
A Pilot Study on the Relationship between Obstructive Sleep Apnoea–Hypopnea Syndrome, Neurodevelopment, and Ricketts’ Cephalometry
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Data Collection and Analysis
2.3. Data Collection for Ricketts’ VERT Index and Related Measures
3. Results
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Álvarez, C. Alteraciones del sueño en trastornos del neurodesarrollo. Rev. Méd. Clín. Las Condes 2022, 33, 490–501. [Google Scholar] [CrossRef]
- Dionne-Dostie, E.; Paquette, N.; Lassonde, M.; Gallagher, A. Multisensory Integration and Child Neurodevelopment. Brain Sci. 2015, 5, 32–57. [Google Scholar] [CrossRef]
- Asociación Americana de Psiquiatría. In Guía de Consulta de los Criterios Diagnósticos del DSM-5; Asociación Americana de Psiquiatría: Arlington, VA, USA, 2013.
- Blackmer, A.B.; Feinstein, J.A. Management of Sleep Disorders in Children with Neurodevelopmental Disorders: A Review. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2016, 36, 84–98. [Google Scholar] [CrossRef]
- Beebe, D.W.; Gozal, D. Obstructive sleep apnea and the prefrontal cortex: Towards a comprehensive model linking nocturnal upper airway obstruction to daytime cognitive and behavioral deficits. J. Sleep. Res. 2002, 11, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Capistrano, A.; Cordeiro, A.; Filho, L.C.; Almeida, V.C.; Martinez, S.; Almeida-Pedrin, R.R.D. Facial morphology and obstructive sleep apnea. Dent. Press. J. Orthod. 2015, 20, 60–67. [Google Scholar] [CrossRef] [PubMed]
- De Luca Canto, G.; Singh, V.; Major, M.P.; Witmans, M.; El-Hakim, H.; Major, P.W.; Flores-Mir, C. Diagnostic capability of questionnaires and clinical examinations to assess sleep-disordered breathing in children: A systematic review and meta-analysis. J. Am. Dent. Assoc. 2014, 145, 165–178. [Google Scholar] [CrossRef]
- Larramona Carrera, H.; Cortell Aznar, I. Polisomnografía nocturna y métodos alternativos para el estudio de los trastornos respiratorios del sueño. Protoc. Diagn. Pediatr. 2017, 1, 67–84. [Google Scholar]
- Bidart-Santander, C.; Díaz-Muñoz, A.; Dentista, C.; asistente, P.; de Odontología, F. Obstructive sleep apnea: Role of dentomaxillary orthopedics Apnea obstructiva del sueño: Rol de la ortopedia dentomaxilar. Oral 2018, 18, 1463–1466. [Google Scholar]
