
Optimizing Outcomes in Mismatched Unrelated Donor Allogeneic Transplantation: Post-Transplant Cyclophosphamide’s Dual Impact on Graft versus Host Disease Incidence and Overall Survival: Retrospective Analysis on Behalf of Polish Adult Leukemia Group

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Conditioning Regimen
2.3. GvHD Prophylaxis
2.4. Outcomes
2.5. Statistical Methods
3. Results
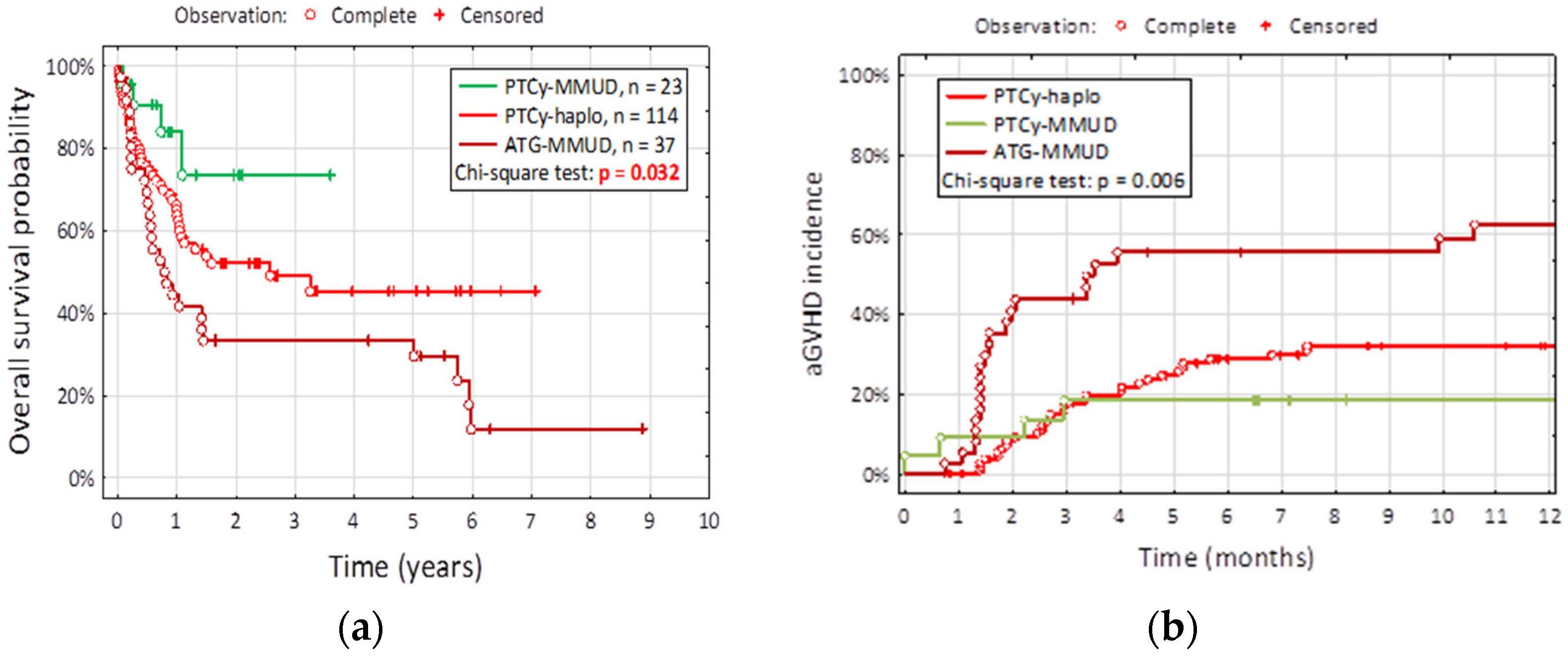
3.1. Survival
3.2. GvHD
3.3. CMV Reactivation
3.4. Neutrophil Recovery
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, X.J.; Liu, D.H.; Liu, K.Y.; Xu, L.P.; Chen, H.; Han, W.; Chen, Y.H.; Zhang, X.H.; Lu, D.P. Treatment of Acute Leukemia with Unmanipulated HLA-Mismatched/Haploidentical Blood and Bone Marrow Transplantation. Biol. Blood Marrow Transplant. 2009, 15, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Baron, F.; Labopin, M.; Tischer, J.; Ciceri, F.; Raiola, A.M.; Blaise, D.; Sica, S.; Vydra, J.; Fanin, R.; Diez-Martin, J.L.; et al. Comparison of HLA-Mismatched Unrelated Donor Transplantation with Post-Transplant Cyclophosphamide versus HLA-Haploidentical Transplantation in Patients with Active Acute Myeloid Leukemia. Bone Marrow Transplant. 2022, 57, 1657–1663. [Google Scholar] [CrossRef] [PubMed]
- Moiseev, I.S.; Pirogova, O.V.; Alyanski, A.L.; Babenko, E.V.; Gindina, T.L.; Darskaya, E.I.; Slesarchuk, O.A.; Bondarenko, S.N.; Afanasyev, B.V. Graft-versus-Host Disease Prophylaxis in Unrelated Peripheral Blood Stem Cell Transplantation with Post-Transplantation Cyclophosphamide, Tacrolimus, and Mycophenolate Mofetil. Biol. Blood Marrow Transplant. 2016, 22, 1037–1042. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wu, D.P.; Liu, Q.F.; Xu, L.P.; Liu, K.Y.; Zhang, X.H.; Yu, W.J.; Xu, Y.; Huang, F.; Huang, X.J. Low-Dose Post-Transplant Cyclophosphamide and Anti-Thymocyte Globulin as an Effective Strategy for GVHD Prevention in Haploidentical Patients. J. Hematol. Oncol. 2019, 12, 88. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Rastogi, N.; Chatterjee, G.; Kapoor, R.; Nivargi, S.; Yadav, S.P. Haploidentical Stem Cell Transplantation with Post-Transplant Cyclophosphamide for Pediatric Acute Leukemia Is Safe and Effective. J. Pediatr. Hematol. Oncol. 2021, 43, E1033–E1036. [Google Scholar] [CrossRef] [PubMed]
