
Expression of Endometrial Receptivity Markers throughout the Menstrual Cycle in Women with and without Uterine Adenomyosis

 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants and Sample Collection
2.2. Immunohistochemistry
2.3. Image Acquisition and Staining Quantification
2.4. Statistical Analysis
2.5. Scanning Electron Microscopy (SEM)
3. Results
3.1. Progesterone Receptor
3.2. Glycodelin
3.3. Leukemia Inhibitory Factor
3.4. Homeobox A10
3.5. Integrin Beta Chain Beta 3
3.6. Osteopontin
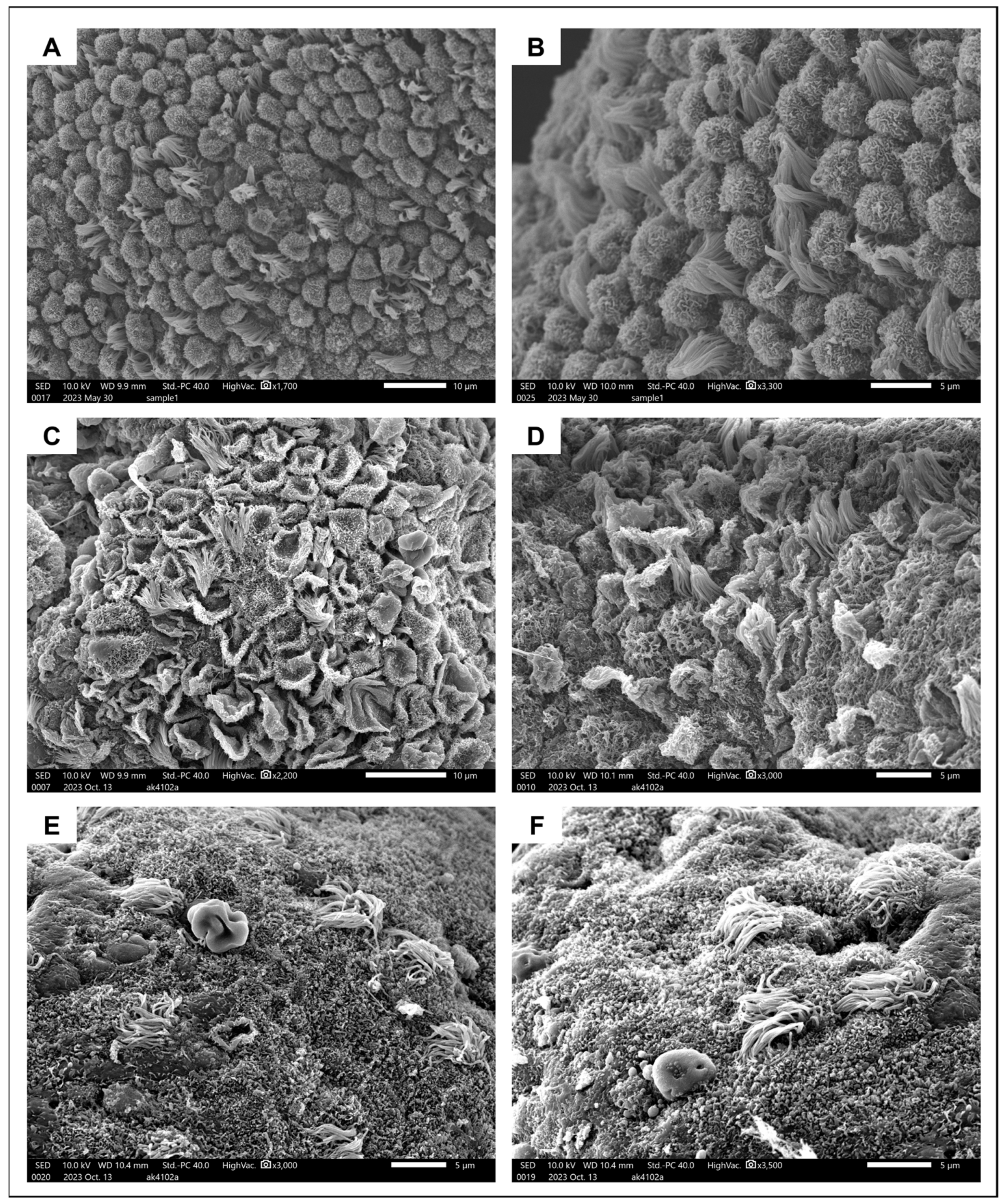
3.7. Pinopodes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lessey, B.A.; Young, S.L. What exactly is endometrial receptivity? Fertil. Steril. 2019, 111, 611–617. [Google Scholar] [CrossRef]
- Gellersen, B.; Brosens, J.J. Cyclic decidualization of the human endometrium in reproductive health and failure. Endocr. Rev. 2014, 35, 851–905. [Google Scholar] [CrossRef] [PubMed]
- Burton, G.J.; Watson, A.L.; Hempstock, J.; Skepper, J.N.; Jauniaux, E. Uterine glands provide histiotrophic nutrition for the human fetus during the first trimester of pregnancy. J. Clin. Endocrinol. Metab. 2002, 87, 2954–2959. [Google Scholar] [CrossRef] [PubMed]
- Noyes, R.W.; Hertig, A.T.; Rock, J. Dating the endometrial biopsy. Am. J. Obstet. Gynecol. 1975, 122, 262–263. [Google Scholar] [CrossRef]
- Vercellini, P.; Consonni, D.; Dridi, D.; Bracco, B.; Frattaruolo, M.P.; Somigliana, E. Uterine adenomyosis and in vitro fertilization outcome: A systematic review and meta-analysis. Hum. Reprod. 2014, 29, 964–977. [Google Scholar] [CrossRef]
- Nirgianakis, K.; Kalaitzopoulos, D.R.; Schwartz, A.S.K.; Spaanderman, M.; Kramer, B.W.; Mueller, M.D.; Mueller, M. Fertility, pregnancy and neonatal outcomes of patients with adenomyosis: A systematic review and meta-analysis. Reprod. Biomed. Online 2021, 42, 185–206. [Google Scholar] [CrossRef]
- Horton, J.; Sterrenburg, M.; Lane, S.; Maheshwari, A.; Li, T.C.; Cheong, Y. Reproductive, obstetric, and perinatal outcomes of women with adenomyosis and endometriosis: A systematic review and meta-analysis. Hum. Reprod. Update 2019, 25, 592–632. [Google Scholar] [CrossRef] [PubMed]
- Younes, G.; Tulandi, T. Effects of adenomyosis on in vitro fertilization treatment outcomes: A meta-analysis. Fertil. Steril. 2017, 108, 483–490.e3. [Google Scholar] [CrossRef]
- Szubert, M.; Koziróg, E.; Olszak, O.; Krygier-Kurz, K.; Kazmierczak, J.; Wilczynski, J. Adenomyosis and Infertility—Review of Medical and Surgical Approaches. Int. J. Environ. Res. Public Health 2021, 18, 1235. [Google Scholar] [CrossRef]
