

Does Indocyanine Green Utilization during Esophagectomy Prevent Anastomotic Leaks? Systematic Review and Meta-Analysis
 , , , ,
, , , ,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Data Extraction
2.3. Outcomes
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Systematic Review
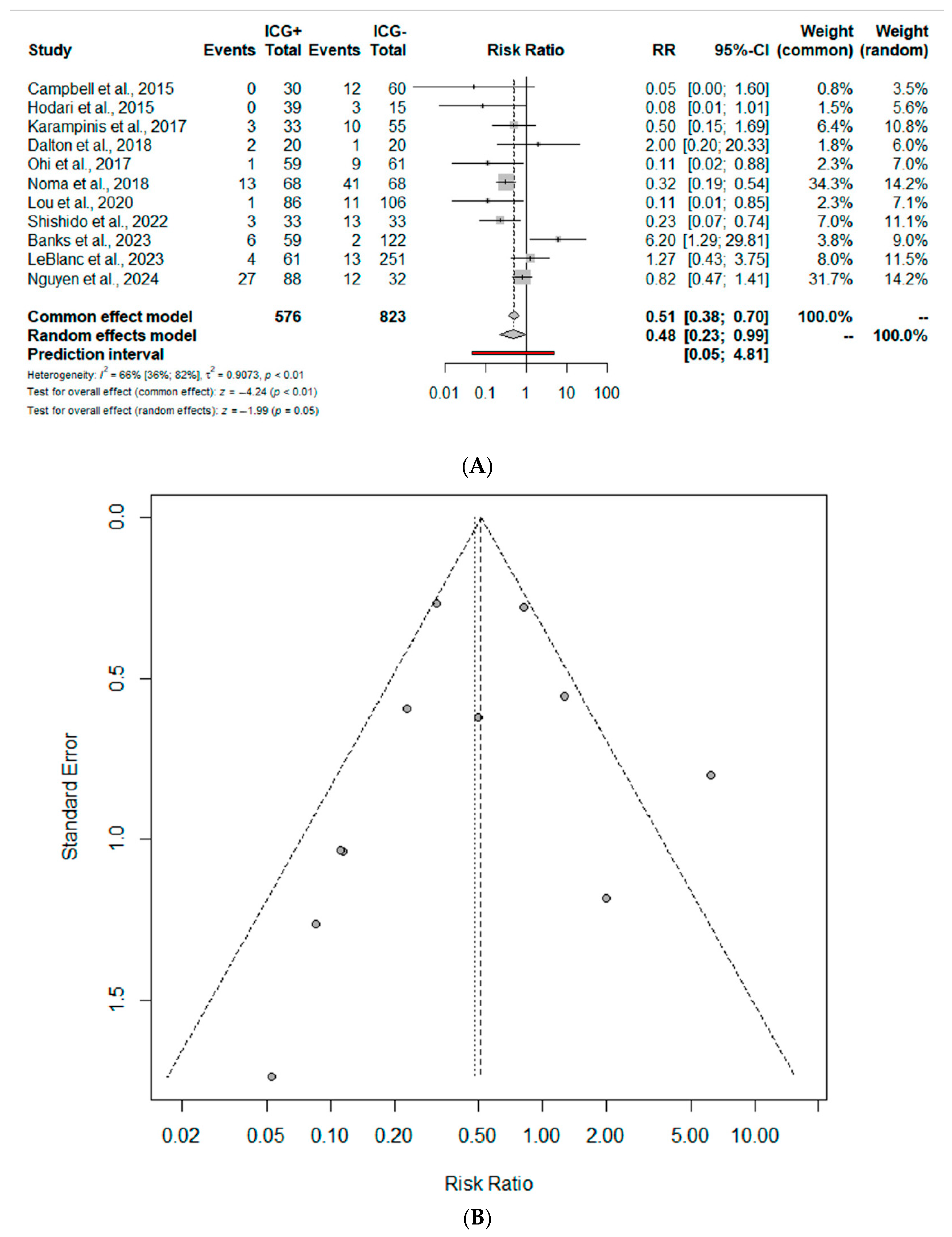
3.2. Meta-Analysis: Primary Outcome
3.3. Meta-Analysis: Secondary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Search Strategy
References
- Morgan, E.; Soerjomataram, I.; Rumgay, H.; Coleman, H.G.; Thrift, A.P.; Vignat, J.; Laversanne, M.; Ferlay, J.; Arnold, M. The Global Landscape of Esophageal Squamous Cell Carcinoma and Esophageal Adenocarcinoma Incidence and Mortality in 2020 and Projections to 2040: New Estimates From GLOBOCAN 2020. Gastroenterology 2022, 163, 649–658.e2. [Google Scholar] [CrossRef]
- Hirst, J.; Smithers, B.M.; Gotley, D.C.; Thomas, J.; Barbour, A. Defining Cure for Esophageal Cancer: Analysis of Actual 5-Year Survivors Following Esophagectomy. Ann. Surg. Oncol. 2011, 18, 1766–1774. [Google Scholar] [CrossRef]
- Miyata, H.; Yamasaki, M.; Kurokawa, Y.; Takiguchi, S.; Nakajima, K.; Fujiwara, Y.; Mori, M.; Doki, Y. Multimodal treatment for resectable esophageal cancer. Gen. Thorac. Cardiovasc. Surg. 2011, 59, 461–466. [Google Scholar] [CrossRef]
- Aiolfi, A.; Sozzi, A.; Bonitta, G.; Lombardo, F.; Cavalli, M.; Cirri, S.; Campanelli, G.; Danelli, P.; Bona, D. Linear- versus circular-stapled esophagogastric anastomosis during esophagectomy: Systematic review and meta-analysis. Langenbeck’s Arch. Surg. 2022, 407, 3297–3309. [Google Scholar] [CrossRef] [PubMed]
- Goense, L.; Meziani, J.; Ruurda, J.P.; Van Hillegersberg, R. Impact of postoperative complications on outcomes after oesophagectomy for cancer. Br. J. Surg. 2018, 106, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Markar, S.; Gronnier, C.; Duhamel, A.; Mabrut, J.-Y.; Bail, J.-P.; Carrere, N.; Lefevre, J.H.; Brigand, C.; Vaillant, J.-C.; Adham, M.; et al. The Impact of Severe Anastomotic Leak on Long-term Survival and Cancer Recurrence after Surgical Resection for Esophageal Malignancy. Ann. Surg. 2015, 262, 972–980. [Google Scholar] [CrossRef]
- Aiolfi, A.; Griffiths, E.A.; Sozzi, A.; Manara, M.; Bonitta, G.; Bonavina, L.; Bona, D. Effect of Anastomotic Leak on Long-Term Survival after Esophagectomy: Multivariate Meta-analysis and Restricted Mean Survival Times Examination. Ann. Surg. Oncol. 2023, 30, 5564–5572. [Google Scholar] [CrossRef]
