

The Respiratory Adjusted Shock Index at Admission Is a Valuable Predictor of In-Hospital Outcomes for Elderly Emergency Patients with Medical Diseases at a Japanese Community General Hospital

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Participants, and Ethics Statement
2.2. Statistical Analysis
3. Results
3.1. Patient Characteristics
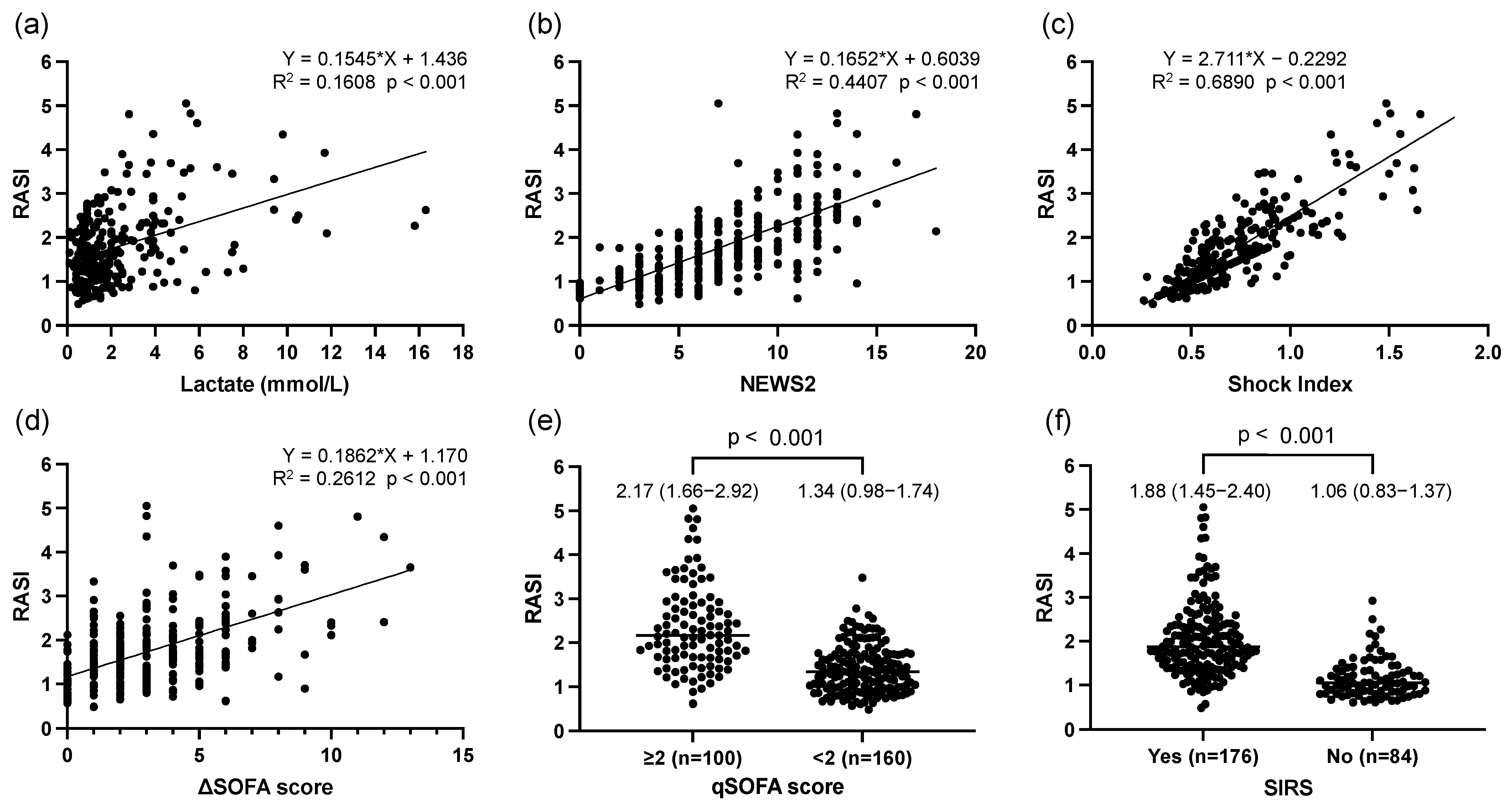
3.2. Association of RASI with Lactate, NEWS2, SI, ΔSOFA Score, qSOFA Score, and SIRS Criteria
3.3. Comparison of RASI between Individuals Who Died within 7 or 30 Days and Those Who Survived
3.4. Predictive Capacity of RASI and Other Clinical Indices for Death within 7 and 30 Days
3.5. Predictive Capacity of RASI for Death within 7 and 30 Days Compared between Patients on and off Anti-Hypertensive Drugs
3.6. Comparison of Indices Including the RASI and the Predictive Capacities of the RASI for Mortality within 7 or 30 Days with and without Prehospital Administration
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tokushima Prefecture Planning and General Affairs Department, Statistical Information and Analysis Section. Tokushima Prefecture Estimated Population by Age. 2024. Available online: https://www.pref.tokushima.lg.jp/statistics/year/nenrei/ (accessed on 25 May 2024).
