
Diabetes Management Based on the Phenotype and Stage of the Disease: An Expert Proposal from the AGORA Diabetes Collaborative Group
 , , and
, , and {kind=link}
Abstract
1. Introduction
2. Update on (Type 2) Diabetes Classification
3. Update on (Type 2) Diabetes Staging
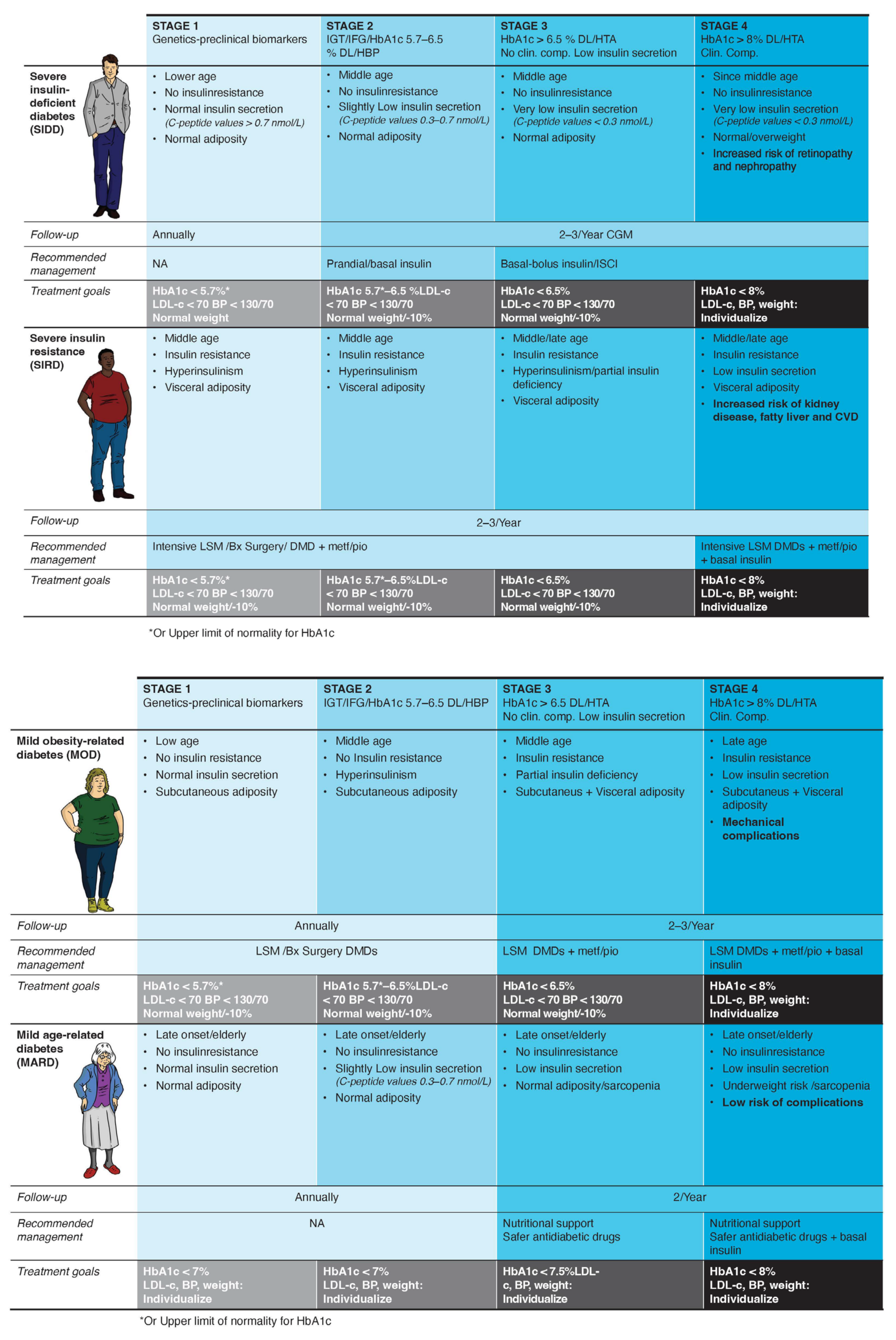
4. Proposal of Classification and Therapeutic Algorithm
- Diabetes syndrome with severe insulin deficiency: Early detection and treatment of insulin deficiency are critical to avoid microvascular complications [37]. The use of continuous glucose monitoring is strongly recommended to guide insulin requirements by providing both real-time and predictive glycemic data [38].
