



Volumetric Analyses of Dysmorphic Maxillofacial Structures Using 3D Surface-Based Approaches: A Scoping Review

 ,
,  , , , ,
, , , ,  ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility and Exclusion Criteria
2.3. Study Selection
2.4. Data Charting
2.5. Data Items
2.6. Critical Appraisal Assessment
2.7. Synthesis of Results
3. Results
3.1. Overview of Studies
Individual Study Characteristics
3.2. Summary of the Methodologies Employed in the Selected Studies
3.3. Image Acquisition and Software
3.3.1. Stereophotogrammetry
3.3.2. Laser Scanning
3.3.3. Electromechanical Digitizers
3.4. Selection of the Structure of Interest
3.4.1. Landmarks-Based Methods
3.4.2. Planes-Based Methods
3.4.3. Combination: Landmarks- and Planes-Based Methods
3.4.4. Other Methods
3.5. Protocols for Volume Calculation
3.5.1. Custom Algorithms
3.5.2. Automatic Software Calculation
3.6. Volumetric Data Reporting
3.6.1. Studies Reporting Effective Volumes
3.6.2. Studies Reporting Volumetric Changes
3.6.3. Studies Reporting Dimensionless Indices
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Figueroa, D.A.A.; Friede, D.H. Craniofacial Growth in Unoperated Craniofacial Malformations. Cleft Palate-Craniofacial J. 2000, 37, 431–432. [Google Scholar] [CrossRef]
- Hunt, J.A.; Hobar, P.C. Common Craniofacial Anomalies: Conditions of Craniofacial Atrophy/Hypoplasia and Neoplasia. Plast. Reconstr. Surg. 2003, 111, 1497–1508;quiz 1509–1510. [Google Scholar] [CrossRef] [PubMed]
- Cronin, A.; McLeod, S. Craniofacial Anomalies. In The SAGE Encyclopedia of Human Communication Sciences and Disorders; Damico, J.S., Ball, M.J., Eds.; SAGE Publications Ltd.: London, UK, 2019; pp. 515–519. ISBN 978-1-4833-8081-0. [Google Scholar]
- Hunter, A.G.W. Medical Genetics: 2. The Diagnostic Approach to the Child with Dysmorphic Signs. CMAJ 2002, 167, 367–372. [Google Scholar] [PubMed]
- Van Den Elzen, M.E.P.; Versnel, S.L.; Hovius, S.E.R.; Passchier, J.; Duivenvoorden, H.J.; Mathijssen, I.M.J. Adults with Congenital or Acquired Facial Disfigurement: Impact of Appearance on Social Functioning. J. Cranio-Maxillofac. Surg. 2012, 40, 777–782. [Google Scholar] [CrossRef] [PubMed]
- Hickey, A.J.; Salter, M. Prosthodontic and Psychological Factors in Treating Patients with Congenital and Craniofacial Defects. J. Prosthet. Dent. 2006, 95, 392–396. [Google Scholar] [CrossRef] [PubMed]
- Wiechers, C.; Thjen, T.; Koos, B.; Reinert, S.; Poets, C.F. Treatment of Infants with Craniofacial Malformations. Arch. Dis. Child. Fetal Neonatal Ed. 2021, 106, 104–109. [Google Scholar] [CrossRef] [PubMed]
- American Cleft Palate–Craniofacial Association. Parameters: For Evaluation and Treatment of Patients with Cleft Lip/Palate or Other Craniofacial Differences. Cleft Palate-Craniofacial J. 2018, 55, 141. [Google Scholar] [CrossRef]
- Bohm, L.A.; Sidman, J.D.; Roby, B. Early Airway Intervention for Craniofacial Anomalies. Facial Plast. Surg. Clin. N. Am. 2016, 24, 427–436. [Google Scholar] [CrossRef] [PubMed]
- Prahl-Andersen, B. Controversies in the Management of Craniofacial Malformations. Semin. Orthod. 2005, 11, 67–75. [Google Scholar] [CrossRef]
- Trainor, P.A.; Richtsmeier, J.T. Facing up to the Challenges of Advancing Craniofacial Research. Am. J. Med. Genet. A 2015, 167, 1451–1454. [Google Scholar] [CrossRef]
- Mai, H.N.; Kim, J.; Choi, Y.H.; Lee, D.H. Accuracy of Portable Face-Scanning Devices for Obtaining Three-Dimensional Face Models: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public. Health 2021, 18, 94. [Google Scholar] [CrossRef] [PubMed]
- Cen, Y.; Huang, X.; Liu, J.; Qin, Y.; Wu, X.; Ye, S.; Du, S.; Liao, W. Application of Three-Dimensional Reconstruction Technology in Dentistry: A Narrative Review. BMC Oral. Health 2023, 23, 630. [Google Scholar] [CrossRef] [PubMed]
