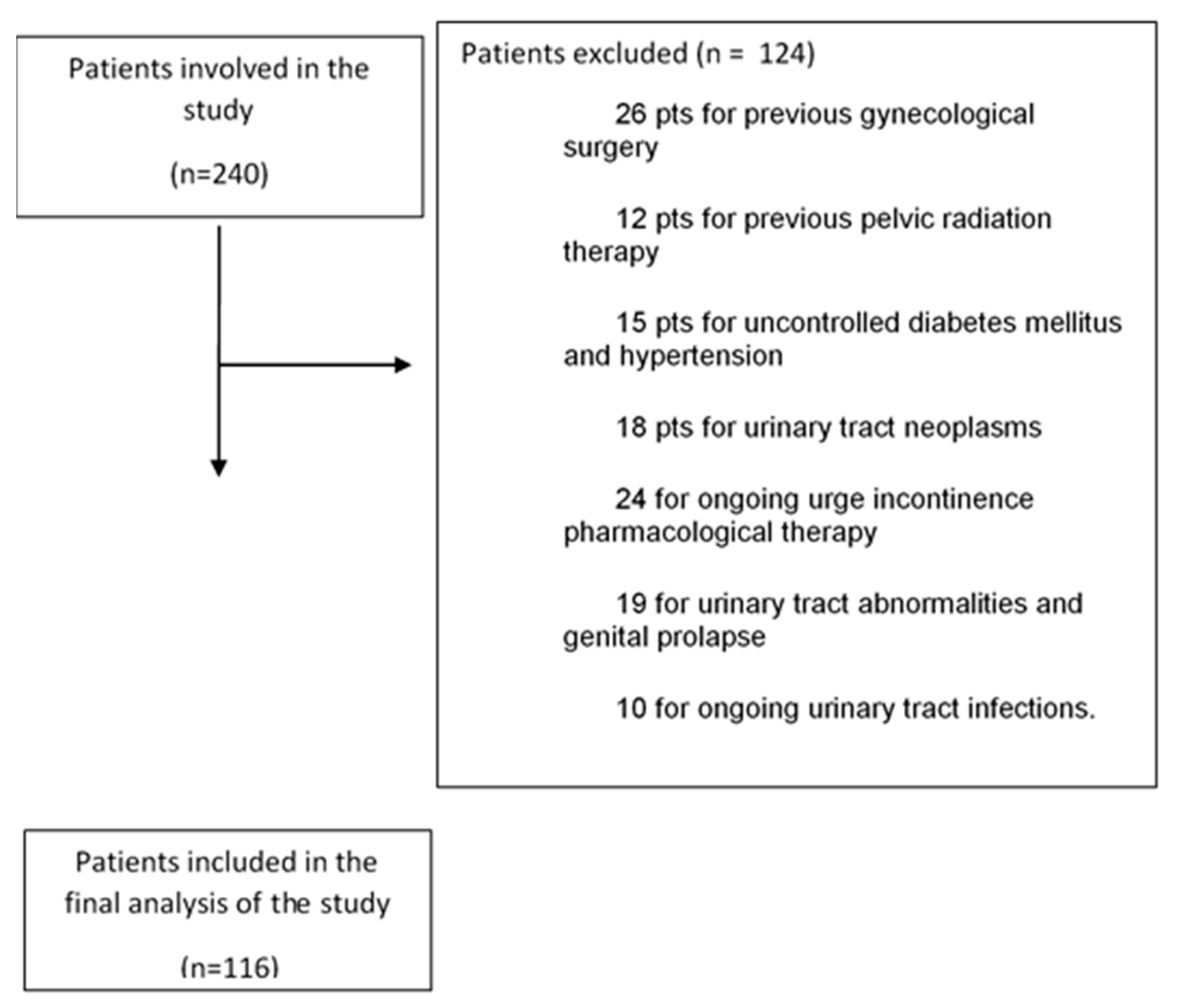
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Franco, A.V.M. Recurrent urinary tract infections. Best Pract. Res. Clin. Obstet. Gynaecol. 2005, 19, 861–873. [Google Scholar] [CrossRef] [PubMed]
- Foxman, B. Urinary tract infection syndromes: Occurrence, recurrence, bacteriology, risk factors, and disease burden. Infect. Dis. Clin. 2014, 28, 1–13. [Google Scholar]
- Shanberg, A.M.; Baghdassarian, R.; Tansey, L.A. Treatment of interstitial cystitis with the neodymium-YAG laser. J. Urol. 1985, 134, 885–888. [Google Scholar] [CrossRef] [PubMed]
- Hanno, P.; Dmochowski, R. Status of international consensus on interstitial cystitis/bladder pain syndrome/painful bladder syndrome: 2008 snapshot. Neurourol. Urodyn. 2009, 28, 274. [Google Scholar] [CrossRef] [PubMed]
- Abrams, P.; Cardozo, L.; Fall, M.; Griffiths, D.; Rosier, P.; Ulmsten, U.; van Kerrebroeck, P.; Victor, A.; Wein, A. Standardisation Sub-committee of the International Continence Society. The standardisation of terminology of lower urinary tract function: Report from the Standardisation Sub-committee of the International Continence Society. Neurourol. Urodyn. 2002, 21, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.; Leslie, S.W.; O’Rourke, S. Interstitial Cystitis/Bladder Pain Syndrome. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Homma, Y.; Ueda, T.; Tomoe, H.; Lin, A.T.; Kuo, H.C.; Lee, M.H.; Lee, J.G.; Kim, D.Y.; Lee, K.S.; The Interstitial Cystitis Guideline Committee. Interstitial cystitis guideline committee. Clinical guidelines for interstitial cystitis and hypersensitive bladder syndrome. Int. J. Urol. 2009, 16, 597–615. [Google Scholar] [CrossRef] [PubMed]
- Clemens, J.Q.; Erickson, D.R.; Varela, N.P.; Lai, H.H. Diagnosis and Treatment of Interstitial Cystitis/Bladder Pain Syndrome. J. Urol. 2022, 208, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Anger, J.; Lee, U.; Ackerman, A.L.; Chou, R.; Chughtai, B.; Clemens, J.Q.; Hickling, D.; Kapoor, A.; Kenton, K.S.; Kaufman, M.R.; et al. Recurrent uncomplicated urinary tract infections in women: AUA/CUA/SUFU guideline. J. Urol. 2019, 202, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Bonkat, G.; Bartoletti, R.; Bruyere, F.; Cai, T.; Geerlings, S.E.; Köves, B.; Schubert, S.; Wagenlehner, F.; Mezei, T.; Pilatz, A.; et al. EAU Guidelines on Urological Infections; European Association of Urology, EAU Guidelines Office: Arnhem, The Netherlands, 2019. [Google Scholar]
- Arnold, J.J.; Hehn, L.E.; Klein, D.A. Common questions about recurrent urinary tract infections in women. Am. Fam. Physician 2016, 93, 560–569. [Google Scholar] [PubMed]
