
Effects of Environmental Conditions on Athlete’s Cardiovascular System
 , , , , , , , and
, , , , , , , and {kind=link}
Abstract
:1. Introduction
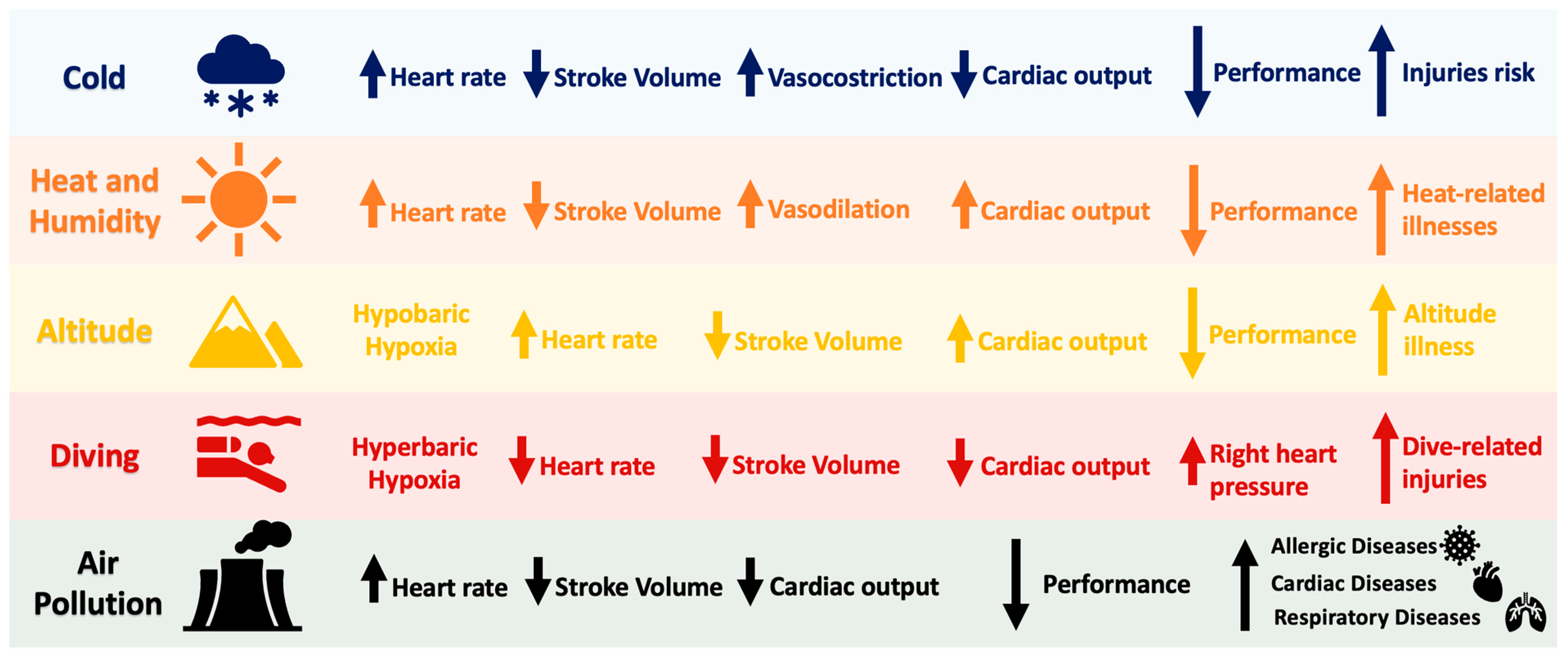
2. Effects of Environmental Factors
2.1. Cold
2.2. Heat
2.3. Air Pollution
2.4. Altitude
2.5. Diving
3. Precautions for Individuals Practicing Sports in Adverse Environmental Conditions
3.1. Clothing and Environmental Protection
3.2. Pre-Cooling Strategies, Hydration, and Nutrition
3.3. Heat Acclimatization
3.4. Cold Adaptation
3.5. High-Altitude and Diving Adaptation
3.6. Organizational and Environmental Considerations
4. Conclusions
Funding
Conflicts of Interest
References
- Bowler, D.E.; Buyung-Ali, L.M.; Knight, T.M.; Pullin, A.S. A systematic review of evidence for the added benefits to health of exposure to natural environments. BMC Public Health 2010, 10, 456. [Google Scholar] [CrossRef]
- Hartig, T.; Mitchell, R.; de Vries, S.; Frumkin, H. Nature and health. Annu. Rev. Public Health 2014, 35, 207–228. [Google Scholar] [CrossRef]
- Burtscher, M.; Gatterer, H.; Burtscher, J.; Mairbäurl, H. Extreme Terrestrial Environments: Life in Thermal Stress and Hypoxia. A Narrative Review. Front. Physiol. 2018, 9, 572. [Google Scholar] [CrossRef]
- Tetzlaff, K.; Thorsen, E. Breathing at depth: Physiologic and clinical aspects of diving while breathing compressed gas. Clin. Chest Med. 2005, 26, 355–380. [Google Scholar] [CrossRef]
- Iso-Ahola, S.E. Intrapersonal and interpersonal factors in athletic performance. Scand. J. Med. Sci. Sports 1995, 5, 191–199. [Google Scholar] [CrossRef]
- Nowak, A.S.; Kennelley, G.E.; Krabak, B.J.; Roberts, W.O.; Tenforde, K.M.; Tenforde, A.S. Endurance athletes and climate change. J. Clim. Chang. Health 2022, 6, 100118. [Google Scholar] [CrossRef]
- Orr, M.; Inoue, Y.; Seymour, R.; Dingle, G. Impacts of climate change on organized sport: A scoping review. Wiley Interdiscip. Rev. Clim. Chang. 2022, 13, e760. [Google Scholar] [CrossRef]
- Çalik, F.; Geri, S. Effects of global climate changes on sports and athletes. J. Rom. Sports Med. Soc. 2022, 18, 3422–3429. [Google Scholar]
- Ngota, J.O.; Odhiambo, D.; Okoti, D. Interrogating the Impact of Climate Change on Multiple Outdoor Sports Activities: A Critical Review. Int. J. Res. Innov. Soc. Sci. 2024, 8, 2193–2199. [Google Scholar] [CrossRef]