- Karatas, O.H.; Toy, E. Three-Dimensional Imaging Techniques: A Literature Review. Eur. J. Dent. 2014, 8, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Heike, C.L.; Upson, K.; Stuhaug, E.; Weinberg, S.M. 3D Digital Stereophotogrammetry: A Practical Guide to Facial Image Acquisition. Head. Face Med. 2010, 6, 18. [Google Scholar] [CrossRef] [PubMed]
- Honrado, C.P.; Larrabee, W.F. Update in Three-Dimensional Imaging in Facial Plastic Surgery. Curr. Opin. Otolaryngol. Head. Neck Surg. 2004, 12, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Lo, L.J.; Lin, H.H. Applications of Three-Dimensional Imaging Techniques in Craniomaxillofacial Surgery: A Literature Review. Biomed. J. 2023, 46, 100615. [Google Scholar] [CrossRef] [PubMed]
- D’Ettorre, G.; Farronato, M.; Candida, E.; Quinzi, V.; Grippaudo, C. A Comparison between Stereophotogrammetry and Smartphone Structured Light Technology for Three-Dimensional Face Scanning. Angle Orthod. 2022, 93, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Gibelli, D.; Dolci, C.; Cappella, A.; Sforza, C. Reliability of Optical Devices for Three-Dimensional Facial Anatomy Description: A Systematic Review and Meta-Analysis. Int. J. Oral. Maxillofac. Surg. 2020, 49, 1092–1106. [Google Scholar] [CrossRef]
- Gibelli, D.; Cappella, A.; Dolci, C.; Sforza, C. 3D Surface Acquisition Systems and Their Applications to Facial Anatomy: Let’s Make a Point. Ital. J. Anat. Embryol. 2019, 124, 422–431. [Google Scholar] [CrossRef]
- Kau, C.; Zhurov, A.; Scheer, R.; Bouwman, S.; Richmond, S. The Feasibility of Measuring Three-dimensional Facial Morphology in Children. Orthod. Craniofac Res. 2004, 7, 198–204. [Google Scholar] [CrossRef]
- Primozic, J.; Ovsenik, M.; Richmond, S.; Kau, C.H.; Zhurov, A. Early Crossbite Correction: A Three-Dimensional Evaluation. Eur. J. Orthod. 2009, 31, 352–356. [Google Scholar] [CrossRef] [PubMed]
- Gibelli, D.; Tarabbia, F.; Restelli, S.; Allevi, F.; Dolci, C.; Dell’Aversana Orabona, G.; Cappella, A.; Codari, M.; Sforza, C.; Biglioli, F. Three-Dimensional Assessment of Restored Smiling Mobility after Reanimation of Unilateral Facial Palsy by Triple Innervation Technique. Int. J. Oral. Maxillofac. Surg. 2020, 49, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Da Pozzo, F.; Gibelli, D.; Beltramini, G.A.; Dolci, C.; Giannì, A.B.; Sforza, C. The Effect of Orthognathic Surgery on Soft-Tissue Facial Asymmetry: A Longitudinal Three-Dimensional Analysis. J. Craniofacial Surg. 2020, 31, 1578–1582. [Google Scholar] [CrossRef] [PubMed]
- Farkas, L.G.; Deutsch, C.K. Anthropometric Determination of Craniofacial Morphology. Am. J. Med. Genet. 1996, 65, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Farkas, L.G. Anthropometry of the Head and Face, 2nd ed.; Raven Press: New York, NY, USA, 1994. [Google Scholar]
- Ambrosio, E.C.P.; Fusco, N.D.S.; Carrara, C.F.C.; Bergamo, M.T.; Lourenço Neto, N.; Cruvinel, T.; Rios, D.; Almeida, A.L.P.F.; Soares, S.; Machado, M.A.A.M.; et al. Digital Volumetric Monitoring of Palate Growth in Children with Cleft Lip and Palate. J. Craniofacial Surg. 2022, 33, E143–E145. [Google Scholar] [CrossRef] [PubMed]
- Hohoff, A.; Stamm, T.; Meyer, U.; Wiechmann, D.; Ehmer, U. Objective Growth Monitoring of the Maxilla in Full Term Infants. Arch. Oral. Biol. 2006, 51, 222–235. [Google Scholar] [CrossRef] [PubMed]
- Ackerman, J.L.; Proffit, W.R.; Sarver, D.M. The Emerging Soft Tissue Paradigm in Orthodontic Diagnosis and Treatment Planning. Clin. Orthod. Res. 1999, 2, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Proffit, W.R. The Soft Tissue Paradigm in Orthodontic Diagnosis and Treatment Planning: A New View for a New Century. J. Esthet. Dent. 2000, 12, 46–49. [Google Scholar] [CrossRef] [PubMed]
- Jansma, J.; Schepers, R.H. Adjunctive Aesthetic Procedures in Orthognathic Surgery. Oral. Maxillofac. Surg. Clin. N. Am. 2023, 35, 139–152. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated Methodological Guidance for the Conduct of Scoping Reviews. JBI Evid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef]