- Baldassari, C.M.; Mitchell, R.B.; Schubert, C.; Rudnick, E.F. Pediatric obstructive sleep apnea and quality of life: A meta-analysis. Otolaryngol.—Head Neck Surg. 2008, 138, 265–273. [Google Scholar] [CrossRef]
- Patel, A.P.; Meghji, S.; Phillips, J.S. Accuracy of clinical scoring tools for the diagnosis of pediatric obstructive sleep apnea. Laryngoscope 2020, 130, 1034–1043. [Google Scholar] [CrossRef]
- Kheirandish-Gozal, L.; Sahib, A.K.; Macey, P.M.; Philby, M.F.; Gozal, D.; Kumar, R. Regional Brain Tissue Integrity in Pediatric Obstructive Sleep Apnea. Neurosci. Lett. 2018, 682, 118–123. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, L.M.; Tauman, R.; Gozal, D. Sleep pressure correlates of cognitive and behavioral morbidity in snoring children. Sleep 2004, 27, 279–282. [Google Scholar] [CrossRef] [PubMed]
- Tauman, R.; O’Brien, L.M.; Holbrook, C.R.; Gozal, D. Sleep Pressure Score: A New Index of Sleep Disruption in Snoring Children. Sleep 2004, 27, 274–278. [Google Scholar] [CrossRef]
- Cerda-Peralta, B.; Schulz-Rosales, R.; López-Garrido, J.; Romo-Ormazabal, F. Parámetros cefalométricos para determinar biotipo facial en adultos chilenos. Rev. Clín. Periodoncia Implantol. Rehabil. Oral. 2019, 12, 8–11. [Google Scholar] [CrossRef]
- Ricketts, R.M. A foundation for cephalometric communication. Am. J. Orthod. 1960, 46, 330–357. [Google Scholar] [CrossRef]
- Ricketts, R.M. Cephalometric synthesis. An exercise in stating objectives and planning treatment with tracings of the head roentgenogram. Am. J. Orthod. 1960, 46, 647–673. [Google Scholar] [CrossRef]
- Alomri, R.M.; Kennedy, G.A.; Wali, S.O.; Alhejaili, F.; Robinson, S.R. Association between nocturnal activity of the sympathetic nervous system and cognitive dysfunction in obstructive sleep apnoea. Sci. Rep. 2021, 11, 11990. [Google Scholar] [CrossRef]
- Lord, C.; Rutter, M.; Goode, S.; Heemsbergen, J.; Jordan, H.; Mawhood, L.; Schopler, E. Autism diagnostic observation schedule: A standardized observation of communicative and social behavior. J. Autism Dev. Disord. 1989, 19, 185–212. [Google Scholar] [CrossRef]
- Lyall, K.; Croen, L.; Daniels, J.; Fallin, M.D.; Ladd-Acosta, C.; Lee, B.K.; Park, B.Y.; Snyder, N.W.; Schendel, D.; Volk, H.; et al. The Changing Epidemiology of Autism Spectrum Disorders. Ann. Rev. Public. Health 2017, 38, 81–102. [Google Scholar] [CrossRef]