- Diabetes syndrome associated with severe insulin resistance: Early and intensive treatment is crucial for delaying progression. Abnormal adiposity distribution and function are usually accompanied by inflammation, dyslipidemia, hypertension, and fatty liver disease [39]. Thus, this subgroup is likely to benefit from enhanced monitoring and support and the early use of diabetes/disease-modifying drugs (DMDs), such as sodium glucose co-transporter type 2 inhibitors (SGLT2i) and glucagon-like peptide-1 receptor agonists (GLP-1 RA), which are prognosis-changing agents [40].
- Mild diabetes associated with obesity: This phenotype is characterized by subclinical hyperinsulinism. Treatment of this subset of patients primarily involves weight loss, with a potential role for GLP-1 RA in enhancing remission of the disease beyond healthy habits [41].
- Mild age-related diabetes: This subgroup includes older people who have the most benign course of the disease, mainly caused by age-related impaired beta-cell function. In fact, when adjusted for current age, older age at T2D diagnosis is associated with a reduced risk of mortality and microvascular and macrovascular complications [42]. Conservative management, including medical monitoring and pharmacological treatment, is advisable.
5. Methods and Values Recommended for the Clinical Classification of Diabetes
- Autoimmunity
- Age
- Insulin secretion
- C-peptide levels < 0.3 nmol/L: a multiple-insulin regimen is recommended as for T1D.
- C-peptide values ≥ 0.3 and <0.7 nmol/L: non-insulin agents plus basal insulin should be considered.
- C-peptide values > 0.7 nmol/L: non-insulin agents according to the specific phenotype are recommended.
- Insulin resistance
- Adiposity
6. Limitations, Gaps, and Further Research
7. Conclusions and Call to Action
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- American Diabetes Association Professional Practice Committee 2. Diagnosis and Classification of Diabetes: Standards of Care in Diabetes—2024. Diabetes Care 2024, 47, S20–S42. [Google Scholar] [CrossRef]
- Aroda, V.R.; Eckel, R.H. Reconsidering the Role of Glycaemic Control in Cardiovascular Disease Risk in Type 2 Diabetes: A 21st Century Assessment. Diabetes. Obes. Metab. 2022, 24, 2297–2308. [Google Scholar] [CrossRef]
- Silvia, P.; Simona, Z.; Ernesto, M.; Raffaella, B. “H” for Heterogeneity in the Algorithm for Type 2 Diabetes Management. Curr. Diab. Rep. 2020, 20, 14. [Google Scholar] [CrossRef] [PubMed]
- Redondo, M.J.; Hagopian, W.A.; Oram, R.; Steck, A.K.; Vehik, K.; Weedon, M.; Balasubramanyam, A.; Dabelea, D. The Clinical Consequences of Heterogeneity within and between Different Diabetes Types. Diabetologia 2020, 63, 2040–2048. [Google Scholar] [CrossRef] [PubMed]
- Ahlqvist, E.; Storm, P.; Käräjämäki, A.; Martinell, M.; Dorkhan, M.; Carlsson, A.; Vikman, P.; Prasad, R.B.; Aly, D.M.; Almgren, P.; et al. Novel Subgroups of Adult-Onset Diabetes and Their Association with Outcomes: A Data-Driven Cluster Analysis of Six Variables. Lancet Diabetes Endocrinol. 2018, 6, 361–369. [Google Scholar] [CrossRef]
- Udler, M.S.; Kim, J.; von Grotthuss, M.; Bonàs-Guarch, S.; Cole, J.B.; Chiou, J.; Boehnke, M.; Laakso, M.; Atzmon, G.; Glaser, B.; et al. Type 2 Diabetes Genetic Loci Informed by Multi-Trait Associations Point to Disease Mechanisms and Subtypes: A Soft Clustering Analysis. PLoS Med. 2018, 15, e1002654. [Google Scholar] [CrossRef]
