

Distal Triceps Tendon Repair in Strength Athletes Leads to Satisfactory Return to Sports: A Retrospective Analysis of 22 Cases

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Surgical Technique
2.2. Postoperative Rehab
2.3. Follow-Up Questionnaire
2.4. Statistical Methods
3. Results
3.1. Demographics
3.2. Sports Disciplines
3.3. Subjective Rating and Well-Being
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stucken, C.; Ciccotti, M.G. Distal Biceps and Triceps Injuries in Athletes. Sports Med. Arthrosc. Rev. 2014, 22, 153–163. [Google Scholar] [CrossRef]
- Lee, E.; Stillson, Q.A.; Seidel, H.D.; Bhattacharjee, S.; Koh, J.L.; Strelzow, J.A.; Shi, L.L. Surgical Outcomes, Trends, and Risk Factors of Distal Triceps Repairs. HAND 2023, 18, 1300–1306. [Google Scholar] [CrossRef]
- Anzel, S.H.; Covey, K.W.; Weiner, A.D.; Lipscomb, P.R. Disruption of Muscles and Tendons; an Analysis of 1014 Cases. Surgery 1959, 45, 406–414. [Google Scholar]
- Yeh, P.C.; Dodds, S.D.; Smart, R.L.; Mazzocca, A.D.; Sethi, P.M. Distal Triceps Rupture. Am. Acad. Orthop. Surg. 2010, 18, 31–40. [Google Scholar] [CrossRef]
- Mair, S.D.; Isbell, W.M.; Gill, T.J.; Schlegel, T.F.; Hawkins, R.J. Triceps Tendon Ruptures in Professional Football Players. Am. J. Sports Med. 2004, 32, 431–434. [Google Scholar] [CrossRef] [PubMed]
- Stannard, J.P.; Bucknell, A.L. Rupture of the Triceps Tendon Associated with Steroid Injections. Am. J. Sports Med. 1993, 21, 482–485. [Google Scholar] [CrossRef] [PubMed]
- Visuri, T.; Lindholm, H. Bilateral Distal Biceps Tendon Avulsions with Use of Anabolic Steroids. Med. Sci. Sports Exerc. 1994, 26, 941–944. [Google Scholar] [CrossRef]
- García-Arnés, J.A.; García-Casares, N. Doping and Sports Endocrinology: Anabolic-Androgenic Steroids. Rev. Clín. Esp. (Engl. Ed.) 2022, 222, 612–620. [Google Scholar] [CrossRef] [PubMed]
- van Riet, R.P.; Morrey, B.F.; Ho, E.; O’Driscoll, S.W. Surgical Treatment of Distal Triceps Ruptures. J. Bone Jt. Surg. Am. 2003, 85, 1961–1967. [Google Scholar] [CrossRef]
- Horneff, J.G.; Aleem, A.; Nicholson, T.; Lervick, G.; Murthi, A.; Sethi, P.; Getz, C.; Lazarus, M.D.; Ramsey, M.L.; Abboud, J.A.; et al. Functional Outcomes of Distal Triceps Tendon Repair Comparing Transosseous Bone Tunnels with Suture Anchor Constructs. J. Shoulder Elbow Surg. 2017, 26, 2213–2219. [Google Scholar] [CrossRef]
- Mirzayan, R.; Acevedo, D.C.; Sodl, J.F.; Yian, E.H.; Navarro, R.A.; Anakwenze, O.; Singh, A. Operative Management of Acute Triceps Tendon Ruptures: Review of 184 Cases. Am. J. Sports Med. 2018, 46, 1451–1458. [Google Scholar] [CrossRef]
