
Monoclonal Anti-PCSK9 Antibodies: Real-World Data

 ,
,
Abstract
1. Introduction
2. Materials and Methods
- Asymptomatic HeFH with LDL-C levels ≥ 130 mg/dL despite at least 6 months of treatment with a high-intensity statin at the highest tolerated dose in combination with ezetimibe, or with demonstrated statin and/or ezetimibe intolerance;
- Known ASCVD with LDL-C levels ≥ 70 mg/dL (≥100 mg/dL until 15 June 2022) despite at least 6 months of treatment with a high-intensity statin at the highest tolerated dose in combination with ezetimibe or with demonstrated statin and/or ezetimibe intolerance or after a single LDL-C detection in cases of recent acute myocardial infarction (within the last 12 months) or multiple cardiovascular events;
- Diabetes mellitus (DM) with target organ damage or an additional major risk factor and LDL-C levels ≥ 70 mg/dL despite at least 6 months of treatment with a high-intensity statin at the highest tolerated dose in combination with ezetimibe, or with demonstrated statin and/or ezetimibe intolerance.
Staistical Analysis
3. Results
3.1. Baseline Characteristics
3.1.1. High-CV-Risk Patients
3.1.2. Very-High-Risk Patients
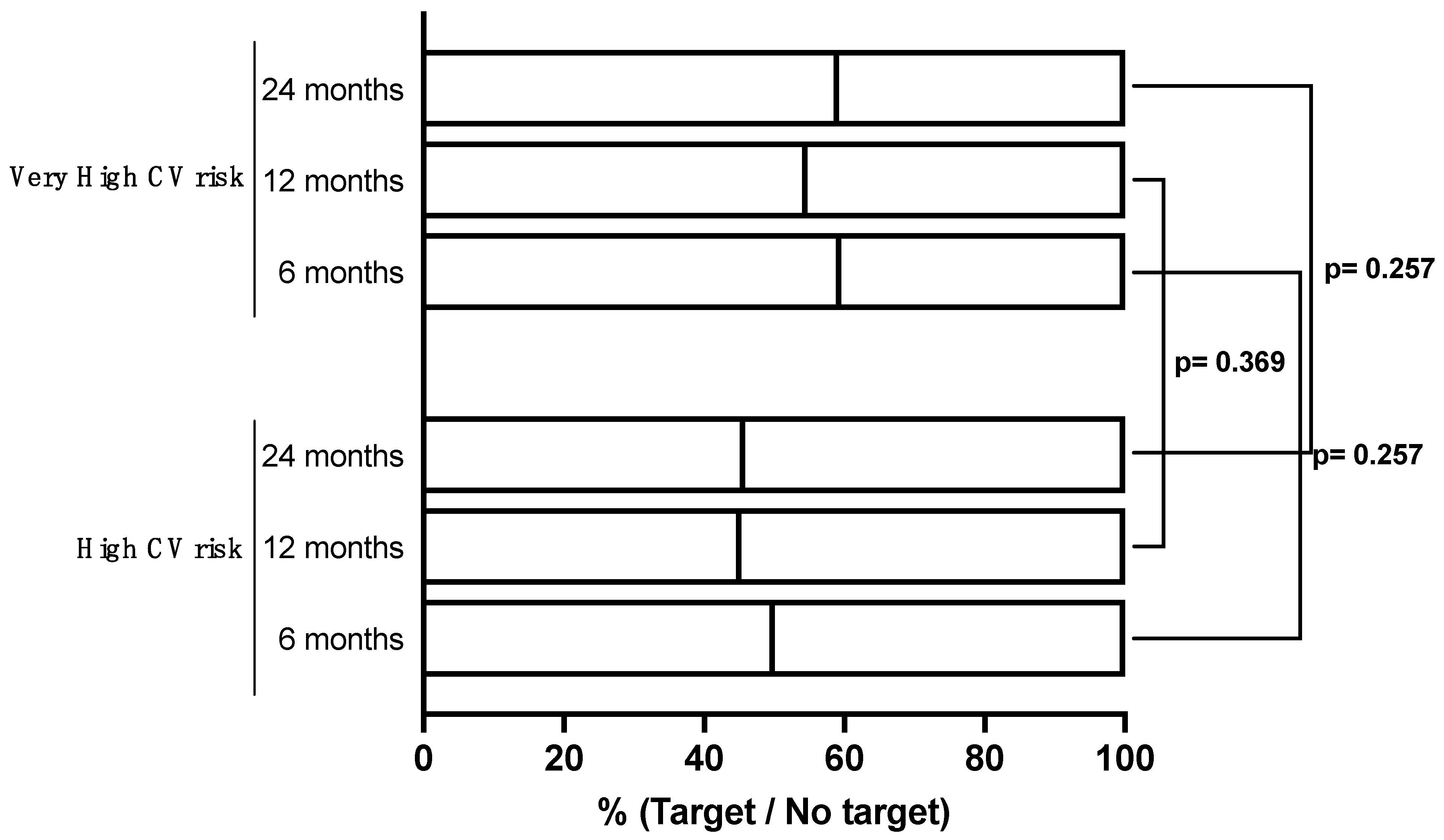
3.2. Follow-Up: Efficacy
3.2.1. High-CV-Risk Patients
3.2.2. Very-High-Risk Patients
3.3. Predictors of LDL-C Target Achievement
3.3.1. High-CV-Risk Patients
3.3.2. Very-High-Risk Patients
3.4. Safety
3.4.1. High-CV-Risk Patients
3.4.2. Very-High-Risk Patients
4. Discussion
- In our cohort, which included patients at high and very high cardiovascular risk, nearly 60% of patients demonstrated full adherence to the ESC Guidelines’ recommendations after one year of PCSK9mAb treatment. This was defined as achieving at least a 50% reduction in LDL-C levels along with reaching the LDL-C target levels based on the cardiovascular risk classification (≤55 and ≤70 mg/dL respectively).
- A background oral LLT involving a high-dose statin emerged as the primary predictor of LDL-C target attainment.
- HeFH and statin intolerance were associated with a significantly lower probability of achieving LDL-C target levels. Unexpectedly, female gender also emerged as a negative predictive factor for a favorable treatment response.
- We reaffirmed the high levels of adherence to these treatments in a real-world setting.
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fan, J.; Watanabe, T. Atherosclerosis: Known and unknown. Pathol. Int. 2022, 72, 151–160. [Google Scholar] [CrossRef]
- Silverman, M.G.; Ference, B.A.; Im, K.; Wiviott, S.D.; Giugliano, R.P.; Grundy, S.M.; Braunwald, E.; Sabatine, M.S. Association Between Lowering LDL-C and Cardiovascular Risk Reduction Among Different Therapeutic Interventions: A Systematic Review and Meta-Analysis. JAMA 2016, 316, 1289–1297. [Google Scholar] [CrossRef]
