
Barriers and Challenges to Implementing Whole Blood Transfusion Protocols in Civilian Hospitals: A Systematic Review and Meta-Analysis

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Eligibility Criteria
2.2. Inclusion and Exclusion Criteria
2.3. Information Sources and Search Strategy
2.4. The Selection Process, Data Collection Process, and Analysis
2.5. Data Items
2.6. Quality Assessment
2.7. Data Analysis
3. Results
3.1. Mortality
3.1.1. Six-Hour Mortality
3.1.2. 24 h Mortality
3.1.3. Delayed Mortality (28–30 Days)
3.2. Course of the Disease Outcomes
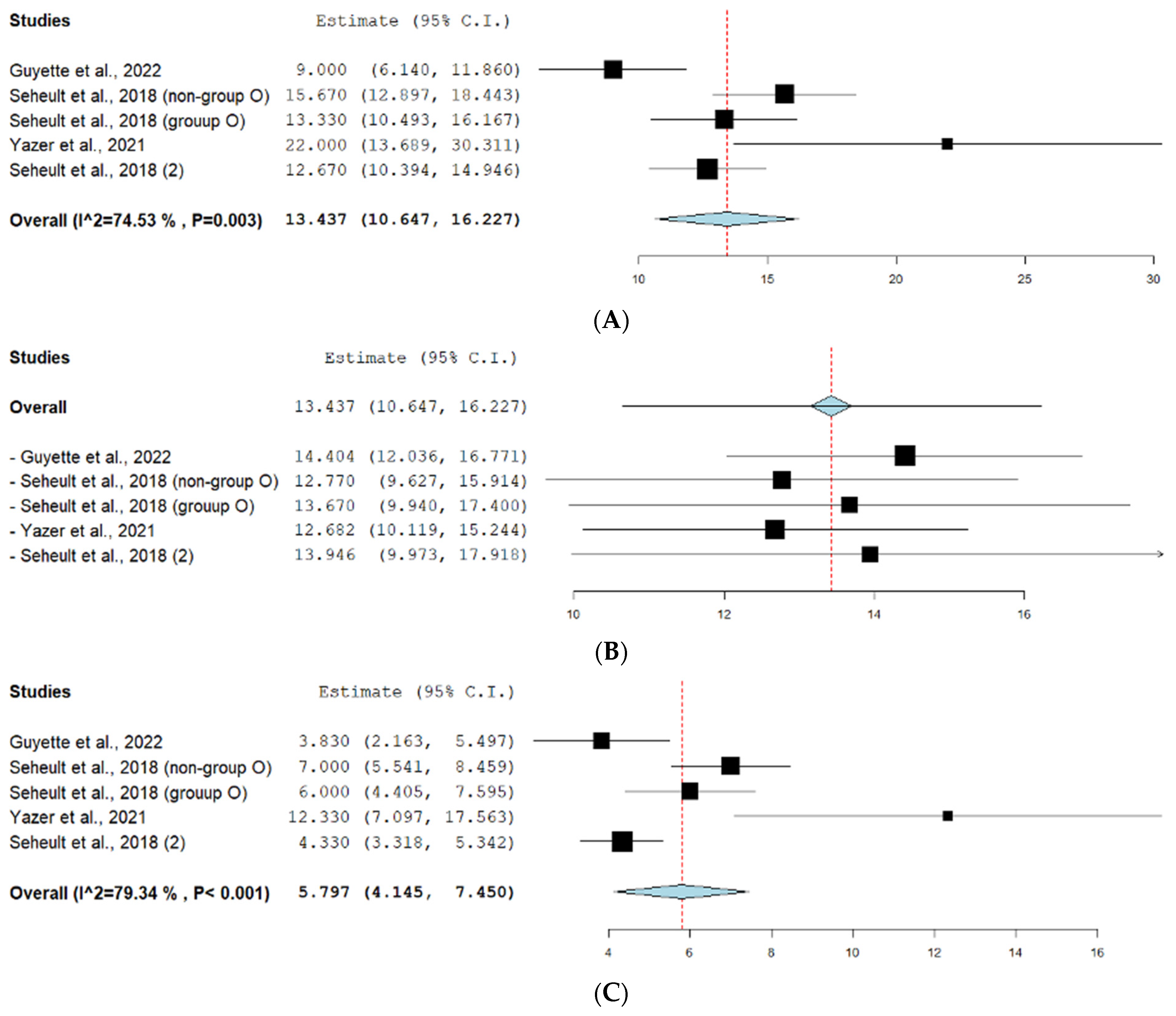
3.2.1. Hospital Length of Stay
3.2.2. ICU Days
3.2.3. Days on Ventilator
3.2.4. ICU Free Days
3.2.5. Ventilator-Free Days
