
Efficacy and Accuracy of Ultrasound Guided Injections in the Treatment of Cervical Facet Joint Syndrome: A Systematic Review

 , , , , , ,
, , , , , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources, Search Strategy and Study Selection
2.2. Data Extraction and Outcome Measures
2.3. Quality Assessment
2.4. Risk of Bias Assessment
3. Results
3.1. Identification of Studies
3.2. Characteristics of the Included Studies
3.3. Anaesthetics and/or Corticosteroid Used in the Trials
3.4. Efficacy, Accuracy, Performance Time and Pain Relief of US-Guided Cervical Facet Injections
3.5. Assessment of Methodology and Quality of the Studies
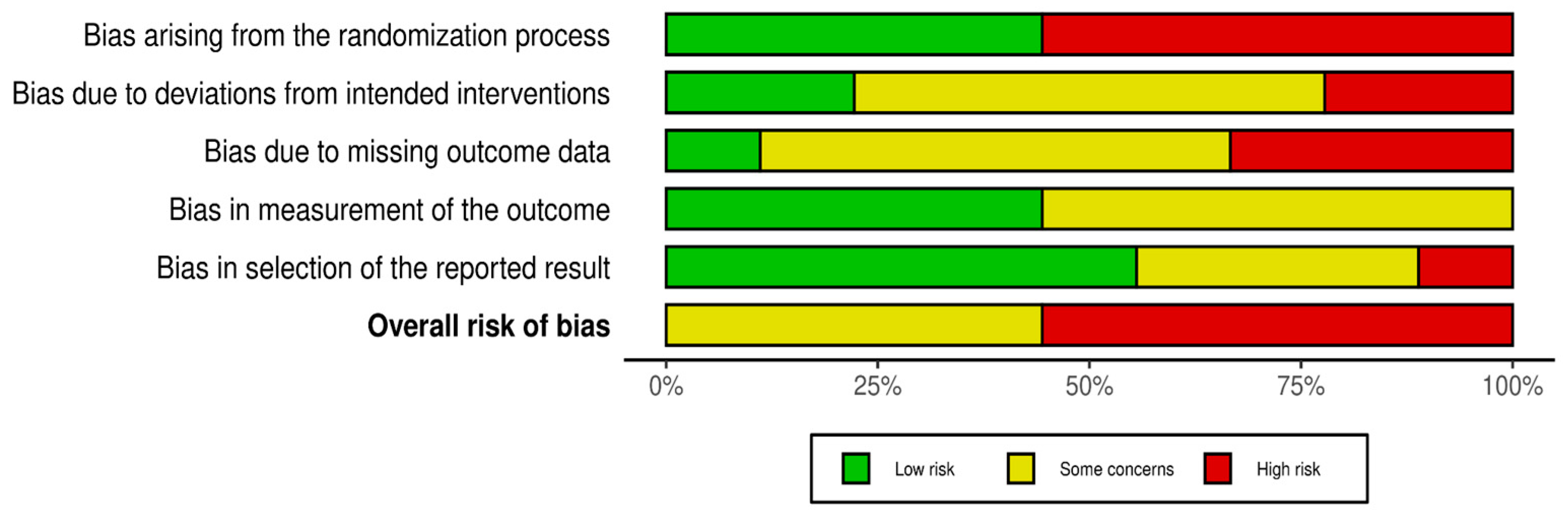
3.6. Evaluation of Risk of Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hoy, D.G.; Protani, M.; De, R.; Buchbinder, R. The epidemiology of neck pain. Best Pract. Res. Clin. Rheumatol. 2010, 24, 783–792. [Google Scholar] [CrossRef] [PubMed]
- Kazeminasab, S.; Nejadghaderi, S.A.; Amiri, P.; Pourfathi, H.; Araj-Khodaei, M.; Sullman, M.J.M.; Kolahi, A.-A.; Safiri, S. Neck pain: Global epidemiology, trends and risk factors. BMC Musculoskelet. Disord. 2022, 23, 26. [Google Scholar] [CrossRef] [PubMed]
- Moreno, B.; Barbosa, J. Ultrasound-Guided Procedures in the Cervical Spine. Cureus 2021, 13, e20361. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.-M.; Cross, M.; Elliott, J.M.; Culbreth, G.T.; Haile, L.M.; Steinmetz, J.D.; Hagins, H.; Kopec, J.A.; Brooks, P.M.; Woolf, A.D.; et al. Global, regional, and national burden of neck pain, 1990–2020, and projections to 2050: A systematic analysis of the Global Burden of Disease Study 2021. Lancet Rheumatol. 2024, 6, e142–e155. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, S.; Shu, P. Global burden of neck pain in 204 countries from 1990–2019. Arch. Med. Sci. 2023, 19, 1811–1821. [Google Scholar] [CrossRef]
- Manchikanti, L.; Singh, V.; Rivera, J.; Pampati, V. Prevalence of cervical facet joint pain in chronic neck pain. Pain Physician 2002, 5, 243–249. [Google Scholar] [CrossRef]
- Perolat, R.; Kastler, A.; Nicot, B.; Pellat, J.-M.; Tahon, F.; Attye, A.; Heck, O.; Boubagra, K.; Grand, S.; Krainik, A. Facet joint syndrome: From diagnosis to interventional management. Insights Imaging 2018, 9, 773–789. [Google Scholar] [CrossRef]
- Yoo, Y.-M.; Kim, K.-H. Facet joint disorders: From diagnosis to treatment. Korean J. Pain 2024, 37, 3–12. [Google Scholar] [CrossRef]
- Büsken, F.; Lataster, A.; Herrler, A. The innervation of the cervical facet joints—An anatomical and histological approach. Clin. Anat. 2022, 35, 780–788. [Google Scholar] [CrossRef]
- Yin, W.; Bogduk, N. The Nature of Neck Pain in a Private Pain Clinic in the United States. Pain Med. 2008, 9, 196–203. [Google Scholar] [CrossRef]