- Münzel, T.; Daiber, A. Environmental Stressors and Their Impact on Health and Disease with Focus on Oxidative Stress. Antioxid. Redox Signal. 2018, 28, 735–740. [Google Scholar] [CrossRef]
- Segreti, A.; Picarelli, F.; DI Gioia, G.; Coletti, F.; Crispino, S.P.; Fanale, V.; Fossati, C.; Antonelli Incalzi, R.; Pigozzi, F.; Grigioni, F. Athlete’s heart or heart disease in the athlete? Evaluation by cardiopulmonary exercise testing. J. Sports Med. Phys. Fit. 2023, 63, 873–890. [Google Scholar] [CrossRef]
- Segreti, A.; Celeski, M.; Monticelli, L.M.; Perillo, A.; Crispino, S.P.; Di Gioia, G.; Cammalleri, V.; Fossati, C.; Mega, S.; Papalia, R.; et al. Mitral and Tricuspid Valve Disease in Athletes. J. Clin. Med. 2023, 12, 3562. [Google Scholar] [CrossRef]
- Knechtle, B.; Knechtle, P.; Lepers, R. Participation and performance trends in ultra-triathlons from 1985 to 2009. Scand. J. Med. Sci. Sports 2011, 21, e82–e90. [Google Scholar] [CrossRef]
- Bergeron, M.F.; Bahr, R.; Bärtsch, P.; Bourdon, L.; Calbet, J.A.; Carlsen, K.H.; Castagna, O.; González-Alonso, J.; Lundby, C.; Maughan, R.J.; et al. International Olympic Committee consensus statement on thermoregulatory and altitude challenges for high-level athletes. Br. J. Sports Med. 2012, 46, 770–779. [Google Scholar] [CrossRef]
- Nabeshima, Y.; Addetia, K.; Asch, F.M.; Lang, R.M.; Takeuchi, M. Application of Allometric Methods for Indexation of Left Ventricular End-Diastolic Volume to Normal Echocardiographic Data and Assessing Gender and Racial Differences. J. Am. Soc. Echocardiogr. 2023, 36, 596–603.e593. [Google Scholar] [CrossRef]
- Feng, Z.; Hu, Y.; Yu, S.; Bai, H.; Sun, Y.; Gao, W.; Li, J.; Qin, X.; Zhang, X. Exercise in cold: Friend than foe to cardiovascular health. Life Sci. 2023, 328, 121923. [Google Scholar] [CrossRef] [PubMed]
- Castellani, J.W.; Tipton, M.J. Cold Stress Effects on Exposure Tolerance and Exercise Performance. Compr. Physiol. 2015, 6, 443–469. [Google Scholar] [CrossRef]
- El Helou, N.; Tafflet, M.; Berthelot, G.; Tolaini, J.; Marc, A.; Guillaume, M.; Hausswirth, C.; Toussaint, J.F. Impact of environmental parameters on marathon running performance. PLoS ONE 2012, 7, e37407. [Google Scholar] [CrossRef] [PubMed]
- Corbett, J.; Neal, R.A.; Lunt, H.C.; Tipton, M.J. Adaptation to heat and exercise performance under cooler conditions: A new hot topic. Sports Med. 2014, 44, 1323–1331. [Google Scholar] [CrossRef]