- Apperley, J.; Niederwieser, D.; Huang, X.-J.; Nagler, A.; Fuchs, E.; Szer, J.; Kodera, Y. Haploidentical Hematopoietic Stem Cell Transplantation: A Global Overview Comparing Asia, the European Union, and the United States. Biol. Blood Marrow Transplant. 2016, 22, 23–26. [Google Scholar] [CrossRef] [PubMed]
- Camargo, J.F.; Ebisu, Y.; Jimenez-Jimenez, A.; Natori, Y.; Moroz, I.; Morris, M.I.; Alencar, M.; Anderson, A.D.; Lekakis, L.; Beitinjaneh, A.; et al. Lower Incidence of Cytomegalovirus Reactivation Following Post-Transplantation Cyclophosphamide HLA-Mismatched Unrelated Donor Transplantation. Transplant. Cell. Ther. 2021, 27, 1017.e1–1017.e7. [Google Scholar] [CrossRef]
- Modi, D.; Kondrat, K.; Kim, S.; Deol, A.; Ayash, L.; Ratanatharathorn, V.; Uberti, J.P. Post-Transplant Cyclophosphamide Versus Thymoglobulin in HLA-Mismatched Unrelated Donor Transplant for Acute Myelogenous Leukemia and Myelodysplastic Syndrome. Transplant. Cell. Ther. 2021, 27, 760–767. [Google Scholar] [CrossRef]
- Dybko, J.; Sobczyk-Kruszelnicka, M.; Makuch, S.; Agrawal, S.; Dudek, K.; Giebel, S.; Gil, L. The Benefits of the Post-Transplant Cyclophosphamide in Both Haploidentical and Mismatched Unrelated Donor Setting in Allogeneic Stem Cells Transplantation. Int. J. Mol. Sci. 2023, 24, 5764. [Google Scholar] [CrossRef]
- Bonifazi, F.; Rubio, M.T.; Bacigalupo, A.; Boelens, J.J.; Finke, J.; Greinix, H.; Mohty, M.; Nagler, A.; Passweg, J.; Rambaldi, A.; et al. Rabbit ATG/ATLG in Preventing Graft-versus-Host Disease after Allogeneic Stem Cell Transplantation: Consensus-Based Recommendations by an International Expert Panel. Bone Marrow Transplant. 2020, 55, 1093–1102. [Google Scholar] [CrossRef]
- EBMT 2023—Program. Available online: https://ebmt2023.abstractserver.com/program/#/details/presentations/1753 (accessed on 22 August 2023).