- Bona, D.; Manara, M.; Bonitta, G.; Guerrazzi, G.; Guraj, J.; Lombardo, F.; Biondi, A.; Cavalli, M.; Bruni, P.G.; Campanelli, G.; et al. Long-Term Impact of Severe Postoperative Complications after Esophagectomy for Cancer: Individual Patient Data Meta-Analysis. Cancers 2024, 16, 1468. [Google Scholar] [CrossRef]
- Manara, M.; Bona, D.; Bonavina, L.; Aiolfi, A.; Bonitta, G.; Guraj, J.; Guerrazzi, G.; Campanelli, G.; Cavalli, M.; Popa, C.; et al. Impact of pulmonary complications following esophagectomy on long-term survival: Multivariate meta-analysis and restricted mean survival time assessment. Updates Surg. 2024, 76, 757–767. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, Y.; Niimi, M.; Kan, S.; Shatari, T.; Takami, H.; Kodaira, S. Clinical significance of tissue blood flow during esophagectomy by laser Doppler flowmetry. J. Thorac. Cardiovasc. Surg. 2001, 122, 1101–1106. [Google Scholar] [CrossRef]
- Aiolfi, A.; Bona, D.; Bonitta, G.; Bonavina, L.; Cayre, L.; Gutschow, C.A.; Lipham, J.; Manara, M.; Popa, C.; Rausa, E.; et al. Effect of gastric ischemic conditioning prior to esophagectomy: Systematic review and meta-analysis. Updates Surg. 2023, 75, 1633–1643. [Google Scholar] [CrossRef]
- Aiolfi, A.; Bona, D.; Bonitta, G.; Bonavina, L.; Gastric Ischemic Conditioning (GIC) International Collaborative Group. Short-term Outcomes of Different Techniques for Gastric Ischemic Preconditioning Before Esophagectomy: A Network Meta-analysis. Ann. Surg. 2024, 279, 410–418. [Google Scholar] [CrossRef]
- Sakr, Y. Techniques to assess tissue oxygenation in the clinical setting. Transfus. Apher. Sci. 2010, 43, 79–94. [Google Scholar] [CrossRef] [PubMed]
- Urbanavičius, L. How to assess intestinal viability during surgery: A review of techniques. World J. Gastrointest. Surg. 2011, 3, 59–69. [Google Scholar] [CrossRef]
- Schröder, W.; Stippel, D.; Beckurts, K.; Lacher, M.; Gutschow, C.; Hölscher, A. Intraoperative changes of mucosal pCO2 during gastric tube formation. Langenbeck’s Arch. Surg. 2001, 386, 324–327. [Google Scholar] [CrossRef]
- Pham, T.H.; Perry, K.A.; Enestvedt, C.K.; Gareau, D.; Dolan, J.P.; Sheppard, B.C.; Jacques, S.L.; Hunter, J.G. Decreased Conduit Perfusion Measured by Spectroscopy Is Associated with Anastomotic Complications. Ann. Thorac. Surg. 2011, 91, 380–385. [Google Scholar] [CrossRef]
- Karliczek, A.; Harlaar, N.J.; Zeebregts, C.J.; Wiggers, T.; Baas, P.C.; Van Dam, G.M. Surgeons lack predictive accuracy for anastomotic leakage in gastrointestinal surgery. Int. J. Color. Dis. 2009, 24, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Ladak, F.; Dang, J.T.; Switzer, N.; Mocanu, V.; Tian, C.; Birch, D.; Turner, S.R.; Karmali, S. Indocyanine green for the prevention of anastomotic leaks following esophagectomy: A meta-analysis. Surg. Endosc. 2019, 33, 384–394. [Google Scholar] [CrossRef] [PubMed]