- Marston, N.A.; Giugliano, R.P.; Melloni, G.E.M.; Park, J.-G.; Morrill, V.; Blazing, M.A.; Ference, B.; Stein, E.; Stroes, E.S.; Braunwald, E.; et al. Association of Apolipoprotein B-Containing Lipoproteins and Risk of Myocardial Infarction in Individuals with and Without Atherosclerosis: Distinguishing Between Particle Concentration, Type, and Content. JAMA Cardiol. 2022, 7, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Ference, B.A.; Ginsberg, H.N.; Graham, I.; Ray, K.K.; Packard, C.J.; Bruckert, E.; Hegele, R.A.; Krauss, R.M.; Raal, F.J.; Schunkert, H.; et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur. Heart J. 2017, 38, 2459–2472. [Google Scholar] [CrossRef]
- Cholesterol Treatment Trialists’ (CTT) Collaborators. Efficacy and safety of cholesterol-lowering treatment: Prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 2005, 366, 1267–1278. [Google Scholar] [CrossRef] [PubMed]
- Catapano, A.L.; Graham, I.; De Backer, G.; Wiklund, O.; Chapman, M.J.; Drexel, H.; Hoes, A.W.; Jennings, C.S.; Landmesser, U.; Pedersen, T.R.; et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias. Eur. Heart J. 2016, 37, 2999–3058. [Google Scholar] [CrossRef]
- Authors/Task Force Members; ESC Committee for Practice Guidelines (CPG); ESC National Cardiac Societies. 2019 ESC/EAS guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Atherosclerosis 2019, 290, 140–205. [Google Scholar] [CrossRef]
- Ray, K.K.; Molemans, B.; Schoonen, W.M.; Giovas, P.; Bray, S.; Kiru, G.; Murphy, J.; Banach, M.; De Servi, S.; Gaita, D.; et al. EU-Wide Cross-Sectional Observational Study of Lipid-Modifying Therapy Use in Secondary and Primary Care: The DA VINCI study. Eur. J. Prev. Cardiol. 2021, 28, 1279–1289. [Google Scholar] [CrossRef] [PubMed]
- Ferrieres, J.; De Ferrari, G.M.; Hermans, M.P.; Elisaf, M.; Toth, P.P.; Horack, M.; Brudi, P.; Lautsch, D.; Bash, L.D.; Baxter, C.A.; et al. Predictors of LDL-cholesterol target value attainment differ in acute and chronic coronary heart disease patients: Results from DYSIS II Europe. Eur. J. Prev. Cardiol. 2018, 25, 1966–1976. [Google Scholar] [CrossRef]
- Gitt, A.K.; Lautsch, D.; Ferrieres, J.; Kastelein, J.; Drexel, H.; Horack, M.; Brudi, P.; Vanneste, B.; Bramlage, P.; Chazelle, F.; et al. Low-density lipoprotein cholesterol in a global cohort of 57,885 statin-treated patients. Atherosclerosis 2016, 255, 200–209. [Google Scholar] [CrossRef]
- De Backer, G.; Jankowski, P.; Kotseva, K.; Mirrakhimov, E.; Reiner, Ž.; Rydén, L.; Tokgözoğlu, L.; Wood, D.; De Bacquer, D.; EUROASPIRE V Collaborators; et al. Management of dyslipidaemia in patients with coronary heart disease: Results from the ESC-EORP EUROASPIRE V survey in 27 countries. Atherosclerosis 2019, 285, 135–146. [Google Scholar] [CrossRef] [PubMed]