- Ferrario, V.F.; Dellavia, C.; Colombo, A.; Sforza, C. Three-Dimensional Assessment of Nose and Lip Morphology in Subjects with Down Syndrome. Ann. Plast. Surg. 2004, 53, 577–583. [Google Scholar] [CrossRef]
- Sforza, C.; Grandi, G.; Pisoni, L.; Di Blasio, C.; Gandolfini, M.; Ferrario, V.F. Soft Tissue Facial Morphometry in Subjects with Moebius Syndrome. Eur. J. Oral. Sci. 2009, 117, 695–703. [Google Scholar] [CrossRef]
- Sforza, C.; Elamin, F.; Rosati, R.; Lucchini, M.A.; Tommasi, D.G.; Ferrario, V.F. Three-Dimensional Assessment of Nose and Lip Morphology in North Sudanese Subjects with Down Syndrome. Angle Orthod. 2011, 81, 107–114. [Google Scholar] [CrossRef]
- Ambrosio, E.C.P.; Sforza, C.; de Menezes, M.; Carrara, C.F.C.; Soares, S.; Machado, M.A.A.M.; Oliveira, T.M. Prospective Cohort 3D Study of Dental Arches in Children with Bilateral Orofacial Cleft: Assessment of Volume and Superimposition. Int. J. Paediatr. Dent. 2021, 31, 606–612. [Google Scholar] [CrossRef]
- Chattopadhyay, D.; Kapoor, A.; Vathulya, M.; Bera, S. Volumetric Assessment of the Nose after Primary Unilateral Cleft Rhinoplasty Using Laberge’s Technique. J. Plast. Reconstr. Aesthet. Surg. 2023, 85, 446–453. [Google Scholar] [CrossRef]
- Paoloni, V.; Cretella Lombardo, E.; Placidi, F.; Ruvolo, G.; Cozza, P.; Laganà, G. Obstructive Sleep Apnea in Children with Marfan Syndrome: Relationships between Three-Dimensional Palatal Morphology and Apnea-Hypopnea Index. Int. J. Pediatr. Otorhinolaryngol. 2018, 112, 6–9. [Google Scholar] [CrossRef]
- Chan, F.C.; Kawamoto, H.K.; Federico, C.; Bradley, J.P. Soft-Tissue Volumetric Changes Following Monobloc Distraction Procedure. J. Craniofacial Surg. 2013, 24, 416–420. [Google Scholar] [CrossRef]
- Jayaratne, Y.S.N.; Lo, J.; Zwahlen, R.A.; Cheung, L.K. Three-dimensional Photogrammetry for Surgical Planning of Tissue Expansion in Hemifacial Microsomia. Head. Neck 2010, 32, 1728–1735. [Google Scholar] [CrossRef]
- Mercan, E.; Morrison, C.S.; Stuhaug, E.; Shapiro, L.G.; Tse, R.W. Novel Computer Vision Analysis of Nasal Shape in Children with Unilateral Cleft Lip. J. Cranio-Maxillofac. Surg. 2018, 46, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Ozdemir, A.S.; Esenlik, E. Three-Dimensional Soft-Tissue Evaluation in Patients with Cleft Lip and Palate. Med. Sci. Monit. 2018, 24, 8608–8620. [Google Scholar] [CrossRef] [PubMed]
- Pucciarelli, V.; Pisoni, L.; De Menezes, M.; Ceron Zapata, A.M.; Lopez-Palacio, A.M.; Codari, M.; Sforza, C. Palatal Volume Changes in Unilateral Cleft Lip and Palate Paediatric Patients. In Proceedings of the 6th International Conference on 3D Body Scanning Technologies, Lugano, Switzerland, 27–28 October 2015; pp. 139–146. [Google Scholar]
- Pucciarelli, V.; Baserga, C.; Codari, M.; Beltramini, G.A.; Sforza, C.; Giannì, A.B. Three-Dimensional Stereophotogrammetric Evaluation of the Efficacy of Autologous Fat Grafting in the Treatment of Parry-Romberg Syndrome. J. Craniofacial Surg. 2018, 29, 2124–2127. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, M.I.; Zadeh, R.; Bucci, D.; Palmieri, A.; Monarca, C.; Staderini, E.; Oliva, G.; Candida, E.; Gallenzi, P.; Cordaro, M.; et al. Volumetric Analysis of Cleft Lip Deformity Using 3D Stereophotogrammetry. Ann. Ital. Chir. 2019, 90, 281–286. [Google Scholar] [PubMed]
- Susarla, S.M.; Berli, J.U.; Kumar, A. Midfacial Volumetric and Upper Lip Soft Tissue Changes After Le Fort I Advancement of the Cleft Maxilla. J. Oral. Maxillofac. Surg. 2015, 73, 708–718. [Google Scholar] [CrossRef] [PubMed]
- van Loon, B.; Maal, T.J.; Plooij, J.M.; Ingels, K.J.; Borstlap, W.A.; Kuijpers-Jagtman, A.M.; Spauwen, P.H.; Bergé, S.J. 3D Stereophotogrammetric Assessment of Pre- and Postoperative Volumetric Changes in the Cleft Lip and Palate Nose. Int. J. Oral. Maxillofac. Surg. 2010, 39, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Vaughan, S.M.; Kau, C.H.; Waite, P.D. Novel Three-Dimensional Understanding of Maxillary Cleft Distraction. J. Craniofacial Surg. 2016, 27, 1462–1464. [Google Scholar] [CrossRef] [PubMed]
