
The Burden of Deep Vein Thrombosis and Risk Factors in Pregnancy and Postpartum—Mirroring Our Region’s Particularities

 , , , and
, , , and
Abstract
1. Introduction
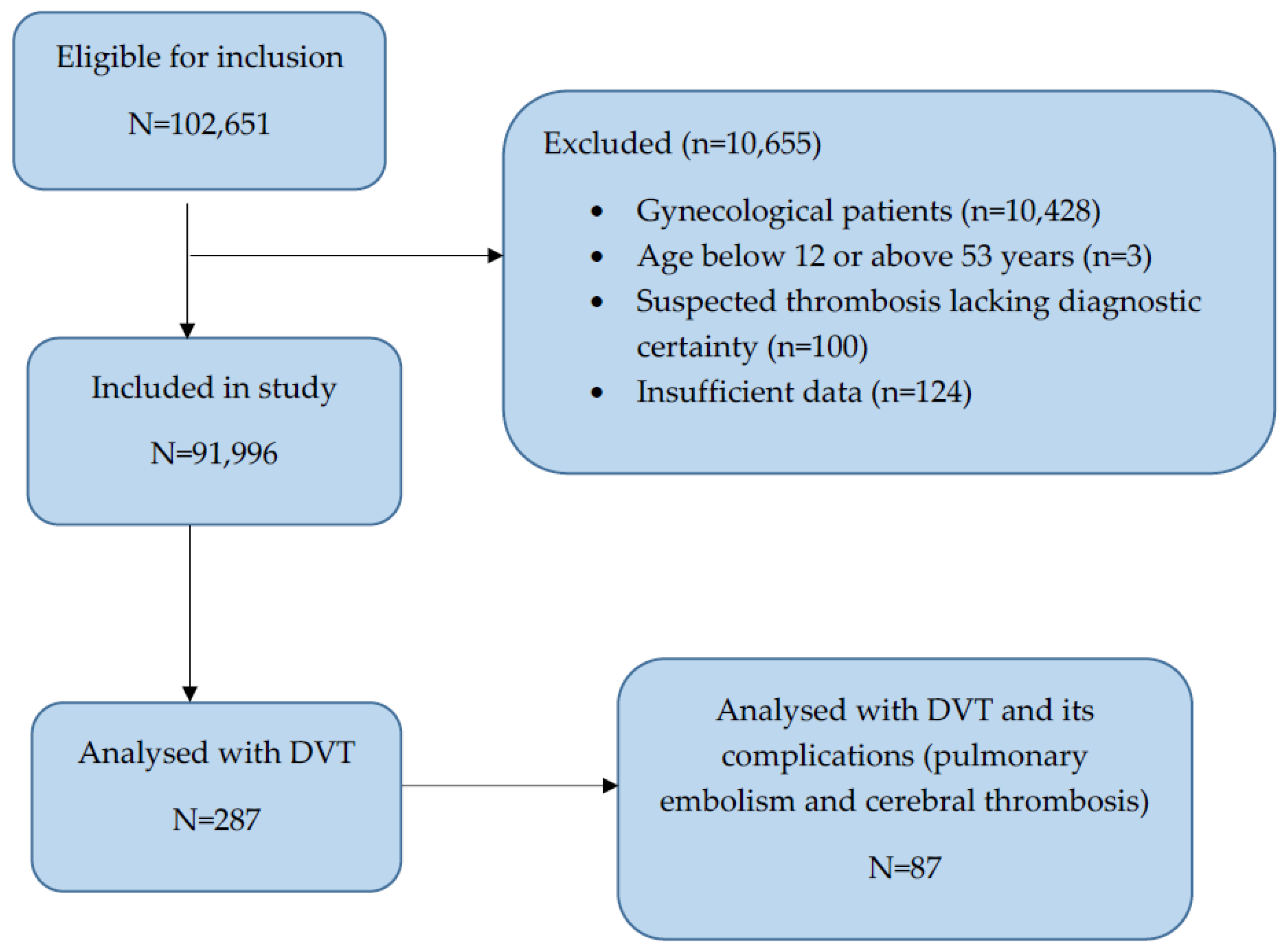
2. Materials and Methods
Statistical Analyses
3. Results
- (a)
- Univariate analysis of the risk for deep vein thrombosis (DVT)
- (b)
- Univariate analysis of the risk for pulmonary thromboembolism
- (c)
- Univariate analysis of the risk for cerebral thromboembolism (CTE)
- (d)
- Multivariate analysis of the risk factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bitsadze, V.; Khizroeva, J.; Alexander, M.; Elalamy, I. Venous thrombosis risk factors in pregnant women. J. Perinat. Med. 2022, 50, 505–518. [Google Scholar] [CrossRef] [PubMed]
- Kyrle, P.A.; Eichinger, S. Deep vein thrombosis. Lancet 2005, 365, 1163–1174. [Google Scholar] [CrossRef] [PubMed]
- Abe, K.; Kuklina, E.V.; Hooper, W.C.; Callaghan, W.M. Venous thromboembolism as a cause of severe maternal morbidity and mortality in the United States. Semin. Perinatol. 2019, 43, 200–204. [Google Scholar] [CrossRef] [PubMed]
- van Lennep, J.E.R.; Nerenberg, K.A. Delivering evidence to prevent recurrent venous thromboembolism in pregnancy. Lancet 2022, 400, 1743–1745. [Google Scholar] [CrossRef] [PubMed]
- Rosendaal, F.R. Causes of venous thrombosis. Thromb. J. 2016, 14, 24. [Google Scholar] [CrossRef] [PubMed]
- Hough, R.E.; Makris, M.E.D.; Preston, F.E. Pregnancy in women with thrombophilia: Incidence of thrombosis and pregnancy outcome. Br. J. Haematol. 1996, 16, 742–748. [Google Scholar]
- James, A.H. Thrombosis in pregnancy and maternal outcomes. Birth Defects Res. Part C Embryo Today: Rev. 2015, 105, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, A.F.; Skjeldestad, F.E.; Sandset, P.M. Incidence and risk patterns of venous thromboembolism in pregnancy and puerperium—A register-based case-control study. Am. J. Obstet. Gynecol. 2008, 198, 233.e1–233.e7. [Google Scholar] [CrossRef] [PubMed]
- Maughan, B.C.; Marin, M.; Han, J.; Gibbins, K.J.; Brixey, A.G.; Caughey, A.B.; Kline, J.A.; Jarman, A.F. Venous Thromboembolism During Pregnancy and the Postpartum Period: Risk Factors, Diagnostic Testing, and Treatment. Obstet. Gynecol. Surv. 2022, 77, 433–444. [Google Scholar] [CrossRef]
- Devis, P.; Knuttinen, M.G. Deep venous thrombosis in pregnancy: Incidence, pathogenesis and endovascular management. Cardiovasc. Diagn. Ther. 2017, 7, S309–S319. [Google Scholar] [CrossRef]
- Levinta, S.; Castravet, I. The pulmonary embolism and venous thrombosis. In Scientific Annals, 5th ed.; State University of Medicine and Pharmacy “Nicolae Testemiţanu”: Chisinau, Moldova, 2011. [Google Scholar]