- Farì, G.; De Sire, A.; Fallea, C.; Albano, M.; Grossi, G.; Bettoni, E.; Di Paolo, S.; Agostini, F.; Bernetti, A.; Puntillo, F.; et al. Efficacy of Radiofrequency as Therapy and Diagnostic Support in the Management of Musculoskeletal Pain: A Systematic Review and Meta-Analysis. Diagnostics 2022, 12, 600. [Google Scholar] [CrossRef] [PubMed]
- Tabassum, H.; Mariam, M.; Gondal, K.S. Comparison of muscle energy technique and facet joint mobilisation in the patient with chronic neck pain: A randomized controlled trial. J. Pak. Med. Assoc. 2023, 74, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Park, S.-C.; Kim, K.-H. Effect of adding cervical facet joint injections in a multimodal treatment program for long-standing cervical myofascial pain syndrome with referral pain patterns of cervical facet joint syndrome. J. Anesth. 2012, 26, 738–745. [Google Scholar] [CrossRef] [PubMed]
- Bernetti, A.; La Russa, R.; De Sire, A.; Agostini, F.; De Simone, S.; Farì, G.; Lacasella, G.V.; Santilli, G.; De Trane, S.; Karaboue, M.; et al. Cervical Spine Manipulations: Role of Diagnostic Procedures, Effectiveness, and Safety from a Rehabilitation and Forensic Medicine Perspective: A Systematic Review. Diagnostics 2022, 12, 1056. [Google Scholar] [CrossRef]
- Manchikanti, L.; Kaye, A.D.; Soin, A.; Albers, S.L.; Beall, D.; Latchaw, R.; Sanapati, M.R.; Shah, S.; Atluri, S.; Abd-Elsayed, A.; et al. Comprehensive Evidence-Based Guidelines for Facet Joint Interventions in the Management of Chronic Spinal Pain: American Society of Interventional Pain Physicians (ASIPP) Guidelines Facet Joint Interventions 2020 Guidelines. Pain Physician 2020, 23, S1–S127. [Google Scholar] [CrossRef]
- Hurley, R.W.; Adams, M.C.B.; Barad, M.; Bhaskar, A.; Bhatia, A.; Chadwick, A.; Deer, T.R.; Hah, J.; Hooten, W.M.; Kissoon, N.R.; et al. Consensus practice guidelines on interventions for cervical spine (facet) joint pain from a multispecialty international working group. Reg. Anesth. Pain Med. 2022, 47, 3–59. [Google Scholar] [CrossRef]
- Hurdle, M.-F.B. Ultrasound-Guided Spinal Procedures for Pain. Phys. Med. Rehabil. Clin. N. Am. 2016, 27, 673–686. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Olivo, S.A.; Macedo, L.G.; Gadotti, I.C.; Fuentes, J.; Stanton, T.; Magee, D.J. Scales to Assess the Quality of Randomized Controlled Trials: A Systematic Review. Phys. Ther. 2008, 88, 156–175. [Google Scholar] [CrossRef]
- Mohsina, S.; Gurushankari, B.; Niranjan, R.; Sureshkumar, S.; Sreenath, G.; Kate, V. Assessment of the quality of randomized controlled trials in surgery using Jadad score: Where do we stand? J. Postgrad. Med. 2022, 68, 207–212. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Monticone, M.; Cedraschi, C.; Ambrosini, E.; Rocca, B.; Fiorentini, R.; Restelli, M.; Gianola, S.; Ferrante, S.; Zanoli, G.A.; Moja, L. Cognitive-Behavioural Treatment for Subacute and Chronic Neck Pain-Monticone, M-2015|Cochrane Library. Available online: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD010664.pub2 (accessed on 21 August 2024).