- Heike, C.L.; Cunningham, M.L.; Hing, A.V.; Stuhaug, E.; Starr, J.R. Picture Perfect? Reliability of Craniofacial Anthropometry Using Three-Dimensional Digital Stereophotogrammetry. Plast. Reconstr. Surg. 2009, 124, 1261–1272. [Google Scholar] [CrossRef] [PubMed]
- Gibelli, D.; Pucciarelli, V.; Cappella, A.; Dolci, C.; Sforza, C. Are Portable Stereophotogrammetric Devices Reliable in Facial Imaging? A Validation Study of VECTRA H1 Device. J. Oral. Maxillofac. Surg. 2018, 76, 1772–1784. [Google Scholar] [CrossRef]
- Hall, R.L. Energetics of Nose and Mouth Breathing, Body Size, Body Composition, and Nose Volume in Young Adult Males and Females. Am. J. Human. Biol. 2005, 17, 321–330. [Google Scholar] [CrossRef]
- Tzou, C.-H.J.; Artner, N.M.; Pona, I.; Hold, A.; Placheta, E.; Kropatsch, W.G.; Frey, M. Comparison of Three-Dimensional Surface-Imaging Systems. J. Plast. Reconstr. Aesthetic Surg. 2014, 67, 489–497. [Google Scholar] [CrossRef]
- Fastuca, R.; Campobasso, A.; Zecca, P.A.; Caprioglio, A. 3D Facial Soft Tissue Changes after Rapid Maxillary Expansion on Primary Teeth: A Randomized Clinical Trial. Orthod. Craniofac Res. 2018, 21, 140–145. [Google Scholar] [CrossRef]
- Miranda, R.E.D.; Matayoshi, S.; Brabo, J.L.; Miyoshi, L.H. Use of Stereophotogrammetry for Measuring the Volume of External Facial Anatomy: A Systematic Review. Rev. Bras. Cir. Plástica RBCP Braz. J. Plast. Sugery 2018, 33, 572–579. [Google Scholar] [CrossRef]
- Silva, R.; Silva, B.; Fernandes, C.; Morouço, P.; Alves, N.; Veloso, A. A Review on 3D Scanners Studies for Producing Customized Orthoses. Sensors 2024, 24, 1373. [Google Scholar] [CrossRef]
- Azzi, A.J.; Hilzenrat, R.; Viezel-Mathieu, A.; Hemmerling, T.; Gilardino, M. A Review of Objective Measurement of Flap Volume in Reconstructive Surgery. Plast. Reconstr. Surg. Glob. Open 2018, 6, e1752. [Google Scholar] [CrossRef] [PubMed]
- Persing, S.; Timberlake, A.; Madari, S.; Steinbacher, D. Three-Dimensional Imaging in Rhinoplasty: A Comparison of the Simulated versus Actual Result. Aesthetic Plast. Surg. 2018, 42, 1331–1335. [Google Scholar] [CrossRef]
- Topsakal, O.; Sawyer, P.; Akinci, T.C.; Topsakal, E.; Celikoyar, M.M. Reliability and Agreement of Free Web-Based 3D Software for Computing Facial Area and Volume Measurements. BioMedInformatics 2024, 4, 690–708. [Google Scholar] [CrossRef]
- Lewyllie, A.; Cadenas De Llano-Pérula, M.; Verdonck, A.; Willems, G. Three-Dimensional Imaging of Soft and Hard Facial Tissues in Patients with Craniofacial Syndromes: A Systematic Review of Methodological Quality. Dentomaxillofac Radiol. 2018, 47, 20170154. [Google Scholar] [CrossRef] [PubMed]
- Todorović, J.; Zelić, M.; Jerkić, L. Eating and Swallowing Disorders in Children with Cleft Lip and/or Palate. Acta Fac. Medicae Naissensis 2022, 39, 5–13. [Google Scholar] [CrossRef]
- Kosowski, T.; Weathers, W.; Wolfswinkel, E.; Ridgway, E. Cleft Palate. Semin. Plast. Surg. 2013, 26, 164–169. [Google Scholar] [CrossRef]
- Haleem, A.; Javaid, M.; Singh, R.P.; Rab, S.; Suman, R.; Kumar, L.; Khan, I.H. Exploring the Potential of 3D Scanning in Industry 4.0: An Overview. Int. J. Cogn. Comput. Eng. 2022, 3, 161–171. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scopus | |
| TITLE-ABS-KEY(“3D imaging” OR “Laser scan*” OR “Facial imaging” OR “Stereophotogrammetry” OR “Surface imaging” OR “Topograph*”) AND ALL (volumetr* OR “volume measur*” OR soft tissue measurement) AND ALL(“Cleft lip” OR “Cleft palate” OR syndrom* OR dysmorph* OR disorder* OR deform*) AND PUBYEAR AFT 2002 | |
| Embase | |
| ‘3d imag*’ OR ‘3-d imag*’ OR ‘three-dimensional imag*’ OR ‘laser scan*’ OR ‘facial imaging’ OR ‘stereophotogrammetry’/exp OR ‘stereophotogrammetry’ OR ‘surface imaging’ OR ‘topograph*’ | #1 |
| ‘volumetr*’ OR ‘volume measur*’ OR ‘soft tissue measurement’ | #2 |
| ‘cleft lip’ OR ‘cleft palate’ OR ‘syndrom’ OR ‘dysmorph*’ OR ‘disorder*’ OR ‘deform*’ | #3 |
| #1 AND #2 AND #3 AND [2002–2024]/py | #4 |