- Luznik, L.; Bolaños-Meade, J.; Zahurak, M.; Chen, A.R.; Smith, B.D.; Brodsky, R.; Huff, C.A.; Borrello, I.; Matsui, W.; Powell, J.D.; et al. High-Dose Cyclophosphamide as Single-Agent, Short-Course Prophylaxis of Graft-versus-Host Disease. Blood 2010, 115, 3224–3230. [Google Scholar] [CrossRef] [PubMed]
- McCurdy, S.R.; Luznik, L. Post-Transplantation Cyclophosphamide for Chimerism-Based Tolerance. Bone Marrow Transplant. 2019, 54, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Luznik, L.; Pasquini, M.C.; Logan, B.; Soiffer, R.J.; Wu, J.; Devine, S.M.; Geller, N.; Giralt, S.; Heslop, H.E.; Horowitz, M.M.; et al. Randomized Phase III BMT CTN Trial of Calcineurin Inhibitor–Free Chronic Graft-Versus-Host Disease Interventions in Myeloablative Hematopoietic Cell Transplantation for Hematologic Malignancies. J. Clin. Oncol. 2022, 40, 356–368. [Google Scholar] [CrossRef] [PubMed]
- Mielcarek, M.; Furlong, T.; O’Donnell, P.V.; Storer, B.E.; McCune, J.S.; Storb, R.; Carpenter, P.A.; Flowers, M.E.D.; Appelbaum, F.R.; Martin, P.J. Posttransplantation Cyclophosphamide for Prevention of Graft-versus-Host Disease after HLA-Matched Mobilized Blood Cell Transplantation. Blood 2016, 127, 1502–1508. [Google Scholar] [CrossRef] [PubMed]
- Carnevale-Schianca, F.; Caravelli, D.; Gallo, S.; Becco, P.; Paruzzo, L.; Poletto, S.; Polo, A.; Mangioni, M.; Salierno, M.; Berger, M.; et al. Post-Transplant Cyclophosphamide and Tacrolimus—Mycophenolate Mofetil Combination Governs Gvhd and Immunosuppression Need, Reducing Late Toxicities in Allogeneic Peripheral Blood Hematopoietic Cell Transplantation from Hla-Matched Donors. J. Clin. Med. 2021, 10, 1173. [Google Scholar] [CrossRef] [PubMed]
- Greco, R.; Lorentino, F.; Morelli, M.; Giglio, F.; Mannina, D.; Assanelli, A.; Mastaglio, S.; Dalto, S.; Perini, T.; Lazzari, L.; et al. Posttransplantation Cyclophosphamide and Sirolimus for Prevention of GVHD after HLA-Matched PBSC Transplantation. Blood 2016, 128, 1528–1531. [Google Scholar] [CrossRef] [PubMed]
- Holtick, U.; Chemnitz, J.M.; Shimabukuro-Vornhagen, A.; Theurich, S.; Chakupurakal, G.; Krause, A.; Fiedler, A.; Luznik, L.; Hellmich, M.; Wolf, D.; et al. OCTET-CY: A Phase II Study to Investigate the Efficacy of Post-Transplant Cyclophosphamide as Sole Graft-versus-Host Prophylaxis after Allogeneic Peripheral Blood Stem Cell Transplantation. Eur. J. Haematol. 2016, 96, 27–35. [Google Scholar] [CrossRef] [PubMed]
- EBMT 2023—Program. Available online: https://ebmt2023.abstractserver.com/program/#/details/persons/446 (accessed on 4 January 2024).