- Casas, M.A.; Angeramo, C.A.; Bras Harriott, C.; Dreifuss, N.H.; Schlottmann, F. Indocyanine green (ICG) fluorescence imaging for prevention of anastomotic leak in totally minimally invasive Ivor Lewis esophagectomy: A systematic review and meta-analysis. Dis. Esophagus 2022, 35, doab056. [Google Scholar] [CrossRef]
- Nusrath, S.; Kalluru, P.; Shukla, S.; Dharanikota, A.; Basude, M.; Jonnada, P.; Abualjadayel, M.; Alabbad, S.; Mir, T.A.; Broering, D.C.; et al. Current status of indocyanine green fluorescent angiography in assessing perfusion of gastric conduit and oesophago-gastric anastomosis. Int. J. Surg. 2024, 110, 1079–1089. [Google Scholar] [CrossRef]
- Brooke, B.S.; Schwartz, T.A.; Pawlik, T.M. MOOSE Reporting Guidelines for Meta-analyses of Observational Studies. JAMA Surg. 2021, 156, 787–788. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Booth, A.; Clarke, M.; Dooley, G.; Ghersi, D.; Moher, D.; Petticrew, M.; Stewart, L. The nuts and bolts of PROSPERO: An international prospective register of systematic reviews. Syst. Rev. 2012, 1, 2. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res. Synth. Method 2010, 1, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Statist. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- R Foundation for Statistical Computing. R A Language and Environment Gor Statistical Computing: Reference Index; R Foundation for Statistical Computing: Vienna, Austria, 2010. [Google Scholar]
- Campbell, C.; Reames, M.K.; Robinson, M.; Symanowski, J.; Salo, J.C. Conduit Vascular Evaluation is Associated with Reduction in Anastomotic Leak after Esophagectomy. J. Gastrointest. Surg. 2015, 19, 806–812. [Google Scholar] [CrossRef]
- Hodari, A.; Park, K.U.; Lace, B.; Tsiouris, A.; Hammoud, Z. Robot-Assisted Minimally Invasive Ivor Lewis Esophagectomy with Real-Time Perfusion Assessment. Ann. Thorac. Surg. 2015, 100, 947–952. [Google Scholar] [CrossRef]
- Karampinis, I.; Ronellenfitsch, U.; Mertens, C.; Gerken, A.; Hetjens, S.; Post, S.; Kienle, P.; Nowak, K. Indocyanine green tissue angiography affects anastomotic leakage after esophagectomy. A retrospective, case-control study. Int. J. Surg. 2017, 48, 210–214. [Google Scholar] [CrossRef]
- Dalton, B.G.A.; Ali, A.A.; Crandall, M.; Awad, Z.T. Near infrared perfusion assessment of gastric conduit during minimally invasive Ivor Lewis esophagectomy. Am. J. Surg. 2018, 216, 524–527. [Google Scholar] [CrossRef] [PubMed]