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef]
- Bodor, M.; Murthy, N.; Uribe, Y. Ultrasound-guided cervical facet joint injections. Spine J. 2022, 22, 983–992. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.P.; Strassels, S.A.; Kurihara, C.; Forsythe, A.; Buckenmaier, C.C.; McLean, B.; Riedy, G.; Seltzer, S. Randomized study assessing the accuracy of cervical facet joint nerve (medial branch) blocks using different injectate volumes. Anesthesiology 2010, 112, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Finlayson, R.J.; Etheridge, J.-P.B.; Vieira, L.; Gupta, G.; Tran, D.Q.H. A randomized comparison between ultrasound- and fluoroscopy-guided third occipital nerve block. Reg. Anesth. Pain Med. 2013, 38, 212–217. [Google Scholar] [CrossRef]
- Finlayson, R.J.; Etheridge, J.-P.B.; Tiyaprasertkul, W.; Nelems, B.; Tran, D.Q.H. A randomized comparison between ultrasound- and fluoroscopy-guided c7 medial branch block. Reg. Anesth. Pain Med. 2015, 40, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Obernauer, J.; Galiano, K.; Gruber, H.; Bale, R.; Obwegeser, A.A.; Schatzer, R.; Loizides, A. Ultrasound-guided versus Computed Tomography-controlled facet joint injections in the middle and lower cervical spine: A prospective randomized clinical trial. Med. Ultrason. 2013, 15, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Park, K.D.; Lim, D.-J.; Lee, W.Y.; Ahn, J.; Park, Y. Ultrasound versus fluoroscopy-guided cervical medial branch block for the treatment of chronic cervical facet joint pain: A retrospective comparative study. Skelet. Radiol. 2017, 46, 81–91. [Google Scholar] [CrossRef]
- Pasuhirunnikorn, P.; Tanasansomboon, T.; Singhatanadgige, W.; Yingsakmongkol, W.; Chalermkitpanit, P. Comparative Outcome of Lidocaine Versus Bupivacaine for Cervical Medial Branch Block in Chronic Cervical Facet Arthropathy: A Randomized Double-Blind Study. World Neurosurg. 2023, 175, e662–e668. [Google Scholar] [CrossRef]
- Smith, A.D.; Jull, G.; Schneider, G.; Frizzell, B.; Hooper, R.A.; Sterling, M. A comparison of physical and psychological features of responders and non-responders to cervical facet blocks in chronic whiplash. BMC Musculoskelet. Disord. 2013, 14, 313. [Google Scholar] [CrossRef]
- Farì, G.; Mancini, R.; Dell’Anna, L.; Ricci, V.; Della Tommasa, S.; Bianchi, F.P.; Ladisa, I.; De Serio, C.; Fiore, S.; Donati, D.; et al. Medial or Lateral, That Is the Question: A Retrospective Study to Compare Two Injection Techniques in the Treatment of Knee Osteoarthritis Pain with Hyaluronic Acid. J. Clin. Med. 2024, 13, 1141. [Google Scholar] [CrossRef] [PubMed]
- Ricci, V.; Chang, K.-V.; Farì, G.; Özçakar, L. Imaging, Guidance, and Follow-up for Recalcitrant Trigger Finger: Physiatrists’ Greed for Ultrasonography. Am. J. Phys. Med. Rehabil. 2024, 103, e18–e19. [Google Scholar] [CrossRef] [PubMed]
- Boswell, M.V.; Manchikanti, L.; Kaye, A.D.; Bakshi, S.; Gharibo, C.G.; Gupta, S.; Jha, S.S.; Nampiaparampil, D.E.; Simopoulos, T.T.; Hirsch, J.A. A Best-Evidence Systematic Appraisal of the Diagnostic Accuracy and Utility of Facet (Zygapophysial) Joint Injections in Chronic Spinal Pain. Pain Physician 2015, 18, E497–E533. [Google Scholar] [CrossRef]
- Won, H.-S.; Yang, M.; Kim, Y.-D. Facet joint injections for management of low back pain: A clinically focused review. Anesth Pain Med. 2020, 15, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Peh, W. Image-guided facet joint injection. Biomed. Imaging Interv. J. 2011, 7, e4. [Google Scholar] [CrossRef]
- Li, J.; Szabova, A. Ultrasound-Guided Nerve Blocks in the Head and Neck for Chronic Pain Management: The Anatomy, Sonoanatomy, and Procedure. Pain Physician 2021, 24, 533–548. [Google Scholar]