- Stratopoulou, C.A.; Donnez, J.; Dolmans, M.M. Conservative Management of Uterine Adenomyosis: Medical vs. Surgical Approach. J. Clin. Med. 2021, 10, 4878. [Google Scholar] [CrossRef] [PubMed]
- Stratopoulou, C.A.; Cussac, S.; d’Argent, M.; Donnez, J.; Dolmans, M.M. M2 macrophages enhance endometrial cell invasiveness by promoting collective cell migration in uterine adenomyosis. Reprod. Biomed. Online 2023, 46, 729–738. [Google Scholar] [CrossRef] [PubMed]
- Cha, J.; Sun, X.; Dey, S.K. Mechanisms of implantation: Strategies for successful pregnancy. Nat. Med. 2012, 18, 1754–1767. [Google Scholar] [CrossRef]
- Young, S.L.; Savaris, R.F.; Lessey, B.A.; Sharkey, A.M.; Balthazar, U.; Zaino, R.J.; Sherwin, R.A.; Fritz, M.A. Effect of randomized serum progesterone concentration on secretory endometrial histologic development and gene expression. Hum. Reprod. 2017, 32, 1903–1914. [Google Scholar] [CrossRef] [PubMed]
- d’Argent, M.; Stratopoulou, C.A.; Cussac, S.; Camboni, A.; Jadoul, P.; Donnez, J.; Dolmans, M.M. Are lower levels of apoptosis and autophagy behind adenomyotic lesion survival? Reprod. Biomed. Online 2023, 47, 103248. [Google Scholar] [CrossRef] [PubMed]
- Donnez, J.; Stratopoulou, C.A.; Dolmans, M.M. Uterine Adenomyosis: From Disease Pathogenesis to a New Medical Approach Using GnRH Antagonists. Int. J. Environ. Res. Public Health 2021, 18, 9941. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Jin, Z.; Liu, H.; Xu, C. Impaired decidualization of human endometrial stromal cells from women with adenomyosis†. Biol. Reprod. 2021, 104, 1034–1044. [Google Scholar] [CrossRef]
- Squatrito, M.; Vervier, J.; Bindels, J.; Bernet, L.; Blacher, S.; Nisolle, M.; Munaut, C. Impaired fertility in adenomyosis: A murine model reveals endometrial receptivity and progesterone resistance imbalances. Reproduction 2024, 167, e240019. [Google Scholar] [CrossRef]
- Uchida, H.; Maruyama, T.; Nishikawa-Uchida, S.; Miyazaki, K.; Masuda, H.; Yoshimura, Y. Glycodelin in reproduction. Reprod. Med. Biol. 2013, 12, 79–84. [Google Scholar] [CrossRef]
- Stewart, C.L.; Kaspar, P.; Brunet, L.J.; Bhatt, H.; Gadi, I.; Köntgen, F.; Abbondanzo, S.J. Blastocyst implantation depends on maternal expression of leukaemia inhibitory factor. Nature. 1992, 359, 76–79. [Google Scholar] [CrossRef]