- Seto, C.K.; Way, D.; O’Connor, N. Environmental illness in athletes. Clin. Sports Med. 2005, 24, 695–718. [Google Scholar] [CrossRef]
- Bushman, B.A. Maximizing Safety When Exercising in the Cold. ACSM’s Health Fit. J. 2018, 22, 4–8. [Google Scholar] [CrossRef]
- Pendergast, D.R. The effect of body cooling on oxygen transport during exercise. Med. Sci. Sports Exerc. 1988, 20, S171–S176. [Google Scholar] [CrossRef]
- Cheung, S.S. Responses of the hands and feet to cold exposure. Temperature 2015, 2, 105–120. [Google Scholar] [CrossRef] [PubMed]
- Golden, F.S.; Hampton, I.F.; Hervey, G.R.; Knibbs, A.V. Shivering intensity in humans during immersion in cold water [proceedings]. J. Physiol. 1979, 290, 48p. [Google Scholar]
- Tipton, M.; Bradford, C. Moving in extreme environments: Open water swimming in cold and warm water. Extrem. Physiol. Med. 2014, 3, 12. [Google Scholar] [CrossRef]
- Daniel Tang, K.H. A Review of the Association between Environmental Factors and Athletic Performance. J. Specif. Sport Sci. 2021, 1, 21–30. [Google Scholar]
- Pellicer-Caller, R.; Vaquero-Cristóbal, R.; González-Gálvez, N.; Abenza-Cano, L.; Horcajo, J.; de la Vega-Marcos, R. Influence of Exogenous Factors Related to Nutritional and Hydration Strategies and Environmental Conditions on Fatigue in Endurance Sports: A Systematic Review with Meta-Analysis. Nutrients 2023, 15, 2700. [Google Scholar] [CrossRef]
- Donaldson, G.C.; Keatinge, W.R.; Saunders, R.D. Cardiovascular responses to heat stress and their adverse consequences in healthy and vulnerable human populations. Int. J. Hyperth. 2003, 19, 225–235. [Google Scholar] [CrossRef]
- Sawka, M.N.; Leon, L.R.; Montain, S.J.; Sonna, L.A. Integrated physiological mechanisms of exercise performance, adaptation, and maladaptation to heat stress. Compr. Physiol. 2011, 1, 1883–1928. [Google Scholar] [CrossRef]
- Liu, W.H.; Li, Z.Y.; Loh, Y.C. Evaluation of the impact of hot environmental conditions on physical activity among soccer players. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 8216–8223. [Google Scholar] [CrossRef]
- Cui, J.; Arbab-Zadeh, A.; Prasad, A.; Durand, S.; Levine, B.D.; Crandall, C.G. Effects of heat stress on thermoregulatory responses in congestive heart failure patients. Circulation 2005, 112, 2286–2292. [Google Scholar] [CrossRef]