- United Nations, Department of Economic and Social Affairs. Population Division (2022). World Population Prospects. 2022. Available online: https://population.un.org/wpp/ (accessed on 28 May 2024).
- Fire and Disaster Management Agency (Japan). Current Status of Emergency Rescue. 2023. Available online: https://www.fdma.go.jp/publication/rescue/items/kkkg_r05_01_kyukyu.pdf (accessed on 25 May 2024).
- Datta, D.; Walker, C.; Gray, A.J.; Graham, C. Arterial Lactate Levels in an Emergency Department are Associated with Mortality: A Prospective Observational Cohort Study. Emerg. Med. J. 2015, 32, 673–677. [Google Scholar] [CrossRef]
- Park, Y.J.; Kim, D.H.; Kim, S.C.; Kim, T.Y.; Kang, C.; Lee, S.H.; Jeong, J.H.; Lee, S.B.; Lim, D. Serum lactate upon emergency department arrival as a predictor of 30-day in-hospital mortality in an unselected population. PLoS ONE 2018, 13, e0190519. [Google Scholar] [CrossRef]
- Masson, H.; Stephenson, J. Investigation into the predictive capability for mortality and the trigger points of the National Early Warning Score 2 (NEWS2) in emergency department patients. Emerg. Med. J. 2022, 39, 685–690. [Google Scholar] [CrossRef]
- Wei, S.; Xiong, D.; Wang, J.; Liang, X.; Wang, J.; Chen, Y. The accuracy of the National Early Warning Score 2 in predicting early death in prehospital and emergency department settings: A systematic review and meta-analysis. Ann. Transl. Med. 2023, 11, 95. [Google Scholar] [CrossRef]
- Al Jalbout, N.; Balhara, K.S.; Hamade, B.; Hsieh, Y.H.; Kelen, G.D.; Bayram, J.D. Shock index as a predictor of hospital admission and inpatient mortality in a US national database of emergency departments. Updated report of a working party. Emerg. Med. J. 2019, 36, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, L.U.; Pires, E.M.C.; Vieira, J.M., Jr.; Azevedo, L.C.P. Systemic inflammatory response syndrome criteria and the prediction of hospital mortality in critically ill patients: A retrospective cohort study. Rev. Bras. Ter. Intensiv. 2017, 29, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Asayama, K.; Aikawa, N. Evaluation of systemic inflammatory response syndrome criteria as a predictor of mortality in emergency patients transported by ambulance. Keio J. Med. 1998, 47, 19–27. [Google Scholar] [CrossRef]
- Royal College of Physicians. National Early Warning Score (NEWS): Standardising the assessment of acute-illness severity in the NHS. In Report of Working Party; Royal College of Physicians: London, UK, 2012. [Google Scholar]
- RCpNational Early Warning Score (NEWS) 2: Standardising the assessment of acute-illness severity in the NHS. In Updated Report of a Working Party; Royal College of Physicians: London, UK, 2017.