- Berteotti, M.; Profili, F.; Nreu, B.; Casolo, G.; Zuppiroli, A.; Mannucci, E.; Marcucci, R.; Francesconi, P. LDL-cholesterol target levels achievement in high-risk patients: An (un)expected gender bias. Nutr. Metab. Cardiovasc. Dis. 2024, 34, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Gazzetta Ufficiale. Consultato. 2022. Available online: https://www.gazzettaufficiale.it/eli/gu/2022/06/15/138/sg/html (accessed on 20 June 2022).
- Schwartz, G.G.; Steg, P.G.; Szarek, M.; Bhatt, D.L.; Bittner, V.A.; Diaz, R.; Edelberg, J.M.; Goodman, S.G.; Hanotin, C.; Harrington, R.A.; et al. Alirocumab and Cardiovascular Outcomes after Acute Coronary Syndrome. N. Engl. J. Med. 2018, 379, 2097–2107. [Google Scholar] [CrossRef] [PubMed]
- Sabatine, M.S.; Giugliano, R.P.; Keech, A.C.; Honarpour, N.; Wiviott, S.D.; Murphy, S.A.; Kuder, J.F.; Wang, H.; Liu, T.; Wasserman, S.M.; et al. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N. Engl. J. Med. 2017, 376, 1713–1722. [Google Scholar] [CrossRef]
- Grześk, G.; Dorota, B.; Wołowiec, Ł.; Wołowiec, A.; Osiak, J.; Kozakiewicz, M.; Banach, J. Safety of PCSK9 inhibitors. Biomed. Pharmacother. 2022, 156, 113957. [Google Scholar] [CrossRef] [PubMed]
- Echevarría, A.B.; Díaz, J.D.D.G.; Caixas, A.; Gil, N.P.; Corral, M.Á.R.; Bridges, I.; Dhalwani, N.; Menchen, S.G.; Ray, K.K. Long-term treatment persistence and maintained reduction of LDL-cholesterol levels with evolocumab over 30 months: Results from the Spanish cohort of the European prospective HEYMANS study. Clínica Investig. Arteriosclerosis 2023, 35, 263–271. [Google Scholar] [CrossRef]
- Gargiulo, P.; Basile, C.; Cesaro, A.; Marzano, F.; Buonocore, D.; Asile, G.; Abbate, V.; Vicidomini, F.; Paolillo, S.; Spaccarotella, C.A.M.; et al. Efficacy, safety, adherence and persistence of PCSK9 inhibitors in clinical practice: A single country, multicenter, observational study (AT-TARGET-IT). Atherosclerosis 2023, 366, 32–39. [Google Scholar] [CrossRef]
- Ray, K.K.; Haq, I.; Bilitou, A.; Manu, M.C.; Burden, A.; Aguiar, C.; Arca, M.; Connolly, D.L.; Eriksson, M.; Ferrières, J.; et al. Treatment gaps in the implementation of LDL cholesterol control among high- and very high-risk patients in Europe between 2020 and 2021: The multinational observational SANTORINI study. Lancet Reg. Health Eur. 2023, 29, 100624. [Google Scholar] [CrossRef]
- Blanco-Ruiz, M.; Amaya-Pascasio, L.; Chacón, R.d.T.; Soria, M.J.Á.; Arjona-Padillo, A.; Bailén, M.M.C.; Pinilla, R.M.; Ortega, I.P.; Rodríguez, B.S.; Zumárraga, L.A.; et al. Effectiveness and safety of PCSK9 inhibitors in real-world clinical practice. An observational multicentre study. The IRIS-PCSK9I study. Atheroscler. Plus 2021, 45, 32–38. [Google Scholar] [CrossRef]