| PubMed | |
| ((“3D imaging” OR “laser scan*” OR “Facial imaging” OR “Stereophotogrammetry” OR “imaging, three dimensional” OR “Surface imaging” OR “topograph*”) AND (“volumetr*” OR “volume measur*” OR (“soft” AND (“tissue s” OR “tissues” OR “tissues” OR “tissue”) AND (“measurability” OR “measurable” OR “measurably” OR “measure s” OR “measureable” OR “measured” OR “measurement” OR “measurement s” OR “measurements” OR “measurer” OR “measurers” OR “measuring” OR “measurings” OR “measurment” OR “measurments” OR “weights and measures” OR (“weights” AND “measures”) OR “weights and measures” OR “measure” OR “measures”))) AND (“Cleft lip” OR “Cleft palate” OR “syndrom*” OR “dysmorph*” OR “disorder*” OR “deform*”)) AND (2002:2024[pdat]) | |
| Web of Science | |
| ALL = (“3D imag*” OR “3-D imag*” OR “Three-dimensional imag*” OR “Laser scan*” OR “Facial imaging” OR “Stereophotogrammetry” OR “Surface imaging” OR “Topograph*”) | #1 |
| ALL = (volumetr* OR “volume measur*” OR soft tissue measurement) | #2 |
| ALL = (“Cleft lip” OR “Cleft palate” OR syndrom* OR dysmorph* OR disorder* OR deform*) | #3 |
| #1 AND #2 AND #3 and 2002 or 2003 or 2004 or 2005 or 2006 or 2007 or 2008 or 2009 or 2010 or 2011 or 2012 or 2013 or 2014 or 2015 or 2016 or 2017 or 2018 or 2019 or 2020 or 2021 or 2022 or 2023 or 2024 (Publication Years) | #4 |
| Patients Age-Class | Number of Studies | Number of Patients | |
|---|---|---|---|
| Only Children (<13 yo) | I + P + S | 7 | 269 |
| Only Teenagers (13 to 18 yo) | T | 2 | 2 |
| Only Adults (≥18 yo) | A | 1 | 1 |
| Subjects < 18 yo | C + T | 1 | 12 (10C, 2T) |
| Subjects ≥ 13 yo | T + A | 2 | 23 |
| Subadults and adults | C + T + A | 4 | 169 |
| Total | 17 | 476 | |
| Pathology | Number of Studies | Number of Patients | |
|---|---|---|---|
| Cleft Lip and/or Palate | Unilateral Cleft Lip | 10 | 143 |
| Unilateral Cleft Lip and Palate | 108 | ||
| Bilateral Cleft Lip | 14 | ||
| Bilateral Cleft Lip and Palate | 63 | ||
| Total CL/P | 10 | 328 | |
| Syndromes | Down | 2 | 92 |
| Moebius | 1 | 26 | |
| Hemifacial microsomia | 1 | 1 | |
| Parry-Romberg | 1 | 1 | |
| Marfan | 1 | 16 | |
| Craniosynostosis: Crouzon Apert Pfeiffer Saethre–Chotzen Unknown | 1 | 12: 5 3 2 1 1 | |
| Total Syndromes | 7 | 148 | |
| Total | 17 | 476 | |
| First Author (Year of Publication) | Pathology/ Syndrome | Sample Size | Age Group of Patients | Mean Age | Number of Females (% of Females) | Ethnicity/ Country of Origin |
|---|---|---|---|---|---|---|
| Ferrario et al. (2004) [35] | Down syndrome | 28 | S, T, A | Males: 26.4 ± 9.4 yo Range: 12–41 yoFemales: 27.5 ± 8.9 yo Range: 15–45 yo | 11 (39%) | Northern Italy |
| Sforza et al. (2009) [36] | Moebius syndrome | 26 | P, S, T, A | 17 ± 14 yo Range: 3–52 yo | 14 (54%) | NA |
| Jayaratne et al. (2010) [42] | Hemifacial microsomia | 1 | A | 19 yo | 1 (100%) | Asian * |
| Van Loon et al. (2010) [49] | UCL and UCLP | Total 12 | T, A | 18 § yo Range: 13–40 yo | 4 (33%) | NA |
| UCL 2 | ||||||
| UCLP 10 | ||||||
| Sforza et al. (2011) [37] | Down syndrome | 64 | P, S, T, A | 15 ± 7 yo Range 4–34 yo | 18 (28%) | North Sudan with North African origins |
| Chan et al. (2013) [41] | Crouzon, Apert, Pfeiffer, Saethre-Chotzen syndromes | 12 | S, T | 10.1 yo | NA | NA |
| Pucciarelli et al. (2015) [45] | UCLP | 32 | I | 10.5 ± 4.8 days | 15 (47%) | NA |
| Susarla et al. (2015) [48] | UCLP and BCLP | Total 11 | T, A | 17.9 ± 1.3 yo | 4 (36%) | NA |
| UCLP 6 | ||||||
| BCLP 5 | ||||||
| Vaughan et al. (2016) [50] | UCLP | 1 | T | 14 yo | NA | NA |
| Mercan et al. (2018) [43] | UCL | Total 89 | I, S | 30 (34%) | Mixed: Caucasian 44 Asian 23 Native American 1 Mixed Caucasian 7 Other 9 Not specififed 5 | |
| Group A 45 | Group A Pre-surgery (T1) 7.5 mo Post-surgery (T2) 10 mo | Group A 13 (29%) | ||||
| Group B 44 | Group B Post-surgery 9.5 yo | Group B 17 (39%) | ||||
| Ozdemir et al. (2018) [44] | UCLP and BCLP | Total 51 | S, T, A | NA | NA | |