- Vogiagis, D.; Marsh, M.M.; Fry, R.C.; Salamonsen, L.A. Leukaemia inhibitory factor in human endometrium throughout the menstrual cycle. J. Endocrinol. 1996, 148, 95–102. [Google Scholar] [CrossRef]
- Daftary, G.S.; Taylor, H.S. Pleiotropic effects of Hoxa10 on the functional development of peri-implantation endometrium. Mol. Reprod. Dev. 2004, 67, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Rarani, F.Z.; Borhani, F.; Rashidi, B. Endometrial pinopode biomarkers: Molecules and microRNAs. J. Cell Physiol. 2018, 233, 9145–9158. [Google Scholar] [CrossRef]
- Doherty, L.F.; Taylor, H.S. Leiomyoma-derived transforming growth factor-β impairs bone morphogenetic protein-2-mediated endometrial receptivity. Fertil. Steril. 2015, 103, 845–852. [Google Scholar] [CrossRef] [PubMed]
- Achache, H.; Revel, A. Endometrial receptivity markers, the journey to successful embryo implantation. Hum. Reprod. Update 2006, 12, 731–746. [Google Scholar] [CrossRef] [PubMed]
- Johnson, G.A.; Burghardt, R.C.; Bazer, F.W.; Spencer, T.E. Osteopontin: Roles in implantation and placentation. Biol. Reprod. 2003, 69, 1458–1471. [Google Scholar] [CrossRef] [PubMed]
- Koel, M.; Krjutškov, K.; Saare, M.; Samuel, K.; Lubenets, D.; Katayama, S.; Einarsdottir, E.; Vargas, E.; Sola-Leyva, A.; Lalitkumar, P.G.; et al. Human endometrial cell-type-specific RNA sequencing provides new insights into the embryo-endometrium interplay. Hum. Reprod. Open 2022, 2022, hoac043. [Google Scholar] [CrossRef]
- Lessey, B.A. Two pathways of progesterone action in the human endometrium: Implications for implantation and contraception. Steroids 2003, 68, 809–815. [Google Scholar] [CrossRef]
- Nikas, G.; Psychoyos, A. Uterine pinopodes in peri-implantation human endometrium. Clinical relevance. Ann. N. Y. Acad. Sci. 1997, 816, 129–142. [Google Scholar] [CrossRef]
- Jin, X.Y.; Zhao, L.J.; Luo, D.H.; Liu, L.; Dai, Y.D.; Hu, X.X.; Wang, Y.Y.; Lin, X.; Hong, F.; Li, T.C.; et al. Pinopode score around the time of implantation is predictive of successful implantation following frozen embryo transfer in hormone replacement cycles. Hum. Reprod. 2017, 32, 2394–2403. [Google Scholar] [CrossRef]
- Qiong, Z.; Jie, H.; Yonggang, W.; Bin, X.; Jing, Z.; Yanping, L. Clinical validation of pinopode as a marker of endometrial receptivity: A randomized controlled trial. Fertil. Steril. 2017, 108, 513–517.e2. [Google Scholar] [CrossRef]