- Ohi, M.; Toiyama, Y.; Mohri, Y.; Saigusa, S.; Ichikawa, T.; Shimura, T.; Yasuda, H.; Okita, Y.; Yoshiyama, S.; Kobayashi, M.; et al. Prevalence of anastomotic leak and the impact of indocyanine green fluorescein imaging for evaluating blood flow in the gastric conduit following esophageal cancer surgery. Esophagus 2017, 14, 351–359. [Google Scholar] [CrossRef] [PubMed]
- Noma, K.; Shirakawa, Y.; Kanaya, N.; Okada, T.; Maeda, N.; Ninomiya, T.; Tanabe, S.; Sakurama, K.; Fujiwara, T. Visualized Evaluation of Blood Flow to the Gastric Conduit and Complications in Esophageal Reconstruction. J. Am. Coll. Surg. 2018, 226, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Luo, R.-J.; Zhu, Z.-Y.; He, Z.-F.; Xu, Y.; Wang, Y.-Z.; Chen, P. Efficacy of Indocyanine Green Fluorescence Angiography in Preventing Anastomotic Leakage after McKeown Minimally Invasive Esophagectomy. Front. Oncol. 2021, 10, 619822. [Google Scholar] [CrossRef]
- Shishido, Y.; Matsunaga, T.; Makinoya, M.; Miyauchi, W.; Shimizu, S.; Miyatani, K.; Uejima, C.; Morimoto, M.; Murakami, Y.; Hanaki, T.; et al. Circular stapling anastomosis with indocyanine green fluorescence imaging for cervical esophagogastric anastomosis after thoracoscopic esophagectomy: A propensity score-matched analysis. BMC Surg. 2022, 22, 152. [Google Scholar] [CrossRef]
- Banks, K.C.; Barnes, K.E.; Wile, R.K.; Hung, Y.-Y.; Santos, J.; Hsu, D.S.; Choe, G.; Elmadhun, N.Y.; Ashiku, S.K.; Patel, A.R.; et al. Outcomes of Anastomotic Evaluation Using Indocyanine Green Fluorescence during Minimally Invasive Esophagectomy. Am. Surg. TM 2023, 89, 5124–5130. [Google Scholar] [CrossRef]
- LeBlanc, G.; Takahashi, C.; Huston, J.; Shridhar, R.; Meredith, K. The use of indocyanine green (ICYG) angiography intraoperatively to evaluate gastric conduit perfusion during esophagectomy: Does it impact surgical decision-making? Surg. Endosc. 2023, 37, 8720–8727. [Google Scholar] [CrossRef]
- Nguyen, D.T.; Dat, T.Q.; Thong, D.Q.; Hai, N.V.; Bac, N.H.; Long, V.D. Role of indocyanine green fluorescence imaging for evaluating blood supply in the gastric conduit via the substernal route after McKeown minimally invasive esophagectomy. J. Gastrointest. Surg. 2024, 28, 351–358. [Google Scholar] [CrossRef]
- Bonavina, L.; Asti, E.; Sironi, A.; Bernardi, D.; Aiolfi, A. Hybrid and total minimally invasive esophagectomy: How I do it. J. Thorac. Dis. 2017, 9, S761–S772. [Google Scholar] [CrossRef] [PubMed]
- Bona, D.; Lombardo, F.; Matsushima, K.; Cavalli, M.; Lastraioli, C.; Bonitta, G.; Cirri, S.; Danelli, P.; Aiolfi, A. Three-field versus two-field lymphadenectomy for esophageal squamous cell carcinoma: A long-term survival meta-analysis. Surgery 2022, 171, 940–947. [Google Scholar] [CrossRef]