- Alnaji, O.; Erdogan, S.; Shanmugaraj, A.; AlQahtani, S.; Prada, C.; Leroux, T.; Khan, M. The Surgical Management of Distal Triceps Tendon Ruptures: A Systematic Review. J. Shoulder Elbow Surg. 2022, 31, 217–224. [Google Scholar] [CrossRef]
- Dorweiler, M.A.; Van Dyke, R.O.; Siska, R.C.; Boin, M.A.; DiPaola, M.J. A Comparative Biomechanical Analysis of 2 Double-Row, Distal Triceps Tendon Repairs. Orthop. J. Sports Med. 2017, 5, 232596711770830. [Google Scholar] [CrossRef]
- Yeh, P.C.; Stephens, K.T.; Solovyova, O.; Obopilwe, E.; Smart, L.R.; Mazzocca, A.D.; Sethi, P.M. The Distal Triceps Tendon Footprint and a Biomechanical Analysis of 3 Repair Techniques. Am. J. Sports Med. 2010, 38, 1025–1033. [Google Scholar] [CrossRef] [PubMed]
- Agarwalla, A.; Gowd, A.K.; Jan, K.; Liu, J.N.; Garcia, G.H.; Naami, E.; Wysocki, R.W.; Fernandez, J.J.; Cohen, M.S.; Verma, N.N. Return to Work Following Distal Triceps Repair. J. Shoulder Elbow Surg. 2021, 30, 906–912. [Google Scholar] [CrossRef]
- Agarwalla, A.; Gowd, A.K.; Liu, J.N.; Garcia, G.H.; Jan, K.; Naami, E.; Wysocki, R.W.; Fernandez, J.J.; Cohen, M.S.; Verma, N.N. Return to Sport Following Distal Triceps Repair. J. Hand Surg. Am. 2022, 4, 507.e1–507.e8. [Google Scholar] [CrossRef]
- Blackmore, S.M.; Jander, R.M.; Culp, R.W. Management of Distal Biceps and Triceps Ruptures. J. Hand Ther. 2006, 19, 154–169. [Google Scholar] [CrossRef] [PubMed]
- Giannicola, G.; Bullitta, G.; Rotini, R.; Murena, L.; Blonna, D.; Iapicca, M.; Restuccia, G.; Merolla, G.; Fontana, M.; Greco, A.; et al. Results of Primary Repair of Distal Triceps Tendon Ruptures in a General Population: A Multicentre Study. Bone Jt. J. 2018, 100, 610–616. [Google Scholar] [CrossRef] [PubMed]
- Demirhan, M.; Ersen, A. Distal Triceps Ruptures. EFORT Open Rev. 2016, 1, 255–259. [Google Scholar] [CrossRef]
- Gaviria, M.; Ren, B.; Brown, S.M.; McCluskey, L.C.; Savoie, F.H.; Mulcahey, M.K. Triceps Tendon Ruptures. JBJS Rev. 2020, 8, e0172. [Google Scholar] [CrossRef]
- Khiami, F.; Tavassoli, S.; De Ridder Baeur, L.; Catonné, Y.; Sariali, E. Distal Partial Ruptures of Triceps Brachii Tendon in an Athlete. Orthop. Traumatol. Surg. Res. 2012, 98, 242–246. [Google Scholar] [CrossRef] [PubMed]
- Bain, G.I.; Durrant, A.W. Sports-Related Injuries of the Biceps and Triceps. Clin. Sports Med. 2010, 29, 555–576. [Google Scholar] [CrossRef]