- Gallo, G.; Volpe, M.; Savoia, C. Endothelial Dysfunction in Hypertension: Current Concepts and Clinical Implications. Front. Med. 2022, 8, 798958. [Google Scholar] [CrossRef] [PubMed]
- Gorar, S.; Alioglu, B.; Ademoglu, E.; Uyar, S.; Bekdemir, H.; Candan, Z.; Saglam, B.; Koc, G.; Culha, C.; Aral, Y. Is There a Tendency for Thrombosis in Gestational Diabetes Mellitus? J. Lab. Physicians 2016, 8, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, K.; Hunt, B.J. Managing antiphospholipid syndrome in pregnancy. Thromb. Res. 2019, 181, S41–S46. [Google Scholar] [CrossRef] [PubMed]
- Dahlquist, K.; Stuart, A.; Källén, K. Planned cesarean section vs planned vaginal delivery among women without formal medical indication for planned cesarean section: A retrospective cohort study of maternal short-term complications. Acta Obstet. Gynecol. Scand. 2022, 101, 1026–1032. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, A.F.; Skjeldestad, F.E.; Sandset, P.M. Ante- and postnatal risk factors of venous thrombosis: A hospital-based case-control study. J. Thromb. Haemost. 2008, 6, 905–912. [Google Scholar] [CrossRef] [PubMed]
- Liao, S.; Woulfe, T.; Hyder, S.; Merriman, E.; Simpson, D.; Chunilal, S. Incidence of venous thromboembolism in different ethnic groups: A regional direct comparison study. J. Thromb. Haemost. 2014, 12, 214–219. [Google Scholar] [CrossRef] [PubMed]
- White, R.H.; Keenan, C.R. Effects of race and ethnicity on the incidence of venous thromboembolism. Thromb. Res. 2009, 123, S11–S17. [Google Scholar] [CrossRef] [PubMed]
- Tabaraii, R.; Farahmand, H.; Ahmadi, J.; Rezvan, S.; Arjmandnia, M.H.; Yosefi, M.; Naye, M.R.; Barati, A.; Razavinia, F.S. Deep vein thrombosis in pregnancy: A review article. J. Vessel Circ. 2020, 1, 27–34. [Google Scholar] [CrossRef]
- Gaudineau, A.; Sananes, N.; Korganow, A.S.; Langer, B. Accidents thromboliques veineux et grossesse. EMC Obstet. Gynecol. 2014, 9, 1–9. [Google Scholar] [CrossRef]
- Mohammed, A.A.; Alhanouf, M.A.; Albassam, R.A.; Alarfaj, R.M.; Zaidi, A.R.Z.; Al-Arfaj, O.; Abu-Shaheen, A. Pregnancy and Venous Thromboembolism: Risk Factors, Trends, Management, and Mortality. BioMed Res. Int. 2020, 2020, 4071892. [Google Scholar] [CrossRef]
- Pană, R.C.; Pană, L.M.; Istratoaie, O.; Duță, L.M.; Gheorman, L.M.; Calborean, V.; Popescu, M.; Voinea, B.; Gheorman, V.V. Incidence of Pulmonary and/or Systemic Thromboembolism in Pregnancy. Curr. Health Sci. J. 2016, 42, 283–288. [Google Scholar] [CrossRef]