- Garbero, R.F.; Simões, A.A.; Martins, G.A.; Cruz, L.V.D.; von Zuben, V.G.M. SOFA and qSOFA at admission to the emergency department: Diagnostic sensitivity and relation with prognosis in patients with suspected infection. Turk. J. Emerg. Med. 2019, 19, 106–110. [Google Scholar] [CrossRef]
- Li, Y.; Yan, C.; Gan, Z.; Xi, X.; Tan, Z.; Li, J.; Li, G. Prognostic values of SOFA score, qSOFA score, and LODS score for patients with sepsis. Ann. Palliat. Med. 2020, 9, 1037–1044. [Google Scholar] [CrossRef]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Bone, R.C.; Balk, R.A.; Cerra, F.B.; Dellinger, R.P.; Fein, A.M.; Knaus, W.A.; Schein, R.M.; Sibbald, W.J. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest 1992, 101, 1644–1655. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.; Caputo, N.D.; Chang, B.P. Respiratory adjusted shock index for identifying occult shock and level of Care in Sepsis Patients. Am. J. Emerg. Med. 2019, 37, 506–509. [Google Scholar] [CrossRef] [PubMed]
- Caputo, N.; Reilly, J.; Kanter, M.; West, J. A retrospective analysis of the respiratory adjusted shock index to determine the presence of occult shock in trauma patients. J. Trauma Acute Care Surg. 2018, 84, 674–678. [Google Scholar] [CrossRef] [PubMed]
- Hashemian, A.M.; Baghshani, Z.; Farzaneh, R.; Zamani Moghadam, H.; Maleki, F.; Bagherian, F.; Ahmadnezhad, S.; Foroughian, M. Comparison of the Relationship Between SI and RASI Scores With the Outcome of Sepsis Patients. Front. Med. 2022, 9, 872725. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR‘ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Kraut, J.A.; Madias, N.E. Lactic acidosis. N. Engl. J. Med. 2014, 371, 2309–2319. [Google Scholar] [CrossRef]
- Foucher, C.D.; Tubben, R.E. Lactic Acidosis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- del Portal, D.A.; Shofer, F.; Mikkelsen, M.E.; Dorsey, P.J., Jr.; Gaieski, D.F.; Goyal, M.; Synnestvedt, M.; Weiner, M.G.; Pines, J.M. Emergency department lactate is associated with mortality in older adults admitted with and without infections. Acad. Emerg. Med. 2010, 17, 260–268. [Google Scholar] [CrossRef]
- Cetinkaya, H.B.; Gunes, H. Use of Shock Index and Lactate to Predict Mortality in Acute Heart Failure Patients in Emergency Department. J. Coll. Physicians Surg. Pak. 2021, 31, 262–266. [Google Scholar]
- Çay, F.; Çetinkaya, H.B. The usability of shock index and lactate in predicting mortality in multitrauma patients presenting to the emergency department. Anatol. Curr. Med. J. 2022, 4, 185–189. [Google Scholar] [CrossRef]
- Kemp, K.; Alakare, J.; Harjola, V.P.; Strandberg, T.; Tolonen, J.; Lehtonen, L.; Castrén, M. National Early Warning Score 2 (NEWS2) and 3-level triage scale as risk predictors in frail older adults in the emergency department. BMC Emerg. Med. 2020, 20, 83. [Google Scholar] [CrossRef] [PubMed]
- Minne, L.; Abu-Hanna, A.; de Jonge, E. Evaluation of SOFA-based models for predicting mortality in the ICU: A systematic review. Crit. Care 2008, 12, R161. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, F.L.; Bota, D.P.; Bross, A.; Mélot, C.; Vincent, J.L. Serial evaluation of the SOFA score to predict outcome in critically ill patients. JAMA 2001, 286, 1754–1758. [Google Scholar] [CrossRef] [PubMed]
- Raith, E.P.; Udy, A.A.; Bailey, M.; McGloughlin, S.; MacIsaac, C.; Bellomo, R.; Pilcher, D.V. Prognostic Accuracy of the SOFA Score, SIRS Criteria, and qSOFA Score for In-Hospital Mortality Among Adults With Suspected Infection Admitted to the Intensive Care Unit. JAMA 2017, 317, 290–300. [Google Scholar] [CrossRef] [PubMed]