- Ronzoni, G.; De Giovanni, L.; Weir, J.M.; Pasqui, F.; Menchinelli, P. Transposing the urethral meatus in the treatment of recurrent and postcoital cystitis in women with hypospadias. BJU Int. 2001, 87, 894–896. [Google Scholar] [CrossRef] [PubMed]
- Gyftopoulos, K. The aberrant urethral meatus as a possible aetiological factor of recurrent post-coital urinary infections in young women. Med. Hypotheses 2018, 113, 6–8. [Google Scholar] [CrossRef] [PubMed]
- Preti, M.; Vieira-Baptista, P.; Digesu, G.A.; Bretschneider, C.E.; Damaser, M.; Demirkesen, O.; Heller, D.S.; Mangir, N.; Marchitelli, C.; Mourad, S.; et al. The Clinical Role of LASER for Vulvar and Vaginal Treatments in Gynecology and Female Urology: An ICS/ISSVD Best Practice Consensus Document. J. Low. Genit. Tract Dis. 2019, 23, 151–160. [Google Scholar] [CrossRef]
- Filippini, M.; Luvero, D.; Salvatore, S.; Pieralli, A.; Montera, R.; Plotti, F.; Candiani, M.; Angioli, R. Efficacy of fractional CO2 laser treatment in postmenopausal women with genitourinary syndrome: A multicenter study. Menopause 2020, 27, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Perino, A.; Cucinella, G.; Gugliotta, G.; Saitta, S.; Polito, S.; Adile, B.; Marci, R.; Calagna, G. Is vaginal fractional CO2 laser treatment effective in improving overactive bladder symptoms in post-menopausal patients? Preliminary results. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 2491–2497. [Google Scholar] [PubMed]
- Piovano, E.; Macchi, C.; Attamante, L.; Fuso, L.; Maina, G.; Pasero, L.; Volante, R.; Zola, P. CO2 laser vaporization for the treatment of vaginal intraepithelial neoplasia: Effectiveness and predictive factors for recurrence. Eur. J. Gynaecol. Oncol. 2015, 36, 383–388. [Google Scholar] [PubMed]
- Ruffolo, A.F.; Braga, A.; Torella, M.; Frigerio, M.; Cimmino, C.; De Rosa, A.; Sorice, P.; Castronovo, F.; Salvatore, S.; Serati, M. Vaginal Laser Therapy for Female Stress Urinary Incontinence: New Solutions for a Well-Known Issue-A Concise Review. Medicina 2022, 58, 512. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Okui, N. Vaginal Laser Treatment for the Genitourinary Syndrome of Menopause in Breast Cancer Survivors: A Narrative Review. Cureus 2023, 15, e45495. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bhide, A.A.; Khullar, V.; Swift, S.; Digesu, G.A. The use of laser in urogynaecology. Int. Urogynecology J. 2019, 30, 683–692. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ogrinc, U.B.; Senčar, S.; Lenasi, H. Novel minimally invasive laser treatment of urinary incontinence in women. Lasers Surg. Med. 2015, 47, 689–697. [Google Scholar] [CrossRef] [PubMed]
- Gaspar, A.; Addamo, G.; Brandi, H. Vaginal fractional CO2 laser: A minimally invasive option for vaginal rejuvenation. Am. J. Cosmet. Surg. 2011, 28, 156–162. [Google Scholar] [CrossRef]