- Ritsch, M.; Regauer, M.; Schoch, C. Surgical Treatment of Distal Triceps Tendon Ruptures. Oper. Orthop. Traumatol. 2022, 34, 438–446. [Google Scholar] [CrossRef]
- Dunn, J.C.; Kusnezov, N.; Fares, A.; Rubin, S.; Orr, J.; Friedman, D.; Kilcoyne, K. Triceps Tendon Ruptures: A Systematic Review. Hand 2017, 12, 431–438. [Google Scholar] [CrossRef]
- Tran, D.V.; Yetter, T.R.; Somerson, J.S. Surgical Repair of Distal Triceps Rupture: A Systematic Review of Outcomes and Complications. JSES Rev. Rep. Tech. 2022, 2, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Walker, C.M.; Noonan, T.J. Distal Triceps Tendon Injuries. Clin. Sports Med. 2020, 39, 673–685. [Google Scholar] [CrossRef] [PubMed]
- Sagoe, D.; Molde, H.; Andreassen, C.S.; Torsheim, T.; Pallesen, S. The Global Epidemiology of Anabolic-Androgenic Steroid Use: A Meta-Analysis and Meta-Regression Analysis. Ann. Epidemiol. 2014, 24, 383–398. [Google Scholar] [CrossRef]
- Kose, O.; Kilicaslan, O.F.; Guler, F.; Acar, B.; Yuksel, H.Y. Functional Outcomes and Complications after Surgical Repair of Triceps Tendon Rupture. Eur. J. Orthop. Surg. Traumatol. 2015, 25, 1131–1139. [Google Scholar] [CrossRef]
- Harris, P.C.; Atkinson, D.; Moorehead, J.D. Bilateral Partial Rupture of Triceps Tendon. Am. J. Sports Med. 2004, 32, 787–792. [Google Scholar] [CrossRef]
- Balazs, G.C.; Brelin, A.M.; Dworak, T.C.; Brooks, D.I.; Mauntel, T.C.; Tintle, S.M.; Dickens, J.F. Outcomes and Complications of Triceps Tendon Repair Following Acute Rupture in American Military Personnel. Injury 2016, 47, 2247–2251. [Google Scholar] [CrossRef]
- Freislederer, F.; Papillo, D.; Glanzmann, M.; Scheibel, M. Distale Bizepssehnen- und Trizepssehnenrupturen. Z. Orthop. Unfall 2020, 158, 663–682. [Google Scholar] [CrossRef]
- Macknet, D.M.; Ford, S.E.; Mak, R.A.; Loeffler, B.J.; Connor, P.M.; Gaston, R.G. Complications after Traumatic Distal Triceps Tears: An Analysis of 107 Cases. JSES Rev. Rep. Tech. 2022, 2, 520–525. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| <45 Years (n = 11) | ≥45 Years (n = 11) | Overall (n = 22) | |
|---|---|---|---|
| Gender (m/f) | 11/0 (100%/0%) | 11/0 (100%/0%) | 22/0 (100%/0%) |
| Age (years) | 35.5 (4.4) | 53.1 (4.7) | 44.3 (9.9) |
| BMI (kg/m2) | 30.5 (8.97) | 29.4 (2.83) | 29.94 (6.71) |
| Affected side (L/r) | 6/5 (55%/45%) | 6/5 (55%/45%) | 12/10 (55%/45%) |
| Cause of injury (sports-related/other) | 10/1 (91%/9%) | 8/3 (73%/27%) | 18/4 (82%/18%) |
| Subgroup | <45 Years (n = 11) | ≥45 Years (n = 11) | p-Value b | Overall (n = 22) |
|---|---|---|---|---|
