
The Indirect Effect of Future Anxiety on the Relationship between Self-Efficacy and Depression in a Convenience Sample of Adults: Revisiting Social Cognitive Theory

 , and
, and
Abstract
:1. Introduction
1.1. Depression in Emerging Adults
1.2. Association between Future Anxiety and Depression
1.3. The Relationship between Depression, Future Anxiety, and Self-Efficacy
1.4. The Current Study
- There are age (emerging and middle adulthood) and gender (women, men) differences in symptoms of depression, future anxiety, and self-efficacy (H1).
- Self-efficacy is related negatively to symptoms of depression and future anxiety (H2).
- The higher the level of future anxiety, the higher the level of depression symptoms (H3).
- Low self-efficacy contributes to higher depression directly and indirectly through increased levels of future anxiety (H4).
2. Materials and Methods
2.1. Study Design and Procedure
2.2. Participant Characteristics
2.3. Measures
2.3.1. Depression
2.3.2. Future Anxiety
2.3.3. Self-Efficacy
2.3.4. Demographic Survey
2.4. Statistical Analysis
3. Results
3.1. A Preliminary Statistical Analysis
3.2. Gender and Age Differences in Depression Symptoms, Future Anxiety, and Self-Efficacy
3.3. Associations between Depression, Future Anxiety, and Self-Efficacy
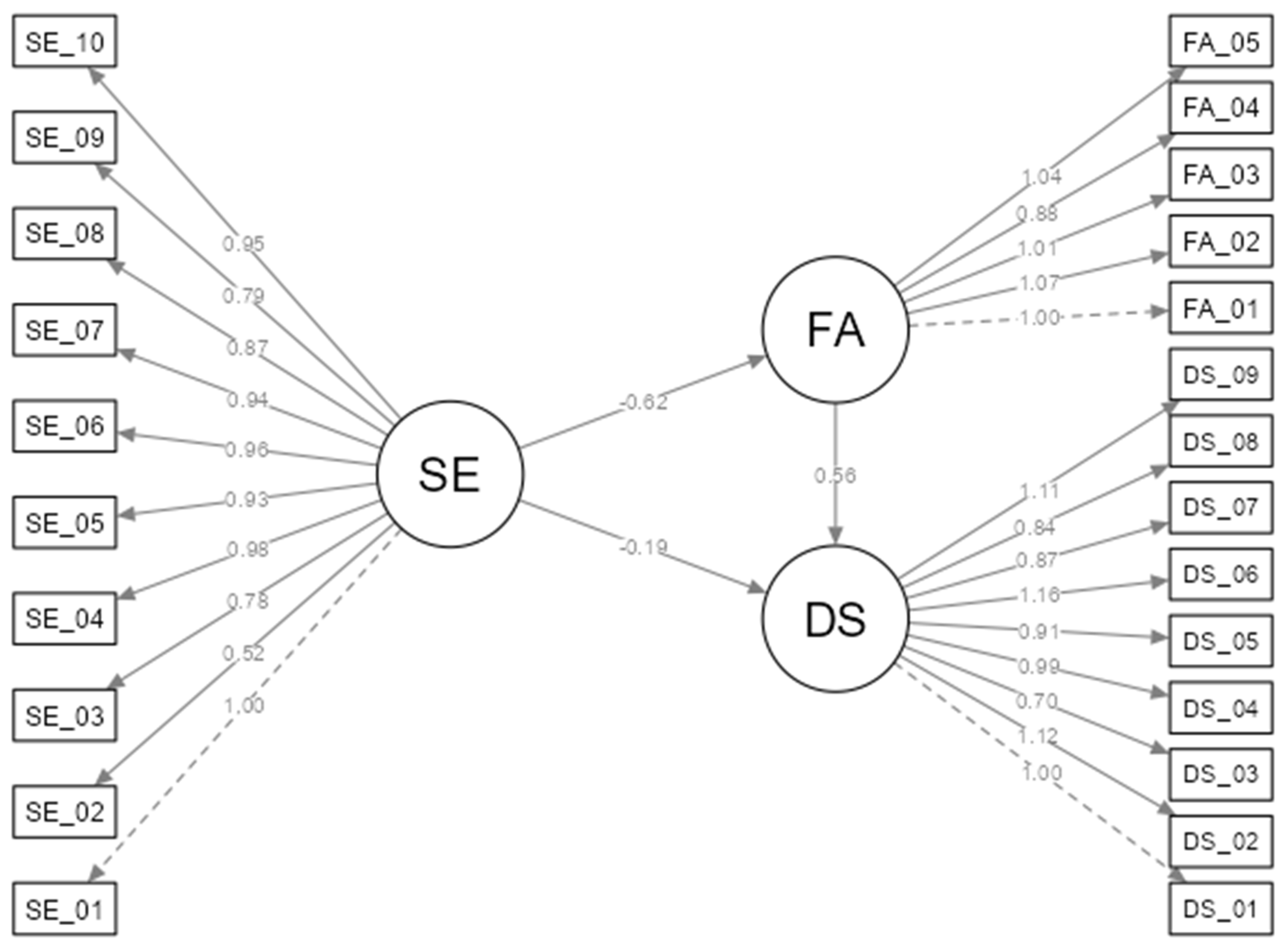
3.4. Analysis of Mediation
4. Discussion
4.1. Age and Gender Differences in Depression, Future Anxiety, and Self-Efficacy
4.2. The Relationships between Depression, Future Anxiety, and Self-Efficacy
4.3. Mediating Effect of Future Anxiety on the Relationships between Self-Efficacy and Depression
4.4. Limitation of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO Depressive Disorder (Depression). Available online: https://www.who.int/news-room/fact-sheets/detail/depression (accessed on 23 July 2024).