- Bergeron, M.F. Heat cramps: Fluid and electrolyte challenges during tennis in the heat. J. Sci. Med. Sport. 2003, 6, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Hanna, E.G.; Tait, P.W. Limitations to Thermoregulation and Acclimatization Challenge Human Adaptation to Global Warming. Int. J. Environ. Res. Public Health 2015, 12, 8034–8074. [Google Scholar] [CrossRef]
- Dugas, J.P. How hot is too hot?: Some considerations regarding temperature and performance. Int. J. Sports Physiol. Perform. 2010, 5, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Ozgünen, K.T.; Kurdak, S.S.; Maughan, R.J.; Zeren, C.; Korkmaz, S.; Yazici, Z.; Ersöz, G.; Shirreffs, S.M.; Binnet, M.S.; Dvorak, J. Effect of hot environmental conditions on physical activity patterns and temperature response of football players. Scand. J. Med. Sci. Sports 2010, 20 (Suppl. S3), 140–147. [Google Scholar] [CrossRef] [PubMed]
- Montain, S.J.; Ely, M.R.; Cheuvront, S.N. Marathon performance in thermally stressing conditions. Sports Med. 2007, 37, 320–323. [Google Scholar] [CrossRef] [PubMed]
- Walters, T.J.; Ryan, K.L.; Tate, L.M.; Mason, P.A. Exercise in the heat is limited by a critical internal temperature. J. Appl. Physiol. 2000, 89, 799–806. [Google Scholar] [CrossRef]
- Coyle, E.F. Physiological regulation of marathon performance. Sports Med. 2007, 37, 306–311. [Google Scholar] [CrossRef]
- Yankelson, L.; Sadeh, B.; Gershovitz, L.; Werthein, J.; Heller, K.; Halpern, P.; Halkin, A.; Adler, A.; Steinvil, A.; Viskin, S. Life-threatening events during endurance sports: Is heat stroke more prevalent than arrhythmic death? J. Am. Coll. Cardiol. 2014, 64, 463–469. [Google Scholar] [CrossRef]
- Binkley, H.M.; Beckett, J.; Casa, D.J.; Kleiner, D.M.; Plummer, P.E. National Athletic Trainers’ Association position statement: Exertional heat illnesses. J. Athl. Train. 2002, 37, 329. [Google Scholar] [PubMed]
- Hartung, T. Toxicology for the twenty-first century. Nature 2009, 460, 208–212. [Google Scholar] [CrossRef]
- World Health Organization. Regional Office for Europe: Review of Evidence on Health Aspects of Air Pollution: REVIHAAP Project: Technical Report; World Health Organization, Regional Office for Europe: Copenhagen, Denmark, 2021; Available online: https://apps.who.int/iris/handle/10665/341712 (accessed on 13 January 2023).