- Kumagai, Y.; Ishiguro, T.; Haga, N.; Kuwabara, K.; Kawano, T.; Ishida, H. Hemodynamics of the Reconstructed Gastric Tube during Esophagectomy: Assessment of Outcomes with Indocyanine Green Fluorescence. World J. Surg. 2014, 38, 138–143. [Google Scholar] [CrossRef]
- Pacheco, P.E.; Hill, S.M.; Henriques, S.M.; Paulsen, J.K.; Anderson, R.C. The novel use of intraoperative laser-induced fluorescence of indocyanine green tissue angiography for evaluation of the gastric conduit in esophageal reconstructive surgery. Am. J. Surg. 2013, 205, 349–353. [Google Scholar] [CrossRef] [PubMed]
- Rino, Y.; Yukawa, N.; Sato, T.; Yamamoto, N.; Tamagawa, H.; Hasegawa, S.; Oshima, T.; Yoshikawa, T.; Masuda, M.; Imada, T. Visualization of blood supply route to the reconstructed stomach by indocyanine green fluorescence imaging during esophagectomy. BMC Med. Imaging 2014, 14, 18. [Google Scholar] [CrossRef]
- Yukaya, T.; Saeki, H.; Kasagi, Y.; Nakashima, Y.; Ando, K.; Imamura, Y.; Ohgaki, K.; Oki, E.; Morita, M.; Maehara, Y. Indocyanine Green Fluorescence Angiography for Quantitative Evaluation of Gastric Tube Perfusion in Patients Undergoing Esophagectomy. J. Am. Coll. Surg. 2015, 221, e37–e42. [Google Scholar] [CrossRef] [PubMed]
- Koyanagi, K.; Ozawa, S.; Oguma, J.; Kazuno, A.; Yamazaki, Y.; Ninomiya, Y.; Ochiai, H.; Tachimori, Y. Blood flow speed of the gastric conduit assessed by indocyanine green fluorescence: New predictive evaluation of anastomotic leakage after esophagectomy. Medicine 2016, 95, e4386. [Google Scholar] [CrossRef]
- Kitagawa, H.; Namikawa, T.; Iwabu, J.; Fujisawa, K.; Uemura, S.; Tsuda, S.; Hanazaki, K. Assessment of the blood supply using the indocyanine green fluorescence method and postoperative endoscopic evaluation of anastomosis of the gastric tube during esophagectomy. Surg. Endosc. 2018, 32, 1749–1754. [Google Scholar] [CrossRef]
- Thammineedi, S.R.; Patnaik, S.C.; Reddy, P.; Saksena, A.R.; Bollineni, N.; Nusrath, S. The Emerging Role of ICG Fluorescence during Minimally Invasive Esophagectomy. Indian J. Surg. Oncol. 2021, 12, 635–636. [Google Scholar] [CrossRef]
- Yamaguchi, K.; Kumagai, Y.; Saito, K.; Hoshino, A.; Tokairin, Y.; Kawada, K.; Nakajima, Y.; Yamazaki, S.; Ishida, H.; Kinugasa, Y. The evaluation of the gastric tube blood flow by indocyanine green fluorescence angiography during esophagectomy: A multicenter prospective study. Gen. Thorac. Cardiovasc. Surg. 2021, 69, 1118–1124. [Google Scholar] [CrossRef]