3.3. Side Effects
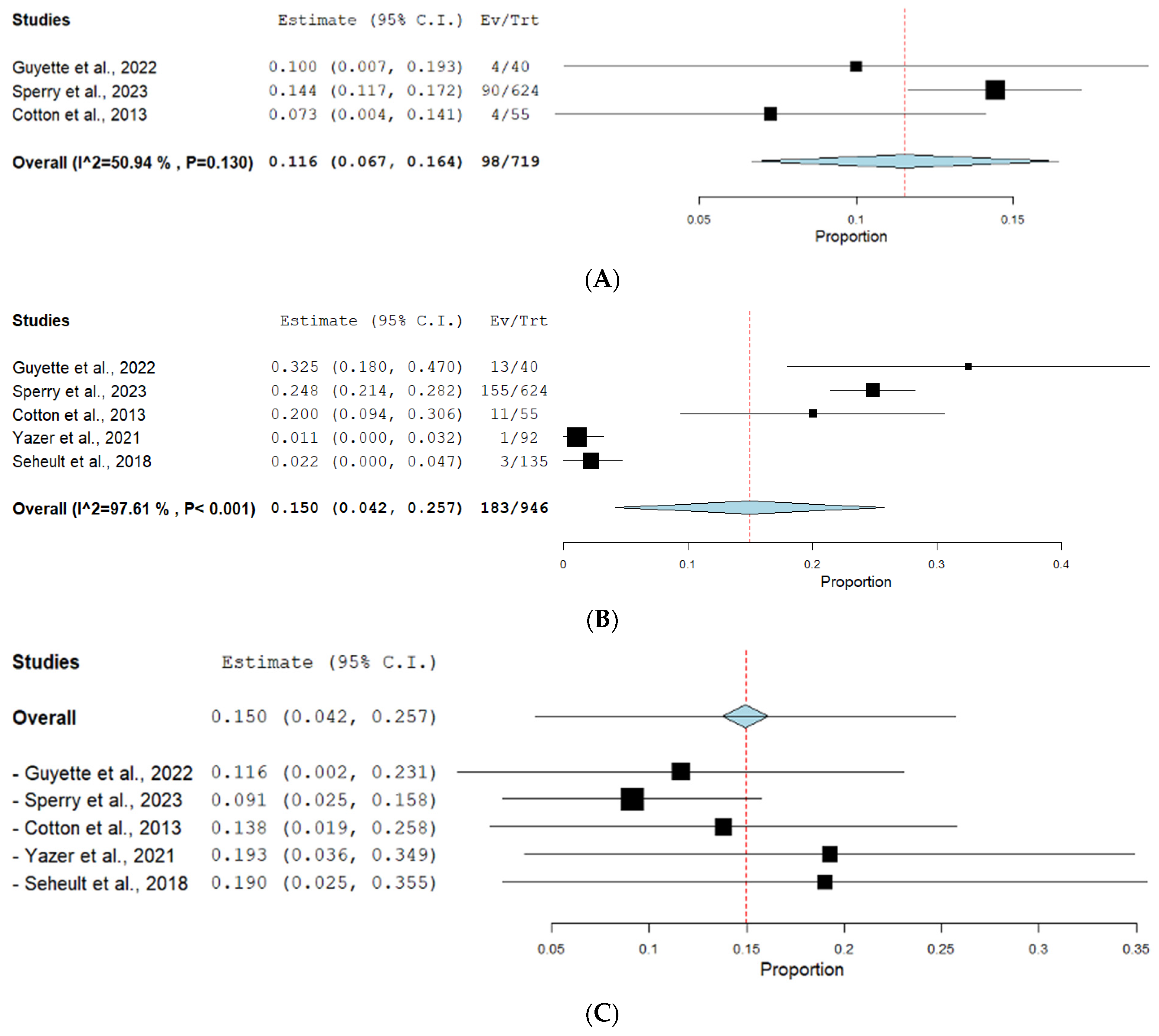
3.3.1. Multiorgan Failure
3.3.2. Nosocomial Infections
4. Discussion
4.1. Mortality Outcomes
4.2. Disease Outcomes
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jackson, B.; Murphy, C.; Fontaine, M.J. Current state of whole blood transfusion for civilian trauma resuscitation. Transfusion 2020, 60, S45–S51. [Google Scholar] [CrossRef] [PubMed]
- Safe Blood and Blood Products Guidelines and Principles for Safe Blood Transfusion Practice. 2009, p. 57. Available online: https://cdn.who.int/media/docs/default-source/blood-transfusion-safety/guidelines-and-principles-for-safe-blood-transfudion-practice.pdf?sfvrsn=f249f9a_1&download=true (accessed on 26 July 2024).