- Tomás Vila, M.; Miralles Torres, A.; Beseler Soto, B. Versión española del Pediatric Sleep Questionnaire. Un instrumento útil en la investigación de los trastornos del sueño en la infancia. Análisis de su fiabilidad. An. Pediatr. 2007, 66, 121–128. [Google Scholar] [CrossRef]
- Alvial-Vergara, L.; Linker-Navarro, K.; Vergara-Núñez, C.; Alvial-Vergara, L.; Linker-Navarro, K.; Vergara-Núñez, C. Posición Natural de Cabeza y su relación con el Plano de Frankfurt en cefalometría ortodóncica. Int. J. Interdiscip. Dent. 2021, 14, 218–221. [Google Scholar] [CrossRef]
- Leitao, P.; Nanda, R.S. Relationship of natural head position to craniofacial morphology. Am. J. Orthod. Dentofac. Orthop. 2000, 117, 406–417. [Google Scholar] [CrossRef] [PubMed]
- Naini, F.B. The Frankfort plane and head positioning in facial aesthetic analysis—The perpetuation of a myth. JAMA Facial Plast. Surg. 2013, 15, 333–334. [Google Scholar] [CrossRef] [PubMed]
- Bozzini, M.F.; Di Francesco, R.C.; Soster, L.A. Clinical and anatomical characteristics associated with obstructive sleep apnea severity in children. Clinics 2022, 77, 100131. [Google Scholar] [CrossRef]
- Di Francesco, R.; Monteiro, R.; de Melo Paulo, M.L.; Buranello, F.; Imamura, R. Craniofacial morphology and sleep apnea in children with obstructed upper airways: Differences between genders. Sleep Med. 2012, 13, 616–620. [Google Scholar] [CrossRef]
- Galeotti, A.; Festa, P.; Viarani, V.; Pavone, M.; Sitzia, E.; Piga, S.; Cutrera, R.; De Vincentiis, G.C.; D’Anto, V. Correlation between cephalometric variables and obstructive sleep apnoea severity in children. Eur. J. Paediatr. Dent. 2019, 20, 43–47. [Google Scholar] [CrossRef]
- Liu, Y.; Zhao, T.; Ngan, P.; Qin, D.; Hua, F.; He, H. The dental and craniofacial characteristics among children with obstructive sleep apnoea: A systematic review and meta-analysis. Eur. J. Orthod. 2023, 45, 346–355. [Google Scholar] [CrossRef]
- Hasanin, M.; ElNaghy, R.; Olson, D.; Al-Jewair, T. Three-dimensional analysis of upper airway and craniofacial morphology in orthodontic adolescents with Attention Deficit Hyperactivity Disorder (ADHD): A comparative retrospective study. Int. Orthod. 2021, 19, 622–632. [Google Scholar] [CrossRef]
- Wang, W.; Wang, Y.; Wang, X. Cephalometry study of craniofacial growth in mixed dentition with OSAHS children. Lin. Chung Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 2012, 26, 1127–1129. [Google Scholar]