- Reinhart, M.B.; Huntington, C.R.; Blair, L.J.; Heniford, B.T.; Augenstein, V.A. Indocyanine Green: Historical Context, Current Applications, and Future Considerations. Surg. Innov. 2016, 23, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Murawa, D.; Hünerbein, M.; Spychała, A.; Nowaczyk, P.; Połom, K.; Murawa, P. Indocyanine green angiography for evaluation of gastric conduit perfusion during esophagectomy—First experience. Acta Chir. Belg. 2012, 112, 275–280. [Google Scholar] [CrossRef]
- Zehetner, J.; DeMeester, S.R.; Alicuben, E.T.; Oh, D.S.; Lipham, J.C.; Hagen, J.A.; DeMeester, T.R. Intraoperative Assessment of Perfusion of the Gastric Graft and Correlation with Anastomotic Leaks after Esophagectomy. Ann. Surg. 2015, 262, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Daele, E.V.; Nieuwenhove, Y.V.; Ceelen, W.; Vanhove, C.; Braeckman, B.P.; Hoorens, A.; Limmen, J.V.; Varin, O.; Putte, D.V.D.; Willaert, W.; et al. Near-infrared fluorescence guided esophageal reconstructive surgery: A systematic review. World J. Gastrointest. Oncol. 2019, 11, 250–263. [Google Scholar] [CrossRef] [PubMed]
- Slooter, M.D.; Mansvelders, M.S.E.; Bloemen, P.R.; Gisbertz, S.S.; Bemelman, W.A.; Tanis, P.J.; Hompes, R.; Van Berge Henegouwen, M.I.; De Bruin, D.M. Defining indocyanine green fluorescence to assess anastomotic perfusion during gastrointestinal surgery: Systematic review. BJS Open 2021, 5, zraa074. [Google Scholar] [CrossRef] [PubMed]
- Joosten, J.J.; Slooter, M.D.; van den Elzen, R.M.; Bloemen, P.R.; Gisbertz, S.S.; Eshuis, W.J.; Daams, F.; de Bruin, D.M.; van Berge Henegouwen, M.I. Perfusion assessment by fluorescence time curves in esophagectomy with gastric conduit reconstruction: A prospective clinical study. Surg. Endosc. 2023, 37, 6343–6352. [Google Scholar] [CrossRef] [PubMed]
- Cahill, R.A.; O’Shea, D.F.; Khan, M.F.; Khokhar, H.A.; Epperlein, J.P.; Mac Aonghusa, P.G.; Nair, R.; Zhuk, S.M. Artificial intelligence indocyanine green (ICG) perfusion for colorectal cancer intra-operative tissue classification. Br. J. Surg. 2021, 108, 5–9. [Google Scholar] [CrossRef]
- Bonavina, L. Progress in the esophagogastric anastomosis and the challenges of minimally invasive thoracoscopic surgery. Ann. Transl. Med. 2021, 9, 907. [Google Scholar] [CrossRef]
- Van Workum, F.; Stenstra, M.H.B.C.; Berkelmans, G.H.K.; Slaman, A.E.; Van Berge Henegouwen, M.I.; Gisbertz, S.S.; Van Den Wildenberg, F.J.H.; Polat, F.; Irino, T.; Nilsson, M.; et al. Learning Curve and Associated Morbidity of Minimally Invasive Esophagectomy: A Retrospective Multicenter Study. Ann. Surg. 2019, 269, 88–94. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Author, Year | Study Design | No. Pts | ICG | Gender (M) | BMI (kg/m2) | Age (Years) | NT | Histology | Tumour Stage | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AdK | SCC | Other | 1 | 2 | 3 | 4 | |||||||||