- Guarnieri, M.; Balmes, J.R. Outdoor air pollution and asthma. Lancet 2014, 383, 1581–1592. [Google Scholar] [CrossRef] [PubMed]
- Rundell, K.W.; Caviston, R. Ultrafine and fine particulate matter inhalation decreases exercise performance in healthy subjects. J. Strength Cond. Res. 2008, 22, 2–5. [Google Scholar] [CrossRef]
- Puett, R.C.; Hart, J.E.; Suh, H.; Mittleman, M.; Laden, F. Particulate matter exposures, mortality, and cardiovascular disease in the health professionals follow-up study. Environ. Health Perspect. 2011, 119, 1130–1135. [Google Scholar] [CrossRef]
- Rundell, K.W.; Hoffman, J.R.; Caviston, R.; Bulbulian, R.; Hollenbach, A.M. Inhalation of ultrafine and fine particulate matter disrupts systemic vascular function. Inhal. Toxicol. 2007, 19, 133–140. [Google Scholar] [CrossRef]
- Pope, C.A., 3rd; Bhatnagar, A.; McCracken, J.P.; Abplanalp, W.; Conklin, D.J.; O’Toole, T. Exposure to Fine Particulate Air Pollution Is Associated With Endothelial Injury and Systemic Inflammation. Circ. Res. 2016, 119, 1204–1214. [Google Scholar] [CrossRef]
- Bhatnagar, A. Environmental cardiology: Studying mechanistic links between pollution and heart disease. Circ. Res. 2006, 99, 692–705. [Google Scholar] [CrossRef]
- Brook, R.D.; Rajagopalan, S.; Pope III, C.A.; Brook, J.R.; Bhatnagar, A.; Diez-Roux, A.V.; Holguin, F.; Hong, Y.; Luepker, R.V.; Mittleman, M.A. Particulate matter air pollution and cardiovascular disease: An update to the scientific statement from the American Heart Association. Circulation 2010, 121, 2331–2378. [Google Scholar] [CrossRef] [PubMed]
- Zoladz, J.A.; Nieckarz, Z. Marathon race performance increases the amount of particulate matter deposited in the respiratory system of runners: An incentive for “clean air marathon runs”. PeerJ 2021, 9, e11562. [Google Scholar] [CrossRef] [PubMed]
- Marr, L.C.; Ely, M.R. Effect of air pollution on marathon running performance. Med. Sci. Sports Exerc. 2010, 42, 585–591. [Google Scholar] [CrossRef]
- Florida-James, G.; Donaldson, K.; Stone, V. Athens 2004: The pollution climate and athletic performance. J. Sports Sci. 2004, 22, 967–980; discussion 980. [Google Scholar] [CrossRef] [PubMed]
- Rundell, K.W. Effect of air pollution on athlete health and performance. Br. J. Sports Med. 2012, 46, 407–412. [Google Scholar] [CrossRef]
- Burtscher, M. Effects of living at higher altitudes on mortality: A narrative review. Aging Dis. 2014, 5, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Mohanna, S.; Baracco, R.; Seclén, S. Lipid profile, waist circumference, and body mass index in a high altitude population. High Alt. Med. Biol. 2006, 7, 245–255. [Google Scholar] [CrossRef]
- Domínguez Coello, S.; Cabrera De León, A.; Bosa Ojeda, F.; Pérez Méndez, L.I.; Díaz González, L.; Aguirre-Jaime, A.J. High density lipoprotein cholesterol increases with living altitude. Int. J. Epidemiol. 2000, 29, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Faeh, D.; Moser, A.; Panczak, R.; Bopp, M.; Röösli, M.; Spoerri, A.; Group, S.N.C.S. Independent at heart: Persistent association of altitude with ischaemic heart disease mortality after consideration of climate, topography and built environment. J. Epidemiol. Community Health 2016, 70, 798–806. [Google Scholar] [CrossRef]