- Cohen, J.R.; Thomsen, K.N.; Racioppi, A.; Ballespi, S.; Sheinbaum, T.; Kwapil, T.R.; Barrantes-Vidal, N. Emerging Adulthood and Prospective Depression: A Simultaneous Test of Cumulative Risk Theories. J. Youth Adolesc. 2019, 48, 1353–1364. [Google Scholar] [CrossRef]
- Soysa, C.K.; Wilcomb, C.J. Mindfulness, Self-Compassion, Self-Efficacy, and Gender as Predictors of Depression, Anxiety, Stress, and Well-Being. Mindfulness 2015, 6, 217–226. [Google Scholar] [CrossRef]
- Rohde, P.; Lewinsohn, P.M.; Klein, D.N.; Seeley, J.R.; Gau, J.M. Key Characteristics of Major Depressive Disorder Occurring in Childhood, Adolescence, Emerging Adulthood, and Adulthood. Clin. Psychol. Sci. 2013, 1, 41–53. [Google Scholar] [CrossRef] [PubMed]
- Costello, D.M.; Swendsen, J.; Rose, J.S.; Dierker, L.C. Risk and Protective Factors Associated With Trajectories of Depressed Mood From Adolescence to Early Adulthood. J. Consult. Clin. Psychol. 2008, 76, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Albert, P.R. Why Is Depression More Prevalent in Women? J. Psychiatry Neurosci. 2015, 40, 219. [Google Scholar] [CrossRef]
- Arnett, J.J.; Žukauskienė, R.; Sugimura, K. Adolescent Mental Health 3 The New Life Stage of Emerging Adulthood at Ages 18-29 Years: Implications for Mental Health. Lancet Psychiatry 2014, 1, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Berry, D. The Relationship between Depression and Emerging Adulthood: Theory Generation. ANS Adv. Nurs. Sci. 2004, 27, 53–69. [Google Scholar] [CrossRef] [PubMed]
- Frye, A.A.; Liem, J.H. Diverse Patterns in the Development of Depressive Symptoms among Emerging Adults. J. Adolesc. Res. 2011, 26, 570–590. [Google Scholar] [CrossRef]
- Brito, A.D.; Soares, A.B. Well-Being, Character Strengths, and Depression in Emerging Adults. Front. Psychol. 2023, 14, 1238105. [Google Scholar] [CrossRef] [PubMed]
- Walensky, R.P.; Bunnell, R.; Kent, C.K.; Damon, G.; Farley, J.; Garrett-Cherry, T.; Morici, A.; Simon, S.; Thompson, M.; Webb, S.; et al. National, State-Level, and County-Level Prevalence Estimates of Adults Aged ≥18 Years Self-Reporting a Lifetime Diagnosis of Depression—United States. Morb. Mortal. Wkly. Rep. 2023, 72, 644–650. [Google Scholar]
- Collins, S.; Lotfalian, M.; Marx, W.; Lane, M.; Allender, S.; Jacka, F.; Hoare, E. Associations between Indicators of Diet Quality and Psychological Distress, Depression and Anxiety in Emerging Adults: Results from a Nationally Representative Observational Sample. Ment. Health Prev. 2021, 24, 200220. [Google Scholar] [CrossRef]
- Collins, S.; Hoare, E.; Allender, S.; Olive, L.; Leech, R.M.; Winpenny, E.M.; Jacka, F.; Lotfalian, M. A Longitudinal Study of Lifestyle Behaviours in Emerging Adulthood and Risk for Symptoms of Depression, Anxiety, and Stress. J. Affect. Disord. 2023, 327, 244–253. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Shi, L.; Xia, Y.; Shi, Z.; Wang, D. Recent Trend in the Prevalence and Correlates of Depression Among Chinese Young Adults from 2010 to 2018. Youth Soc. 2024, 56, 946–966. [Google Scholar] [CrossRef]
- Galambos, N.L.; Barker, E.T.; Krahn, H.J. Depression, Self-Esteem, and Anger in Emerging Adulthood: Seven-Year Trajectories. Dev. Psychol. 2006, 42, 350–365. [Google Scholar] [CrossRef]
- Regli, J.; Sadeghi-Bahmani, D.; Rigotti, V.; Stanga, Z.; Ülgür, I.I.; Fichter, C.; Lang, U.E.; Brühl, A.B.; Brand, S. Psychiatric Characteristics, Symptoms of Insomnia and Depression, Emotion Regulation, and Social Activity among Swiss Medical Students. J. Clin. Med. 2024, 13, 4372. [Google Scholar] [CrossRef]