- Cap, A.; Beckett, A.; Benov, A.; Borgman, M.; Chen, J.; Corley, J.; Doughty, H.; Fisher, A.; Kane, S.; Mallory, W.; et al. Whole blood transfusion. Mil. Med. 2018, 183 (Suppl. S2), 44–51. [Google Scholar] [CrossRef] [PubMed]
- Lotterman, S.; Sharma, S. Blood transfusion. In Lotterman, StatPearls, Bethesda; StatPearls Publishing LLC: San Diego, CA, USA, 2023. [Google Scholar]
- McCoy, C.C.; Brenner, M.; Duchesne, J.; Roberts, D.; Ferrada, P.; Horer, T.; Kauvar, D.; Khan, M.; Kirkpatrick, A.; Ordonez, C.; et al. Back to the Future: Whole Blood Resuscitation of the Severely Injured Trauma Patient. Shock 2020, 56, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Nursing, O.R.F.; Ernstmeyer, K.; Christman, E.; Chapter 3 Administer Blood Products. Nursing Advanced Skills—NCBI Bookshelf. 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK594497/ (accessed on 2 July 2024).
- Hanna, M.; Knittel, J.; Gillihan, J. The Use of Whole Blood Transfusion in Trauma. Curr. Anesthesiol. Rep. 2022, 12, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Chand, N.; Subramanya, H.; Rao, G. Management of patients who refuse blood transfusion. Indian J. Anaesth. 2014, 58, 658–664. [Google Scholar] [CrossRef] [PubMed]
- Thompson, H.A. Blood Transfusions and Jehovah’s Witnesses, Texas Medicine. Available online: https://pubmed.ncbi.nlm.nih.gov/2727941/#:~:text=Thus%2C%20Jehovah’s%20Witnesses%20regularly%20refuse,risk%20of%20losing%20eternal%20salvation (accessed on 19 June 2024).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.4 (Updated August 2023). Cochrane, 2023. Available online: www.training.cochrane.org/handbook (accessed on 2 July 2024).
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial. Évid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef]
- Guyette, F.X.; Zenati, M.; Triulzi, D.J.; Yazer, M.H.; Skroczky, H.B.; Early, B.J.B.; Adams, P.W.B.; Brown, J.B.M.; Alarcon, L.; Neal, M.D.; et al. Prehospital low titer group O whole blood is feasible and safe: Results of a prospective randomized pilot trial. J. Trauma Inj. Infect. Crit. Care 2022, 92, 839–847. [Google Scholar] [CrossRef]
- Rahbar, E.; Cardenas, J.C.; Matijevic, N.; Del Junco, D.; Podbielski, J.; Cohen, M.J.; Early Whole Blood Investigators. Trauma, time, and transfusions: A longitudinal analysis of coagulation markers in severely injured trauma patients receiving modified whole blood or component blood products. Shock 2015, 44, 417–425. [Google Scholar] [CrossRef]
- Cotton, B.A.; Podbielski, J.; Camp, E.; Welch, T.; del Junco, D.; Bai, Y.; Hobbs, R.; Scroggins, J.; Hartwell, B.; Kozar, R.A.; et al. A randomized controlled pilot trial of modified whole blood versus component therapy in severely injured patients requiring large volume transfusions. Ann. Surg. 2013, 258, 527–533. [Google Scholar] [CrossRef]
- Lo, C.K.-L.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef] [PubMed]
- Sperry, J.L.M.; Cotton, B.A.; Luther, J.F.; Cannon, J.W.; Schreiber, M.A.; Moore, E.E.; Namias, N.; Minei, J.P.; Wisniewski, S.R.; Guyette, F.X.; et al. Whole Blood Resuscitation and Association with Survival in Injured Patients with an Elevated Probability of Mortality. J. Am. Coll. Surg. 2023, 237, 206–219. [Google Scholar] [CrossRef] [PubMed]
- Seheult, J.N.; Bahr, M.; Anto, V.; Alarcon, L.H.; Corcos, A.; Sperry, J.L.; Triulzi, D.J.; Yazer, M.H. Safety profile of uncrossmatched, cold-stored, low-titer, group O+ whole blood in civilian trauma patients. Transfusion 2018, 58, 2280–2288. [Google Scholar] [CrossRef] [PubMed]
- Yazer, M.H.; Freeman, A.; Harrold, I.M.; Anto, V.; Neal, M.D.; Triulzi, D.J.; Seheult, J.N. Injured recipients of low-titer group O whole blood have similar clinical outcomes compared to recipients of conventional component therapy: A single-center, retrospective study. Transfusion 2021, 61, 1710–1720. [Google Scholar] [CrossRef]