- Morze, J.; Wittenbecher, C.; Schwingshackl, L.; Danielewicz, A.; Rynkiewicz, A.; Hu, F.B.; Guasch-Ferré, M. Metabolomics and Type 2 Diabetes Risk: An Updated Systematic Review and Meta-Analysis of Prospective Cohort Studies. Diabetes Care 2022, 45, 1013–1024. [Google Scholar] [CrossRef]
- Ghatan, S.; van Rooij, J.; van Hoek, M.; Boer, C.G.; Felix, J.F.; Kavousi, M.; Jaddoe, V.W.; Sijbrands, E.J.G.; Medina-Gomez, C.; Rivadeneira, F.; et al. Defining Type 2 Diabetes Polygenic Risk Scores through Colocalization and Network-Based Clustering of Metabolic Trait Genetic Associations. Genome Med. 2024, 16, 10. [Google Scholar] [CrossRef] [PubMed]
- Chung, W.K.; Erion, K.; Florez, J.C.; Hattersley, A.T.; Hivert, M.-F.; Lee, C.G.; McCarthy, M.I.; Nolan, J.J.; Norris, J.M.; Pearson, E.R.; et al. Precision Medicine in Diabetes: A Consensus Report from the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia 2020, 63, 1671–1693. [Google Scholar] [CrossRef]
- Cai, X.; Zhang, Y.; Li, M.; Wu, J.H.; Mai, L.; Li, J.; Yang, Y.; Hu, Y.; Huang, Y. Association between Prediabetes and Risk of All Cause Mortality and Cardiovascular Disease: Updated Meta-Analysis. BMJ 2020, 370, m2297. [Google Scholar] [CrossRef]
- Honigberg, M.C.; Zekavat, S.M.; Pirruccello, J.P.; Natarajan, P.; Vaduganathan, M. Cardiovascular and Kidney Outcomes Across the Glycemic Spectrum: Insights From the UK Biobank. J. Am. Coll. Cardiol. 2021, 78, 453–464. [Google Scholar] [CrossRef]
- Hostalek, U. Global Epidemiology of Prediabetes-Present and Future Perspectives. Clin. Diabetes Endocrinol. 2019, 5, 5. [Google Scholar] [CrossRef]
- Insel, R.A.; Dunne, J.L.; Atkinson, M.A.; Chiang, J.L.; Dabelea, D.; Gottlieb, P.A.; Greenbaum, C.J.; Herold, K.C.; Krischer, J.P.; Lernmark, Å.; et al. Staging Presymptomatic Type 1 Diabetes: A Scientific Statement of JDRF, the Endocrine Society, and the American Diabetes Association. Diabetes Care 2015, 38, 1964–1974. [Google Scholar] [CrossRef] [PubMed]
- Redondo, M.J.; Evans-Molina, C.; Steck, A.K.; Atkinson, M.A.; Sosenko, J. The Influence of Type 2 Diabetes-Associated Factors on Type 1 Diabetes. Diabetes Care 2019, 42, 1357–1364. [Google Scholar] [CrossRef] [PubMed]
- WHO Study Group Diabetes Mellitus. World Health Organ. Tech. Rep. Ser. 1985, 727, 1–113.
- UK Prospective Diabetes Study (UKPDS) Group. Intensive Blood-Glucose Control with Sulphonylureas or Insulin Compared with Conventional Treatment and Risk of Complications in Patients with Type 2 Diabetes (UKPDS 33). Lancet 1998, 352, 837–853. [Google Scholar] [CrossRef]
- UK Prospective Diabetes Study (UKPDS) Group. Effect of Intensive Blood-Glucose Control with Metformin on Complications in Overweight Patients with Type 2 Diabetes (UKPDS 34). Lancet 1998, 352, 854–865. [Google Scholar] [CrossRef]
- Nathan, D.M.; Buse, J.B.; Davidson, M.B.; Heine, R.J.; Holman, R.R.; Sherwin, R.; Zinman, B. Management of Hyperglycemia in Type 2 Diabetes: A Consensus Algorithm for the Initiation and Adjustment of Therapy: A Consensus Statement from the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2006, 29, 1963–1972. [Google Scholar] [CrossRef]
- Wagner, R.; Heni, M.; Tabák, A.G.; Machann, J.; Schick, F.; Randrianarisoa, E.; Hrabě de Angelis, M.; Birkenfeld, A.L.; Stefan, N.; Peter, A.; et al. Pathophysiology-Based Subphenotyping of Individuals at Elevated Risk for Type 2 Diabetes. Nat. Med. 2021, 27, 49–57. [Google Scholar] [CrossRef]
