
The Effectiveness and Validity of Inspiratory Muscle Training in the Training Process of Disabled Swimmers

Abstract
:1. Introduction
2. Materials and Methods
- −
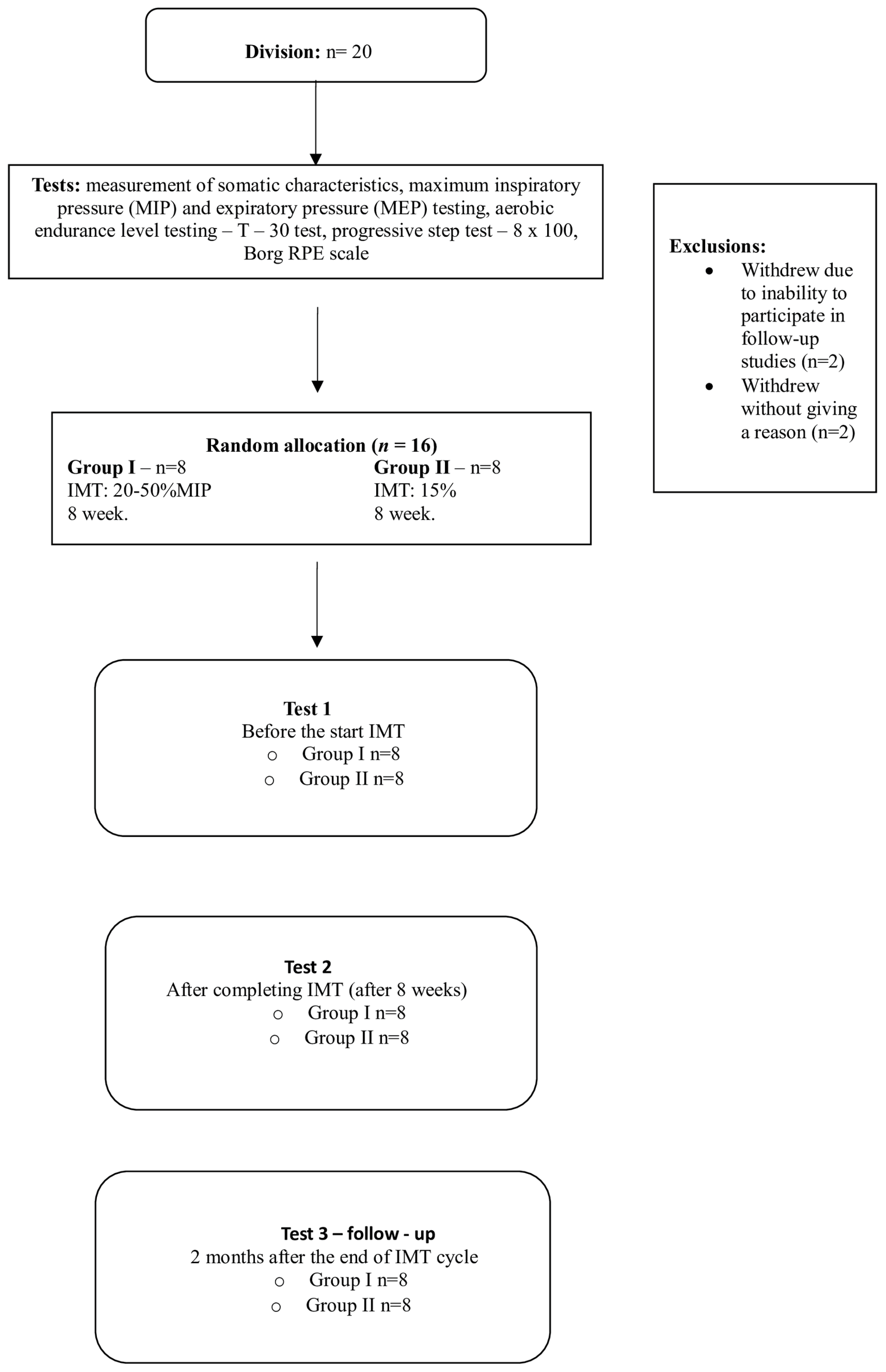
- Group I (IMT group)→Competitors training according to the standard swimming training model and additionally supplemented with medium-intensity inspiratory muscle training at a load level of 50% of the MIP.
- −
- Group II (sham-IMT group)→Competitors training according to the standard swimming training model and additionally supplemented with low-intensity inspiratory muscle training at a load level of 15% of the MIP, in accordance with the literature indicating the need to use a minimum load in the control group, meeting the time requirements of the training used in both groups [17].
2.1. Swimming Test
- −
- Level I—swimming 3 times the distance of 100 m in the starting time, i.e., approximately 77% in relation to the best result obtained in the competition in a given training period. Exercise at this level can be treated as a warm-up for the stimulation of individual functional mechanisms of the body for further work.
- −
- Level II—swimming 2 sections of 100 m with an intensity of approximately 83% in relation to the best result.
- −
- Level III—swimming 100 m at a speed of 88% of the maximum speed.
- −
- Level IV—swimming 100 m at a speed of 93% of the maximum speed.
- −
- Level V—swimming 100 m at the maximum intensity.
2.2. Intervention
2.3. Sports Training Program
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
- Inspiratory muscle training at 50% MIP significantly reduced the fatigue response to exercise as assessed by the Borg scale.
