
Chronic Right Ventricular Pacing Post-Transcatheter Aortic Valve Replacement Attenuates the Benefit on Left Ventricular Function
 , and
, and
Abstract
:1. Background/Introduction
2. Methods
2.1. Study Design
2.2. Patient Cohort
2.3. Two-Dimensional Transthoracic Echocardiography and Speckle-Tracking Strain Imaging
2.4. ECG/Pacemaker Data
2.5. Clinical Outcomes
2.6. Statistical Analysis
3. Results
3.1. Patient Cohort
3.2. ECG/Pacemaker Data
3.3. Two-Dimensional Transthoracic Echocardiography and Speckle-Tracking Strain Imaging
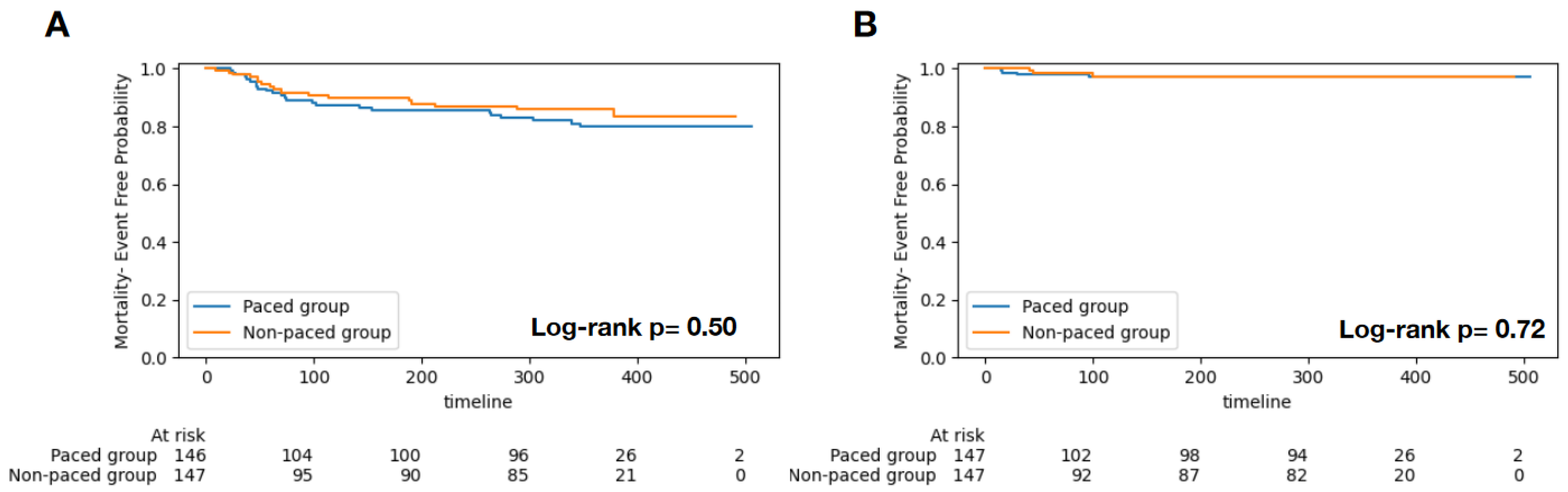
3.4. Clinical Outcomes
4. Discussion
4.1. Impact of Chronic Pacing on TAVI Patients
4.2. The Effect of Chronic RV Pacing on Clinical Outcomes
4.3. The Effect of Chronic RV Pacing on LV Function
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| STS: | Society of Thoracic Surgeons |
| SAVR: | surgical aortic valve replacement |
| TAVI: | transcatheter aortic valve implantation |
| RV: | right ventricular |
| TTE: | transthoracic echocardiography |
| HFH: | heart failure hospitalization |
| PPM: | permanent pacemaker |
| ICD: | implantable cardioverter-defibrillator |
| DDD/DDDR: | pacing mode |
| VVI/VVIR: | pacing mode |
References
- Saad, A.M.; Kassis, N.; Isogai, T.; Gad, M.M.; Ahuja, K.R.; Abdelfattah, O.; Shekhar, S.; Farwati, M.; Yun, J.J.; Krishnaswamy, A.; et al. Trends in Outcomes of Transcatheter and Surgical Aortic Valve Replacement in the United States (2012–2017). Am. J. Cardiol. 2021, 141, 79–85. [Google Scholar] [CrossRef]
- Winter, M.-P.; Bartko, P.; Hofer, F.; Zbiral, M.; Burger, A.; Ghanim, B.; Kastner, J.; Lang, I.M.; Mascherbauer, J.; Hengstenberg, C.; et al. Evolution of outcome and complications in TAVR: A meta-analysis of observational and randomized studies. Sci. Rep. 2020, 10, 15568. [Google Scholar] [CrossRef] [PubMed]
- Nazif, T.M.; Dizon, J.M.; Hahn, R.T.; Xu, K.; Babaliaros, V.; Douglas, P.S.; El-Chami, M.F.; Herrmann, H.C.; Mack, M.; Makkar, R.R.; et al. Predictors and clinical outcomes of permanent pacemaker implantation after transcatheter aortic valve replacement: The PARTNER (Placement of AoRtic TraNscathetER Valves) trial and registry. JACC Cardiovasc. Interv. 2015, 8, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Siontis, G.C.; Jüni, P.; Pilgrim, T.; Stortecky, S.; Büllesfeld, L.; Meier, B.; Wenaweser, P.; Windecker, S. Predictors of Permanent Pacemaker Implantation in Patients with Severe Aortic Stenosis Undergoing TAVR: A Meta-Analysis. J. Am. Coll. Cardiol. 2014, 64, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Fadahunsi, O.O.; Olowoyeye, A.; Ukaigwe, A.; Li, Z.; Vora, A.N.; Vemulapalli, S.; Elgin, E.; Donato, A. Incidence, predictors, and outcomes of permanent pacemaker implantation following transcatheter aortic valve replacement: Analysis from the U.S. Society of Thoracic Surgeons/ American College of Cardiology TVT Registry. JACC Cardiovasc. Interv. 2016, 9, 2189–2199. [Google Scholar] [CrossRef] [PubMed]