| Sporting activities | ||||
| preOP | 2.7 (1.7) | 2.0 (0.9) | 0.224 | 2.4 (1.4) |
| postOP | 2.7 (1.9) | 2.2 (1.3) | 0.427 | 2.5 (1.6) |
| p-value c | 1 | 0.341 | 0.540 | |
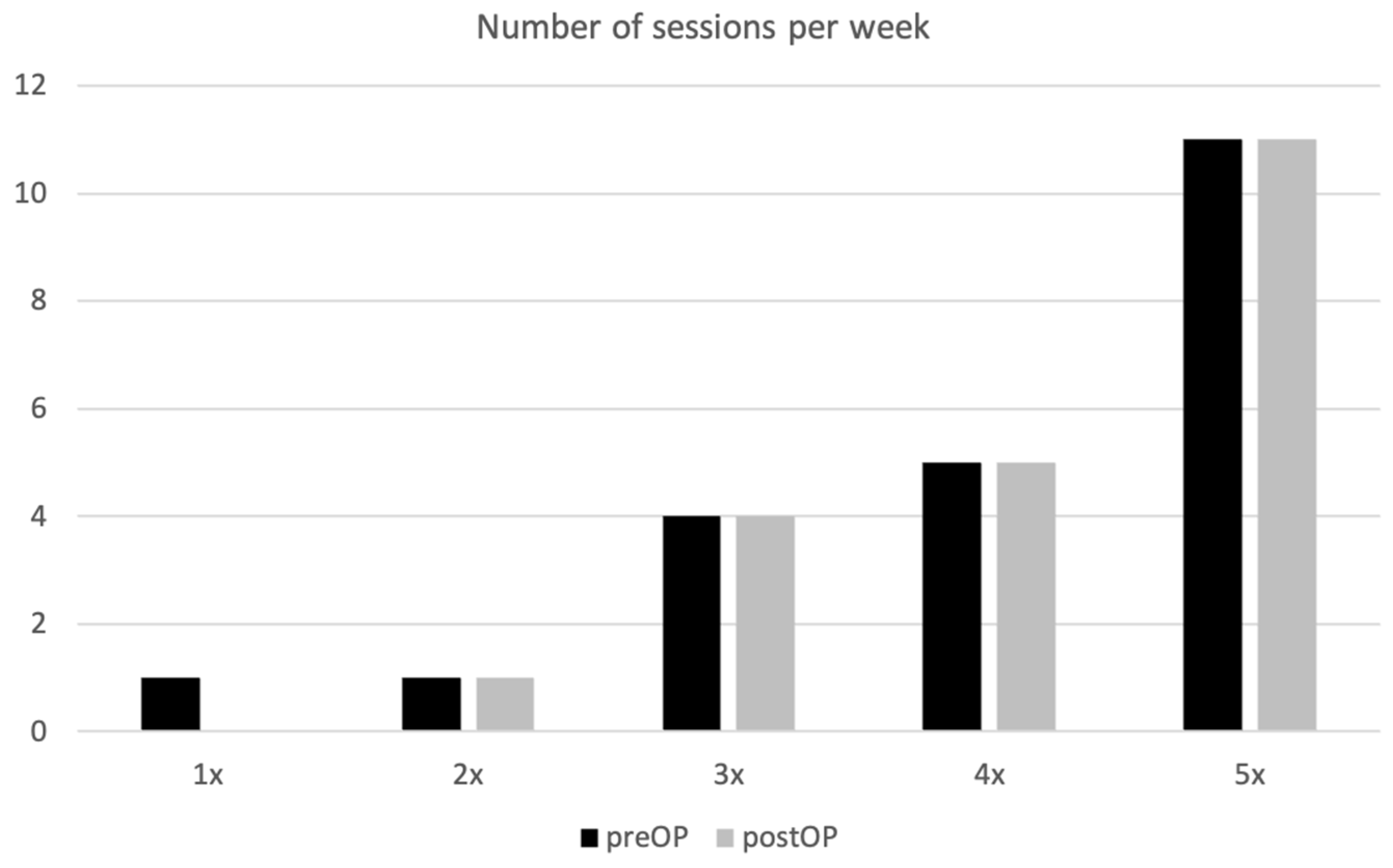
| Frequency (per week) | ||||
| preOP | 4.2 (1.3) | 4.0 (1.0) | 0.721 | 4.1 (1.2) |
| postOP | 4.1 (1.6) | 4.0 (1.0) | 0.873 | 4.1 (1.3) |
| p-value c | 0.341 | 1 | 0.329 |
| Subgroup | <45 Years (n = 11) | ≥45 Years (n = 11) | p-Value b | Overall (n = 22) |
|---|---|---|---|---|
| VAS pain (0–10) | ||||
| preOP | 5.5 (3.3) | 6.7 (2.6) | 0.422 | 6.0 (3.0) |
| postOP | 1.6 (1.8) | 1.6 (1.1) | 0.416 | 1.6 (1.5) |
| p-value c | 0.016 | <0.001 | <0.001 | |
| Level of fitness (0–10) | ||||
| preOP | 5.0 (3.6) | 5.3 (3.3) | 0.952 | 5.1 (3.4) |
| postOP | 2.8 (2.2) | 2.3 (2.1) | 0.592 | 2.6 (2.1) |
| p-value c | 0.041 | 0.027 | 0.002 | |
| Ability to train (0–10) | ||||
| preOP | 3.6 (3.4) | 7.3 (2.5) | 0.013 | 5.2 (3.4) |
| postOP | 1.8 (1.5) | 1.1 (0.3) | 0.166 | 1.3 (0.6) |
| p-value c | 0.051 | <0.001 | <0.001 | |
| Satisfaction (0–10) | ||||
| Clinical outcome | 1.8 (2.4) | 1.0 (0.0) | 0.386 | 1.5 (1.9) |
| Cosmetic outcome | 1.7 (1.0) | 1.3 (0.5) | 0.210 | 1.5 (0.8) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gruber, M.S.; Bischofreiter, M.; Rittenschober, F.; Schachermayr, M.; Ortmaier, R.; Ritsch, M. Distal Triceps Tendon Repair in Strength Athletes Leads to Satisfactory Return to Sports: A Retrospective Analysis of 22 Cases. J. Clin. Med. 2024, 13, 4913. https://doi.org/10.3390/jcm13164913
Gruber MS, Bischofreiter M, Rittenschober F, Schachermayr M, Ortmaier R, Ritsch M. Distal Triceps Tendon Repair in Strength Athletes Leads to Satisfactory Return to Sports: A Retrospective Analysis of 22 Cases. Journal of Clinical Medicine. 2024; 13(16):4913. https://doi.org/10.3390/jcm13164913
Chicago/Turabian StyleGruber, Michael Stephan, Martin Bischofreiter, Felix Rittenschober, Michael Schachermayr, Reinhold Ortmaier, and Mathias Ritsch. 2024. "Distal Triceps Tendon Repair in Strength Athletes Leads to Satisfactory Return to Sports: A Retrospective Analysis of 22 Cases" Journal of Clinical Medicine 13, no. 16: 4913. https://doi.org/10.3390/jcm13164913
APA StyleGruber, M. S., Bischofreiter, M., Rittenschober, F., Schachermayr, M., Ortmaier, R., & Ritsch, M. (2024). Distal Triceps Tendon Repair in Strength Athletes Leads to Satisfactory Return to Sports: A Retrospective Analysis of 22 Cases. Journal of Clinical Medicine, 13(16), 4913. https://doi.org/10.3390/jcm13164913