| Campbell et al., 2015 [31] | Ret | 90 | ICG | 30 | 27 | NR | 64 (44–81) | 3 | 27 | 1 | 2 | NR | NR | NR | NR |
| nICG | 60 | 47 | NR | 62 (22–76) | 34 | 48 | 7 | 4 | NR | NR | NR | NR | |||
| Hodari et al., 2015 [32] | Ret | 54 | ICG | 39 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| nICG | 15 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | |||
| Karampinis et al., 2017 [33] | Ret | 88 | ICG | 33 | 24 | 28.8 ± 4.2 | 65.7 ± 8.5 | 25 | 25 | 7 | 1 | 7 | 10 | 12 | 4 |
| nICG | 55 | 41 | 25.8 ± 4.3 | 60.5 ± 8.5 | 44 | NR | NR | NR | 17 | 25 | 10 | 3 | |||
| Dalton et al., 2017 [34] | Pros | 40 | ICG | 20 | 16 | 26.4 ± 4.9 | 61.8 ± 12.8 | 17 | NR | NR | NR | NR | NR | NR | NR |
| nICG | 20 | 16 | 26.3 ± 4.1 | 66.2 ± 8.0 | 19 | NR | NR | NR | NR | NR | NR | NR | |||
| Ohi et al., 2017 [35] | Ret | 120 | ICG | 59 | NR | NR | 68 (63–74) | NR | NR | NR | NR | NR | NR | NR | NR |
| nICG | 61 | NR | NR | 68 (63–74) | NR | NR | NR | NR | NR | NR | NR | NR | |||
| Noma et al., 2018 [36] | Ret, PS | 136 | ICG | 68 | 56 | 22.1 ± 2.7 | 65.3 ± 8.1 | 39 | 3 | 62 | 3 | 33 | 17 | 13 | 5 |
| nICG | 68 | 59 | 22.1 ± 3.4 | 64.3 ± 7.5 | 37 | 2 | 64 | 2 | 31 | 10 | 25 | 2 | |||
| Luo et al., 2020 [37] | Ret | 192 | ICG | 86 | 74 | 22.6 ± 2.9 | 65.8 ± 6.5 | 14 | 2 | 84 | 0 | 28 | 22 | 34 | 2 |
| nICG | 106 | 97 | 22.1 ± 3.3 | 64.9 ± 6.9 | 12 | 0 | 101 | 5 | 32 | 26 | 42 | 6 | |||
| Shishido et al., 2022 [38] | Pros, PS | 66 | ICG | 33 | 27 | 21.9 ± 3.3 | 67 (63–73) | 17 | 2 | 30 | 1 | 13 | 10 | 10 | 0 |
| nICG | 33 | 30 | 21.8 ± 3.1 | 65 (61–73) | 17 | 2 | 30 | 1 | 16 | 5 | 12 | 0 | |||
| Banks et al., 2023 [39] | Ret | 181 | ICG | 59 | 46 | 25.9 ± 4.9 | 66.9 ± 8.6 | 52 | 49 | 9 | 1 | 20 | 12 | 20 | 7 |
| nICG | 122 | 98 | 27.3 ± 5.2 | 64.4 ± 10.2 | 114 | 107 | 14 | 1 | 40 | 30 | 29 | 23 | |||
| LeBlanc et al., 2023 [40] | Pros | 312 | ICG | 61 | 48 | 27.5 ± 5.9 | 70 (51–82) | 47 | 48 | 10 | 3 | NR | NR | NR | NR |
| nICG | 251 | 202 | 27.3 ± 6.6 | 67 (30–91) | 199 | 206 | 33 | 12 | NR | NR | NR | NR | |||
| Nguyen et al., 2024 [41] | Ret | 120 | ICG | 88 | 82 | 20.3 ± 2.9 | 62.5 ± 8.1 | 25 | 6 | 81 | 1 | NR | NR | NR | NR |
| nICG | 32 | 32 | 18.9 ± 3.1 | 63.3 ± 8.1 | 8 | 2 | 30 | 0 | NR | NR | NR | NR | |||
| Author, Year | ICG | Procedure | Thoracic Approach | Anastomosis | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| IL | MK | O | TS | R | HS | CS | LS | |||
| Campbell et al., 2015 [31] | ICG | 30 | 30 | 0 | 2 | 28 | 0 | 0 | 30 | 0 |
| nICG | 60 | 60 | 0 | 6 | 54 | 0 | 0 | 60 | 0 | |
| Hodari et al., 2015 [32] | ICG | 39 | 39 | 0 | 0 | 0 | 39 | 0 | 0 | 39 |