- Arnett, J.J. Emerging Adulthood A Theory of Development from the Late Teens Through the Twenties. Am. Psychol. 2000, 55, 469. [Google Scholar] [CrossRef] [PubMed]
- Arnett, J.J. Emerging Adulthood: What Is It, and What Is It Good For? Child Dev. Perspect. 2007, 1, 68–73. [Google Scholar] [CrossRef]
- Arnett, J.J. Emerging Adulthood: The Winding Road from the Late Teens Through the Twenties; Oxford University Press: New York, NY, USA, 2023. [Google Scholar]
- Salmela-Aro, K.; Aunola, K.; Nurmi, J.-E. Trajectories of Depressive Symptoms during Emerging Adulthood: Antecedents and Consequences. Eur. J. Dev. Psychol. 2008, 5, 439–465. [Google Scholar] [CrossRef]
- Halliburton, A.E.; Hill, M.B.; Dawson, B.L.; Hightower, J.M.; Rueden, H. Increased Stress, Declining Mental Health: Emerging Adults’ Experiences in College During COVID-19. Emerg. Adulthood 2021, 9, 433–448. [Google Scholar] [CrossRef]
- Alzueta, E.; Podhajsky, S.; Zhao, Q.; Tapert, S.F.; Thompson, W.K.; De Zambotti, M.; Yuksel, D.; Kiss, O.; Wang, R.; Volpe, L.; et al. Risk for Depression Tripled during the COVID-19 Pandemic in Emerging Adults Followed for the Last 8 Years. Psychol. Med. 2023, 53, 2156–2163. [Google Scholar] [CrossRef]
- Maia, B.R.; Dias, P.C. Anxiety, Depression and Stress in University Students: The Impact of COVID-19. Estud. Psicol. (Camp.) 2020, 37, e200067. [Google Scholar] [CrossRef]
- Vujčić, I.; Safiye, T.; Milikić, B.; Popović, E.; Dubljanin, D.; Dubljanin, E.; Dubljanin, J.; Čabarkapa, M. Coronavirus Disease 2019 (COVID-19) Epidemic and Mental Health Status in the General Adult Population of Serbia: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 1957. [Google Scholar] [CrossRef] [PubMed]
- Braet, C.; Van Vlierberghe, L.; Vandevivere, E.; Theuwis, L.; Bosmans, G. Depression in Early, Middle and Late Adolescence: Differential Evidence for the Cognitive Diathesis-Stress Model. Clin. Psychol. Psychother. 2013, 20, 369–383. [Google Scholar] [CrossRef] [PubMed]
- Othman, A.A.; Jaafar, W.M.W. Features of Emerging Adulthood: What Are Their Relationship with Depression Symptoms? Open Psychol. J. 2022, 15, e187435012208010. [Google Scholar] [CrossRef]
- Kuwabara, S.A.; Van Voorhees, B.W.; Gollan, J.K.; Alexander, G.C. A Qualitative Exploration of Depression in Emerging Adulthood: Disorder, Development, and Social Context. Gen. Hosp. Psychiatry 2007, 29, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W.; Löwe, B. The Patient Health Questionnaire Somatic, Anxiety, and Depressive Symptom Scales: A Systematic Review. Gen. Hosp. Psychiatry 2010, 32, 345–359. [Google Scholar] [CrossRef] [PubMed]
- Knowles, K.A.; Olatunji, B.O. Specificity of Trait Anxiety in Anxiety and Depression: Meta-Analysis of the State-Trait Anxiety Inventory. Clin. Psychol. Rev. 2020, 82, 101928. [Google Scholar] [CrossRef] [PubMed]
- Radulovic, D.; Masic, S.; Stanisavljevic, D.; Bokonjic, D.; Radevic, S.; Rajovic, N.; Mili’, N.V.; Simic Vukomanovic, I.; Mijovic, B.; Vukovic, M.; et al. A Complex Relationship between Quality of Life, Anxiety, and Depression among General Population during Second Year of COVID-19 Pandemic: A Population-Based Study. J. Clin. Med. 2024, 13, 3874. [Google Scholar] [CrossRef]
- Jacobson, N.C.; Newman, M.G. Anxiety and Depression as Bidirectional Risk Factors for One Another: A Meta-Analysis of Longitudinal Studies. Psychol. Bull. 2017, 143, 1155–1200. [Google Scholar] [CrossRef] [PubMed]
- MacLeod, A.K.; Tata, P.; Kentish, J.; Jacobsen, H. Retrospective and Prospective Cognitions in Anxiety and Depression. Cogn. Emot. 1997, 11, 467–479. [Google Scholar] [CrossRef]