- Hollstein, T.; Kassner, U.; Grenkowitz, T.; Schumann, F.; Bobbert, T.; Steinhagen-Thiessen, E. PCSK9 Inhibitors in a German Single-Center Clinical Practice: Real-World Treatment of Patients at High Cardiovascular Risk Over 68 Weeks. Am. J. Cardiovasc. Drugs 2021, 21, 83–92. [Google Scholar] [CrossRef]
- Gayoso-Rey, M.; Díaz-Trastoy, O.; Romero-Ventosa, E.Y.; García-Beloso, N.; González-Freire, L.; Lorenzo-Lorenzo, K.; Mantiñán-Gil, B.; Palmeiro-Carballeira, R.; Bravo-Amaro, M.; López-Gil-Otero, M.d.M.; et al. Effectiveness, Safety, and Adherence to Treatment of Proprotein Convertase Subtilisin/Kexin Type 9 Inhibitors in Real Practice. Clin. Ther. 2021, 43, e111–e121. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.G.; Farnier, M.; Krempf, M.; Bergeron, J.; Luc, G.; Averna, M.; Stroes, E.S.; Langslet, G.; Raal, F.J.; El Shahawy, M.; et al. Efficacy and Safety of Alirocumab in Reducing Lipids and Cardiovascular Events. N. Engl. J. Med. 2015, 372, 1489–1499. [Google Scholar] [CrossRef] [PubMed]
- Altschmiedová, T.; Todorovová, V.; Šnejdrlová, M.; Šatný, M.; Češka, R. PCSK9 Inhibitors in Real-world Practice: Analysis of Data from 314 Patients and 2 Years of Experience in a Center of Preventive Cardiology. Curr. Atheroscler. Rep. 2022, 24, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Vicente-Valor, J.; García-González, X.; Ibáñez-García, S.; Durán-García, M.E.; de Lorenzo-Pinto, A.; Rodríguez-González, C.; Méndez-Fernández, I.; Percovich-Hualpa, J.C.; Herranz-Alonso, A.; Sanjurjo-Sáez, M. PCSK9 inhibitors revisited: Effectiveness and safety of PCSK9 inhibitors in a real-life Spanish cohort. Biomed. Pharmacother. 2022, 146, 112519. [Google Scholar] [CrossRef] [PubMed]
- O’Donoghue, M.L.; Giugliano, R.P.; Wiviott, S.D.; Atar, D.; Keech, A.C.; Kuder, J.F.; Im, K.; Murphy, S.A.; Flores-Arredondo, J.H.; López, J.A.G.; et al. Long-Term Evolocumab in Patients with Established Atherosclerotic Cardiovascular Disease. Circulation 2022, 146, 1109–1119. [Google Scholar] [CrossRef] [PubMed]
- Toth, P.P.; Bray, S.; Villa, G.; Palagashvili, T.; Sattar, N.; Stroes, E.S.G.; Worth, G.M. Network Meta-Analysis of Randomized Trials Evaluating the Comparative Efficacy of Lipid-Lowering Therapies Added to Maximally Tolerated Statins for the Reduction of Low-Density Lipoprotein Cholesterol. J. Am. Heart Assoc. 2022, 11, e025551. [Google Scholar] [CrossRef] [PubMed]
- Toth, P.P.; Granowitz, C.; Hull, M.; Anderson, A.; Philip, S. Long-term statin persistence is poor among high-risk patients with dyslipidemia: A real-world administrative claims analysis. Lipids Health Dis. 2019, 18, 175. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Ding, L.; Devera, J.; Magee, G.A.; Garg, P.K. Prescribing of Statins After Lower Extremity Revascularization Procedures in the US. JAMA Netw. Open 2021, 4, e2136014. [Google Scholar] [CrossRef]