- Hamdan, A.; Guetta, V.; Klempfner, R.; Konen, E.; Raanani, E.; Glikson, M.; Goitein, O.; Segev, A.; Barbash, I.; Fefer, P.; et al. Inverse Relationship Between Membranous Septal Length and the Risk of Atrioventricular Block in Patients Undergoing Transcatheter Aortic Valve Implantation. JACC Cardiovasc. Interv. 2015, 8, 1218–1228. [Google Scholar] [CrossRef] [PubMed]
- Tarantini, G.; Mojoli, M.; Purita, P.; Napodano, M.; D’onofrio, A.; Frigo, A.; Covolo, E.; Facchin, M.; Isabella, G.; Gerosa, G.; et al. Unravelling the (arte)fact of increased pacemaker rate with the Edwards SAPIEN 3 valve. EuroIntervention 2015, 11, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Bhardwaj, A.; Ramanan, T.; Sawant, A.C.; Sinibaldi, E.; Pham, M.; Khan, S.; Qureshi, R.; Agrawal, N.; Khalil, C.; Hansen, R.; et al. Quality of life outcomes in transcatheter aortic valve replacement patients requiring pacemaker implantation. J. Arrhythmia 2018, 34, 441–449. [Google Scholar] [CrossRef]
- Buellesfeld, L.; Stortecky, S.; Heg, D.; Hausen, S.; Mueller, R.; Wenaweser, P.; Pilgrim, T.; Gloekler, S.; Khattab, A.A.; Huber, C.; et al. Impact of Permanent Pacemaker Implantation on Clinical Outcome Among Patients Undergoing Transcatheter Aortic Valve Implantation. J. Am. Coll. Cardiol. 2012, 60, 493–501. [Google Scholar] [CrossRef]
- Naqvi, T.Z.; Chao, C.-J. Adverse Effects of Right Ventricular Pacing on Cardiac Function: Prevalence, Prevention and Treatment with Physiologic Pacing. Trends Cardiovasc. Med. 2021, 33, 109–122. [Google Scholar] [CrossRef]
- Urena, M.; Webb, J.G.; Tamburino, C.; Muñoz-García, A.J.; Cheema, A.; Dager, A.E.; Serra, V.; Amat-Santos, I.J.; Barbanti, M.; Immè, S.; et al. Permanent Pacemaker Implantation After Transcatheter Aortic Valve Implantation. Circulation 2014, 129, 1233–1243. [Google Scholar] [CrossRef] [PubMed]
- Chamandi, C.; Barbanti, M.; Munoz-Garcia, A.; Latib, A.; Nombela-Franco, L.; Gutiérrez-Ibanez, E.; Veiga-Fernandez, G.; Cheema, A.N.; Cruz-Gonzalez, I.; Serra, V.; et al. Long-Term Outcomes in Patients with New Permanent Pacemaker Implantation Following Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2018, 11, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Tops, L.F.; Schalij, M.J.; Bax, J.J. The effects of right ventricular apical pacing on ventricular function and dyssynchrony implications for therapy. J. Am. Coll. Cardiol. 2009, 54, 764–776. [Google Scholar] [CrossRef] [PubMed]
- Tops, L.F.; Suffoletto, M.S.; Bleeker, G.B.; Boersma, E.; van der Wall, E.E.; Gorcsan, J.; Schalij, M.J.; Bax, J.J. Speckle-Tracking Radial Strain Reveals Left Ventricular Dyssynchrony in Patients with Permanent Right Ventricular Pacing. J. Am. Coll. Cardiol. 2007, 50, 1180–1188. [Google Scholar] [CrossRef]