- Ehsanian, R.; Kennedy, D.J.; Schneider, B. Cervical Ultrasound Utilization in Selective Cervical Nerve Root Injection for the Treatment of Cervical Radicular Pain: A Review. Curr. Phys. Med. Rehabil. Rep. 2019, 7, 386–396. [Google Scholar] [CrossRef]
- Oliveira, M.; Navarro, M.; Costa, E.; Kremer, D.; Pinheiro, R.; Freitas, V.; Modesto, I.; Macedo, E.; Ferreira, J.; Andrade, D.; et al. Potential risk assessment: A model for quality evaluation in fluoroscopy-guided interventional procedures. Radiat. Prot. Dosim. 2024, 200, 693–699. [Google Scholar] [CrossRef]
- Sveva, V.; Farì, G.; Fai, A.; Savina, A.; Viva, M.G.; Agostini, F.; Ranieri, M.; Megna, M.; Mangone, M.; Paoloni, M.; et al. Safety and Efficacy of Ultrasound-Guided Perineural Hydrodissection as a Minimally Invasive Treatment in Carpal Tunnel Syndrome: A Systematic Review. J. Pers. Med. 2024, 14, 154. [Google Scholar] [CrossRef]
- Galiano, K.; Obwegeser, A.A.; Bodner, G.; Freund, M.C.; Gruber, H.; Maurer, H.; Schatzer, R.; Fiegele, T.; Ploner, F. Ultrasound-guided facet joint injections in the middle to lower cervical spine: A CT-controlled sonoanatomic study. Clin. J. Pain 2006, 22, 538–543. [Google Scholar] [CrossRef]
- Freire, V.; Grabs, D.; Lepage-Saucier, M.; Moser, T.P. Ultrasound-Guided Cervical Facet Joint Injections: A Viable Substitution for Fluoroscopy-Guided Injections? J. Ultrasound Med. 2016, 35, 1253–1258. [Google Scholar] [CrossRef]
- Siegenthaler, A.; Schliessbach, J.; Curatolo, M.; Eichenberger, U. Ultrasound anatomy of the nerves supplying the cervical zygapophyseal joints: An exploratory study. Reg. Anesth. Pain Med. 2011, 36, 606–610. [Google Scholar] [CrossRef] [PubMed]
- Ye, L.; Wen, C.; Liu, H. Ultrasound-guided versus low dose computed tomography scanning guidance for lumbar facet joint injections: Same accuracy and efficiency. BMC Anesthesiol. 2018, 18, 160. [Google Scholar] [CrossRef] [PubMed]
- Biglia, A.; Morandi, V.; Zanframundo, G.; Donati, D.; Maggiore, F.; Vita, F.; Sammarchi, L.; Pagani, C.; Cavagna, L.; Galletti, S.; et al. Adhesive capsulitis after COVID-19 vaccine injection: A peculiar case treated with combined bursa distention and glenohumeral capsular hydrodilatation. J. Ultrasound 2023, 26, 909–911. [Google Scholar] [CrossRef] [PubMed]
- Donati, D.; Vita, F.; Tedeschi, R.; Galletti, S.; Biglia, A.; Gistri, T.; Arcuri, P.; Origlio, F.; Castagnini, F.; Faldini, C.; et al. Ultrasound-Guided Infiltrative Treatment Associated with Early Rehabilitation in Adhesive Capsulitis Developed in Post-COVID-19 Syndrome. Medicina 2023, 59, 1211. [Google Scholar] [CrossRef]
- Narouze, S.N.; Provenzano, D.; Peng, P.; Eichenberger, U.; Lee, S.C.; Nicholls, B.; Moriggl, B. The American Society of Regional Anesthesia and Pain Medicine, the European Society of Regional Anaesthesia and Pain Therapy, and the Asian Australasian Federation of Pain Societies Joint Committee recommendations for education and training in ultrasound-guided interventional pain procedures. Reg. Anesth. Pain Med. 2012, 37, 657–664. [Google Scholar] [CrossRef]
- Kwon, S.Y.; Kim, J.-W.; Cho, M.J.; Al-Sinan, A.H.; Han, Y.-J.; Kim, Y.H. The efficacy of cervical spine phantoms for improving resident proficiency in performing ultrasound-guided cervical medial branch block: A prospective, randomized, comparative study. Medicine 2018, 97, e13765. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Authors | Sample | Research Design | Collected Data and Outcomes | Results |
|---|---|---|---|---|
| Bodor et al. (2022) [24] | 60 facet joints in 36 patients with chronic cervical facet joint syndrome (CFJS). | Type of Study: Cohort study. Objective: To determine the accuracy of ultrasound-guided cervical facet joint injections using a lateral technique and to describe the technique. Contrast dye was used to confirm it be intra-articular. Drugs: A mixture of 0.3 to 0.5 mL ropivacaine 0.5% plus 5 to 10 mg of triamcinolone acetonide 40 mg/mL was injected. Anatomical targets: facet joints C2-C3; C3-C4; C4-C5; C5-C6. | Data collected included: type of contrast pattern, Age, Sex, facet joint level, body mass index (BMI) and ponderal index (PI). | The accuracy of ultrasound-guided cervical facet joint injections using the lateral technique ranged from 92% to 98%. |