- Nadler, R.; Tsur, A.M.; Yazer, M.H.; Shinar, E.; Moshe, T.; Benov, A.; Glassberg, E.; Epstein, D.; Chen, J. Early experience with transfusing low titer group O whole blood in the pre-hospital setting in Israel. Transfusion 2020, 60, S10–S16. [Google Scholar] [CrossRef] [PubMed]
- Seheult, J.N.; Anto, V.; Alarcon, L.H.; Sperry, J.L.; Triulzi, D.J.; Yazer, M.H. Clinical outcomes among low-titer group O whole blood recipients compared to recipients of conventional components in civilian trauma resuscitation. Transfusion 2018, 58, 1838–1845. [Google Scholar] [CrossRef]
- Williams, J.; Merutka, N.; Meyer, D.; Bai, Y.; Prater, S.; Cabrera, R.; Holcomb, J.B.; Wade, C.E.; Love, J.D.; Cotton, B.A. Safety profile and impact of low-titer group O whole blood for emergency use in trauma. J. Trauma Inj. Infect. Crit. Care 2020, 88, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Shea, S.M.; Staudt, A.M.; Thomas, K.A.; Schuerer, D.; Mielke, J.E.; Folkerts, D.; Lowder, E.; Martin, C.; Bochicchio, G.V.; Spinella, P.C. The use of low-titer group O whole blood is independently associated with improved survival compared to component therapy in adults with severe traumatic hemorrhage. Transfusion 2020, 60, S2–S9. [Google Scholar] [CrossRef]
- Braverman, M.A.; Smith, A.; Pokorny, D.; Axtman, B.; Shahan, C.P.; Barry, L.; Corral, H.; Jonas, R.B.; Shiels, M.; Schaefer, R.; et al. Prehospital whole blood reduces early mortality in patients with hemorrhagic shock. Transfusion 2021, 61, S15–S21. [Google Scholar] [CrossRef]
- OpenMeta[analyst]. Brown.edu. Available online: http://www.cebm.brown.edu/openmeta/ (accessed on 2 July 2024).
- Kronstedt, S.; Lee, J.; Millner, D.; Mattivi, C.; LaFrankie, H.; Paladino, L.; Siegler, J. The Role of Whole Blood Transfusions in Civilian Trauma: A Review of Literature in Military and Civilian Trauma. Cureus 2022, 14, e24263. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ramakrishnan, V.; Cattamanchi, S. Transfusion practices in trauma. Indian J. Anaesth. 2014, 58, 609–615. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Malkin, M.; Nevo, A.; Brundage, S.I.; Schreiber, M. Effectiveness and safety of whole blood compared to balanced blood components in resuscitation of hemorrhaging trauma patients—A systematic review. Injury 2020, 52, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, A.D.; Ntambwe, P.; Crawford, A.M. Barriers to Effective Transfusion Practices in Limited-Resource Settings: From Infrastructure to Cultural Beliefs. World J. Surg. 2020, 44, 2094–2099. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sivanandan, A.; Abhilash, K.P.P. Early Management of Trauma: The Golden Hour. Curr. Med. Issues 2020, 18, 36. [Google Scholar] [CrossRef]
- Ngatuvai, M.; Zagales, I.; Sauder, M.; Andrade, R.; Santos, R.; Bilski, T.; Kornblith, L.; Elkbuli, A. Outcomes of Transfusion With Whole Blood, Component Therapy, or Both in Adult Civilian Trauma Patients: A Systematic Review and Meta-Analysis. J. Surg. Res. 2023, 287, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Crowe, E.; DeSantis, S.M.; Bonnette, A.; Jansen, J.O.; Yamal, J.; Holcomb, J.B.; Pedroza, C.; Harvin, J.A.; Marques, M.B.; Avritscher, E.B.; et al. Whole blood transfusion versus component therapy in trauma resuscitation: A systematic review and meta-analysis. J. Am. Coll. Emerg. Physicians Open 2020, 1, 633–641. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Meizoso, J.P.M.; Cotton, B.A.; Lawless, R.A.; Kodadek, L.M.; Lynde, J.M.D.; Russell, N.; Gaspich, J.; Maung, A.; Anderson, C.; Reynolds, J.M.M.; et al. Whole Blood Resuscitation for Injured Patients Requiring Transfusion: A Systematic Review, Meta-Analysis, and Practice Management Guideline from the Eastern Association for the Surgery of Trauma. J. Trauma Inj. Infect. Crit. Care 2024. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Selection | Comparability | Outcome | Quality Score | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Study ID | Representativeness of the Exposed Cohort | Selection of the Non- Exposed Cohort | Ascertainment of Exposure | Demonstration That Outcome of Interest Was not Present at Start of Study | Comparability of Cohorts on the Basis of the Design or Analysis | Assessment of Outcome | Was Follow-Up Long Enough for Outcomes to Occur | Adequacy of Forest Plot for This Outcome of cohorts | |
| Sperry et al. [18] | * | * | * | * | ** | * | * | * | 9 Good |
| Seheult et al. [19] | * | * | * | * | * | * | 6 fair | ||
| Yazer et al. [20] | * | * | * | * | ** | * | * | * | 9 Good |
| Nadler et al. [21] | * | * | * | ** | * | * | 7 fair | ||
| Seheult et al. [22] | * | * | * | * | ** | * | * | 8 Good | |
| Williams et al. [23] | * | * | * | * | ** | * | * | * | 9 Good |
| Shea et al. [24] | * | * | * | * | ** | * | * | * | 9 Good |
| Braverman et al. [25] | * | * | * | * | ** | * | * | 8 Good | |
| Author and Year | Country | Study Design | Sample Size | Age [Median, (IQR)] | Males (n %) | Blunt Injury (n %) |
|---|---|---|---|---|---|---|
| Guyette et al., 2022 [14] | United States | RCT | 40 | 46 (27–64) | 23 (57.5%) | 34 (85%) |
| Sperry et al., 2023 [18] | United States | Prospective Cohort | 624 | 35.0 (26.0–51.0) | 546 (87.5%) | 252 (40.38%) |
| Seheult et al., 2018 (non-group O) [19] | United States | Prospective Cohort | 102 | 38 (26–58) | 94 (92.16%) | - |
| Seheult et al., 2018 (group O) [19] | 70 | 41 (26–60) | 70 (100%) | - | ||
| Yazer et al., 2021 [20] | United States | Retrospective Cohort | 92 | 47 (19–83) | 86 (93.48%) | 74 (80.43%) |
| Nadler et al., 2020 [21] | Israel | Retrospective review | 8 | 25.0 (2.0, 45.0) | 6 (75%) | 8 (100%) |
| Seheult et al., 2018 [22] | United States | Retrospective Cohort | 135 | 40 (26–61) | 129 (95.56%) | 109 (80.74%) |
| Rahbar et al., 2015 [15] | United States | RCT | 25 | 40 (29, 55) | 21 (84%) | 16 (64%) |
| Williams et al., 2019 [23] | United States | Retrospective cohort | 198 | 41 (26, 56) | 143 (72.22%) | 141 (71.2%) |
| Cotton et al., 2013 [16] | United States | RCT | 55 | 40 (29, 56) | 43 (78.2%) | - |
| Shea et al., 2020 [24] | United States | Prospective Cohort | 44 | 32 (28–32) | 35 (79.55%) | 12 (27.27%) |
| Braverman et al., 2021 [25] | United States | Retrospective Cohort | 107 | 32 (24–46) | 90 (84.11%) | 39 (36.45%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nouh, T.; Shalhoub, M.; Alburakan, A.; Alshahwan, N.; Alzelfawi, L.; Almajed, E.; Alhindawi, Z.; Bin Salamah, R.; AlMutiri, W.; Alruwaili, E.; et al. Barriers and Challenges to Implementing Whole Blood Transfusion Protocols in Civilian Hospitals: A Systematic Review and Meta-Analysis. J. Clin. Med. 2024, 13, 4726. https://doi.org/10.3390/jcm13164726
Nouh T, Shalhoub M, Alburakan A, Alshahwan N, Alzelfawi L, Almajed E, Alhindawi Z, Bin Salamah R, AlMutiri W, Alruwaili E, et al. Barriers and Challenges to Implementing Whole Blood Transfusion Protocols in Civilian Hospitals: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2024; 13(16):4726. https://doi.org/10.3390/jcm13164726
Chicago/Turabian StyleNouh, Thamer, Mishary Shalhoub, Ahmed Alburakan, Nawaf Alshahwan, Lama Alzelfawi, Ebtesam Almajed, Zeena Alhindawi, Rawan Bin Salamah, Wijdan AlMutiri, Ebtisam Alruwaili, and et al. 2024. "Barriers and Challenges to Implementing Whole Blood Transfusion Protocols in Civilian Hospitals: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 13, no. 16: 4726. https://doi.org/10.3390/jcm13164726