| UCLP 29 | UCLP group: 15.45 ± 5.15 yo | |||||
| BCLP 22 | BCLP group: 16.18 ± 5.89 yo | |||||
| Paoloni et al. (2018) [40] | Marfan syndrome | 16 | S | 8.8 ± 1.5 yo | 7 (49%) | Caucasian |
| Pucciarelli et al. (2018) [46] | Parry-Romberg syndrome | 1 | T | 15 yo | 0 (0%) | Caucasian * |
| Rizzo et al. (2019) [47] | UCLP | 10 | I | 3 mo | 3 (30%) | NA |
| Ambrosio et al. (2021) [38] | BCL and BCLP | Total 50 | I | Pre-surgery (T1): 0.41 ± 0.16 yo | NA | NA |
| BCL 14 | Post-cheiloplasty (T2): 1.33 ± 0.33 yo | |||||
| BCLP 36 | Post-palatoplasty (T3): 2.45 ± 0.45 yo | |||||
| Ambrosio et al. (2022) [27] | UCL and UCLP | Total 41 | I | Pre-surgery (T1): 0.35 ± 0.07 yo | 17 (41%) | NA |
| UCL 21 | Post-cheiloplasty (T2): 1.30 ± 0.18 yo | UCL 11 (52%) | ||||
| UCLP 20 | Post-palatoplasty (T3): 2.1 ± 0.22 yo | UCLP 6 (30%) | ||||
| Chattopadhyay et al. (2023) [39] | UCL | 31 | I | Pre-surgery (T1): 5 mo range: 3–8 mo Post-surgery (T2): after 3 weeks Post-surgery (T3): after 2 years | 13 (42%) | NA |
| First author (Year of Publication) | Pathology/ Syndrome | Scanning System Type | Type of Acquisition | Software Associate with Device | Software | Structures Analysed | ROI Selection Protocol | Volume Calculation Protocol | Protocol Validation |
|---|---|---|---|---|---|---|---|---|---|
| Ferrario et al. (2004) [35] | Down syndrome | Electromechanical digitizer (Microscribe G2) | Direct acquisition | No | In-house-built software | Lip and Nose | Use of anatomical landmarks | Approximation with polyhedra using a custom computer program for offline calculation | Yes, in previous studies |
| Sforza et al. (2009) [36] | Moebius syndrome | Electromechanical digitizer (Microscribe G2) | Direct acquisition | No | In-house-built software | Whole face, forehead, maxilla, mandible and nose | Use of anatomical landmarks and planes | Approximation with polyhedra using a custom computer program for offline calculation | Yes, in previous studies |
| Jayaratne et al. (2010) [42] | Hemifacial Microsomia | Stereophotogrammetry (3dMD face) | Direct acquisition | Yes | Manufacturer software | Maxilla and mandibular areas | NA | Registration and superimposition of post- on pre-operative facial image to automatically calculate volumetric changes | Only reliability |
| Van Loon et al. (2010) [49] | UCL and UCLP | Stereophotogrammetry (3dMD face) | Direct acquisition | Yes, partially | Manufacturer software (3dMDpatient version 3.0.1) and Maxilim software version 2.2.2.1 | Nose | Use of landmarks-based planes | NA | Only reliability |
| Sforza et al. (2011) [37] | Down syndrome | Laser scanning (FastSCAN Cobra) | Direct acquisition | No | Rhinoceros Nurbs for Windows 4.0 software | Nasolabial area | Use of anatomical landmarks | Approximation with polyhedra using a custom computer program for offline calculation | Yes, in previous studies |
| Chan et al. (2013) [41] | Crouzon, Apert, Pfeiffer, Saethre–Chotzen syndromes | Stereophotogrammetry (MU-4 Imaging System) | Direct acquisition | Yes | Manufacturer software | Whole face | Entire 3D model | Registration and superimposition of post- on pre-operative facial image to automatically calculate volumetric changes | Unspecified |
| Pucciarelli et al. (2015) [45] | UCLP | Stereophotogrammetry (VECTRA 3D) | Indirect acquisition from casts | Yes | Manufacturer software | Palate | Use of contouring points | Projection of the ROI’s points on a virtual plane, registration of the two surfaces for closing the ROI, and automatic calculation of the volume | Yes |
| Susarla et al. (2015) [48] | CLP | Stereophotogrammetry (Vectra XT) | Direct acquisition | Yes | Manufacturer software | Nasolabial area | Use of anatomical landmarks and manual selection | Registration and superimposition of post- on pre-operative facial image to automatically calculate volumetric changes | Unspecified |
| Vaughan et al. (2016) [50] | UCLP | Stereophotogrammetry (3dMD face) | Direct acquisition | No | Rapidform 2006 and Invivo version 5.2.3 software | Maxilla | NA | NA | Only reliability |