- Gambacciani, M.; Levancini, M. Vaginal erbium laser: The second generation thermotherapy for the genitourinary syndrome of menopause (GSM) in breast cancer survivors. A preliminary report of a pilot study. Ital. J. Gynaecol. Obstet. 2015, 27, 15–17. [Google Scholar] [CrossRef] [PubMed]
- Pitsouni, E.; Grigoriadis, T.; Tsiveleka, A.; Zacharakis, D.; Salvatore, S.; Athanasiou, S. Microablative fractional CO2-laser therapy and the genitourinary syndrome of menopause: An observational study. Maturitas 2016, 94, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Gambacciani, M.; Levancini, M.; Russo, E.; Vacca, L.; Simoncini, T.; Cervigni, M. Long-term effects of vaginal erbium laser in the treatment of genitourinary syndrome of menopause. Climacteric 2018, 21, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Gambacciani, M.; Palacios, S. Laser therapy for the restoration of vaginal function. Maturitas 2017, 99, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Salvatore, S.; Nappi, R.E.; Parma, M.; Chionna, R.; Lagona, F.; Zerbinati, N.; Ferrero, S.; Origoni, M.; Candiani, M.; Maggiore, U.L.R. Sexual function after fractional microablative CO2 laser in women with vulvovaginal atrophy. Climacteric 2015, 18, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Salvatore, S.; Ruffolo, A.F.; Phillips, C.; Athanasiou, S.; Cardozo, L.; Serati, M.; EUGA Working Group. Vaginal laser therapy for GSM/VVA: Where we stand now—A review by the EUGA Working Group on Laser. Climacteric 2023, 26, 336–352. [Google Scholar] [CrossRef] [PubMed]
- Barba, M.; Cola, A.; De Vicari, D.; Costa, C.; Castelli, A.P.; Volontè, S.; Fruscio, R.; Frigerio, M. Efficacy of a Diode Vaginal Laser in the Treatment of the Genitourinary Syndrome of Menopause. Bioengineering 2023, 10, 1158. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Omi, T.; Numano, K. The role of the CO2 laser and fractional CO2 laser in dermatology. Laser Ther. 2014, 23, 49–60. [Google Scholar] [CrossRef] [PubMed]
- Samuels, J.B.; Garcia, M.A. Treatment to external labia and vaginal canal with CO2 laser for symptoms of vulvovaginal atrophy in postmenopausal women. Aesthetic Surg. J. 2019, 39, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Behnia-Willison, F.; Sarraf, S.; Miller, J.; Mohamadi, B.; Care, A.S.; Lam, A.; Willison, N.; Behnia, L.; Salvatore, S. Safety and long-term efficacy of fractional CO2 laser treatment in women suffering from genitourinary syndrome of menopause. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 213, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Gambacciani, M.; Torelli, M.G.; Martella, L.; Bracco, G.L.; Casagrande, A.G.; Albertin, E.; Tabanelli, S.; Viglietta, M.; D’ambrogio, G.; Garone, G.; et al. Rationale and design for the vaginal erbium laser academy study (Velas): An international multicenter observational study on genitourinary syndrome of menopause and stress urinary incontinence. Climacteric 2015, 18 (Suppl. 1), 43–48. [Google Scholar] [CrossRef] [PubMed]