| nICG | 15 | 15 | 0 | 0 | 0 | 15 | 0 | 0 | 15 | |
| Karampinis et al., 2017 [33] | ICG | 33 | 25 | 8 | 0 | 33 | 0 | 8 | 25 | 0 |
| nICG | 55 | 38 | 17 | 0 | 55 | 0 | 17 | 38 | 0 | |
| Dalton et al., 2017 [34] | ICG | 20 | 20 | 0 | 0 | 20 | 0 | 0 | 20 | 0 |
| nICG | 20 | 20 | 0 | 0 | 20 | 0 | 0 | 20 | 0 | |
| Ohi et al., 2017 [35] | ICG | 59 | NR | NR | NR | NR | NR | NR | NR | NR |
| nICG | 61 | NR | NR | NR | NR | NR | NR | NR | NR | |
| Noma et al., 2018 [36] | ICG | 68 | 0 | 68 | 8 | 60 | 0 | 14 | 49 | 5 |
| nICG | 68 | 0 | 68 | 21 | 47 | 0 | 14 | 50 | 6 | |
| Luo et al., 2020 [37] | ICG | 86 | 0 | 86 | NR | NR | NR | 0 | 86 | 0 |
| nICG | 106 | 0 | 106 | NR | NR | NR | 0 | 106 | 0 | |
| Shishido et al., 2022 [38] | ICG | 33 | 33 | 0 | 0 | 30 | 3 | 0 | 33 | 0 |
| nICG | 33 | 33 | 0 | 0 | 33 | 0 | 0 | 33 | 0 | |
| Banks et al., 2023 [39] | ICG | 59 | 59 | 0 | 0 | 59 | 0 | 0 | 59 | 0 |
| nICG | 122 | 122 | 0 | 0 | 122 | 0 | 0 | 122 | 0 | |
| LeBlanc et al., 2023 [40] | ICG | 61 | NR | NR | 0 | 0 | 61 | NR | NR | NR |
| nICG | 251 | NR | NR | 0 | 0 | 251 | NR | NR | NR | |
| Nguyen et al., 2024 [41] | ICG | 88 | 0 | 88 | 0 | 88 | 0 | NR | NR | NR |
| nICG | 32 | 0 | 32 | 0 | 32 | 0 | NR | NR | NR | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sozzi, A.; Bona, D.; Yeow, M.; Habeeb, T.A.A.M.; Bonitta, G.; Manara, M.; Sangiorgio, G.; Biondi, A.; Bonavina, L.; Aiolfi, A. Does Indocyanine Green Utilization during Esophagectomy Prevent Anastomotic Leaks? Systematic Review and Meta-Analysis. J. Clin. Med. 2024, 13, 4899. https://doi.org/10.3390/jcm13164899
Sozzi A, Bona D, Yeow M, Habeeb TAAM, Bonitta G, Manara M, Sangiorgio G, Biondi A, Bonavina L, Aiolfi A. Does Indocyanine Green Utilization during Esophagectomy Prevent Anastomotic Leaks? Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2024; 13(16):4899. https://doi.org/10.3390/jcm13164899
Chicago/Turabian StyleSozzi, Andrea, Davide Bona, Marcus Yeow, Tamer A. A. M. Habeeb, Gianluca Bonitta, Michele Manara, Giuseppe Sangiorgio, Antonio Biondi, Luigi Bonavina, and Alberto Aiolfi. 2024. "Does Indocyanine Green Utilization during Esophagectomy Prevent Anastomotic Leaks? Systematic Review and Meta-Analysis" Journal of Clinical Medicine 13, no. 16: 4899. https://doi.org/10.3390/jcm13164899
APA StyleSozzi, A., Bona, D., Yeow, M., Habeeb, T. A. A. M., Bonitta, G., Manara, M., Sangiorgio, G., Biondi, A., Bonavina, L., & Aiolfi, A. (2024). Does Indocyanine Green Utilization during Esophagectomy Prevent Anastomotic Leaks? Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 13(16), 4899. https://doi.org/10.3390/jcm13164899