- Lenfant, C.; Sullivan, K. Adaptation to high altitude. N. Engl. J. Med. 1971, 284, 1298–1309. [Google Scholar] [CrossRef]
- Naeije, R. Physiological adaptation of the cardiovascular system to high altitude. Prog. Cardiovasc. Dis. 2010, 52, 456–466. [Google Scholar] [CrossRef]
- Derby, R.; deWeber, K. The athlete and high altitude. Curr. Sports Med. Rep. 2010, 9, 79–85. [Google Scholar] [CrossRef]
- Chen, B.; Wu, Z.; Huang, X.; Li, Z.; Wu, Q.; Chen, Z. Effect of altitude training on the aerobic capacity of athletes: A systematic review and meta-analysis. Heliyon 2023, 9, e20188. [Google Scholar] [CrossRef]
- Khodaee, M.; Grothe, H.L.; Seyfert, J.H.; VanBaak, K. Athletes at High Altitude. Sports Health 2016, 8, 126–132. [Google Scholar] [CrossRef]
- Burtscher, M.; Ponchia, A. The risk of cardiovascular events during leisure time activities at altitude. Prog. Cardiovasc. Dis. 2010, 52, 507–511. [Google Scholar] [CrossRef] [PubMed]
- Burtscher, M. Risk and Protective Factors for Sudden Cardiac Death During Leisure Activities in the Mountains: An Update. Heart Lung Circ. 2017, 26, 757–762. [Google Scholar] [CrossRef]
- Levine, B.D.; Zuckerman, J.H.; deFilippi, C.R. Effect of high-altitude exposure in the elderly: The Tenth Mountain Division study. Circulation 1997, 96, 1224–1232. [Google Scholar] [CrossRef]
- Wolff, S.; Picco, J.M.; Díaz-González, L.; Valenzuela, P.L.; Gonzalez-Dávila, E.; Santos-Lozano, A.; Matile, P.; Wolff, D.; Boraita, A.; Lucia, A. Exercise-Induced Cardiac Fatigue in Recreational Ultramarathon Runners at Moderate Altitude: Insights From Myocardial Deformation Analysis. Front. Cardiovasc. Med. 2021, 8, 744393. [Google Scholar] [CrossRef]
- Foster, G.E.; Sheel, A.W. The human diving response, its function, and its control. Scand. J. Med. Sci. Sports 2005, 15, 3–12. [Google Scholar] [CrossRef]
- Brugniaux, J.V.; Coombs, G.B.; Barak, O.F.; Dujic, Z.; Sekhon, M.S.; Ainslie, P.N. Highs and lows of hyperoxia: Physiological, performance, and clinical aspects. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2018, 315, R1–R27. [Google Scholar] [CrossRef]
- Tso, J.V.; Powers, J.M.; Kim, J.H. Cardiovascular considerations for scuba divers. Heart 2022, 108, 1084–1089. [Google Scholar] [CrossRef] [PubMed]
- Pendergast, D.R.; Lundgren, C.E. The underwater environment: Cardiopulmonary, thermal, and energetic demands. J. Appl. Physiol. 2009, 106, 276–283. [Google Scholar] [CrossRef]
- Heusser, K.; Dzamonja, G.; Tank, J.; Palada, I.; Valic, Z.; Bakovic, D.; Obad, A.; Ivancev, V.; Breskovic, T.; Diedrich, A.; et al. Cardiovascular regulation during apnea in elite divers. Hypertension 2009, 53, 719–724. [Google Scholar] [CrossRef]
- Dumić, J.; Cvetko, A.; Abramović, I.; Šupraha Goreta, S.; Perović, A.; Njire Bratičević, M.; Kifer, D.; Sinčić, N.; Gornik, O.; Žarak, M. Changes in Specific Biomarkers Indicate Cardiac Adaptive and Anti-inflammatory Response of Repeated Recreational SCUBA Diving. Front. Cardiovasc. Med. 2022, 9, 855682. [Google Scholar] [CrossRef]
- Burtscher, M.; Kofler, P.; Gatterer, H.; Faulhaber, M.; Philippe, M.; Fischer, K.; Walther, R.; Herten, A. Effects of lightweight outdoor clothing on the prevention of hypothermia during low-intensity exercise in the cold. Clin. J. Sport. Med. 2012, 22, 505–507. [Google Scholar] [CrossRef] [PubMed]