- Societatea de Obstetrică şi Ginecologie din România (SOGR) şi Colegiul Medicilor din România. Boala Tromboembolică în Sarcină și Lehuzie; Cîrstoiu, M.M., România; 2019; Volume 17, pp. 1–29. Available online: https://sogr.ro/wp-content/uploads/2019/06/13.-Boala-tromboembolică-în-sarcină-și-lehuzie.pdf (accessed on 29 July 2024).
- Varrias, D.; Spanos, M.; Kokkinidis, D.G.; Zoumpourlis, P.; Kalaitzopoulos, D.R. Venous Thromboembolism in Pregnancy: Challenges and Solutions. Vasc. Health Risk Manag. 2023, 19, 469–484. [Google Scholar] [CrossRef] [PubMed]
- Park, J.E.; Park, Y.; Yuk, J.S. Incidence of and risk factors for thromboembolism during pregnancy and postpartum: A 10-year nationwide population-based study. Taiwan. J. Obstet. Gynecol. 2021, 60, 103–110. [Google Scholar] [CrossRef]
- Pechlivani, N.; Ajjan, R.A. Thrombosis and Vascular Inflammation in Diabetes: Mechanisms and Potential Therapeutic Targets. Front. Cardiovasc. Med. 2018, 5, 1. [Google Scholar] [CrossRef]
- Won, H.S.; Kim, D.Y.; Yang, M.S.; Lee, S.J.; Shin, H.H.; Park, J.B. Pregnancy-induced hypertension, but not gestational diabetes mellitus, is a risk factor for venous thromboembolism in pregnancy. Korean Circ. J. 2011, 41, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Deischinger, C.; Dervic, E.; Nopp, S.; Kaleta, M.; Klimek, P.; Kautzky-Willer, A. Diabetes mellitus is associated with a higher relative risk for venous thromboembolism in females than in males. Diabetes Res. Clin. Pract. 2022, 194, 110190. [Google Scholar] [CrossRef]
- Mahmoud, A.; Sandblad, K.G.; Lundberg, C.E.; Hellsén, G.; Hansson, P.O.; Adiels, M.; Rosengren, A. Prepregnancy overweight and obesity and long-term risk of venous thromboembolism in women. Sci. Rep. 2023, 13, 14597. [Google Scholar] [CrossRef]
- Wik, H.S.; Jacobsen, A.F.; Sandvik, L.; Sandset, P.M. Prevalence and predictors for post-thrombotic syndrome 3 to 16 years after pregnancy-related venous thrombosis: A population-based, cross-sectional, case-control study. J. Thromb. Haemost. 2012, 10, 840–847. [Google Scholar] [CrossRef] [PubMed]
- Fardiazar, Z.; Hajizadeh, K.; Dinparvar, S.; Esmaili, F. Thromboembolism and Thrombosis during Pregnancy and After Delivery between 2009 and 2012 in Al-Zahra Educational Center. J. Caring Sci. 2014, 3, 221–226. [Google Scholar] [CrossRef]
- Malhotra, A.; Weinberger, S. Deep Vein Thrombosis in Pregnancy Epidemiology, Pathogenesis and Diagnosis. 2023. Available online: https://www.uptodate.com/contents/deep-vein-thrombosis-in-pregnancy-epidemiology-pathogenesis-and-diagnosis?search=4.%09Atul%20Malhotra,%20MD,%20Steven%20E%20Weinberger%20et%20al.%20Deep%20vein%20thrombosis%20in%20pregnancy:%20Epidemiology,%20pathogenesis,%20and%20diagnosis&source=search_result&selectedTitle=2~150&usage_type=default&display_rank=2 (accessed on 19 December 2023).