- Austin, M.P.; Tully, L.; Parker, G. Examining the Relationship between Antenatal Anxiety and Postnatal Depression. J. Affect. Disord. 2007, 101, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Borkovec, T.D.; Ray, W.J.; Stöber, J. Worry: A Cognitive Phenomenon Intimately Linked to Affective, Physiological, and Interpersonal Behavioral Processes. Cogn. Ther. Res. 1998, 22, 561–576. [Google Scholar] [CrossRef]
- Borkovec, T.D.; Robinson, E.; Pruzinsky, T.; DePree, J.A. Preliminary Exploration of Worry: Some Characteristics and Processes. Behav. Res. Ther. 1983, 21, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Roepke, A.M.; Seligman, M.E.P. Depression and Prospection. Br. J. Clin. Psychol. 2016, 55, 23–48. [Google Scholar] [CrossRef] [PubMed]
- Dar, K.A.; Iqbal, N.; Mushtaq, A. Intolerance of Uncertainty, Depression, and Anxiety: Examining the Indirect and Moderating Effects of Worry. Asian J. Psychiatr. 2017, 29, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Zaleski, Z. Future Anxiety: Concept, Measurement, and Preliminary Research. Pers. Individ. Differ. 1996, 21, 165–174. [Google Scholar] [CrossRef]
- Strathman, A.; Joireman, J. Understanding Behavior in the Context of Time: Theory, Research, and Application, 1st ed.; Strathman, A., Joireman, J., Eds.; Psychology Press: London, England, UK, 2005. [Google Scholar]
- Duplaga, M.; Grysztar, M. The Association between Future Anxiety, Health Literacy and the Perception of the COVID-19 Pandemic: A Cross-Sectional Study. Healthcare 2021, 9, 43. [Google Scholar] [CrossRef] [PubMed]
- Zaleski, Z.; Sobol-Kwapinska, M.; Przepiorka, A.; Meisner, M. Development and Validation of the Dark Future Scale. Time Soc. 2019, 28, 107–123. [Google Scholar] [CrossRef]
- Jannini, T.B.; Rossi, R.; Socci, V.; Di Lorenzo, G. Validation of the Dark Future Scale (DFS) for Future Anxiety on an Italian Sample. J. Psychopathol. 2022, 28, 86–93. [Google Scholar] [CrossRef]
- Bandura, A. On the Functional Properties of Perceived Self-Efficacy Revisited. J. Manag. 2012, 38, 9–44. [Google Scholar] [CrossRef]
- Bandura, A. Social Cognitive Theory of Self-Regulation. Organ. Behav. Hum. Decis. Process. 1991, 50, 248–287. [Google Scholar] [CrossRef]
- Bandura, A. Social Learning Theory; Prentice Hall: Englewood Cliffs, NJ, USA, 1977. [Google Scholar]
- Bandura, A. Self-Efficacy: Toward a Unifying Theory of Behavioral Change. Adv. Behav. Res. Ther. 1978, 1, 139–161. [Google Scholar] [CrossRef]
- Shulman, S.; Kalnitzki, E.; Shahar, G. Meeting Developmental Challenges During Emerging Adulthood: The Role of Personality and Social Resources. J. Adolesc. Res. 2009, 24, 242–267. [Google Scholar] [CrossRef]
- Robinson, K.A.; Perez, T.; White-Levatich, A.; Linnenbrink-Garcia, L. Gender Differences and Roles of Two Science Self-Efficacy Beliefs in Predicting Post-College Outcomes. J. Exp. Educ. 2022, 90, 344. [Google Scholar] [CrossRef] [PubMed]
- Bausch, S.; Michel, A.; Sonntag, K. How Gender Influences the Effect of Age on Self-Efficacy and Training Success. Int. J. Train. Dev. 2014, 18, 171–187. [Google Scholar] [CrossRef]
- Priyadharsan, S.; Saravanabawan, A. Does age Matter to influence self-efficacy: Review of related literature. J. Manag. 2021, 16, 1391–8230. [Google Scholar]
- Rabei, S.; Ramadan, S.; Abdallah, N. Self-Efficacy and Future Anxiety among Students of Nursing and Education Colleges of Helwan University. Middle East Curr. Psychiatry 2020, 27, 39. [Google Scholar] [CrossRef]