- Vatcheva, K.P.; Aparicio, V.; Araya, A.; Gonzalez, E.; Laing, S.T. Statin Prescription for Patients with Atherosclerotic Cardiovascular Disease from National Survey Data. Am. J. Cardiol. 2019, 124, 1–7. [Google Scholar] [CrossRef]
- Patti, G.; Cavallari, I.; Cesaro, A.; Gragnano, F.; Riva, L.; Fimiani, F.; Cuccia, C.; Fresco, C.; Calabrò, P.; Leonardi, S.; et al. Use of bempedoic acid for LDL cholesterol lowering and cardiovascular risk reduction: A consensus document from the Italian study group on atherosclerosis, thrombosis and vascular biology. Vascul. Pharmacol. 2023, 148, 107137. [Google Scholar] [CrossRef]
- Arca, M.; Celant, S.; Olimpieri, P.P.; Colatrella, A.; Tomassini, L.; D’Erasmo, L.; Averna, M.; Zambon, A.; Catapano, A.L.; Russo, P. Real-World Effectiveness of PCSK9 Inhibitors in Reducing LDL-C in Patients with Familial Hypercholesterolemia in Italy: A Retrospective Cohort Study Based on the AIFA Monitoring Registries. J. Am. Heart Assoc. 2023, 12, e026550. [Google Scholar] [CrossRef]
- Schreuder, M.M.; Hamkour, S.; Siegers, K.; Holven, K.; Johansen, A.; van de Ree, M.; Imholz, B.; Boersma, E.; Louters, L.; Bogsrud, M.; et al. LDL cholesterol targets rarely achieved in familial hypercholesterolemia patients: A sex and gender-specific analysis. Atherosclerosis 2023, 384, 117117. [Google Scholar] [CrossRef] [PubMed]
- Rachamin, Y.; Grischott, T.; Rosemann, T.; Meyer, M.R. Inferior control of low-density lipoprotein cholesterol in women is the primary sex difference in modifiable cardiovascular risk: A large-scale, cross-sectional study in primary care. Atherosclerosis 2021, 324, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Hyun, K.K.; Redfern, J.; Patel, A.; Peiris, D.; Brieger, D.; Sullivan, D.; Harris, M.; Usherwood, T.; MacMahon, S.; Lyford, M.; et al. Gender inequalities in cardiovascular risk factor assessment and management in primary healthcare. Heart 2017, 103, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Cordero, A.; del Olmo, M.R.F.; Quiroga, G.A.C.; Romero-Menor, C.; Fácila, L.; Seijas-Amigo, J.; Fornovi, A.; Murillo, J.R.; Rodríguez-Mañero, M.; Mora, M.C.B.; et al. Sex Differences in Low-Density Lipoprotein Cholesterol Reduction with PCSK9 Inhibitors in Real-world Patients: The LIPID-REAL Registry. J. Cardiovasc. Pharmacol. 2022, 79, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Schoen, M.W.; Tabak, R.G.; Salas, J.; Scherrer, J.F.; Buckhold, F.R. Comparison of Adherence to Guideline-Based Cholesterol Treatment Goals in Men Versus Women. Am. J. Cardiol. 2016, 117, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.S.; Woodard, L.D.; Ramsey, D.J.; Urech, T.H.; Akeroyd, J.M.; Shah, T.; Deswal, A.; Bozkurt, B.; Ballantyne, C.M.; Petersen, L.A. Gender disparities in evidence-based statin therapy in patients with cardiovascular disease. Am. J. Cardiol. 