- American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Obstetrics. ACOG Practice Bulletin No. 196: Thromboembolism in Pregnancy. Obstet. Gynecol. 2018, 132, e1–e17. [Google Scholar] [CrossRef]
- Pomp, E.R.; Lenselink, A.M.; Rosendaal, F.R.; Doggen, C.J. Pregnancy, the postpartum period and prothrombotic defects: Risk of venous thrombosis in the MEGA study. J. Thromb. Haemost. 2008, 6, 632–637. [Google Scholar] [CrossRef] [PubMed]
- Dicks, A.B.; Moussallem, E.; Stanbro, M.; Walls, J.; Gandhi, S.; Gray, B.H. A Comprehensive Review of Risk Factors and Thrombophilia Evaluation in Venous Thromboembolism. J. Clin. Med. 2024, 13, 362. [Google Scholar] [CrossRef] [PubMed]
- Blondon, M.; Casini, A.; Hoppe, K.K.; Boehlen, F.; Righini, M.; Smith, N.L. Risks of Venous Thromboembolism After Cesarean Sections: A Meta-Analysis. Chest 2016, 150, 572–596. [Google Scholar] [CrossRef] [PubMed]
- Royal College of Obstetricians and Gynaecologists. Reducing the Risk of Venous Thromboembolism during Pregnancy and the Puerperium: Green-Top Guideline No. 37a. 2015; Royal College of Obstetricians and Gynaecologists: London, UK, 2015. [Google Scholar]

{kind=link}
| General Characteristics | N (%) |
|---|---|
| Age (mean) | 28.2 ± 5.9 years |
| Urban area | 45,305 (49.24%) |
| Rural area | 46,691 (50.75%) |
| Multiple pregnancies | 1469 (1.59%) |
| Twin pregnancies | 1429 (1.55%) |
| Triplet pregnancies | 38 (0.04%) |
| Singleton pregnancy patients | 32,456 (35.27%) |
| Recent postpartum patients (singleton pregnancies) | 59,540 (64.73%) |
| Vaginal birth | 29,200 (49.09%) |
| C-section birth | 30,340 (50.87%) |
| General Characteristics Deep Vein Thrombosis Group | N (%) |
|---|---|
| Age (mean) | 31.3 ± 6.78 years |
| Rural area | 155 (54%) |
| Urban area | 132 (45.99%) |
| Multiparous (more than 4 births) | 48 (16.72%) |
| Multiple pregnancy | 11 (3.83%) |
| Singleton pregnancy patients | 185 (64.45%) |
| Recent postpartum patients (singleton pregnancies) | 102 (35.54%) |
| Vaginal births | 38 (37.25%) |
| C-section births | 64 (62.74%) |
| Mortality | 2 (0.69%) |
| Upper limb | 3 (1.04%) |
| Right lower limb | 67 (23.3%) |
| Left lower limb | 130 (45.2%) |
| Pulmonary embolism | 69 (20.4%) |
| Cerebral thrombosis | 18 (6.27%) |
| Risk Factors Associated with Pulmonary Embolism | N (%) |
|---|---|
| Pregnant women | 28 (40.57%) |
| Gestational age (mean) week | 19.21 |
| Early postpartum women (singleton pregnancies) | 41 (59.42%) |
| Postpartum day (mean) | 16.6 |
| Vaginal birth | 13 (31.7%) |
| C-section birth | 28 (68.29%) |
| Obesity | 13 (18.8%) |