- Madson, R.C.; Perrone, P.B.; Goldstein, S.E.; Lee, C.-Y.S. Self-Efficacy, Perceived Stress, and Individual Adjustment among College-Attending Emerging Adults. Youth 2022, 2, 668–680. [Google Scholar] [CrossRef]
- Yang, Z.-Y.; Wang, Y.-T.; Xia, L.; Zheng, Y.-C.; Feng, Z.-Z. The Relationships between Prospection, Self-Efficacy, and Depression in College Students with Cross-Lagged Analysis. Int. J. Environ. Res. Public Health 2022, 19, 14685. [Google Scholar] [CrossRef]
- Blackburn, L.; Owens, G.P. The Effect of Self Efficacy and Meaning in Life on Posttraumatic Stress Disorder and Depression Severity among Veterans. J. Clin. Psychol. 2015, 71, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Pu, J.; Hou, H.; Ma, R. Direct and Indirect Effects of Self-Efficacy on Depression: The Mediating Role of Dispositional Optimism. Curr. Psychol. 2017, 36, 410–416. [Google Scholar] [CrossRef]
- Tahmassian, K.; Moghadam, N.J. Relationship Between Self-Efficacy and Symptoms of Anxiety, Depression, Worry and Social Avoidance in a Normal Sample of Students. Iran. J. Psychiatry Behav. Sci. 2011, 5, 91. [Google Scholar]
- Starr, L.R.; Davila, J. Temporal Patterns of Anxious and Depressed Mood in Generalized Anxiety Disorder: A Daily Diary Study. Behav. Res. Ther. 2012, 50, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Tak, Y.R.; Brunwasser, S.M.; Lichtwarck-Aschoff, A.; Engels, R.C. The Prospective Associations between Self-Efficacy and Depressive Symptoms from Early to Middle Adolescence: A Cross-Lagged Model. J. Youth Adolesc. 2017, 46, 744–756. [Google Scholar] [CrossRef] [PubMed]
- Reed-Fitzke, K. The Role of Self-Concepts in Emerging Adult Depression: A Systematic Research Synthesis. J. Adult Dev. 2020, 27, 36–48. [Google Scholar] [CrossRef]
- Seligman, M.E. Learned Helplessness. Annu. Rev. Med. 1972, 23, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Maier, S.F.; Seligman, M.E.P. Learned Helplessness at Fifty: Insights from Neuroscience. Psychol. Rev. 2016, 123, 349. [Google Scholar] [CrossRef] [PubMed]
- Rippere, V. Comments on Seligman’s Theory of Helplessness. Behav. Res. Ther. 1977, 15, 207–209. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T. The Development of Depression: A Cognitive Model; John Wiley & Sons: New York, NY, USA, 1974. [Google Scholar]
- Beck, A.T.; Bredemeier, K. A Unified Model of Depression: Integrating Clinical, Cognitive, Biological, and Evolutionary Perspectives. Clin. Psychol. Sci. 2016, 4, 596–619. [Google Scholar] [CrossRef]
- Miloyan, B.; Pachana, N.A.; Suddendorf, T. The Future Is Here: A Review of Foresight Systems in Anxiety and Depression. Cogn. Emot. 2014, 28, 795–810. [Google Scholar] [CrossRef] [PubMed]
- Miranda, R.; Mennin, D.S. Depression, Generalized Anxiety Disorder, and Certainty in Pessimistic Predictions about the Future. Cogn. Ther. Res. 2007, 31, 71–82. [Google Scholar] [CrossRef]
- Hoerger, M.; Quirk, S.W.; Chapman, B.P.; Duberstein, P.R. Affective Forecasting and Self-Rated Symptoms of Depression, Anxiety, and Hypomania: Evidence for a Dysphoric Forecasting Bias. Cogn. Emot. 2012, 26, 1098–1106. [Google Scholar] [CrossRef]
- Hallford, D.J. The Phenomenological Characteristics of Autobiographical Future Thinking in Dysphoric and Non-Dysphoric Individuals. Psychiatry Res. 2019, 273, 481–486. [Google Scholar] [CrossRef]
- Anderson, C.A.; Deuser, W.E. Science and the Reformulated Learned-Helplessness Model of Depression. Psychol. Inq. 1991, 2, 14–19. [Google Scholar] [CrossRef]
- Miloyan, B.; Bulley, A.; Suddendorf, T. Episodic Foresight and Anxiety: Proximate and Ultimate Perspectives. Br. J. Clin. Psychol. 2016, 55, 4–22. [Google Scholar] [CrossRef] [PubMed]