2015, 115, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Karalis, D.G.; Wild, R.A.; Maki, K.C.; Gaskins, R.; Jacobson, T.A.; Sponseller, C.A.; Cohen, J.D. Gender differences in side effects and attitudes regarding statin use in the Understanding Statin Use in America and Gaps in Patient Education (USAGE) study. J. Clin. Lipidol. 2016, 10, 833–841. [Google Scholar] [CrossRef] [PubMed]
- Hsue, P.Y.; Bittner, V.A.; Betteridge, J.; Fayyad, R.; Laskey, R.; Wenger, N.K.; Waters, D.D. Impact of female sex on lipid lowering, clinical outcomes, and adverse effects in atorvastatin trials. Am. J. Cardiol. 2015, 115, 447–453. [Google Scholar] [CrossRef]
- Goldstein, K.M.; Zullig, L.L.; Bastian, L.A.; Bosworth, H.B. Statin Adherence: Does Gender Matter? Curr. Atheroscler. Rep. 2016, 18, 63. [Google Scholar] [CrossRef]
- Lewey, J.; Shrank, W.H.; Bowry, A.D.K.; Kilabuk, E.; Brennan, T.A.; Choudhry, N.K. Gender and racial disparities in adherence to statin therapy: A meta-analysis. Am. Heart J. 2013, 165, 665–678e1. [Google Scholar] [CrossRef] [PubMed]
- Jia, F.; Fei, S.-F.; Tong, D.-B.; Xue, C.; Li, J.-J. Sex difference in circulating PCSK9 and its clinical implications. Front. Pharmacol. 2022, 13, 953845. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Variables | Overall n = 256 | High Risk, n = 53 | Very High Risk, n = 203 | p * | |
|---|---|---|---|---|---|
| Demographical characteristics | Women, n (%) | 95 (37.1) | 33 (62.3) | 62 (30.5) | <0.001 * |
| Age (years old), mean ± DS | 65.43 ± 11.12 | 59.12 ± 13.65 | 67.11 ± 9.67 | <0.001 * | |
| Cardiovascular risk factors | Smokers, n (%) | 28 (10.9) | 6 (11.3) | 22 (10.8) | 0.920 |
| Ex smokers, n (%) | 114 (44.5) | 15 (28.3) | 99 (48.8) | 0.008 * | |
| Hypertension, n (%) | 160 (62.5) | 19 (35.8) | 140 (69) | <0.001 * | |
| T2DM, n (%) | 31 (12.1) | 0 (0) | 31 (15.3) | 0.002 * | |
| Family history of ASCVD, n (%) | 118 (46.3) | 22 (41.5) | 96 (47.5) | 0.435 | |
| Hyperuricemia, n (%) | 5 (2) | 0 (0) | 5 (2.5) | 0.247 | |
| CAD | AMI, n (%) | 100 (39.1) | / | 100 (49.3) | / |
| Unstable angina, n (%) | 26 (10.2) | / | 26 (12.8) | / | |
| Stable angina, n (%) | 68 (26.6) | / | 68 (33.5) | / | |
| PCI, n (%) | 141 (55.1) | / | 141 (69.5) | / | |
| CABG, n (%) | 27 (10) | / | 27 (13.3) | / | |
| Others ASCVD | Stroke/TIA, n (%) | 20 (7.8) | / | 20 (9.9) | / |
| Carotid disease, n (%) | 18 (7) | / | 18 (8.9) | / | |
| PAD, n (%) | 35 (13.7) | / | 35 (17.2) | / | |
| Carotid revascularization, n (%) | 19 (7.4) | / | 19 (9.4) | / | |
| Peripheral revascularization, n (%) | 11 (4.3) | / | 11 (5.4) | / | |
| Comorbidities | Heart failure, n (%) | 10 (3.9) | 1 (1.9) | 9 (4.4) | 0.395 |
| Chronic kidney disease, n (%) | 5 (2) | 0 (0) | 5 (2.5) | 0.249 | |