- Spyridonidis, A. How Much Immunosuppression Do We Need? Blood 2017, 129, 1241–1243. [Google Scholar] [CrossRef] [PubMed]
- Bacigalupo, A.; Ballen, K.; Rizzo, D.; Giralt, S.; Lazarus, H.; Ho, V.; Apperley, J.; Slavin, S.; Pasquini, M.; Sandmaier, B.M.; et al. Defining the Intensity of Conditioning Regimens: Working Definitions. Biol. Blood Marrow Transplant. 2009, 15, 1628–1633. [Google Scholar] [CrossRef]
- Oostenbrink, L.V.E.; Pool, E.S.; Jol-van der Zijde, C.M.; Jansen-Hoogendijk, A.M.; Vervat, C.; van Halteren, A.G.S.; Bredius, R.G.M.; Smiers, F.J.W.; van Tol, M.J.D.; Schilham, M.W.; et al. Successful Mismatched Hematopoietic Stem Cell Transplantation for Pediatric Hemoglobinopathy by Using ATG and Post-Transplant Cyclophosphamide. Bone Marrow Transplant. 2021, 56, 2203–2211. [Google Scholar] [CrossRef]
- Ghosh, N.; Karmali, R.; Rocha, V.; Ahn, K.W.; DiGilio, A.; Hari, P.N.; Bachanova, V.; Bacher, U.; Dahi, P.; De Lima, M.; et al. Reduced-Intensity Transplantation for Lymphomas Using Haploidentical Related Donors versus HLA-Matched Sibling Donors: A Center for International Blood and Marrow Transplant Research Analysis. J. Clin. Oncol. 2016, 34, 3141–3149. [Google Scholar] [CrossRef] [PubMed]
- Rimando, J.; Slade, M.; DiPersio, J.F.; Westervelt, P.; Gao, F.; Liu, C.; Romee, R. HLA Epitope Mismatch in Haploidentical Transplantation Is Associated with Decreased Relapse and Delayed Engraftment. Blood Adv. 2018, 2, 3590–3601. [Google Scholar] [CrossRef] [PubMed]
- Battipaglia, G.; Labopin, M.; Kröger, N.; Vitek, A.; Afanasyev, B.; Hilgendorf, I.; Schetelig, J.; Ganser, A.; Blaise, D.; Itälä-Remes, M.; et al. Posttransplant Cyclophosphamide vs Antithymocyte Globulin in HLA-Mismatched Unrelated Donor Transplantation. Blood 2019, 134, 892–899. [Google Scholar] [CrossRef] [PubMed]
- Nykolyszyn, C.; Granata, A.; Pagliardini, T.; Castagna, L.; Harbi, S.; Bouabdallah, R.; Vey, N.; Fürst, S.; Maisano, V.; Legrand, F.; et al. Posttransplantation Cyclophosphamide vs. Antithymocyte Globulin as GVHD Prophylaxis for Mismatched Unrelated Hematopoietic Stem Cell Transplantation. Bone Marrow Transplant. 2020, 55, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Battipaglia, G.; Labopin, M.; Hamladji, R.M.; Blaise, D.; Chevallier, P.; Brissot, E.; Gerbitz, A.; Socié, G.; Afanasyev, B.; Ciceri, F.; et al. Post-Transplantation Cyclophosphamide versus Antithymocyte Globulin in Patients with Acute Myeloid Leukemia Undergoing Allogeneic Stem Cell Transplantation from HLA-Identical Sibling Donors: A Retrospective Analysis from the Acute Leukemia Working Party of the European Society for Blood and Marrow Transplantation. Cancer 2021, 127, 209–218. [Google Scholar] [CrossRef]
- Massoud, R.; Gagelmann, N.; Fritzsche-Friedland, U.; Zeck, G.; Heidenreich, S.; Wolschke, C.; Ayuk, F.; Christopeit, M.; Kröger, N. Comparison of Immune Reconstitution between Anti-T-Lymphocyte Globulin and Posttransplant Cyclophosphamide as Acute Graft-versus-Host Disease Prophylaxis in Allogeneic Myeloablative Peripheral Blood Stem Cell Transplantation. Haematologica 2022, 107, 857–867. [Google Scholar] [CrossRef]