- MacLeod, A.K.; Byrne, A. Anxiety, Depression, and the Anticipation of Future Positive and Negative Experiences. J. Abnorm. Psychol. 1996, 105, 286–289. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.D.; Root, J.C.; Romano, T.A.; Chang, L.J.; Bryant, R.A.; Hirst, W. Overgeneralized Autobiographical Memory and Future Thinking in Combat Veterans with Posttraumatic Stress Disorder. J. Behav. Ther. Exp. Psychiatry 2013, 44, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.D.; Addis, D.R.; Romano, T.A.; Marmar, C.R.; Bryant, R.A.; Hirst, W.; Schacter, D.L. Episodic and Semantic Components of Autobiographical Memories and Imagined Future Events in Post-Traumatic Stress Disorder. Memory 2014, 22, 595–604. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.D.; Kouri, N.A.; Rahman, N.; Joscelyne, A.; Bryant, R.A.; Marmar, C.R. Enhancing Self-Efficacy Improves Episodic Future Thinking and Social-Decision Making in Combat Veterans with Posttraumatic Stress Disorder. Psychiatry Res. 2016, 242, 19–25. [Google Scholar] [CrossRef]
- Beck, A.T.; Weissman, A.; Lester, D.; Trexler, L. The Measurement of Pessimism: The Hopelessness Scale. J. Consult. Clin. Psychol. 1974, 42, 861–865. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Toward a Psychology of Human Agency. Perspect. Psychol. Sci. 2006, 1, 164–180. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9: Validity of a Brief Depression Severity Measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Tomaszewski, K.; Zarychta, M.; Bienkowska, A.; Chmurowicz, E.; Nowak, W.; Skalska, A. Walidacja Polskiej Wersji Językowej Patient Health Questionnaire-9 w Populacji Hospitalizowanych Osób Starszych. Psychiatr. Pol. 2011, 45, 223–233. [Google Scholar] [PubMed]
- Zaleski, Z.; Paul, J. Niepokój Przyszłościowy: Pojęcie i Narzędzie Pomiaru. Ann. Philos. 1997, 45, 191–197. [Google Scholar]
- Schwarzer, R.; Jerusalem, M. Generalized Self-Efficacy Scale. In Measures in Health Psychology A User’s Portfolio. Causal and Control Beliefs; Weinman, J., Wright, S., Johnston, M., Eds.; NFER-NELSON: Windsor, UK, 1995; pp. 35–37. [Google Scholar]
- Juczyński, Z. Poczucie Własnej Skuteczności-Teoria i Pomiar. Acta Univ. Lodz. 2000, 4, 11–24. [Google Scholar]
- Hair, J.; Alamer, A. Partial Least Squares Structural Equation Modeling (PLS-SEM) in Second Language and Education Research: Guidelines Using an Applied Example. Res. Methods Appl. Linguist. 2022, 1, 100027. [Google Scholar] [CrossRef]
- Hair, J.F.; Hult, G.T.M.; Ringle, C.M.; Sarstedt, M.; Thiele, K.O. Mirror, Mirror on the Wall: A Comparative Evaluation of Composite-Based Structural Equation Modeling Methods. J. Acad. Mark. Sci. 2017, 45, 616–632. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Chen, F.F. Sensitivity of Goodness of Fit Indexes to Lack of Measurement Invariance. Struct. Equ. Model. 2007, 14, 464–504. [Google Scholar] [CrossRef]
- Kim, H.-Y. Statistical Notes for Clinical Researchers: Assessing Normal Distribution (2) Using Skewness and Kurtosis. Restor. Dent. Endod. 2013, 38, 52. [Google Scholar] [CrossRef]
- Gambin, M.; Sękowski, M.; Woźniak-Prus, M.; Cudo, A.; Hansen, K.; Gorgol, J.; Huflejt-Łukasik, M.; Kmita, G.; Kubicka, K.; Łyś, A.E.; et al. Uwarunkowania Objawów Depresji i Lęku Uogólnionego u Dorosłych Polaków w Trakcie Epidemii COVID-19. Raport z Pierwszej Fali Badania Podłużnego. Uniwersytet Warszawski. 2021. Available online: https://psych.strony.uw.edu.pl/wp-content/uploads/sites/98/2021/01/Raport_objawy_depresji_leku_IV_fale.pdf (accessed on 17 August 2024).