| Mercan et al. (2018) [43] | UCL | Stereophotogrammetry (3dMD cranial system) | Direct acquisition | No | In-house-built software | Nose | Use of horizontal contours and reference planes | Approximation of volume as the sum of the areas under left and right sides over all reference planes (own calculation through contours/curvature analysis) | Unspecified |
| Ozdemir et al. (2018) [44] | UCLP and BCLP | Stereophotogrammetry (3dMD face) | Direct acquisition | Yes | Manufacturer software (3dMDvultus version 2.3.0.2) | Nasolabial area and chin | Use of horizontal and vertical reference planes | NA | Only reliability |
| Paoloni et al. (2018) [40] | Marfan syndrome | Laser scanning (OrthoXscan) | Indirect acquisition from casts | NA | NA | Palate | Use of landmarks-based planes | Virtual volume enclosed by the digital casts and planes used for ROI selection | Only reliability |
| Pucciarelli et al. (2018) [46] | Parry–Romberg Syndrome | Stereophotogrammetry (VECTRA 3D) | Direct acquisition | Yes | Manufacturer software | Trigeminal facial thirds | Use of anatomical landmarks | Registration and superimposition of post- on pre-operative facial image to automatically calculate volumetric changes | Unspecified |
| Rizzo et al. (2019) [47] | UCLP | Stereophotogrammetry (3dMD trio) | Direct acquisition | Yes, partially | Manufacturer software and GeoMagic Wrap | Upper lip | Use of anatomical landmarks | Use of a virtual plane for closing the ROI, and automatic computation of the volume | Only reliability |
| Ambrosio et al. (2021) [38] | CLP | Laser scanning (R700 Scanner) | Indirect acquisition from casts | No | Mirror Imaging Software | Palate | Use of contouring points | Projection of the ROI’s points on a virtual plane, registration of the two surfaces for closing the ROI, and automatic calculation of the volume [45] | Yes, in previous studies |
| Ambrosio et al. (2022) [27] | UCL and UCLP | Laser scanning (R700 Scanner) | Indirect acquisition from casts | No | Mirror Imaging Software | Palate | Use of contouring points | Projection of the ROI’s points on a virtual plane, registration of the two surfaces for closing the ROI, and automatic calculation of the volume [45] | Yes, in previous studies |
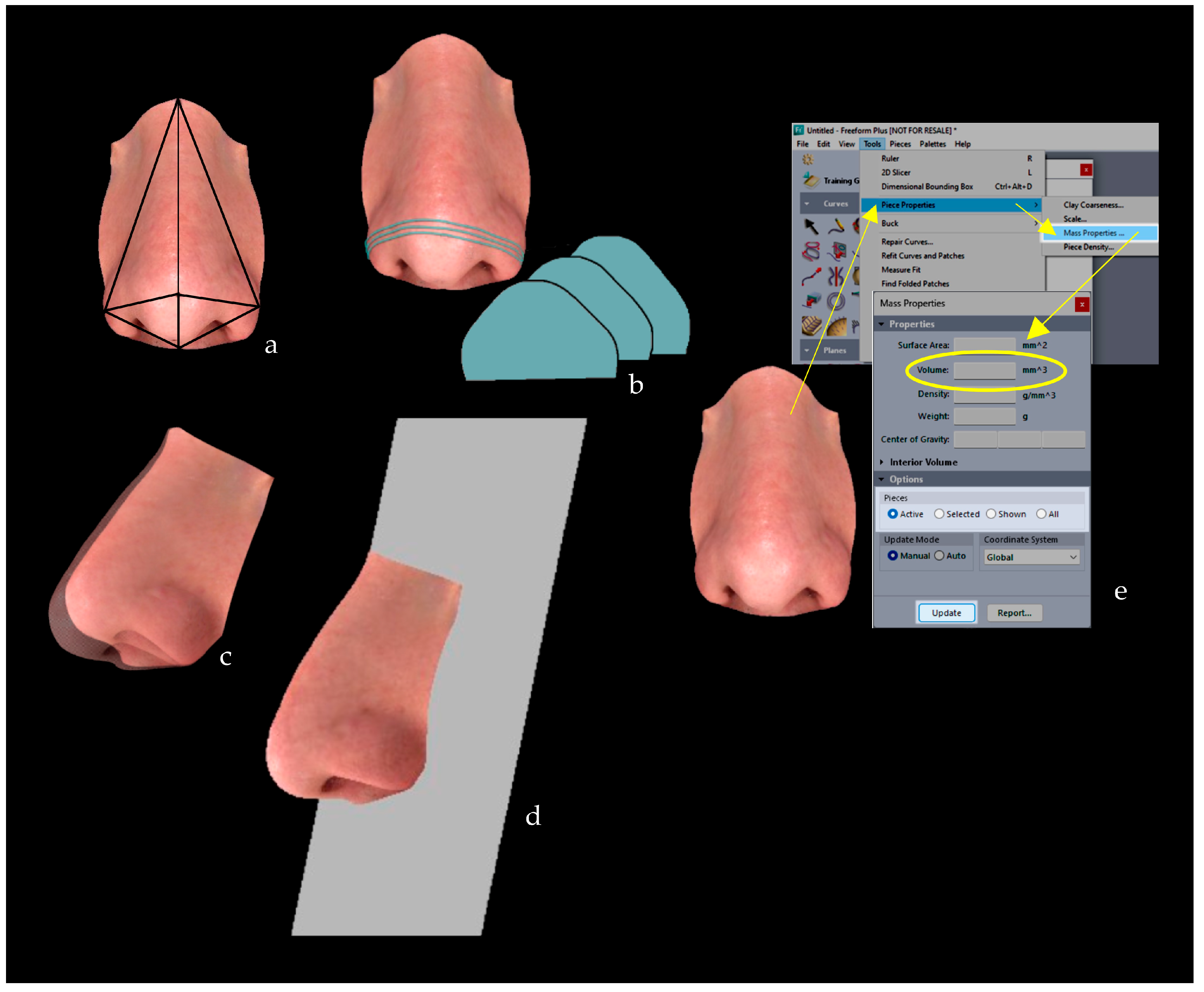
| Chattopadhyay et al. (2023) [39] | UCL | Laser Scanning (Artec Space Spider) | Direct acquisition | No | GeoMagic Freeform Plus software version V2017 | Nose | Use of anatomical landmarks-based planes | Automatic calculation of the ROI’s volume using the “Piece Property” function of the software | Unspecified |
| Author | Pathology/ Syndrome | N | Structure Analysed | Volume Pre-Surgery (cm3) | Volume Post-Surgery (cm3) |
|---|---|---|---|---|---|
| Van Loon et al. (2010) [49] | UCL | 12 | Cleft side nose | T1: 16.49 (3.87) # | T2: 17.45 (4.31) # |
| UCLP | Non-cleft side nose | T1: 18.59 (4.79) # | T2: 18.86 (4.73) # | ||
| Pucciarelli et al. (2015) [45] | UCLP | 16 | Greater palatal segment after PNAM | T1: 1.08 (0.47) | T2: 1.09 (0.49) T3: 1.22 (0.56) |
| Minor palatal segment after PNAM | T1: 0.53 (0.25) | T2: 0.48 (0.26) T3: 0.65 (0.29) | |||
| 16 | Greater palatal segment after Hotz’s | T1: 0.91 (0.29) | T2: 1.09 (0.37) T3: 1.38 (0.51) | ||
| Minor palatal segment after Hotz’s | T1: 0.52 (0.21) | T2: 0.68 (0.23) T3: 0.81 (0.25) | |||
| Vaughan et al. (2016) [50] | UCLP | 1 | Maxilla | T1: 0.36 | T2: 0.41 |
| Ozdemir et al. (2018) [44] | UCLP | 29 | Upper lip | NA | T2: 2.43 (1.03) |
| Lower lip | NA | T1: 3.08 (1.28) | |||
| Nose | NA | T2: 12.44 (3.81) | |||
| Upper lip and paranasal area | NA | T2: 27.7 (5.83) | |||
| Upper lip and paranasal area without nose | NA | T2: 15.19 (4.01) | |||
| Lower lip and chin | NA | T2: 4.55 (2.46) | |||
| BCLP | 22 | Upper lip | NA | T2: 2.52 (1.11) | |
| Lower lip | NA | T2: 3.44 (1.21) | |||
| Nose | NA | T2: 13.31 (4.09) | |||