- Deng, J.; Gao, X. A case—Control study of craniofacial features of children with obstructed sleep apnea. Sleep Breath. 2012, 16, 1219–1227. [Google Scholar] [CrossRef]
- Feng, G.; Gong, X.; Yu, M.; Huang, X.; Gao, X. Differences of Craniofacial Characteristics in Oral Breathing and Pediatric Obstructive Sleep Apnea. J. Craniofacial Surg. 2021, 32, 564–568. [Google Scholar] [CrossRef] [PubMed]
- Lowe, A.A.; Santamaria, J.D.; Fleetham, J.A.; Price, C. Facial morphology and obstructive sleep apnea. Am. J. Orthod. Dentofac. Orthop. 1986, 90, 484–491. [Google Scholar] [CrossRef] [PubMed]
- Agha, B.; Johal, A. Facial phenotype in obstructive sleep apnea—Hypopnea syndrome: A systematic review and meta-analysis. J. Sleep Res. 2017, 26, 122–131. [Google Scholar] [CrossRef] [PubMed]
- Neelapu, B.C.; Kharbanda, O.P.; Sardana, H.K.; Balachandran, R.; Sardana, V.; Kapoor, P.; Gupta, A.; Vasamsetti, S. Craniofacial and upper airway morphology in adult obstructive sleep apnea patients: A systematic review and meta-analysis of cephalometric studies. Sleep Med. Rev. 2017, 31, 79–90. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Severe DCP | DCP | Soft DCP | MCP | BCP | Severe BCP |
|---|---|---|---|---|---|
| −2 | −1 | −0.5 | 0 | +0.5 | +1 |
| OSAHS | N | Mean | Median | SD | Minimum | Maximum |
|---|---|---|---|---|---|---|
| Yes | 19 | 8.73 | 9 | 2.79 | 5 | 14 |
| No | 25 | 10.04 | 10 | 2.26 | 5 | 14 |
| Neurodevelopmental Disorder | |||
|---|---|---|---|
| OSAHS | Yes | No | Total |
| Yes | 19 | 0 | 19 |
| No | 3 | 22 | 25 |
| Total | 22 | 22 | 44 |
| Cephalometric Measurements | Shapiro–Wilk | |||||||
|---|---|---|---|---|---|---|---|---|
| OSAHS | N | Mean | SD | Minimum | Maximum | W | p | |
| Mandibular plane (Relative) | Yes | 19 | 5.16 | 1.76 | 1.92 | 7.79 | 0.94 | 0.319 |
| No | 25 | 2.81 | 1.91 | 0.06 | 7.42 | 0.95 | 0.238 | |
| Facial depth (Relative) | Yes | 19 | 4.55 | 3.00 | 0.35 | 9.95 | 0.93 | 0.162 |
| No | 25 | 2.61 | 2.06 | 0.08 | 8.94 | 0.85 | 0.001 | |
| Mandibular arch (Relative) | Yes | 19 | 9.49 | 5.15 | 3.35 | 22.68 | 0.90 | 0.059 |
| No | 25 | 8.24 | 5.56 | 0.75 | 20.64 | 0.92 | 0.064 | |
| Facial axis (Relative) | Yes | 19 | 3.59 | 3.11 | 0.06 | 8.58 | 0.88 | 0.019 |
| No | 25 | 4.51 | 3.08 | 0.69 | 12.70 | 0.93 | 0.103 | |
| Lower facial height (Relative) | Yes | 19 | 5.04 | 3.49 | 1.17 | 13.12 | 0.89 | 0.036 |