- Sussman, S.; Arnett, J.J. Emerging Adulthood: Developmental Period Facilitative of the Addictions. Eval. Health Prof. 2014, 37, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Muris, P. Relationships between Self-Efficacy and Symptoms of Anxiety Disorders and Depression in a Normal Adolescent Sample. Pers. Individ. Differ. 2002, 32, 337–348. [Google Scholar] [CrossRef]
- Hallford, D.J.; Carmichael, A.M.; Austin, D.W.; Dax, S.; Coulston, M.I.; Wong, A. Brief Inductions in Episodic Past or Future Thinking: Effects on Episodic Detail and Problem-Solving. Cogn. Process. 2022, 23, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Zaleski, Z. Psychologia Lęku Przed Przyszłością; Difin: Warszawa, Poland, 2018. [Google Scholar]
- Zaleski, Z. Future Orientationand Anxiety. In Understanding Behavior in the Context of Time: Theory, Research, and Application; Strathman, A., Joireman, J.A., Eds.; Psychology Press: London, England, UK, 2005; pp. 125–142. ISBN 9781410613516. [Google Scholar]
- Beck, R.; Perkins, T.S. Cognitive Content-Specificity for Anxiety and Depression: A Meta-Analysis. Cogn. Ther. Res. 2001, 25, 651–663. [Google Scholar] [CrossRef]

{kind=link}
| Variable | Categories | Emerging (n = 157) | Middle-Aged (n = 126) | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Age | M/SD | 23.15 | 2.25 | 43.52 | 8.95 |
| Women | 115 | 40.5 | 73 | 25.7 | |
| Gender | Men | 42 | 14.8 | 53 | 18.7 |
| Other | 1 | 0.4 | 0 | 0.0 | |
| Village | 23 | 8.1 | 21 | 7.4 | |
| City up to 50,000 inhabitants | 16 | 5.6 | 27 | 9.5 | |
| Place of residence | A city 50,000–250,000 inhabitants | 42 | 14.8 | 38 | 13.4 |
| A city 250,000–500,000 inhabitants | 33 | 11.6 | 30 | 10.6 | |
| City above 500,000 inhabitants | 44 | 15.5 | 10 | 3.5 | |
| Primary | 3 | 1.1 | 0 | 0.0 | |
| Vocational | 2 | 0.7 | 4 | 1.4 | |
| Secondary | 71 | 25.0 | 48 | 16.9 | |
| Education | Bachelor degree | 56 | 19.7 | 20 | 7.0 |
| Master degree | 26 | 9.2 | 54 | 19.0 | |
| Single | 63 | 22.2 | 25 | 8.8 | |
| Relationship status | In a relationship | 95 | 33.5 | 101 | 35.6 |
| Student | 40 | 14.1 | 1 | 0.4 | |
| Professional status | Student employed | 78 | 27.5 | 7 | 2.5 |
| Employed | 37 | 13.0 | 112 | 39.4 | |
| Unemployed | 3 | 1.1 | 6 | 2.1 | |
| Socioeconomic status | Insufficient | 21 | 7.4 | 12 | 4.2 |
| Enough for basic needs | 75 | 26.4 | 48 | 16.9 | |
| Meets more than basic needs | 62 | 21.8 | 66 | 23.2 | |
| Depression (PHQ-9) | Women (M/SD) | 10.40 | 6.28 | 8.12 | 6.50 |
| Men (M/SD) | 7.31 | 4.76 | 4.53 | 4.08 | |
| Future anxiety (DFS) | Women (M/SD) | 19.40 | 7.77 | 16.22 | 8.56 |
| Men (M/SD) | 14.64 | 7.60 | 12.34 | 8.85 | |
| Self-efficacy (GSES) | Women (M/SD) | 27.16 | 6.13 | 28.86 | 5.50 |
| Men (M/SD) | 32.50 | 4.84 | 33.00 | 4.63 | |