- Dawood, M.; Elsharkawy, E.; Abdel-Hay, M.A.; Nawar, M. Predictors of pacing induced left ventricular dysfunction and cardiomyopathy assessed by three-dimensional echocardiography and speckle tracking strain. Egypt. Heart J. 2021, 73, 10. [Google Scholar] [CrossRef] [PubMed]
- Chung, M.K.; Patton, K.K.; Lau, C.-P.; Forno, A.R.J.D.; Al-Khatib, S.M.; Arora, V.; Birgersdotter-Green, U.M.; Cha, Y.-M.; Chung, E.H.; Cronin, E.M.; et al. 2023 HRS/APHRS/LAHRS guideline on cardiac physiologic pacing for the avoidance and mitigation of heart failure. Heart Rhythm 2023, 20, e17–e91. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Bierig, S.M.; Budoff, M.J.; Desai, M.; Dilsizian, V.; Eidem, B.; Goldstein, S.A.; Hung, J.; Maron, M.S.; Ommen, S.R.; et al. American Society of Echocardiography Clinical Recommendations for Multimodality Cardiovascular Imaging of Patients with Hypertrophic Cardiomyopathy Endorsed by the American Society of Nuclear Cardiology, Society for Cardiovascular Magnetic Resonance, and Society of Cardiovascular Computed Tomography. J. Am. Soc. Echocardiogr. 2011, 24, 473–498. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef]
- Sweeney, M.O.; Hellkamp, A.S.; Ellenbogen, K.A.; Greenspon, A.J.; Freedman, R.A.; Lee, K.L.; Lamas, G.A.; Investigators MOST. Adverse effect of ventricular pacing on heart failure and atrial fibrillation among patients with normal baseline QRS duration in a clinical trial of pacemaker therapy for sinus node dysfunction. Circulation 2003, 107, 2932–2937. [Google Scholar] [CrossRef]
- Wilkoff, B.L.; Cook, J.R.; Epstein, A.E.; Greene, H.L.; Hallstrom, A.P.; Hsia, H.; Kutalek, S.P.; Sharma, A. Dual-chamber pacing or ventricular backup pacing in patients with an implantable defibrillator: The Dual Chamber and VVI Implantable Defibrillator (DAVID). Trial. JAMA 2002, 288, 3115–3123. [Google Scholar]
- Steinberg, J.S.; Fischer, A.; Wang, P.; Schuger, C.; Daubert, J.; Mcnitt, S.; Andrews, M.; Brown, M.; Hall, W.J.; Zareba, W.; et al. The clinical implications of cumulative right ventricular pacing in the multicenter automatic defibrillator trial II. J. Cardiovasc. Electrophysiol. 2005, 16, 359–365. [Google Scholar] [CrossRef]
- Bhardwaj, A.; Ramanan, T.; Khalil, C.; Pham, M.; Sinibaldi, E.; Hansen, R.; Baldo, S.; Colern, G.; Sawant, A.C.; Corbelli, J.; et al. Valvuloarterial Impedance Predicts Heart Failure Readmissions in Patients Undergoing Transcatheter Aortic Valve Replacement. Struct. Heart 2017, 1, 277–284. [Google Scholar] [CrossRef]