- Battipaglia, G.; Galimard, J.E.; Labopin, M.; Raiola, A.M.; Blaise, D.; Ruggeri, A.; Koc, Y.; Gülbas, Z.; Vitek, A.; Sica, S.; et al. Post-Transplant Cyclophosphamide in One-Antigen Mismatched Unrelated Donor Transplantation versus Haploidentical Transplantation in Acute Myeloid Leukemia: A Study from the Acute Leukemia Working Party of the EBMT. Bone Marrow Transplant. 2022, 57, 562–571. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, A.J.; Komanduri, K.; Brown, S.; Wang, T.; Pereira, D.; Goodman, M.; Beitinjaneh, A.; Lekakis, L.; Chinapen, S.; Devlin, S.; et al. Improved GRFS after Posttransplant Cyclophosphamide-Based vs ATG-Based HLA-Mismatched Unrelated Donor Transplant. Blood Adv. 2022, 6, 4491–4500. [Google Scholar] [CrossRef] [PubMed]
- Jorge, A.S.; Suárez-Lledó, M.; Pereira, A.; Gutierrez, G.; Fernández-Avilés, F.; Rosiñol, L.; Llobet, N.; Solano, T.; Urbano-Ispízua, Á.; Rovira, M.; et al. Single Antigen–Mismatched Unrelated Hematopoietic Stem Cell Transplantation Using High-Dose Post-Transplantation Cyclophosphamide Is a Suitable Alternative for Patients Lacking HLA-Matched Donors. Biol. Blood Marrow Transplant. 2018, 24, 1196–1202. [Google Scholar] [CrossRef]
- Tang, L.; Liu, Z.; Li, T.; Dong, T.; Wu, Q.; Niu, T.; Liu, T.; Ji, J. Post-Transplant Cyclophosphamide versus Anti-Thymocyte Globulin in Allogeneic Hematopoietic Stem Cell Transplantation from Unrelated Donors: A Systematic Review and Meta-Analysis. Front. Oncol. 2023, 13, 1071268. [Google Scholar] [CrossRef]
- Marcoux, C.; Marin, D.; Ramdial, J.; AlAtrash, G.; Alousi, A.M.; Oran, B.; Kebriaei, P.; Popat, U.R.; Rezvani, K.; Champlin, R.E.; et al. Younger Haploidentical Donor versus Older Matched Unrelated Donor for Patients with AML/MDS. Am. J. Hematol. 2023, 98, 712–719. [Google Scholar] [CrossRef] [PubMed]
- Abid, M.B.; Estrada-Merly, N.; Zhang, M.J.; Chen, K.; Allan, D.; Bredeson, C.; Sabloff, M.; Guru Murthy, G.S.; Badar, T.; Hashmi, S.; et al. Impact of Donor Age on Allogeneic Hematopoietic Cell Transplantation Outcomes in Older Adults with Acute Myeloid Leukemia. Transplant. Cell Ther. 2023, 29, 578.e1–578.e9. [Google Scholar] [CrossRef] [PubMed]
- Rezvani, A.R.; Storer, B.E.; Guthrie, K.A.; Schoch, H.G.; Maloney, D.G.; Sandmaier, B.M.; Storb, R. Impact of Donor Age on Outcome after Allogeneic Hematopoietic Cell Transplantation. Biol. Blood Marrow Transplant. 2015, 21, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Penack, O.; Abouqateb, M.; Peczynski, C.; Boreland, W.; Gülbas, Z.; Gedde-Dahl, T.; Castilla-Llorente, C.; Kröger, N.; Eder, M.; Rambaldi, A.; et al. PTCy versus ATG as Graft-versus-Host Disease Prophylaxis in Mismatched Unrelated Stem Cell Transplantation. Blood Cancer J. 2024, 14, 45. [Google Scholar] [CrossRef] [PubMed]