| Variable | Items | Range | M | SD | Skew. | Kurt. | ω | AVE | Pearson’s r Correlations | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| SE | FA | DS | |||||||||
| Self-efficacy (SE) | 10 | 11–40 | 29.48 | 6.02 | –0.46 | –0.20 | 0.92 | 0.64 | 0.73 | ||
| Future anxiety (FA) | 5 | 0–30 | 16.56 | 8.55 | –0.25 | –1.00 | 0.91 | 0.71 | –0.58 *** | 0.82 | |
| Depression symptoms (DS) | 9 | 0–27 | 8.26 | 6.14 | 0.83 | 0.01 | 0.88 | 0.55 | –0.55 *** | 0.65 *** | 0.68 |
| Step | Predictor | b | SE | 95% CI | t | R | R ² | F | df 1 | df 2 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| LL | UL | ||||||||||
| 1 | Intercept | 4.71 | 0.67 | 3.40 | 6.03 | 7.06 *** | 0.35 | 0.12 | 19.18 *** | 2 | 281 |
| Age (Emerging) | 2.48 | 0.70 | 1.10 | 3.85 | 3.55 *** | ||||||
| Gender (Women) | 3.28 | 0.73 | 1.83 | 4.72 | 4.46 *** | ||||||
| 2 | Intercept | 21.67 | 1.89 | 17.94 | 25.40 | 11.44 *** | 0.58 | 0.33 | 46.30 *** | 3 | 280 |
| Age (Emerging) | 1.79 | 0.62 | 0.58 | 3.00 | 2.92 ** | ||||||
| Gender (Women) | 0.94 | 0.69 | –0.41 | 2.29 | 1.37 | ||||||
| Self-efficacy | –0.51 | 0.05 | –0.62 | –0.40 | –9.41 *** | ||||||
| 3 | Intercept | 8.81 | 2.22 | 4.44 | 13.18 | 3.96 *** | 0.69 | 0.48 | 63.75 *** | 4 | 279 |
| Age (Emerging) | 1.15 | 0.55 | 0.07 | 2.23 | 2.10 * | ||||||
| Gender (Women) | 0.74 | 0.61 | –0.46 | 1.94 | 1.21 | ||||||
| Self-efficacy | –0.25 | 0.06 | –0.36 | –0.14 | –4.38 *** | ||||||
| Future anxiety | 0.34 | 0.04 | 0.26 | 0.42 | 8.83 *** | ||||||
| 95% CI | ||||||||
|---|---|---|---|---|---|---|---|---|
| Predictor | Dependent | b | SE | LL | UL | β | z | p |
| SE | FA | –0.62 | 0.04 | –0.70 | –0.53 | –0.67 | –14.60 | <0.001 |
| FA | DS | 0.56 | 0.06 | 0.45 | 0.68 | 0.62 | 9.50 | <0.001 |
| SE ⇒ FA ⇒ DS | –0.19 | 0.05 | –0.29 | –0.09 | –0.23 | –3.77 | <0.001 | |
| Indirect effect | –0.35 | 0.04 | –0.43 | –0.26 | –0.41 | –8.05 | <0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szota, M.; Rogowska, A.M.; Kwaśnicka, A.; Chilicka-Hebel, K. The Indirect Effect of Future Anxiety on the Relationship between Self-Efficacy and Depression in a Convenience Sample of Adults: Revisiting Social Cognitive Theory. J. Clin. Med. 2024, 13, 4897. https://doi.org/10.3390/jcm13164897
Szota M, Rogowska AM, Kwaśnicka A, Chilicka-Hebel K. The Indirect Effect of Future Anxiety on the Relationship between Self-Efficacy and Depression in a Convenience Sample of Adults: Revisiting Social Cognitive Theory. Journal of Clinical Medicine. 2024; 13(16):4897. https://doi.org/10.3390/jcm13164897
Chicago/Turabian StyleSzota, Marta, Aleksandra M. Rogowska, Aleksandra Kwaśnicka, and Karolina Chilicka-Hebel. 2024. "The Indirect Effect of Future Anxiety on the Relationship between Self-Efficacy and Depression in a Convenience Sample of Adults: Revisiting Social Cognitive Theory" Journal of Clinical Medicine 13, no. 16: 4897. https://doi.org/10.3390/jcm13164897