| Cohen et al. (2010) [25] | 24 patients with axial (neck arm) cervical pain received cervical medial branch block (CMBB). | Type of Study: Randomized double-blinded trial, 50% of the patients in each group were sub-allocated to receive the blocks in the prone position and the other 50% through a lateral approach. Objective: The objective of this study was to evaluate the accuracy of medial branch blocks by using different injectate volumes. Participants then underwent computed tomography (CT) of the cervical spine to evaluate accuracy. Drugs: A mixture of either 0.5 or 0.25 mL of bupivacaine mixed with contrast was used. Anatomical targets: cervical medial branch. | Data collected: Age, sex, duration of pain, block level, obesity, n° patients on opioid therapy. Outcomes: baseline median Numerical Rating Scale (NRS) score-interquartile range (IQR), baseline median NDRI score (IQR), postblock median NRS score (IQR). | 16 instances of aberrant spread were observed in 9 patients receiving blocks using 0.5 mL versus 7 occurrences in 6 patients in the 0.25 mL group. Foraminal spread occurred in 5 instances using 0.5 mL and in 2 cases with 0.25 mL. No significant difference in any outcome measure was observed between the prone and lateral positions. The two techniques were found to be equally effective in reducing pain. |
| Finlayson et al. (2013) [26] | 40 patients with CFJS | Type of Study: Randomized observer-blinded trial. Patients undergoing third occipital nerve block (TONB) were randomized to FL or US guidance. Objective: Comparison between 2 different guidance modalities (FL, US). Drugs: A mixture of local anesthetic and radiographic contrast was injected in both groups. Anatomical targets: Third Occipital nerve (TON). | Data collected: Age, sex, Body Mass Index (BMI) Outcomes: pre-block NRS score, performance time, success rate, pain levels before and after block, area of sensory hypoesthesia, quality of the block (assessed by electrical perceptual threshold), procedure-related complications. | FL and US guidance provide similar success rates for TONB. US is associated with greater efficiency (decreased performance time, fewer needle passes). |
| Finlayson et al. (2015) [27] | 50 patients with CFJS referral patterns elicited from C7 medial branch stimulation | Type of Study: Randomized observer-blinded trial. Patients undergoing C7 CMBB randomized to FL or US guidance. Objective: US, using a biplanar imaging technique, could provide a shorter performance time than conventional FL for C7 cervical medial branch blocks. Drugs: A 0.6-mL mixture of local anesthetic and radiographic contrast was injected in both groups. Anatomical targets: C7 CMBB. | Data collected: Age, sex, BMI. Outcomes: pre-block NRS score, performance time, success rate, pain levels before and after block, incidence of aberrant spread and procedure-related complications. | US-guided using a biplanar approach provides a similar success rate to FL for C7 cervical medial branch blocks. US is associated with a higher efficiency (decreased performance time and fewer needle passes) in the comparison with FL-guided technique. |