- Gupta, V.; Karnik, N.D.; Agrawal, D. SOFA Score and Critically Ill Elderly Patients. J. Assoc. Physicians India 2017, 65, 47–50. [Google Scholar] [PubMed]
- Kilinc Toker, A.; Kose, S.; Turken, M. Comparison of SOFA Score, SIRS, qSOFA, and qSOFA + L Criteria in the Diagnosis and Prognosis of Sepsis. Eurasian J. Med. 2021, 53, 40–47. [Google Scholar] [CrossRef]
- Madrazo, M.; López-Cruz, I.; Zaragoza, R.; Piles, L.; Eiros, J.M.; Alberola, J.; Artero, A. Prognostic accuracy of Quick SOFA in older adults hospitalised with community acquired urinary tract infection. Int. J. Clin. Pract. 2021, 75, e14620. [Google Scholar] [CrossRef] [PubMed]
- Chester, J.G.; Rudolph, J.L. Vital signs in older patients: Age-related changes. J. Am. Med. Dir. Assoc. 2011, 12, 337–343. [Google Scholar] [CrossRef]
- Kristensen, A.K.; Holler, J.G.; Hallas, J.; Lassen, A.; Shapiro, N.I. Is Shock Index a Valid Predictor of Mortality in Emergency Department Patients With Hypertension, Diabetes, High Age, or Receipt of β- or Calcium Channel Blockers? Ann. Emerg. Med. 2016, 67, 106–113.e6. [Google Scholar] [CrossRef]
- Koracevic, G.; Micic, S.; Stojanovic, M.; Radovanovic, R.V.; Pavlovic, M.; Kostic, T.; Djordjevic, D.; Antonijevic, N.; Koracevic, M.; Atanaskovic, V.; et al. Beta Blockers can Mask not only Hypoglycemia but also Hypotension. Curr. Pharm. Des. 2022, 28, 1660–1668. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Total Subjects (n = 260) | |
|---|---|
| Age (years) | 86 (81–92) |
| Male (n, (%)) | 126 (48.5) |
| Admission (n, (%)) | 234 (90.0) |
| Prehospital oxygen administration (n, (%)) | 160 (61.5) |
| Death within 7 days of admission (n, (%)) | 27 (10.4) |
| Death within 30 days of admission (n, (%)) | 49 (18.8) |
| Diseases that led to emergency transport (n, (%)) | |
| Diseases of the respiratory system | 98 (37.7) |
| Diseases of the circulatory system | 64 (24.6) |
| Diseases of the digestive system | 27 (10.4) |
| Endocrine, nutritional, or metabolic diseases | 20 (7.7) |
| Diseases of the genitourinary system | 19 (7.3) |
| Certain infectious or parasitic diseases | 12 (4.6) |
| Neoplasms | 9 (3.5) |
| Diseases of the skin | 4 (1.5) |
| Diseases of the musculoskeletal system or connective tissue | 4 (1.5) |
| Others | 3 (1.2) |
| Comorbidities (n, (%)) | |
| Hypertension | 179 (68.8) |
| Diabetes mellitus | 61 (23.5) |
| Dyslipidemia | 50 (19.2) |
| Medications used (n, (%)) | |
| ARB/ACEi | 90 (34.6) |
| Calcium channel blocker | 117 (45.0) |
| β-Blocker | 50 (19.2) |
| Loop diuretic | 82 (31.5) |
| Thiazide | 16 (6.2) |
| Mineralocorticoid receptor antagonist | 33 (12.7) |
| Initial evaluation of vital signs | |
| Glasgow Coma Scale (points) | 14 (13–15) |
| Systolic blood pressure (mmHg) | 132 (111–153) |
| Diastolic blood pressure (mmHg) | 77 (65–90) |
| Mean blood pressure (mmHg) | 96 (80–110) |
| Heart rate (/min) | 92 (75–108) |
| Respiratory rate (/min) | 23 (20–28) |
| Percutaneous oxygen saturation (%) | 97 (93–98) |
| Body temperature (°C) | 37.0 (36.4–37.9) |
| National Early Warning Score 2 (NEWS2) | 7 (5–10) |
| Shock Index (SI) | 0.67 (0.55–0.87) |
| Respiratory adjusted shock index (RASI) | 1.62 (1.14–2.18) |
| Quick Sequential Organ Failure Assessment (qSOFA) score ≥ 2 (n, (%)) | 100 (38.5) |
| Initial arterial blood gas tests | |
| pH | 7.44 (7.38–7.48) |
| PaCO2 (mmHg) | 33.0 (28.3–39.8) |
| PaO2 (mmHg) | 85 (67–109) |
| p/F ratio | 316 (204–435) |
| HCO3− (mmol/L) | 22.4 (19.3–26.0) |