- Hue, O. The challenge of performing aerobic exercise in tropical environments: Applied knowledge and perspectives. Int. J. Sports Physiol. Perform. 2011, 6, 443–454. [Google Scholar] [CrossRef]
- Wegmann, M.; Faude, O.; Poppendieck, W.; Hecksteden, A.; Fröhlich, M.; Meyer, T. Pre-cooling and sports performance: A meta-analytical review. Sports Med. 2012, 42, 545–564. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.; Laursen, P.B. Keeping your cool: Possible mechanisms for enhanced exercise performance in the heat with internal cooling methods. Sports Med. 2012, 42, 89–98. [Google Scholar] [CrossRef]
- Périard, J.D.; Travers, G.J.S.; Racinais, S.; Sawka, M.N. Cardiovascular adaptations supporting human exercise-heat acclimation. Auton. Neurosci. 2016, 196, 52–62. [Google Scholar] [CrossRef]
- Siegel, A.J.; d’Hemecourt, P.; Adner, M.M.; Shirey, T.; Brown, J.L.; Lewandrowski, K.B. Exertional dysnatremia in collapsed marathon runners: A critical role for point-of-care testing to guide appropriate therapy. Am. J. Clin. Pathol. 2009, 132, 336–340. [Google Scholar] [CrossRef]
- Périard, J.D.; Racinais, S.; Sawka, M.N. Adaptations and mechanisms of human heat acclimation: Applications for competitive athletes and sports. Scand. J. Med. Sci. Sports 2015, 25 (Suppl. S1), 20–38. [Google Scholar] [CrossRef]
- Roberts, W.O.; Armstrong, L.E.; Sawka, M.N.; Yeargin, S.W.; Heled, Y.; O’Connor, F.G. ACSM Expert Consensus Statement on Exertional Heat Illness: Recognition, Management, and Return to Activity. Curr. Sports Med. Rep. 2021, 20, 470–484. [Google Scholar] [CrossRef]
- Armstrong, L.E.; Maresh, C.M. The induction and decay of heat acclimatisation in trained athletes. Sports Med. 1991, 12, 302–312. [Google Scholar] [CrossRef]
- Guy, J.H.; Deakin, G.B.; Edwards, A.M.; Miller, C.M.; Pyne, D.B. Adaptation to hot environmental conditions: An exploration of the performance basis, procedures and future directions to optimise opportunities for elite athletes. Sports Med. 2015, 45, 303–311. [Google Scholar] [CrossRef]
- Ranalli, G.F.; Demartini, J.K.; Casa, D.J.; McDermott, B.P.; Armstrong, L.E.; Maresh, C.M. Effect of body cooling on subsequent aerobic and anaerobic exercise performance: A systematic review. J. Strength Cond. Res. 2010, 24, 3488–3496. [Google Scholar] [CrossRef] [PubMed]
- Gerrett, N.; Kingma, B.R.M.; Sluijter, R.; Daanen, H.A.M. Ambient Conditions Prior to Tokyo 2020 Olympic and Paralympic Games: Considerations for Acclimation or Acclimatization Strategies. Front. Physiol. 2019, 10, 414. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, M.; Assadi, H. Heat acclimation-mediated cross-tolerance in cardioprotection: Do HSP70 and HIF-1alpha play a role? Ann. N. Y. Acad. Sci. 2010, 1188, 199–206. [Google Scholar] [CrossRef]
- Harris, M.B.; Starnes, J.W. Effects of body temperature during exercise training on myocardial adaptations. Am. J. Physiol. Heart Circ. Physiol. 2001, 280, H2271–H2280. [Google Scholar] [CrossRef]
- Périard, J.D.; Eijsvogels, T.M.H.; Daanen, H.A.M. Exercise under heat stress: Thermoregulation, hydration, performance implications, and mitigation strategies. Physiol. Rev. 2021, 101, 1873–1979. [Google Scholar] [CrossRef]