| Dyslipidemia type | HeFH, n (%) | 132 (51.6) | 53 (100) | 76 (37.4) | <0.001 * |
| Non-familial hypercholesterolemia, n (%) | 93 (36.3) | 0 (0) | 93 (45.8) | <0.001 * | |
| Mixed Dyslipidemia, n (%) | 31 (12.1) | 0 (0) | 31 (15.3) | 0.002 * | |
| LLTs | None, n (%) | 40 (15.6) | 15 (28.3) | 25 (12.3) | 0.004 * |
| High dose statin alone, n (%) | 10 (3.9) | 0 (0) | 10 (4.9) | 0.100 | |
| Moderate dose statin alone, n (%) | 2 (0.8) | 0 (0) | 2 (1) | 0.469 | |
| Low dose statin alone, n (%) | 0 (0) | 0 (0) | 0 (0) | 1.000 | |
| Ezetimibe alone, n (%) | 88 (34.4) | 24 (45.3) | 64 (31.5) | 0.061 | |
| High dose statin + ezetimibe, n (%) | 91 (35.5) | 9 (17) | 82 (40.4) | 0.002 * | |
| Moderate dose statin + ezetimibe, n (%) | 22 (8.6) | 4 (7.5) | 18 (8.9) | 0.761 | |
| Low dose statin + ezetimibe, n (%) | 3 (1.2) | 1 (1.9) | 2 (1) | 0.588 | |
| Statin Intolerance, n (%) | 146 (57) | 40 (75.5) | 106 (52.2) | 0.002 * | |
| PCSK9i type and dose | Repatha 140 mg, n (%) | 137 (53.5) | 19 (35.8) | 118 (58.1) | 0.004 * |
| Praluent 150 mg, n (%) | 97 (37.9) | 28 (52.8) | 69 (34) | 0.012 * | |
| Praluent 75 mg, n (%) | 23 (9) | 6 (11.3) | 17 (8.4) | 0.505 | |
| Visit | Overall, Mean ± DS | High CV Risk, Median ± DS | Very High CV Risk, Median ± DS | p |
|---|---|---|---|---|
| Baseline | 144.59 ± 52.58 | 185.27 ± 45.45 | 133.21 ± 48.73 | <0.001 * |
| 6 month | 59.57 ± 37.56 | 76.79 ± 42.38 | 54.74 ± 34.7 | <0.001 * |
| 12 month | 63.47 ± 38.88 | 82.73 ± 41.15 | 57.89 ± 36.44 | <0.001 * |
| 24 month | 61.38 ± 41.76 | 77.21± 33.32 | 57.5 ± 42.83 | 0.002 * |
| LDL-C Goal of <1.4 mmol/L (<55 mg/dL) | ||||
|---|---|---|---|---|
| Visit | Overall, n (%) | High CV Risk, n (%) | Very High CV Risk, n (%) | p |
| 6 month (n = 256) | 147 (57.4%) | 28 (50%) | 119 (59.5%) | 0.204 |
| 12 month (n = 245) | 129 (52.7%) | 24 (45.3%) | 105 (54.7%) | 0.128 |
| 24 month (n = 122) | 69 (56.6%) | 11 (45.8%) | 58 (59.2%) | 0.237 |
| ≥50% LDL-C reduction from baseline | ||||
| 6 month (n = 256) | 178 (69.5%) | 42 (79.2%) | 136 (67.0%) | 0.314 |
| 12 month (n = 245) | 164 (66.9%) | 36 (67.9) | 128 (66.7%) | 0.790 |
| 24 month (n = 122) | 89 (72.9%) | 16 (66.7%) | 73 (74.5%) | 0.439 |
| ≥50% LDL-C reduction from baseline and an LDL-C goal of <1.4 mmol/L (<55 mg/dL) | ||||
| 6 month (n = 256) | 144 (56.3%) | 28 (52.8%) | 116 (57.1%) | 0.286 |
| 12 month (n = 245) | 126 (51.5%) | 22 (41.5%) | 104 (54.2%) | 0.054 |
| 24 month (n = 122) | 68 (55.8%) | 11 (45.8%) | 57 (58.2%) | 0.276 |
| Very High CV Risk | High CV Risk | |||||
|---|---|---|---|---|---|---|
| Variables | IRR | 95% C.I. | p | IRR | 95% C.I. | p |
| Female gender | 0.465 | 0.25–0.88 | 0.018 * | 0.667 | 0.22–2.02 | 0.473 |
| Smokers | 0.968 | 0.39–2.36 | 0.943 | 2.9 | 0.48–17.38 | 0.244 |