| Upper lip and paranasal area | NA | T2: 28.44 (4.28) | |||
| Upper lip and paranasal area without nose | NA | T2: 16.12 (3.62) | |||
| Lower lip and chin | NA | T2: 5.93 (3.16) | |||
| Paoloni et al. (2018) [40] | Marfan syndrome | 16 | Palate | T1: 2.58 (0.59) | NA |
| Rizzo et al. (2019) [47] | UCL | 10 | Upper lip | T1: 1.64§ | T2: 2.12§ |
| Ambrosio et al. (2021) [38] | BCL | 14 | Sum of palatal segments and palatal arch | T1: 0.97 (0.77) | T2: 2.07 (0.77) |
| BCLP | 36 | Sum of palatal segments | T1: 3.22 (0.91) | T2: 4.40 (1.26) T3: 2.68 (0.97) | |
| Ambrosio et al. (2022) [27] | UCL | 21 | Sum of palatal segments | T1: 0.58 (0.76) * | T2: 1.48 (2.72) * |
| UCLP | 20 | Sum of palatal segments | T1: 1.65 (0.99) * | T2: 3.05 (1.33) * T3: 2.25 (1.43) * | |
| Chattopadhyay et al. (2023) [39] | UCL | 31 | Cleft side nose | T1: 0.004 § | T2: 0.005 § T3: 0.03 (0.002) |
| 31 | Non-cleft side nose | NA | T3: 0.03 (0.002) |
| Author | Pathology/ Syndrome | N | Structure Analysed | Volumetric Changes between Post- and Pre-Surgery 3D Model (cm3) |
|---|---|---|---|---|
| Jayaratne et al. (2010) [42] | Hemifacial Microsomia | 1 | Mid-lower face (left side) | T1Mirrored-T1: −16.41 T2-T1: 20.23 T3-T1: 30.84 T4-T1: 27.08 T5-T1: 23.81 T6-T1: 22.38 T7-T1: 21.43 |
| Chan et al. (2013) [41] | Crouzon syndrome | 5 | Face | T2-T1: 107 (14) # T3-T1: 102 (12) # |
| Apert syndrome | 3 | T2-T1: 92 (5.5) # T3-T1: 88 (5.5) # | ||
| Pfeiffer syndrome | 2 | T2-T1: 101.5 (11) # T3-T1: 95.5 (8) # | ||
| Saethre–Chotzen syndrome | 1 | T2-T1: 74 T3-T1: 71 | ||
| Unknown syndrome | 1 | T2-T1: 105 T3-T1: 102 | ||
| Susarla et al. (2015) [48] | UCLP | 11 | Midface | T2-T1: 12.2 (5.7) |
| BCLP | ||||
| Pucciarelli et al. (2018) [46] | Parry–Romberg syndrome | 1 | Middle third (trigeminal) | T2-T1: 1.6 |
| Lower third (trigeminal) | T2-T1: 2.5 | |||
| Middle + Lower third | T2-T1: 4.1 |
| Author | Pathology/ Syndrome | N | Structure Analysed | Comparison with Control Side or Subjects (Dimensionless Index) |
|---|---|---|---|---|
| Ferrario et al. (2004) [35] | Down Syndrome | 28 | Nose | −1.31 (1.19) Z |
| Upper lip | 0.07 (1.12) Z | |||
| Lower lip | 1.04 (0.71) Z | |||
| Lips | −0.51 (0.68) Z | |||
| Sforza et al. (2009) [36] | Moebius Syndrome | 26 | Face | −0.38 (1.14) Z |
| Forehead | −0.45 (1.19) Z | |||
| Maxilla | 0.17 (1.03) Z | |||
| Mandible | −0.78 (1.27) Z | |||
| Nose | −0.92 (1.40) Z | |||
| Sforza et al. (2011) [37] | Down Syndrome | 64 | Nose | −0.20 (1.12) Z |
| Upper Lip | −0.09 (1.33) Z | |||
| Lips | −0.40 (1.31) Z | |||
| Mercan et al. (2018) [43] | CL | 45 | Nose | T1: 1.59 §R T2: 1.20 §R |
| 44 | T2: 1.18 §R |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cappella, A.; Gaffuri, F.; Yang, J.; Tartaglia, F.C.; Solazzo, R.; Inchingolo, F.; Tartaglia, G.M.; Sforza, C. Volumetric Analyses of Dysmorphic Maxillofacial Structures Using 3D Surface-Based Approaches: A Scoping Review. J. Clin. Med. 2024, 13, 4740. https://doi.org/10.3390/jcm13164740
Cappella A, Gaffuri F, Yang J, Tartaglia FC, Solazzo R, Inchingolo F, Tartaglia GM, Sforza C. Volumetric Analyses of Dysmorphic Maxillofacial Structures Using 3D Surface-Based Approaches: A Scoping Review. Journal of Clinical Medicine. 2024; 13(16):4740. https://doi.org/10.3390/jcm13164740
Chicago/Turabian StyleCappella, Annalisa, Francesca Gaffuri, Josh Yang, Francesco Carlo Tartaglia, Riccardo Solazzo, Francesco Inchingolo, Gianluca Martino Tartaglia, and Chiarella Sforza. 2024. "Volumetric Analyses of Dysmorphic Maxillofacial Structures Using 3D Surface-Based Approaches: A Scoping Review" Journal of Clinical Medicine 13, no. 16: 4740. https://doi.org/10.3390/jcm13164740
APA StyleCappella, A., Gaffuri, F., Yang, J., Tartaglia, F. C., Solazzo, R., Inchingolo, F., Tartaglia, G. M., & Sforza, C. (2024). Volumetric Analyses of Dysmorphic Maxillofacial Structures Using 3D Surface-Based Approaches: A Scoping Review. Journal of Clinical Medicine, 13(16), 4740. https://doi.org/10.3390/jcm13164740