- Bizjak-Ogrinc, U.; Sencar, S.; Vizintin, Z. 3 years follow-up of pelvic organ prolapses treated with Er: YAG laser. Lasers Surg. Med. 2017, 49, 63. [Google Scholar]
- Bizjak-Ogrinc, U.; Sentra, S. Non-surgical minimally invasive Er: YAG Laser treatment for higher grade cystocele. In Proceedings of the 38th Annual IUGA Meeting, Dublin, Ireland, 28 May–1 June 2013. [Google Scholar]
- Stefano, S.; Stavros, A.; Massimo, C. The use of pulsed CO2 lasers for the treatment of vulvovaginal atrophy. Curr. Opin. Obstet. Gynecol. 2015, 27, 504–508. [Google Scholar] [CrossRef] [PubMed]
- Benitez-Roig, V.; Martínez-Carpio, P.A.; Trelles, M.A.; Cosmina-Timircan, A.; Arias-Salgado, E.G.; Perona, R. Clinical and laboratory results in vaginal wall restoration using a fractional-pixel-CO2 laser: Histological findings and changes in the Ki67 protein and telomere length. Lasers Med. Sci. 2023, 38, 206. [Google Scholar] [CrossRef] [PubMed]
- Qi, Y.; Mo, K.; Wang, A.; He, Y. Different effects of CO2 laser and estrogen treatment on vaginal mucosa microbiota and function in genitourinary syndrome of menopause patients. J. Obstet. Gynaecol. Res. 2024, 50, 671–681. [Google Scholar] [CrossRef] [PubMed]
- Gómez de Vicente, J.M.; Trelles Guzmán, C. Uso de la tecnología láser en urología funcional y uroginecología [Laser technology applications in functional urology and urogynecology]. Arch. Esp. Urol. 2020, 73, 709–723. (In Spanish) [Google Scholar] [PubMed]
- Klap, J.; Campagne-Loiseau, S.; Berrogain, N.; Bosset, P.O.; Cardot, V.; Charles, T.; Deffieux, X.; Donon, L.; Girard, F.; Peyrat, L.; et al. Comité d’Urologie et de Pelviperinéologie de la Femme (CUROPF) de l’Association Française d’Urologie. [Vaginal LASER therapy for genito-urinary disorders: A systematic review and statement from the Committee for Female Urology and Pelviperineology of the French Association of Urology]. Prog. Urol. 2021, 31, 634–650. (In French) [Google Scholar] [CrossRef] [PubMed]
- Luvero, D.; Angioli, R.; Baruch, Y.; Salvatore, S.; Filippini, M.; Pieralli, A.; Montera, R. The efficacy and feasibility of fractional CO2 laser therapy for the treatment of urinary incontinence: A multicentric case-control study. Minerva Obstet. Gynecol. 2023; epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Angioli, R.; Stefano, S.; Filippini, M.; Pieralli, A.; Montera, R.; Plotti, F.; Gatti, A.; Bartolone, M.; Luvero, D. Effectiveness of CO2 laser on urogenital syndrome in women with a previous gynecological neoplasia: A multicentric study. Int. J. Gynecol. Cancer 2020, 30, 590–595. [Google Scholar] [CrossRef] [PubMed]