- Slieker, R.C.; Donnelly, L.A.; Fitipaldi, H.; Bouland, G.A.; Giordano, G.N.; Åkerlund, M.; Gerl, M.J.; Ahlqvist, E.; Ali, A.; Dragan, I.; et al. Distinct Molecular Signatures of Clinical Clusters in People With Type 2 Diabetes: An IMI-RHAPSODY Study. Diabetes 2021, 70, 2683–2693. [Google Scholar] [CrossRef]
- Misra, S.; Wagner, R.; Ozkan, B.; Schön, M.; Sevilla-Gonzalez, M.; Prystupa, K.; Wang, C.C.; Kreienkamp, R.J.; Cromer, S.J.; Rooney, M.R.; et al. Precision Subclassification of Type 2 Diabetes: A Systematic Review. Commun. Med. 2023, 3, 138. [Google Scholar] [CrossRef]
- Nair, A.T.N.; Wesolowska-Andersen, A.; Brorsson, C.; Rajendrakumar, A.L.; Hapca, S.; Gan, S.; Dawed, A.Y.; Donnelly, L.A.; McCrimmon, R.; Doney, A.S.F.; et al. Heterogeneity in Phenotype, Disease Progression and Drug Response in Type 2 Diabetes. Nat. Med. 2022, 28, 982–988. [Google Scholar] [CrossRef]
- Shields, B.M.; Dennis, J.M.; Angwin, C.D.; Warren, F.; Henley, W.E.; Farmer, A.J.; Sattar, N.; Holman, R.R.; Jones, A.G.; Pearson, E.R.; et al. Patient Stratification for Determining Optimal Second-Line and Third-Line Therapy for Type 2 Diabetes: The TriMaster Study. Nat. Med. 2023, 29, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Zaharia, O.P.; Strassburger, K.; Strom, A.; Bönhof, G.J.; Karusheva, Y.; Antoniou, S.; Bódis, K.; Markgraf, D.F.; Burkart, V.; Müssig, K.; et al. Risk of Diabetes-Associated Diseases in Subgroups of Patients with Recent-Onset Diabetes: A 5-Year Follow-up Study. Lancet Diabetes Endocrinol. 2019, 7, 684–694. [Google Scholar] [CrossRef] [PubMed]
- Bello-Chavolla, O.Y.; Bahena-López, J.P.; Vargas-Vázquez, A.; Antonio-Villa, N.E.; Márquez-Salinas, A.; Fermín-Martínez, C.A.; Rojas, R.; Mehta, R.; Cruz-Bautista, I.; Hernández-Jiménez, S.; et al. Clinical Characterization of Data-Driven Diabetes Subgroups in Mexicans Using a Reproducible Machine Learning Approach. BMJ Open Diabetes Res. Care 2020, 8, e001550. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Yang, A.; Lau, E.S.H.; Zhang, X.; Fan, B.; Ma, R.C.W.; Kong, A.P.S.; Chow, E.; So, W.-Y.; Chan, J.C.N.; et al. 1-Year Weight Change after Diabetes Diagnosis and Long-Term Incidence and Sustainability of Remission of Type 2 Diabetes in Real-World Settings in Hong Kong: An Observational Cohort Study. PLoS Med. 2024, 21, e1004327. [Google Scholar] [CrossRef]
- Aedh, A.I.; Alshahrani, M.S.; Huneif, M.A.; Pryme, I.F.; Oruch, R. A Glimpse into Milestones of Insulin Resistance and an Updated Review of Its Management. Nutrients 2023, 15, 921. [Google Scholar] [CrossRef]
- Al-Mrabeh, A. Pathogenesis and Remission of Type 2 Diabetes: What Has the Twin Cycle Hypothesis Taught Us? Cardiovasc. Endocrinol. Metab. 2020, 9, 132–142. [Google Scholar] [CrossRef]
- Wu, S.L. Staging of Type 2 Diabetes Mellitus. Genet. Mol. Res. 2015, 14, 2118–2121. [Google Scholar] [CrossRef]
- Dar, M.S.; Bég, S.A. TNM Cancer Staging: Can It Help Develop a Novel Staging System for Type 2 Diabetes? Diabetes Metab. Syndr. Obes. 2018, 11, 845–853. [Google Scholar] [CrossRef]
- Mechanick, J.I.; Garber, A.J.; Grunberger, G.; Handelsman, Y.; Garvey, W.T. Dysglycemia-Based Chronic Disease: An American Association of Clinical Endocrinologists Position Statement. Endocr. Pract. 2018, 24, 995–1011. [Google Scholar] [CrossRef] [PubMed]