- Brosens, J.J.; Pijnenborg, R.; Brosens, I.A. The myometrial junctional zone spiral arteries in normal and abnormal pregnancies: A review of the literature. Am. J. Obstet. Gynecol. 2002, 187, 1416–1423. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.; Zhang, D.; Zhao, S.; Zhang, H.; Sun, Y.; Yan, L. A Preliminary Study on the Correlation Between Age and Endometrial Receptivity. Pharmgenomics Pers. Med. 2023, 16, 425–432. [Google Scholar] [CrossRef]
- Zhao, J.; Huang, B.; Li, N.; Wang, X.; Xu, B.; Li, Y. Relationship between advanced maternal age and decline of endometrial receptivity: A systematic review and meta-analysis. Aging 2023, 15, 2460–2472. [Google Scholar] [CrossRef] [PubMed]
- Soares, S.R.; Troncoso, C.; Bosch, E.; Serra, V.; Simón, C.; Remohí, J.; Pellicer, A. Age and uterine receptiveness: Predicting the outcome of oocyte donation cycles. J. Clin. Endocrinol. Metab. 2005, 90, 4399–4404. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Healthy | Adenomyosis | p-Value |
|---|---|---|---|
| Age (mean ± SD) | 36.52 ± 6.125 Range = 21–43 | 39.96 ± 4.703 Range = 24–45 | * 0.0286 |
| Parity (mean ± SD) | 1.2 ± 1.4 Range = 0–4 | 2 ± 1.3 Range = 0–4 | * 0.03 |
| Menstrual phase | |||
| Proliferative | 10 | 10 | |
| Secretory | 12 | 12 | |
| Menstrual | 4 | 4 | |
| Menorrhagia (%) | 37.5 | 65.38 | * 0.0486 |
| Dysmenorrhea (%) | 16.67 | 42.31 | * 0.0481 |
| Leiomyoma (%) | 45.83 | 38.46 | 0.5977 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stratopoulou, C.A.; El Grari, I.; Camboni, A.; Donnez, J.; Dolmans, M.-M. Expression of Endometrial Receptivity Markers throughout the Menstrual Cycle in Women with and without Uterine Adenomyosis. J. Clin. Med. 2024, 13, 5016. https://doi.org/10.3390/jcm13175016
Stratopoulou CA, El Grari I, Camboni A, Donnez J, Dolmans M-M. Expression of Endometrial Receptivity Markers throughout the Menstrual Cycle in Women with and without Uterine Adenomyosis. Journal of Clinical Medicine. 2024; 13(17):5016. https://doi.org/10.3390/jcm13175016
Chicago/Turabian StyleStratopoulou, Christina Anna, Ines El Grari, Alessandra Camboni, Jacques Donnez, and Marie-Madeleine Dolmans. 2024. "Expression of Endometrial Receptivity Markers throughout the Menstrual Cycle in Women with and without Uterine Adenomyosis" Journal of Clinical Medicine 13, no. 17: 5016. https://doi.org/10.3390/jcm13175016
APA StyleStratopoulou, C. A., El Grari, I., Camboni, A., Donnez, J., & Dolmans, M.-M. (2024). Expression of Endometrial Receptivity Markers throughout the Menstrual Cycle in Women with and without Uterine Adenomyosis. Journal of Clinical Medicine, 13(17), 5016. https://doi.org/10.3390/jcm13175016