| Gestational diabetes | 1 (1.44%) |
| Hypertension | 8 (11.59%) |
| Preeclampsia | 3 (4.34%) |
| Systemic lupus erythematosus | 1 (1.44%) |
| Hereditary thrombophilia | 9 (13.04%) |
| Inferior limb varicose veins associated with venous insufficiency | 12 (17.39%) |
| Risk Factors Associated with Cerebral Thrombosis | N (%) |
|---|---|
| Pregnant women | 4 |
| Gestational age week (mean) | 20 |
| Early postpartum women (singleton pregnancies) | 14 |
| Postpartum day (mean) | 8.5 |
| Vaginal birth | 4 (22.22%) |
| C-section birth | 10 (71.42%) |
| Obesity | 3 (16.6%) |
| Gestational diabetes | 0 |
| Hypertension | 1 (5.55%) |
| Preeclampsia | 1 (5.55%) |
| Systemic lupus erythematosus | 0 |
| Hereditary thrombophilia | 7 (38.88%) |
| Inferior limb varicose veins associated with venous insufficiency | 0 |
| Risk Factors | Risk Factors Encountered in the Entire Lot of Patients Included (91,996 Patients) | Deep Vein Thrombosis Patients That Have Risk Factors | Pulmonary Embolism Patients That Have Risk Factors | Cerebral Thrombosis Patients That Have Risk Factors |
|---|---|---|---|---|
| N (%) | N (%) | N (%) | N (%) | |
| Obesity | 2648 (2.87%) | 28 (9.75%) | 13 (18.8%) | 3 (16.6%) |
| Gestational diabetes | 1791 (1.94%) | 18 (6.27%) | 1 (1.44%) | 0 |
| Hypertension | 4415 (4.79%) | 30 (10.45%) | 8 (11.59%) | 1 (5.55%) |
| Preeclampsia | 558 (0.60%) | 8 (2.78%) | 3 (4.34%) | 1 (5.55%) |
| Systemic lupus erythematosus | 84 (0.091%) | 1 (0.34%) | 1 (1.44%) | 0 |
| Hereditary thrombophilia | 1730 (1.88%) | 50 (17.42%) | 9 (13.04%) | 7 (38.88%) |
| Inferior limb varicose veins associated with venous insufficiency | 2758 (2.99%) | 65 (22.64%) | 12 (17.39%) | 0 |
| Total | 13,984 (15.2%) | 201 (70.03%) | 47 (68.11%) | 12 (66.66%) |
| Risk Factor | Odds Ratio (OR) | Significance (p-Value) | Confidence Interval (CI) |
|---|---|---|---|
| Obesity | 3.676 | <0.001 | 2.484–5.439 |
| Gestational diabetes | 3.394 | <0.001 | 2.101–5.483 |
| Hypertension | 2.325 | <0.001 | 1.591–3.397 |
| Preeclampsia | 4.753 | <0.001 | 2.342–9.645 |
| Systemic lupus erythematosus | 3.860 | 0.180 | 0.536–27.821 |
| Hereditary thrombophilia | 12.138 | <0.001 | 8.973–16.417 |
| Varicose veins | 9.678 | <0.001 | 7.321–12.793 |
| Risk Factor | Odds Ratio (OR) | Significance (p-Value) | Confidence Interval (CI) |
|---|---|---|---|
| Obesity | 7.867 | <0.001 | 4.297–14.401 |
| Gestational diabetes | 0.741 | No significant effect (0.766) | 0.103–5.336 |
| Hypertension | 2.605 | 0.011 | 1.246–5.446 |
| Preeclampsia | 7.483 | <0.001 | 2.346–23.872 |
| Systemic lupus erythematosus | 0.997 | Lower risk | Not applicable |