- González-Rivas, J.P.; Pavlovska, I.; Polcrova, A.; Nieto-Martínez, R.; Mechanick, J.I. Transcultural Lifestyle Medicine in Type 2 Diabetes Care: Narrative Review of the Literature. Am. J. Lifestyle Med. 2023, 17, 518–559. [Google Scholar] [CrossRef] [PubMed]
- Tobias, D.K.; Merino, J.; Ahmad, A.; Aiken, C.; Benham, J.L.; Bodhini, D.; Clark, A.L.; Colclough, K.; Corcoy, R.; Cromer, S.J.; et al. Second International Consensus Report on Gaps and Opportunities for the Clinical Translation of Precision Diabetes Medicine. Nat. Med. 2023, 29, 2438–2457. [Google Scholar] [CrossRef] [PubMed]
- Dennis, J.M.; Shields, B.M.; Henley, W.E.; Jones, A.G.; Hattersley, A.T. Disease Progression and Treatment Response in Data-Driven Subgroups of Type 2 Diabetes Compared with Models Based on Simple Clinical Features: An Analysis Using Clinical Trial Data. Lancet Diabetes Endocrinol. 2019, 7, 442–451. [Google Scholar] [CrossRef] [PubMed]
- Phillips, L.S.; Ratner, R.E.; Buse, J.B.; Kahn, S.E. We Can Change the Natural History of Type 2 Diabetes. Diabetes Care 2014, 37, 2668–2676. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association Professional Practice Committee 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Care in Diabetes—2024. Diabetes Care 2023, 47, S158–S178. [Google Scholar] [CrossRef]
- Li, Y.; Liu, Y.; Liu, S.; Gao, M.; Wang, W.; Chen, K.; Huang, L.; Liu, Y. Diabetic Vascular Diseases: Molecular Mechanisms and Therapeutic Strategies. Signal Transduct. Target. Ther. 2023, 8, 152. [Google Scholar] [CrossRef]
- Miller, E.M. Using Continuous Glucose Monitoring in Clinical Practice. Clin. Diabetes 2020, 38, 429–438. [Google Scholar] [CrossRef]
- Mechanick, J.I.; Farkouh, M.E.; Newman, J.D.; Garvey, W.T. Cardiometabolic-Based Chronic Disease, Adiposity and Dysglycemia Drivers: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 75, 525–538. [Google Scholar] [CrossRef]
- Mosenzon, O.; Del Prato, S.; Schechter, M.; Leiter, L.A.; Ceriello, A.; DeFronzo, R.A.; Raz, I. From Glucose Lowering Agents to Disease/Diabetes Modifying Drugs: A “SIMPLE” Approach for the Treatment of Type 2 Diabetes. Cardiovasc. Diabetol. 2021, 20, 92. [Google Scholar] [CrossRef]
- Sulu, C.; Yumuk, V.D. Treat Obesity to Treat Type 2 Diabetes Mellitus. Diabetes Ther. 2024, 15, 611–622. [Google Scholar] [CrossRef] [PubMed]
- Nanayakkara, N.; Curtis, A.J.; Heritier, S.; Gadowski, A.M.; Pavkov, M.E.; Kenealy, T.; Owens, D.R.; Thomas, R.L.; Song, S.; Wong, J.; et al. Impact of Age at Type 2 Diabetes Mellitus Diagnosis on Mortality and Vascular Complications: Systematic Review and Meta-Analyses. Diabetologia 2021, 64, 275–287. [Google Scholar] [CrossRef]
- American Diabetes Association Proffesional Practice Committee 13. Older Adults: Standards of Care in Diabetes-2024. Diabetes Care 2024, 47, S244–S257. [Google Scholar] [CrossRef] [PubMed]
- Buzzetti, R.; Tuomi, T.; Mauricio, D.; Pietropaolo, M.; Zhou, Z.; Pozzilli, P.; Leslie, R.D. Management of Latent Autoimmune Diabetes in Adults: A Consensus Statement From an International Expert Panel. Diabetes 2020, 69, 2037–2047. [Google Scholar] [CrossRef]
- Westacott, M.J.; Farnsworth, N.L.; St Clair, J.R.; Poffenberger, G.; Heintz, A.; Ludin, N.W.; Hart, N.J.; Powers, A.C.; Benninger, R.K.P. Age-Dependent Decline in the Coordinated [Ca(2+)] and Insulin Secretory Dynamics in Human Pancreatic Islets. Diabetes 2017, 66, 2436–2445. [Google Scholar] [CrossRef] [PubMed]