- Meduri, C.U.; Kereiakes, D.J.; Rajagopal, V.; Makkar, R.R.; O’Hair, D.; Linke, A.; Waksman, R.; Babliaros, V.; Stoler, R.C.; Mishkel, G.J.; et al. Pacemaker Implantation and Dependency After Transcatheter Aortic Valve Replacement in the REPRISE III Trial. J. Am. Heart Assoc. 2019, 8, e012594. [Google Scholar] [CrossRef]
- Mazza, A.; Bendini, M.G.; Leggio, M.; Riva, U.; Ciardiello, C.; Valsecchi, S.; De Cristofaro, R.; Giordano, G. Incidence and predictors of heart failure hospitalization and death in permanent pacemaker patients: A single-centre experience over medium-term follow-up. Europace 2013, 15, 1267–1272. [Google Scholar] [CrossRef]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., III; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2020, 77, e25–e197. [Google Scholar] [CrossRef] [PubMed]
- Gegenava, T.; Vollema, E.M.; van Rosendael, A.; Abou, R.; Goedemans, L.; van der Kley, F.; de Weger, A.; Marsan, N.A.; Bax, J.J.; Delgado, V. Changes in Left Ventricular Global Longitudinal Strain after Transcatheter Aortic Valve Implantation according to Calcification Burden of the Thoracic Aorta. J. Am. Soc. Echocardiogr. 2019, 32, 1058–1066.e2. [Google Scholar] [CrossRef] [PubMed]
- Poulin, F.; Carasso, S.; Horlick, E.M.; Rakowski, H.; Lim, K.-D.; Finn, H.; Feindel, C.M.; Greutmann, M.; Osten, M.D.; Cusimano, R.J.; et al. Recovery of Left Ventricular Mechanics after Transcatheter Aortic Valve Implantation: Effects of Baseline Ventricular Function and Postprocedural Aortic Regurgitation. J. Am. Soc. Echocardiogr. 2014, 27, 1133–1142. [Google Scholar] [CrossRef] [PubMed]
- Eaves, S.; Lipton, J.A. Global longitudinal strain as a risk factor for pacing-induced cardiomyopathy: Another step toward mechanistic insight and prevention strategies. J. Interv. Card. Electrophysiol. 2024, 67, 241–242. [Google Scholar] [CrossRef]
- Algazzar, A.S.; Katta, A.A.; Ahmed, K.S.; Elkenany, N.M.; Ibrahim, M.A. Changes in Left Ventricular Global and Regional Longitudinal Strain During Right Ventricular Pacing. Cardiol. Res. 2016, 7, 17–24. [Google Scholar] [CrossRef]
- Blyakhman, F.A.; Naidich, A.M.; Kolchanova, S.G.; Sokolov, S.Y.; Kremleva, Y.V.; Chestukhin, V.V. Validity of ejection fraction as a measure of myocardial functional state: Impact of asynchrony. Eur. J. Echocardiogr. 2009, 10, 613–618. [Google Scholar] [CrossRef] [PubMed]
- Zile, M.R.; Blaustein, A.S.; Shimizu, G.; Gaasch, W.H. Right ventricular pacing reduces the rate of left ventricular relaxation and filling. J. Am. Coll. Cardiol. 1987, 10, 702–709. [Google Scholar] [CrossRef] [PubMed]
- Orszulak, M.; Filipecki, A.; Wrobel, W.; Berger-Kucza, A.; Orszulak, W.; Urbanczyk-Swic, D.; Kwasniewski, W.; Mizia-Stec, K. Left ventricular global longitudinal strain in predicting CRT response: One more J-shaped curve in medicine. Heart Vessel. 2021, 36, 999–1008. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Non-Pacing Group | Pacing Group | p-Value | |