- Retière, C.; Willem, C.; Guillaume, T.; Vié, H.; Gautreau-Rolland, L.; Scotet, E.; Saulquin, X.; Gagne, K.; Béné, M.C.; Imbert, B.M.; et al. Impact on Early Outcomes and Immune Reconstitution of Highdose Post-Transplant Cyclophosphamide vs Anti-Thymocyte Globulin after Reduced Intensity Conditioning Peripheral Blood Stem Cell Allogeneic Transplantation. Oncotarget 2018, 9, 11451–11464. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.S.; Saliba, R.M.; Rondon, G.; Al-Atrash, G.; Bashir, Q.; Hosing, C.M.; Kebriaei, P.; Khouri, I.; Nieto, Y.; Oran, B.; et al. Post-Transplantation Cyclophosphamide Versus Tacrolimus and Methotrexate Graft-Versus-Host Disease Prophylaxis for HLA-Matched Donor Transplantation. Transplant. Cell Ther. 2022, 28, 695.e1–695.e10. [Google Scholar] [CrossRef] [PubMed]
- Goldsmith, S.R.; Abid, M.B.; Auletta, J.J.; Bashey, A.; Beitinjaneh, A.; Castillo, P.; Chemaly, R.F.; Chen, M.; Ciurea, S.; Dandoy, C.E.; et al. Posttransplant Cyclophosphamide Is Associated with Increased Cytomegalovirus Infection: A CIBMTR Analysis. Blood 2021, 137, 3291–3305. [Google Scholar] [CrossRef]
- Mikulska, M.; Bartalucci, C.; Raiola, A.M.; Oltolini, C. Does PTCY Increase the Risk of Infections? Blood Rev. 2023, 62, 101092. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| PTCy-haplo n = 114 | PTCy-MMUD n = 23 | ATG-MMUD n = 37 | p-Value | |
|---|---|---|---|---|
| Patient age, years, Me (IQR) | 44 (31–56) | 54 (44–60) | 45 (35–53) | 0.101 |
| Sex, n (%) | 0.628 | |||
| Male | 52 (45.6%) | 13 (56.5%) | 18 (48.6%) | |
| Female | 62 (54.4%) | 10 (43.5%) | 19 (51.4%) | |
| Diagnosis, n (%) | 0.004 | |||
| AML + MDS | 56 (49.1%) | 12 (52.2%) | 15 (40.5%) | |
| ALL | 18 (15.8%) | 2 (8.7%) | 7 (18.9%) | |
| HL + NHL + MM | 32 (28.1%) | 1 (4.3%) | 11 (29.7%) | |
| OMF, CML, SAA et al. | 8 (7.0%) | 8 (34.8%) | 4 (10.8%) | |
| Median donor age, years Me (IQR) | 36 (28–47) | 33 (25–39) | 31 (23–40) | 0.027 |
| Donor age, n (%) | 0.021 | |||
| <40 years | 64 (56.1%) | 19 (82.6%) | 27 (73.0%) | |
| ≥40 years | 50 (43.9%) | 4 (17.4%) | 10 (27.0%) | |
| Conditioning, n (%) | <0.001 | |||
| RIC | 34 (29.8%) | 0 (0.0%) | 2 (5.4%) | |
| MAC | 61 (53.5%) | 23 (100.0%) | 32 (86.5%) | |
| NMA | 19 (16.7%) | 0 (0.0%) | 3 (8.1%) | |
| The first day post-transplant when a total neutrophil count > 0.5 | 21 (18–24) | 21 (18–25) | 15 (13–16) | <0.001 |
| Acute GvHD, n (%) | 40 (35.1%) | 5 (21.7%) | 22 (59.5%) | 0.006 |
| 1 or 2 grade of aGvHD, n (%) | 34 (29.8%) | 3 (13%) | 14 (37.8%) | 0.110 |
| 3 or 4 grade of aGvHD, n (%) | 6 (5.3%) | 2 (8.7%) | 8 (21.6%) | 0.014 |
| Median time of onset of acute GvHD, days (IQR) | 41 (25–69) | 27 (8–36) | 18 (17–25) | 0.001 |
| Chronic GvHD, n (%) | 28 (24.6%) | 0 (0.0%) | 4 (10.8%) | 0.009 |
| CMV ≥ 250 copies before treatment, n (%) | 54 (47.4%) | 8 (34.8%) | 25 (67.6%) | 0.030 |
| CMV < 250 copies before treatment, n (%) | 13 (11.4%) | 0 (0.0%) | 11 (29.7%) | 0.002 |
| Number of deceased patients until the end of observation, n (%) | 46 (40.4%) | 4 (17.4%) | 28 (75.7%) | <0.001 |
| Death due to infection, n (%) | 19 (45.2%) | 1 (25.0%) | 14 (58.3%) | 0.369 |