- Leighton, E.; Sainsbury, C.A.; Jones, G.C. A Practical Review of C-Peptide Testing in Diabetes. Diabetes Ther. 2017, 8, 475–487. [Google Scholar] [CrossRef]
- Gastaldelli, A. Measuring and Estimating Insulin Resistance in Clinical and Research Settings. Obesity 2022, 30, 1549–1563. [Google Scholar] [CrossRef]
- Sharma, V.R.; Matta, S.T.; Haymond, M.W.; Chung, S.T. Measuring Insulin Resistance in Humans. Horm. Res. Paediatr. 2020, 93, 577–588. [Google Scholar] [CrossRef] [PubMed]
- Yuge, H.; Okada, H.; Hamaguchi, M.; Kurogi, K.; Murata, H.; Ito, M.; Fukui, M. Triglycerides/HDL Cholesterol Ratio and Type 2 Diabetes Incidence: Panasonic Cohort Study 10. Cardiovasc. Diabetol. 2023, 22, 308. [Google Scholar] [CrossRef]
- Adab, P.; Pallan, M.; Whincup, P.H. Is BMI the Best Measure of Obesity? BMJ 2018, 360, k1274. [Google Scholar] [CrossRef]
- Krakauer, N.Y.; Krakauer, J.C. An Anthropometric Risk Index Based on Combining Height, Weight, Waist, and Hip Measurements. J. Obes. 2016, 2016, 8094275. [Google Scholar] [CrossRef] [PubMed]
- Krakauer, N.Y.; Krakauer, J.C. A New Body Shape Index Predicts Mortality Hazard Independently of Body Mass Index. PLoS ONE 2012, 7, e39504. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Peralta, F.; Abreu, C.; Cruz-Bravo, M.; Alcarria, E.; Gutierrez-Buey, G.; Krakauer, N.Y.; Krakauer, J.C. Relationship between “a Body Shape Index (ABSI)” and Body Composition in Obese Patients with Type 2 Diabetes. Diabetol. Metab. Syndr. 2018, 10, 21. [Google Scholar] [CrossRef] [PubMed]
- International Diabetes Federation IDF Diabetes Atlas, 10th Edn. Available online: https://www.diabetesatlas.org (accessed on 8 May 2024).
- Landgraf, R.; Aberle, J.; Birkenfeld, A.L.; Gallwitz, B.; Kellerer, M.; Klein, H.H.; Müller-Wieland, D.; Nauck, M.A.; Wiesner, T.; Siegel, E. Therapy of Type 2 Diabetes. Exp. Clin. Endocrinol. Diabetes 2024, 132, 340–388. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez-Peralta, F.; Pinés-Corrales, P.J.; Santos, E.; Cuesta, M.; González-Albarrán, O.; Azriel, S.; on behalf the AGORA Diabetes Collaborative Group. Diabetes Management Based on the Phenotype and Stage of the Disease: An Expert Proposal from the AGORA Diabetes Collaborative Group. J. Clin. Med. 2024, 13, 4839. https://doi.org/10.3390/jcm13164839
Gómez-Peralta F, Pinés-Corrales PJ, Santos E, Cuesta M, González-Albarrán O, Azriel S, on behalf the AGORA Diabetes Collaborative Group. Diabetes Management Based on the Phenotype and Stage of the Disease: An Expert Proposal from the AGORA Diabetes Collaborative Group. Journal of Clinical Medicine. 2024; 13(16):4839. https://doi.org/10.3390/jcm13164839
Chicago/Turabian StyleGómez-Peralta, Fernando, Pedro J. Pinés-Corrales, Estefanía Santos, Martín Cuesta, Olga González-Albarrán, Sharona Azriel, and on behalf the AGORA Diabetes Collaborative Group. 2024. "Diabetes Management Based on the Phenotype and Stage of the Disease: An Expert Proposal from the AGORA Diabetes Collaborative Group" Journal of Clinical Medicine 13, no. 16: 4839. https://doi.org/10.3390/jcm13164839
APA StyleGómez-Peralta, F., Pinés-Corrales, P. J., Santos, E., Cuesta, M., González-Albarrán, O., Azriel, S., & on behalf the AGORA Diabetes Collaborative Group. (2024). Diabetes Management Based on the Phenotype and Stage of the Disease: An Expert Proposal from the AGORA Diabetes Collaborative Group. Journal of Clinical Medicine, 13(16), 4839. https://doi.org/10.3390/jcm13164839