|---|---|---|---|
| N = 147 | N = 147 | ||
| Patient Demographics | |||
| Age | 81.0 ± 7.3 | 81.2 ± 7.6 | 0.898 |
| Sex (male) | 92 (62.6%) | 82 (55.8%) | 0.235 |
| Race (white) | 142 (96.6%) | 142 (96.6%) | 0.753 |
| STS risk score | 8.5 ± 5.9 | 8.5 ± 7.8 | 0.922 |
| Prior MI | 31 (21.1%) | 31 (21.1%) | 1.000 |
| Prior PCI | 47 (32.0%) | 26 (17.7%) | 0.005 |
| Prior CABG | 45 (30.6%) | 55 (37.4%) | 0.218 |
| Prior Stroke | 14 (9.5%) | 16 (10.9%) | 0.700 |
| Prior PAD | 75 (51.0%) | 80 (54.4%) | 0.559 |
| Current dialysis | 9 (6.1%) | 8 (5.4%) | 0.803 |
| Smoker | 5 (3.4%) | 6 (4.1%) | 0.759 |
| Hypertension | 124 (84.4%) | 128 (87.1%) | 0.505 |
| Diabetes | 60 (40.8%) | 60 (40.8%) | 1.000 |
| Afib/Aflutter | 54 (36.7%) | 62 (42.2%) | 0.340 |
| Pre-TAVR Conduction defect | 61 (41.5%) | 83 (56.5%) | 0.010 |
| Hgb (g/dL) | 12.1 ± 1.9 | 11.8 ± 1.9 | 0.095 |
| Creatinine (mg/dL) | 1.5 ± 1.5 | 1.4 ± 1.1 | 0.423 |
| Medications | |||
| Aspirin | 121 (82.3%) | 122 (83.0%) | 0.999 |
| Beta blocker | 105 (71.4%) | 103 (70.1%) | 0.344 |
| ACE-I | 30 (20.4%) | 26 (17.7%) | 0.809 |
| ARB | 13 (8.8%) | 11 (7.5%) | 0.760 |
| Warfarin | 75 (51.0%) | 89 (60.5%) | 0.256 |
| ECG (baseline) | |||
| Ventricular rate (bpm) | 70.3 ± 14.2 | 73.4 ± 14.9 | 0.051 |
| PR (ms) | 194.2 ± 44.9 | 187.5 ± 43.4 | 0.128 |
| QRS (ms) | 115.6 ± 28.0 | 111.3 ± 26.2 | 0.095 |
| QT (ms) | 427.8 ± 44.6 | 415.6 ± 41.8 | 0.015 |
| QTc (ms) | 456.5 ± 34.6 | 453.3 ± 34.1 | 0.175 |
| RBBB | 26 (17.7%) | 44 (29.9%) | 0.020 |
| LBBB | 13 (8.8%) | 9 (6.1%) | 0.506 |
| Variable AV Block | 2 (1.4%) | 4 (2.7%) | 0.680 |
| 1st Degree AV Block | 27 (18.4%) | 43 (29.3%) | 0.040 |
| 2nd Degree AV Block | 0 (0.0%) | 1 (0.7%) | 1.000 |
| Left Anterior Fascicular Block | 7 (4.8%) | 22 (15.0%) | 0.006 |
| Left Posterior Fascicular Block | 0 (0.0%) | 5 (3.4%) | 0.071 |
| Procedural Outcomes | |||
| Perforation (with or without tamponade) | 1 (1.1%) | 0 (0.0%) | 0.802 |
| Unplanned Vascular Surgery/Intervention | 6 (6.7%) | 0 (0.0%) | 0.006 |
| Unplanned other Cardiac Surgery/Intervention | 1 (1.1%) | 1 (0.7%) | 0.706 |
| Post-TAVI mean AVG (mmHg) | 12.3 ± 6.4 | 10.9 ± 4.7 | 0.049 |
| Pacing Indication(s) | |||
| AVB | -- | 57 (39.9%) | -- |
| Complete AVB | -- | 31 (21.7%) | -- |
| LBBB | -- | 36 (25.2%) | -- |
| Sinus Node Dysfunction | -- | 10 (7.0%) | -- |
| Bradycardia | -- | 6 (4.2%) | -- |
| Bifascicular block | -- | 2 (1.4%) | -- |
| RBBB | -- | 1 (0.7%) | -- |
| Pacing Mode(s) | |||
| DDD/DDDR | -- | 123 (83.1%) | -- |
| VVI/VVIR | -- | 21 (14.2%) | -- |
| Other | -- | 4 (2.8%) | -- |
| Non-Pacing Group | Pacing Group | Two-Group Comparison | ||||||
|---|---|---|---|---|---|---|---|---|
| N = 147 | N = 147 | Baseline | Follow-Up | |||||