- Castellani, J.W.; Young, A.J. Human physiological responses to cold exposure: Acute responses and acclimatization to prolonged exposure. Auton. Neurosci. 2016, 196, 63–74. [Google Scholar] [CrossRef]
- van der Lans, A.A.; Hoeks, J.; Brans, B.; Vijgen, G.H.; Visser, M.G.; Vosselman, M.J.; Hansen, J.; Jörgensen, J.A.; Wu, J.; Mottaghy, F.M.; et al. Cold acclimation recruits human brown fat and increases nonshivering thermogenesis. J. Clin. Investig. 2013, 123, 3395–3403. [Google Scholar] [CrossRef]
- Yoneshiro, T.; Aita, S.; Matsushita, M.; Kayahara, T.; Kameya, T.; Kawai, Y.; Iwanaga, T.; Saito, M. Recruited brown adipose tissue as an antiobesity agent in humans. J. Clin. Investig. 2013, 123, 3404–3408. [Google Scholar] [CrossRef] [PubMed]
- Blondin, D.P.; Labbé, S.M.; Tingelstad, H.C.; Noll, C.; Kunach, M.; Phoenix, S.; Guérin, B.; Turcotte, E.E.; Carpentier, A.C.; Richard, D.; et al. Increased brown adipose tissue oxidative capacity in cold-acclimated humans. J. Clin. Endocrinol. Metab. 2014, 99, E438–E446. [Google Scholar] [CrossRef]
- Shephard, R.J. Adaptation to exercise in the cold. Sports Med. 1985, 2, 59–71. [Google Scholar] [CrossRef] [PubMed]
- Blondin, D.P.; Daoud, A.; Taylor, T.; Tingelstad, H.C.; Bézaire, V.; Richard, D.; Carpentier, A.C.; Taylor, A.W.; Harper, M.E.; Aguer, C.; et al. Four-week cold acclimation in adult humans shifts uncoupling thermogenesis from skeletal muscles to brown adipose tissue. J. Physiol. 2017, 595, 2099–2113. [Google Scholar] [CrossRef] [PubMed]
- Cypess, A.M.; Lehman, S.; Williams, G.; Tal, I.; Rodman, D.; Goldfine, A.B.; Kuo, F.C.; Palmer, E.L.; Tseng, Y.H.; Doria, A.; et al. Identification and importance of brown adipose tissue in adult humans. N. Engl. J. Med. 2009, 360, 1509–1517. [Google Scholar] [CrossRef]
- Mabhida, S.E.; Mashatola, L.; Kaur, M.; Sharma, J.R.; Apalata, T.; Muhamed, B.; Benjeddou, M.; Johnson, R. Hypertension in African Populations: Review and Computational Insights. Genes 2021, 12, 532. [Google Scholar] [CrossRef]
- Sousa, S.I.; Pires, J.C.; Martins, E.M.; Fortes, J.D.; Alvim-Ferraz, M.C.; Martins, F.G. Short-term effects of air pollution on respiratory morbidity at Rio de Janeiro—Part II: Health assessment. Environ. Int. 2012, 43, 1–5. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Segreti, A.; Celeski, M.; Guerra, E.; Crispino, S.P.; Vespasiano, F.; Buzzelli, L.; Fossati, C.; Papalia, R.; Pigozzi, F.; Grigioni, F. Effects of Environmental Conditions on Athlete’s Cardiovascular System. J. Clin. Med. 2024, 13, 4961. https://doi.org/10.3390/jcm13164961
Segreti A, Celeski M, Guerra E, Crispino SP, Vespasiano F, Buzzelli L, Fossati C, Papalia R, Pigozzi F, Grigioni F. Effects of Environmental Conditions on Athlete’s Cardiovascular System. Journal of Clinical Medicine. 2024; 13(16):4961. https://doi.org/10.3390/jcm13164961
Chicago/Turabian StyleSegreti, Andrea, Mihail Celeski, Emiliano Guerra, Simone Pasquale Crispino, Francesca Vespasiano, Lorenzo Buzzelli, Chiara Fossati, Rocco Papalia, Fabio Pigozzi, and Francesco Grigioni. 2024. "Effects of Environmental Conditions on Athlete’s Cardiovascular System" Journal of Clinical Medicine 13, no. 16: 4961. https://doi.org/10.3390/jcm13164961