| Base excess (mEq/L) | −0.9 (−4.3–1.8) |
| Lactate (mmol/L) | 1.5 (0.8–2.7) |
| Initial peripheral blood tests | |
| White blood cells (×103/μL) | 8.25 (5.76–11.53) |
| Hemoglobin (g/dL) | 10.9 (9.6–12.7) |
| Platelets (×103/μL) | 18.6 (14.0–23.6) |
| Total bilirubin (mg/dL) | 0.7 (0.6–1.0) |
| Creatinine (mg/dL) | 1.03 (0.76–1.47) |
| Systemic inflammatory response syndrome (SIRS) (n, (%)) | 176 (67.7) |
| ΔSequential Organ Failure Assessment (SOFA) score | 3 (1–5) |
| Death within 7 Days | ||||||
|---|---|---|---|---|---|---|
| Cutoff | AUC (95%CI) | Sensitivity (%) | Specificity (%) | Hosmer-Lemeshow Test | p Value (vs. RASI) | |
| RASI | 1.58 | 0.80 (0.73–0.87) | 96.3 | 53.6 | p = 0.10 | − |
| Lactate | 2.20 | 0.73 (0.62–0.84) | 70.4 | 72.5 | p = 0.33 | 0.230 |
| NEWS2 | 10 | 0.76 (0.67–0.84) | 55.6 | 82.8 | p = 0.08 | 0.221 |
| Shock Index | 0.75 | 0.73 (0.62–0.83) | 74.1 | 62.7 | p = 0.53 | 0.055 |
| ΔSOFA score | 4 | 0.78 (0.68–0.87) | 66.7 | 77.7 | p = 0.80 | 0.638 |
| qSOFA score | 2 | 0.75 (0.66–0.84) | 70.4 | 65.2 | p = 0.56 | 0.308 |
| SIRS score | 2 | 0.69 (0.60–0.78) | 63 | 66.1 | p = 0.86 | 0.028 |
| Death within 30 Days | ||||||
|---|---|---|---|---|---|---|
| Cutoff | AUC (95%CI) | Sensitivity (%) | Specificity (%) | Hosmer-Lemeshow Test | p Value (vs. RASI) | |
| RASI | 1.83 | 0.73 (0.66–0.81) | 69.4 | 70.6 | p = 0.68 | − |
| Lactate | 1.60 | 0.68 (0.60–0.76) | 69.4 | 62.1 | p = 0.37 | 0.231 |
| NEWS2 | 10 | 0.72 (0.65–0.80) | 49 | 85.3 | p = 0.23 | 0.698 |
| Shock Index | 0.92 | 0.65 (0.56–0.74) | 38.8 | 85.3 | p = 0.81 | 0.002 |
| ΔSOFA score | 4 | 0.74 (0.66–0.82) | 61.2 | 81 | p = 0.49 | 0.872 |
| qSOFA score | 2 | 0.73 (0.66–0.80) | 65.3 | 67.8 | p = 0.58 | 0.860 |
| SIRS score | 2 | 0.66 (0.58–0.74) | 57.1 | 67.8 | p = 0.98 | 0.081 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hori, T.; Aihara, K.-i.; Watanabe, T.; Inaba, K.; Inaba, K.; Kaneko, Y.; Kawata, S.; Kawahito, K.; Kita, H.; Shimizu, K.; et al. The Respiratory Adjusted Shock Index at Admission Is a Valuable Predictor of In-Hospital Outcomes for Elderly Emergency Patients with Medical Diseases at a Japanese Community General Hospital. J. Clin. Med. 2024, 13, 4866. https://doi.org/10.3390/jcm13164866
Hori T, Aihara K-i, Watanabe T, Inaba K, Inaba K, Kaneko Y, Kawata S, Kawahito K, Kita H, Shimizu K, et al. The Respiratory Adjusted Shock Index at Admission Is a Valuable Predictor of In-Hospital Outcomes for Elderly Emergency Patients with Medical Diseases at a Japanese Community General Hospital. Journal of Clinical Medicine. 2024; 13(16):4866. https://doi.org/10.3390/jcm13164866
Chicago/Turabian StyleHori, Taiki, Ken-ichi Aihara, Takeshi Watanabe, Kaori Inaba, Keisuke Inaba, Yousuke Kaneko, Saki Kawata, Keisuke Kawahito, Hiroki Kita, Kazuma Shimizu, and et al. 2024. "The Respiratory Adjusted Shock Index at Admission Is a Valuable Predictor of In-Hospital Outcomes for Elderly Emergency Patients with Medical Diseases at a Japanese Community General Hospital" Journal of Clinical Medicine 13, no. 16: 4866. https://doi.org/10.3390/jcm13164866
APA StyleHori, T., Aihara, K.-i., Watanabe, T., Inaba, K., Inaba, K., Kaneko, Y., Kawata, S., Kawahito, K., Kita, H., Shimizu, K., Hosoki, M., Mori, K., Kageji, T., Uraoka, H., & Nakamura, S. (2024). The Respiratory Adjusted Shock Index at Admission Is a Valuable Predictor of In-Hospital Outcomes for Elderly Emergency Patients with Medical Diseases at a Japanese Community General Hospital. Journal of Clinical Medicine, 13(16), 4866. https://doi.org/10.3390/jcm13164866