- Ratz, C. Vaginale Lasertherapie bei Harninkontinenz und urogenitalem Syndrom der Menopause: Eine Übersicht [Vaginal laser therapy for urinary incontinence and genitourinary syndrome of menopause: A review]. Urol. A 2019, 58, 284–290. (In German) [Google Scholar] [CrossRef] [PubMed]
- Doumouchtsis, S.K.; Lee, F.Y.; Bramwell, D.; Fynes, M.M. Evaluation of holmium laser for managing mesh/suture complications of continence surgery. BJU Int. 2011, 108, 1472–1478. [Google Scholar] [CrossRef] [PubMed]
- Okui, N.; Okui, M.; Gambacciani, M. Is Erbium/Neodymium Laser Combination Therapy an Effective Treatment Option for Interstitial Cystitis/Bladder Pain Syndrome With Vulvodynia? Cureus 2022, 14, e31228. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Okui, N.; Okui, M.A.; Kouno, Y.; Nakano, K. Laser Treatment for Patients With Vulvodynia and Interstitial Cystitis/Bladder Pain Syndrome: A Case Series (The UNICORN-3 Study). Cureus 2023, 15, e41786. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Droupy, S. The therapeutic approach to different forms of cystitis: Impact on public health. Urologia 2017, 84 (Suppl. 1), 8–15. [Google Scholar] [CrossRef] [PubMed]
- Ciani, O.; Grassi, D.; Tarricone, R. An economic perspective on urinary tract infection: The “costs of resignation”. Clin. Drug Investig. 2013, 33, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Filippini, M.; Porcari, I.; Ruffolo, A.F.; Casiraghi, A.; Farinelli, M.; Uccella, S.; Franchi, M.; Candiani, M.; Salvatore, S. CO2-Laser therapy and Genitourinary Syndrome of Menopause: A Systematic Review and Meta-Analysis. J. Sex Med. 2022, 19, 452–470. [Google Scholar] [CrossRef] [PubMed]
- Machado, A.C.; Judice, L.M.D.P.P.; Riccetto, C.L.Z.; Toledo, L.G.M. Applicability of vaginal energy-based devices in urogynecology: Evidence and controversy. Rev. Assoc. Med. Bras 2023, 69 (Suppl. 1), e2023S129. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Romero-Otero, J.; Lauterbach, R.; Aversa, A.; Serefoglu, E.C.; García-Gómez, B.; Parnham, A.; Skrodzka, M.; Krychman, M.; Reisman, Y.; Corona, G.; et al. Laser-Based Devices for Female Genitourinary Indications: Position Statements From the European Society for Sexual Medicine (ESSM). J. Sex Med. 2020, 17, 841–848. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Numbers | Mean Age | |
|---|---|---|
| Total nr of patients | 116 | 54 (27–75) |
| Pre-menopausal patients | 46 (39.7%) | 37 (21–45) |
| Post-menopausal patients | 70 (60.3%) | 57 (44–75) |
| Patients with contextual intravesical hyaluronic acid therapy | 81 (70%) | 56 (27–76) |
| Patients without contextual intravesical hyaluronic acid therapy | 35 (30%) | 57 (36–72) |
| Patients with vulvo–vaginal atrophy | 50 (34.5%) | 50 (27–72) |