| Baseline | Follow-Up | * p-Value | Baseline | Follow-Up | * p-Value | ** p-Value | *** p-Value | |
| LVEF (%) | 53.8 ± 13.9 | 58.8 ± 11.2 | 0.001 | 56.7 ± 10.9 | 57.1 ± 13.0 | 0.775 | 0.455 | 0.308 |
| E/A ratio | 1.0 ± 0.7 | 1.1 ± 0.6 | 0.784 | 1.1 ± 0.6 | 0.9 ± 0.5 | 0.216 | 0.742 | 0.325 |
| Medial e’ (m/s) | 0.05 ± 0.01 | 0.06 ± 0.02 | 0.002 | 0.06 ± 0.1 | 0.05 ± 0.02 | 0.300 | 0.525 | 0.064 |
| Lateral e’ (m/s) | 0.08 ± 0.03 | 0.07 ± 0.02 | <0.001 | 0.06 ± 0.02 | 0.06 ± 0.02 | 0.165 | 0.331 | 0.059 |
| Average E/e’ ratio | 16.2 ± 8.2 | 16.1 ± 9.9 | 0.846 | 18.7 ± 9.8 | 18.9 ± 8.8 | 0.539 | 0.128 | 0.162 |
| LV mass index (g/m2) | 128.0 ± 99.1 | 121.2 ± 30.5 | 0.280 | 119.7 ± 33.7 | 121.2 ± 33.8 | 0.555 | 0.375 | 0.998 |
| RVSP (mmHg) | 40.6 ± 11.8 | 41.5 ± 12.7 | 0.323 | 42.8 ± 14.9 | 43.6 ± 12.6 | 0.562 | 0.167 | 0.309 |
| LV global longitudinal strain (%) | −14.9 ± 4.3 | −18.8 ± 2.7 | <0.0001 | −13.6 ± 3.5 | −12.7 ± 3.5 | 0.021 | 0.008 | <0.0001 |
| LV Regional Apex (%) | −18.5 ± 6.1 | −23.2 ± 9.2 | <0.0001 | −17.1 ± 5.4 | −12.9 ± 5.5 | <0.0001 | 0.069 | <0.0001 |
| LV Regional Mid (%) | −14.6 ± 5.6 | −18.7 ± 3.4 | <0.0001 | −13.2 ± 4.3 | −12.7 ± 4.6 | 0.283 | 0.018 | <0.0001 |
| LV Regional Basal (%) | −12.5 ± 6.3 | −13.0 ± 3.8 | 0.006 | −10.8 ± 4.3 | −12.9 ± 4.1 | 0.009 | 0.137 | 0.260 |
| NYHA Class | Baseline | Follow-Up | ||
|---|---|---|---|---|
| Pacing | Non-Pacing | Pacing | Non-Pacing | |
| I | 8.0 (5.4%) | 4.0 (2.7%) | 108.0 (73.5%) | 109.0 (74.1%) |
| II | 32.0 (21.8%) | 22.0 (15.0%) | 34.0 (23.1%) | 28.0 (19.0%) |
| III | 94.0 (63.9%) | 104.0 (70.7%) | 3.0 (2.0%) | 9.0 (6.1%) |
| IV | 13.0 (8.8%) | 17.0 (11.6%) | 2.0 (1.4%) | 1.0 (0.7%) |
| p-value | 0.238 | 0.270 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chao, C.-J.; Mandale, D.; Farina, J.M.; Abdou, M.; Rattanawong, P.; Girardo, M.; Agasthi, P.; Ayoub, C.; Alkhouli, M.; Eleid, M.; et al. Chronic Right Ventricular Pacing Post-Transcatheter Aortic Valve Replacement Attenuates the Benefit on Left Ventricular Function. J. Clin. Med. 2024, 13, 4553. https://doi.org/10.3390/jcm13154553
Chao C-J, Mandale D, Farina JM, Abdou M, Rattanawong P, Girardo M, Agasthi P, Ayoub C, Alkhouli M, Eleid M, et al. Chronic Right Ventricular Pacing Post-Transcatheter Aortic Valve Replacement Attenuates the Benefit on Left Ventricular Function. Journal of Clinical Medicine. 2024; 13(15):4553. https://doi.org/10.3390/jcm13154553
Chicago/Turabian StyleChao, Chieh-Ju, Deepa Mandale, Juan M. Farina, Merna Abdou, Pattara Rattanawong, Marlene Girardo, Pradyumma Agasthi, Chadi Ayoub, Mohammad Alkhouli, Mackram Eleid, and et al. 2024. "Chronic Right Ventricular Pacing Post-Transcatheter Aortic Valve Replacement Attenuates the Benefit on Left Ventricular Function" Journal of Clinical Medicine 13, no. 15: 4553. https://doi.org/10.3390/jcm13154553