| Hereditary thrombophilia | 11.035 | <0.001 | 5.910–20.602 |
| Varicose veins | 6.837 | <0.001 | 3.665–12.757 |
| Risk Factor | Odds Ratio (OR) | Significance (p-Value) | Confidence Interval (CI) |
|---|---|---|---|
| Obesity | 0.003 | <0.001 | 1.954–23.347 |
| Gestational diabetes | 0 | Lower risk (0.989) | Not applicable |
| Hypertension | 0.881 | <0.001 | 0.155–8.770 |
| Preeclampsia | 9.655 | <0.001 | 1.283–72.672 |
| Systemic lupus erythematosus | 0 | Lower risk | Not applicable |
| Hereditary thrombophilia | 33.275 | <0.001 | 12.884–85.939 |
| Varicose veins | 0 | No significant effect (0.987) | Not applicable |
| Risk Factor | Coefficient | Odds Ratio | Interpretation (Times More Likely to Develop DVT) |
|---|---|---|---|
| Age | 0.037 | 1.04 | Minimal impact |
| Gestational age | 0.015 | 1.02 | Minimal impact |
| C-section | 1.188 | 3.28 | 3.3 |
| Obesity | 2.301 | 10.00 | 10 |
| Gestational diabetes | 0.860 | 2.36 | 2.4 |
| Hypertension | 1.739 | 5.69 | 5.7 |
| Preeclampsia | 2.197 | 9.00 | 9 |
| Systemic lupus erythematosus | 1.891 | 6.62 | 6.6 |
| Hereditary thrombophilia | 3.007 | 20.22 | 20 |
| Inferior limb varicose veins associated with venous insufficiency | 2.639 | 14.00 | 14 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Filip, C.; Socolov, S.A.; Matasariu, D.R.; Ursache, A.; Pisla, K.D.; Gisca, T.C.; Mihalceanu, E.; Boiculese, V.L.; Socolov, D. The Burden of Deep Vein Thrombosis and Risk Factors in Pregnancy and Postpartum—Mirroring Our Region’s Particularities. J. Clin. Med. 2024, 13, 4705. https://doi.org/10.3390/jcm13164705
Filip C, Socolov SA, Matasariu DR, Ursache A, Pisla KD, Gisca TC, Mihalceanu E, Boiculese VL, Socolov D. The Burden of Deep Vein Thrombosis and Risk Factors in Pregnancy and Postpartum—Mirroring Our Region’s Particularities. Journal of Clinical Medicine. 2024; 13(16):4705. https://doi.org/10.3390/jcm13164705
Chicago/Turabian StyleFilip, Catalina, Sofia Alexandra Socolov, Daniela Roxana Matasariu, Alexandra Ursache, Karina Delia Pisla, Tudor Catalin Gisca, Elena Mihalceanu, Vasile Lucian Boiculese, and Demetra Socolov. 2024. "The Burden of Deep Vein Thrombosis and Risk Factors in Pregnancy and Postpartum—Mirroring Our Region’s Particularities" Journal of Clinical Medicine 13, no. 16: 4705. https://doi.org/10.3390/jcm13164705
APA StyleFilip, C., Socolov, S. A., Matasariu, D. R., Ursache, A., Pisla, K. D., Gisca, T. C., Mihalceanu, E., Boiculese, V. L., & Socolov, D. (2024). The Burden of Deep Vein Thrombosis and Risk Factors in Pregnancy and Postpartum—Mirroring Our Region’s Particularities. Journal of Clinical Medicine, 13(16), 4705. https://doi.org/10.3390/jcm13164705