| Obernauer et al. (2013) [28] | 40 adult patients with chronic neck pain. | Type of Study: Prospective randomized trial. Patients were assigned to one of two groups by chance; one group underwent US-guided infiltrations (US group), the other group underwent CT guided injections (CT group). Objective: To evaluate accuracy, time-saving, radiation doses and pain relief of US-guided facet joint injections versus CT-controlled interventions in the cervical spine. Drugs: 1 mL mixture of betamethasone (4 mg/mL); and Bupivacaine hydrochloride (0.25%, 2.5 mg/mL). Anatomical targets: facet joint of the middle and lower cervical spine(C2-C3; C7-D1) for CMBB. | Data collected: Gender, Age, BMI. Outcomes: Visual Analogue Scale (VAS), accuracy, time to final needle placement, dose of radiation. | US-guided intra-articular injections show the same therapeutic effect as CT-guided intra-articular injections and result in a significant reduction in procedure duration without any radiation exposure. |
| Park et al. (2016) [29] | 186 patients with chronic CFJS. | Type of Study: retrospective comparative study, 68 patients received US-guided and 58 patients received FL-guided CMBB. Objective: To compare the mid-term effects and advantages of the US-guided versus the FL-guided CMBBs for chronic CJFS assessing pain relief, functional improvement, and injection efficiency. Drugs: 1 mL of a mixture of 1% lidocaine (0.5 mL) and dexamethasone (5 mg/mL; 0.5 mL). Anatomical targets: facet joints of the middle and lower cervical spine (C2-C3; C7-D1) for CMBB. | Data collected: Sex, Age, BMI, injection method, number of injections, analgesic use, pain duration. Outcomes: Neck Disability Index (NDI), Visual Numeric Scale (VNS) score. | Both NDI and VNS scores showed improvements at 1, 3, and 6 months after the last injection in both groups, with no significant differences between the groups. US-guided procedure was associated with shorter administration duration and fewer needle passes. |
| Park et al. (2012) [13] | 400 patients with long-standing cervical myofascial pain referred to CFJS over a period of 6 months. | Type of Study: Randomized controlled clinical trial. Patients were divided into two groups of 200 each: group 1 and group N (non-injection). Group 1 also received therapeutic CFJ injections at bilateral C5/C6 and C6/C7 levels after double-blind controlled diagnostic blocks. Objective: To investigate the effects of therapeutic CFJ injections on patients with myofascial pain referred to CFJS. Drugs: local anesthetic blocks using 0.3 mL of 1% lidocaine and 0.25% bupivacaine; then injection using a mixture of 0.5 mL of 1% lidocaine, 5 mg of triamcinolone and 187.5 IU of hyaluronidase. Anatomical targets: CFJ bilateral C5/C6 and C6/C7. |
Data collected: Comorbidities, presence of tension-type headache, Age, Sex, Treatment duration, symptom-free period. Outcomes: Cervical range of motion (CROM), NRS. | During the follow-up, group 1 exhibited a greater CROM, a greater mean NRS pain reduction, and a lower incidence of combined tension-type headache than group N. The treatment cycle for younger patients in group 1 was shorter and they experienced a longer period without symptoms. |
| Pasuhirunnikornt al. (2023) [30] | 62 patients with chronic CFJS. |
Type of study: Prospective, double-blinded study. Objective: To compare the clinical effect of the CMBB using lidocaine versus bupivacaine. Drugs: For CMBB, either 2% lidocaine or 0.5% bupivacaine with a volume of 0.5–1 mL per level. Anatomical targets: Cervical medial branches. | Data collected: Age, gender, referred pain area, BMI, side (right/left), procedure levels, complications. Outcomes: pain intensity (NRS), NDI, duration of pain reduction by at least 50% (in months). | Clinical benefits were achieved using both lidocaine and bupivacaine in the CMBB. No significant difference in the duration of 50% pain relief, but lidocaine yielded better performance in pain reduction in both early and later follow-up after the intervention. No differences in terms of safety and accuracy between the two drugs were reported. Lidocaine could be considered the best local anesthetic due to its better performance. |