| Ex-smokers | 1.361 | 0.77–2.42 | 0.293 | 1.184 | 0.36–3.9 | 0.782 |
| Hypertension | 1.833 | 0.98–3.4 | 0.055 | 1.538 | 0.52–4.57 | 0.438 |
| T2DM | 1.631 | 0.69–3.87 | 0.267 | 0.000 | 0 | 0.999 |
| Family history of ASCVD | 0.805 | 0.45–1.43 | 0.460 | 1.385 | 0.47–4.05 | 0.552 |
| CAD | 2.543 | 1.17–5.53 | 0.019 * | / | / | / |
| Stroke/TIA | 1.033 | 0.4–2.65 | 0.652 | / | / | / |
| PAD | 0.895 | 0.46–1.74 | 0.649 | / | / | / |
| Peripheral revascularization | 2.343 | 0.89–6.16 | 0.052 | / | / | / |
| HEFH | 0.691 | 0.39–1.23 | 0.078 | / | / | / |
| Non-familial hypercholesterolemia | 1.383 | 0.78–2.45 | 0.168 | / | / | / |
| Mixed Dyslipidemia | 0.932 | 0.43–2.03 | 0.817 | / | / | / |
| Statin Intolerance | 0.409 | 0.23–0.74 | 0.003 * | 0.321 | 0.09–1.135 | 0.078 |
| At least one LLT | 2.157 | 1.08–4.34 | 0.031 * | 4.154 | 1.29–13.35 | 0.017 * |
| Statin + ezetimibe | 2.102 | 1.14–3.89 | 0.018 * | 3.111 | 0.68–14.04 | 0.140 |
| High dose statin | 2.890 | 1.41–5.91 | 0.004 * | 7.895 | 0.86–72.88 | 0.068 |
| High dose statin + ezetimibe | 2.321 | 1.1–4.89 | 0.027 * | 0.221 | 0.42–44.1 | 0.221 |
| Very High CV Risk | High CV Risk | |||||
|---|---|---|---|---|---|---|
| Variables | IRR | 95% C.I. | p | IRR | 95% C.I. | p |
| Female gender | 0.473 | 0.24–0.94 | 0.033 * | / | / | / |
| Hypertension | 2.025 | 1–4.1 | 0.050 * | / | / | / |
| HEFH | 0.484 | 0.25–0.96 | 0.037 * | / | / | / |
| Statin Intolerance | 0.484 | 0.23–1.01 | 0.055 * | / | / | / |
| At least one LLT | / | / | / | 4.154 | 1.29–12.35 | 0.013 * |
| High dose statin | 3.244 | 1.27–8.27 | 0.014 * | / | / | / |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guidotti, G.; Liberati, V.; Sorrentino, A.; Lotti, E.; Crudele, F.; Rogolino, A.; Sammartino, A.; Slanzi, M.; Gori, A.M.; Marcucci, R.; et al. Monoclonal Anti-PCSK9 Antibodies: Real-World Data. J. Clin. Med. 2024, 13, 4543. https://doi.org/10.3390/jcm13154543
Guidotti G, Liberati V, Sorrentino A, Lotti E, Crudele F, Rogolino A, Sammartino A, Slanzi M, Gori AM, Marcucci R, et al. Monoclonal Anti-PCSK9 Antibodies: Real-World Data. Journal of Clinical Medicine. 2024; 13(15):4543. https://doi.org/10.3390/jcm13154543
Chicago/Turabian StyleGuidotti, Giulia, Viola Liberati, Andrea Sorrentino, Elena Lotti, Felice Crudele, Angela Rogolino, Aniello Sammartino, Margherita Slanzi, Anna Maria Gori, Rossella Marcucci, and et al. 2024. "Monoclonal Anti-PCSK9 Antibodies: Real-World Data" Journal of Clinical Medicine 13, no. 15: 4543. https://doi.org/10.3390/jcm13154543
APA StyleGuidotti, G., Liberati, V., Sorrentino, A., Lotti, E., Crudele, F., Rogolino, A., Sammartino, A., Slanzi, M., Gori, A. M., Marcucci, R., & Berteotti, M. (2024). Monoclonal Anti-PCSK9 Antibodies: Real-World Data. Journal of Clinical Medicine, 13(15), 4543. https://doi.org/10.3390/jcm13154543