| No | 25 | 4.07 | 2.77 | 0.02 | 9.96 | 0.96 | 0.396 | |
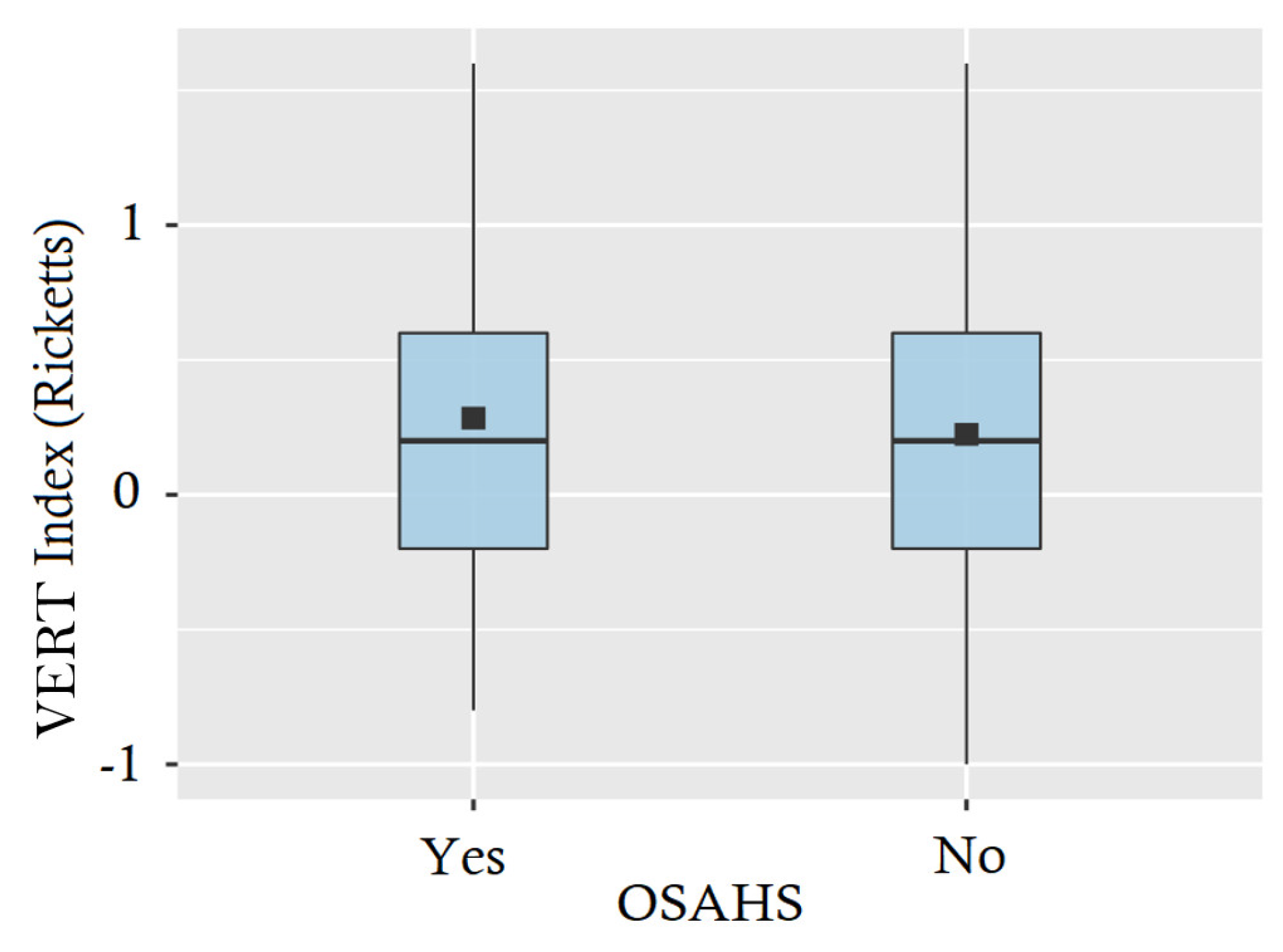
| VERT index | Yes | 19 | 0.28 | 0.63 | −0.80 | 1.60 | 0.96 | 0.632 |
| No | 25 | 0.22 | 0.60 | −1.00 | 1.60 | 0.98 | 0.920 | |
| AGE (Years) | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 |
|---|---|---|---|---|---|---|---|---|
| Facial Axis | 90° | 90° | 90° | 90° | 90° | 90° | 90° | 90° |
| Facial Depth | 87° | 87.3° | 87.6° | 87.9° | 88.2° | 88.5° | 88.8° | 89.1° |
| Mandibular Plane | 26° | 25.7° | 25.4° | 25.1° | 24.8° | 24.5° | 24.2° | 23.9° |
| Facial Height | 47° | 47° | 47° | 47° | 47° | 47° | 47° | 47° |
| Mandibular Arch | 26° | 26.5° | 27° | 27.5° | 28° | 28.5° | 29° | 29.5° |
| 95% Confidence Interval | ||||||
|---|---|---|---|---|---|---|
| Cephalometric Measurements | Statistical | d f | p-Value | Mean Difference | Lower | Upper |
| Facial depth (Relative) | 2.42 | 30.34 | 0.011 | 1.94 | 0.58 | ∞ |
| Mandibular plane (Relative) | 4.24 | 40.40 | <0.001 | 2.35 | 1.42 | ∞ |
| Mandibular arch (Relative) | 0.77 | 40.30 | 0.222 | 1.25 | −1.48 | ∞ |
| Lower facial height (Relative) | 0.99 | 33.62 | 0.164 | 0.97 | −0.68 | ∞ |
| VERT index | 0.32 | 42.00 | 0.749 | 0.06 | −0.32 | 0.44 |
| Facial axis (Relative) | −0.98 | 42.00 | 0.166 | −0.92 | −∞ | 0.66 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Robayna, T.I.G.; Martínez, C.P.-A.; Gandía, J.M.; Martínez, M.D.A.; Pérez, Á.S.; Cascales, R.F. A Pilot Study on the Relationship between Obstructive Sleep Apnoea–Hypopnea Syndrome, Neurodevelopment, and Ricketts’ Cephalometry. J. Clin. Med. 2024, 13, 5274. https://doi.org/10.3390/jcm13175274
Robayna TIG, Martínez CP-A, Gandía JM, Martínez MDA, Pérez ÁS, Cascales RF. A Pilot Study on the Relationship between Obstructive Sleep Apnoea–Hypopnea Syndrome, Neurodevelopment, and Ricketts’ Cephalometry. Journal of Clinical Medicine. 2024; 13(17):5274. https://doi.org/10.3390/jcm13175274
Chicago/Turabian StyleRobayna, Teresa I. González, Carlos Pérez-Albacete Martínez, Jesús M. Gandía, Mª Dolores Austro Martínez, Ángela Sempere Pérez, and Raúl Ferrando Cascales. 2024. "A Pilot Study on the Relationship between Obstructive Sleep Apnoea–Hypopnea Syndrome, Neurodevelopment, and Ricketts’ Cephalometry" Journal of Clinical Medicine 13, no. 17: 5274. https://doi.org/10.3390/jcm13175274