| Smith et al. (2013) [31] | 90 patients with chronic whiplash-associated disorders (WAD) |
Type of study: A cross-sectional comparison study with 3 groups: 58 who responded to cervical facet block procedures (WAD_R); 32 who did not respond (WAD_NR); 30 Healthy Controls (HC)s. Objective: to compare the clinical manifestations after treatment with facet blocks (FB), intra-articular blocks (IAB) or comparative medial branch blocks (MBB), in two WAD groups and the healthy control group. Drugs: IAB: injection of 0.5 cc of local anaesthetic (1% Bupivicaine) and 0.5 cc of corticosteroid. MBB: 0.5 cc of 2% Lidocaine. Anatomical targets: Cervical facet joint, Cervical medial branch. | Data collected and Outcomes: quantitative sensory tests (pressure; thermal pain thresholds; brachial plexus provocation test); nociceptive flexion reflex (NFR); motor function (CROM); activity of the superficial neck flexors during the cranio-cervical flexion test (CCFT). Self-reported measures were gained from the following questionnaires: neuropathic pain (s-LANSS); psychological distress (General Health Questionnaire-28), post-traumatic stress (PDS) and pain catastrophization (PCS). | Both chronic WAD responders and non-responders to facet block procedures exhibit a shared pattern of sensory disturbance, motor dysfunction, and psychological distress. Higher levels of pain catastrophizing and increased medication intake were found in the WAD_NR group. |
| Study | Was the Treatment Randomly Allocated? | Was the Randomization Procedure Described and Appropriate? | Was There a Description of Withdrawals and Dropouts? | Was There a Clear Description of the Inclusion/Exclusion Criteria? | Were the Methods of Statistical Analysis Described? | Jadad Score (0–5) |
|---|---|---|---|---|---|---|
| Bodor et al. (2022) [24] | No | No | Yes | Yes | No | 2 |
| Cohen et al. (2010) [25] | Yes | Yes | Yes | Yes | Yes | 5 |
| Finlayson et al. (2013) [26] | Yes | Yes | Yes | No | Yes | 4 |
| Finlayson et al. (2015) [27] | Yes | Yes | No | No | Yes | 3 |
| Obernauer et al. (2013) [28] | No | No | Yes | Yes | Yes | 3 |
| Park et al. (2012) [13] | No | Yes | Yes | No | Yes | 3 |
| Park et al. (2016) [29] | No | No | Yes | Yes | Yes | 3 |
| Pasuhirunnikorn et al. (2023) [30] | Yes | Yes | Yes | Yes | Yes | 5 |
| Smith et al. (2013) [31] | No | No | Yes | Yes | Yes | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viva, M.G.; Sveva, V.; Ruggiero, M.; Fai, A.; Savina, A.; Perrone, R.; Donati, D.; Tedeschi, R.; Monticone, M.; Farì, G.; et al. Efficacy and Accuracy of Ultrasound Guided Injections in the Treatment of Cervical Facet Joint Syndrome: A Systematic Review. J. Clin. Med. 2024, 13, 5290. https://doi.org/10.3390/jcm13175290
Viva MG, Sveva V, Ruggiero M, Fai A, Savina A, Perrone R, Donati D, Tedeschi R, Monticone M, Farì G, et al. Efficacy and Accuracy of Ultrasound Guided Injections in the Treatment of Cervical Facet Joint Syndrome: A Systematic Review. Journal of Clinical Medicine. 2024; 13(17):5290. https://doi.org/10.3390/jcm13175290
Chicago/Turabian StyleViva, Mattia Giuseppe, Valerio Sveva, Marco Ruggiero, Annatonia Fai, Alessio Savina, Riccardo Perrone, Danilo Donati, Roberto Tedeschi, Marco Monticone, Giacomo Farì, and et al. 2024. "Efficacy and Accuracy of Ultrasound Guided Injections in the Treatment of Cervical Facet Joint Syndrome: A Systematic Review" Journal of Clinical Medicine 13, no. 17: 5290. https://doi.org/10.3390/jcm13175290
APA StyleViva, M. G., Sveva, V., Ruggiero, M., Fai, A., Savina, A., Perrone, R., Donati, D., Tedeschi, R., Monticone, M., Farì, G., & Bernetti, A. (2024). Efficacy and Accuracy of Ultrasound Guided Injections in the Treatment of Cervical Facet Joint Syndrome: A Systematic Review. Journal of Clinical Medicine, 13(17), 5290. https://doi.org/10.3390/jcm13175290