| Death due to GvHD, n (%) | 5 (11.9%) | 0 (0.0%) | 2 (8.3%) | 0.709 |
| Death due to relapse, n (%) | 7 (16.7%) | 1 (25.0%) | 7 (29.2%) | 0.484 |
| Death from another or unknown cause, n (%) | 15 (13.2%) | 2 (50.0%) | 1 (4.2%) | 0.828 |
| 3-years overall survival S (t = 3) | 49.1% | 73.6% | 33.4% | 0.032 |
| Median survival function | 28 months | >12.6 months | 10 months |
| Risk Factor for aGvHD | b | p | beta | p | OR (95% CI) |
|---|---|---|---|---|---|
| PTCy-MMUD [yes] | −0.919 | 0.086 | −1.835 | 0.088 | 0.16 (0.02–1.32) |
| ATG-MMUD [yes] | 1.098 | 0.004 | 1.444 | 0.002 | 4.24 (1.73–10.4) |
| Donor age ≥ 31 years [yes] | 1.163 | 0.001 | 0.057 | <0.001 | 4.34 (1.98–9.49) |
| Risk Factor for cGvHD | b | p | beta | p | OR (95% CI) |
|---|---|---|---|---|---|
| PTCy-haplo [yes] | 1.517 | 0.008 | 1.316 | 0.023 | 3.73 (1.20–11.6) |
| Donor: mismatched MUD [yes] | −1.517 | 0.008 | −0.978 | 0.340 | 0.38 (0.05–2.87) |
| Donor age ≥ 42 years | 1.423 | 0.001 | 1.265 | 0.003 | 3.54 (1.56–8.06) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dybko, J.; Sobczyk-Kruszelnicka, M.; Sadowska-Klasa, A.; Piekarska, A.; Makuch, S.; Agrawal, S.; Dudek, K.; Giordano, U.; Giebel, S.; Gil, L. Optimizing Outcomes in Mismatched Unrelated Donor Allogeneic Transplantation: Post-Transplant Cyclophosphamide’s Dual Impact on Graft versus Host Disease Incidence and Overall Survival: Retrospective Analysis on Behalf of Polish Adult Leukemia Group. J. Clin. Med. 2024, 13, 3569. https://doi.org/10.3390/jcm13123569
Dybko J, Sobczyk-Kruszelnicka M, Sadowska-Klasa A, Piekarska A, Makuch S, Agrawal S, Dudek K, Giordano U, Giebel S, Gil L. Optimizing Outcomes in Mismatched Unrelated Donor Allogeneic Transplantation: Post-Transplant Cyclophosphamide’s Dual Impact on Graft versus Host Disease Incidence and Overall Survival: Retrospective Analysis on Behalf of Polish Adult Leukemia Group. Journal of Clinical Medicine. 2024; 13(12):3569. https://doi.org/10.3390/jcm13123569
Chicago/Turabian StyleDybko, Jarosław, Małgorzata Sobczyk-Kruszelnicka, Alicja Sadowska-Klasa, Agnieszka Piekarska, Sebastian Makuch, Siddarth Agrawal, Krzysztof Dudek, Ugo Giordano, Sebastian Giebel, and Lidia Gil. 2024. "Optimizing Outcomes in Mismatched Unrelated Donor Allogeneic Transplantation: Post-Transplant Cyclophosphamide’s Dual Impact on Graft versus Host Disease Incidence and Overall Survival: Retrospective Analysis on Behalf of Polish Adult Leukemia Group" Journal of Clinical Medicine 13, no. 12: 3569. https://doi.org/10.3390/jcm13123569
APA StyleDybko, J., Sobczyk-Kruszelnicka, M., Sadowska-Klasa, A., Piekarska, A., Makuch, S., Agrawal, S., Dudek, K., Giordano, U., Giebel, S., & Gil, L. (2024). Optimizing Outcomes in Mismatched Unrelated Donor Allogeneic Transplantation: Post-Transplant Cyclophosphamide’s Dual Impact on Graft versus Host Disease Incidence and Overall Survival: Retrospective Analysis on Behalf of Polish Adult Leukemia Group. Journal of Clinical Medicine, 13(12), 3569. https://doi.org/10.3390/jcm13123569