| Patients without vulvo–vaginal atrophy | 66 (65.5%) | 61 (36–76) |
| Pts with Interstitial Cystitis | Pts with Recurrent Cystitis | Pts with Post-Coital Cystitis | Pts with Recurrent and Post-Coital Cystitis | |
|---|---|---|---|---|
| Patients with contextual intravesical hyaluronic acid therapy | 1 (1.2%) | 49 (60.5%) | 23 (28.4%) | 1 (1.2%) |
| Patients without contextual intravesical hyaluronic acid therapy | 2 (5.7%) | 23 (65.7%) | 6 (17.1%) | 3 (8.6%) |
| Patients with vaginal atrophy | 1 (1.5%) | 54 (81.8%) | 6 (9.1%) | 2 (3.0%) |
| Patients without vaginal atrophy | 2 (4.0%) | 18 (36.0%) | 23 (46.0%) | 3 (6.0%) |
| Total nr of patients | 5 (4.5%) | 77 (66%) | 29 (25%) | 5 (4.5%) |
| Pre-Treatment Average Number of Cystitis Episodes per Year | Pos-Treatment Average Number of Cystitis Episodes per Year | |
|---|---|---|
| Patients with contextual intravesical hyaluronic acid therapy | 4.9 (3–11) | 1.7 (0–5) |
| Patients without contextual intravesical hyaluronic acid therapy | 4.8 (3–9) | 1.1 (0–3) |
| Patients with vaginal atrophy | 5.4 (3–11) | 2.4 (0–5) |
| Patients without vaginal atrophy | 5.1 (3–8) | 1.7 (0–4) |
| Total nr of patients | 5.1 (3–9) | 2.4 (0–7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luvero, D.; Silvagni, A.; Angioli, A.M.; Filippini, M.; Plotti, F.; Montera, R.; De Cicco Nardone, C.; Notaro, E.; Branda, F.; Angioli, R. The Efficacy of CO2 Vaginal Laser in the Treatment of Recurrent, Post-Coital and Interstitial Cystitis: A Multicentric Prospective Study. J. Clin. Med. 2024, 13, 3550. https://doi.org/10.3390/jcm13123550
Luvero D, Silvagni A, Angioli AM, Filippini M, Plotti F, Montera R, De Cicco Nardone C, Notaro E, Branda F, Angioli R. The Efficacy of CO2 Vaginal Laser in the Treatment of Recurrent, Post-Coital and Interstitial Cystitis: A Multicentric Prospective Study. Journal of Clinical Medicine. 2024; 13(12):3550. https://doi.org/10.3390/jcm13123550
Chicago/Turabian StyleLuvero, Daniela, Adele Silvagni, Anna Maria Angioli, Maurizio Filippini, Francesco Plotti, Roberto Montera, Carlo De Cicco Nardone, Erika Notaro, Francesco Branda, and Roberto Angioli. 2024. "The Efficacy of CO2 Vaginal Laser in the Treatment of Recurrent, Post-Coital and Interstitial Cystitis: A Multicentric Prospective Study" Journal of Clinical Medicine 13, no. 12: 3550. https://doi.org/10.3390/jcm13123550
APA StyleLuvero, D., Silvagni, A., Angioli, A. M., Filippini, M., Plotti, F., Montera, R., De Cicco Nardone, C., Notaro, E., Branda, F., & Angioli, R. (2024). The Efficacy of CO2 Vaginal Laser in the Treatment of Recurrent, Post-Coital and Interstitial Cystitis: A Multicentric Prospective Study. Journal of Clinical Medicine, 13(12), 3550. https://doi.org/10.3390/jcm13123550