- Inspiratory muscle training a higher-intensity training (50% MIP) level significantly improved the training level of the swimmers tested, which was associated with an increase in swimming distance. The results obtained confirm the validity of inspiratory muscle training among athletes with disabilities. The introduction of higher-intensity inspiratory muscle training significantly reduced the level of blood lactate formation in the progressive test, which authenticates the validity of an additional supplementation of the preparation of athletes with this type of training.
- Higher-intensity training (50% MIP) significantly reduced the heart rate in the 8 × 100 progressive test at 88% and 93% of the maximum speed, thus improving the aerobic endurance of the athletes.
- The use of inspiratory muscle training at 50% MIP effectively improved the training level and physiological parameters of the swimmers’ effort. This indicates the need to include this type of training in the standard of competitive preparation of athletes with disabilities.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Welch, J.F.; Archiza, B.; Guenette, J.A.; West, C.R.; Sheel, A.W. Sex differences in diaphragmatic fatigue: The cardiovascular response to inspiratory resistance. J. Physiol. 2018, 596, 4017–4032. [Google Scholar] [CrossRef]
- Taylor, B.J.; Romer, L.M. Effect of expiratory muscle fatigue on exercise tolerance and locomotor muscle fatigue in healthy humans. J. Appl. Physiol. 2008, 104, 1442–1451. [Google Scholar] [CrossRef] [PubMed]
- Romer, L.M.; Lovering, A.T.; Haverkamp, H.C.; Pegelow, D.F.; Dempsey, J.A. Effect of inspiratory muscle work on peripheral fatigue of locomotor muscles in healthy humans. J. Physiol. 2006, 571, 425–439. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.D.; Norris, S.R. Assessment of physiological capacities of elite athletes and respiratory limitations exercise performance. Paediatr. Respir. Rev. 2009, 10, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Leahy, M.G.; Summers, M.N.; Peters, C.M.; Molgat-Seon, Y.; Geary, C.M.; Sheel, A.W. The mechanics of breathing during swimming. Med. Sci. Sports Exerc. 2009, 51, 1467–1476. [Google Scholar] [CrossRef] [PubMed]
- Cavaggioni, L.; Trecroci, A.; Formenti, D.; Hogarth, L.; Tosin, M.; Alberti, G. Seasonal changes in breathing pattern, trunk stabilization, and muscular power in paralympic swimmers. Adapt. Phys. Act. Q. APAQ 2021, 38, 215–231. [Google Scholar] [CrossRef]
- Lomax, M.E.; McConnell, A.K. Inspiratory muscle fatigue in swimmers after a single 200 m swim. J. Sports Sci. 2003, 21, 659–664. [Google Scholar] [CrossRef]
- Kowalski, T.; Granda, D.; Klusiewicz, K. Practical application of respiratory muscle training in endurance sports. Strength. Cond. J. 2024, 10, 1519. [Google Scholar] [CrossRef]
- Romer, L.M.; Polkey, M.I. Exercise induced respiratory muscle fatigue: Implications for performance. J. Appl. Physiol. 2008, 104, 879–888. [Google Scholar] [CrossRef]
- Oueslatia, F.; Booneb, J.; Ahmaidia, S. Respiratory muscle endurance, oxygen saturation index in vastuslateralisnband performance during heavy exercise. Respir. Physiol. Neurobiol. 2016, 227, 41–47. [Google Scholar] [CrossRef]
- Sales, A.T.N.; Fregonezi, G.A.F.; Ramsook, E.H.; Guenette, J.A.; Lima, I.N.D.F.; Reid, W.D. Respiratory muscle endurance after training in athletes and nonathletes: A systematic review and meta-analysis. Phys. Ther. Sport 2016, 17, 76–86. [Google Scholar] [CrossRef]
- Hellyer, N.J.; Folsom, I.A.; Gaz, D.V.; Kakuk, A.C.; Mack, J.L.; Ver Mulm, J.A. Respiratory muscle activity during simultaneous stationary cycling and inspiratory muscle training. J. Strength Cond. Res. 2015, 29, 3517–3522. [Google Scholar] [CrossRef]
- Segizbaeva, M.O.; Timofeev, N.N.; Donina, Z.A.; Kur’yanovich, E.N.; Aleksandrova, N.P. Effects of inspiratory muscle training on resistance to fatigue of respiratory muscles during exhaustive exercise. Adv. Exp. Med. Biol. 2015, 840, 35–43. [Google Scholar]
- Goosey-Tolfrey, V.; Foden, E.; PeTorret, C. Effects of inspiratory muscle training on respiratory function and repetitive sprint performance in wheelchair basketball players. Br. J. Sports Med. 2010, 44, 665–668. [Google Scholar] [CrossRef] [PubMed]
- Feitosa, W.G.; Correia, R.A.; Barbosa, T.M.; Castro, F.A.S. Performance of disabled swimmers in protocols or tests and competitions: A systematic review and meta-analysis. Sports Biomech. 2022, 21, 255–277. [Google Scholar] [CrossRef] [PubMed]
- Lyn, G.; Litchke, L.G.; Russian, C.J.; Lloyd, L.K.; Schmidt, E.A.; Price, L.; Walker, J.L. Effects of respiratory resistance training with a concurrent flow device on wheelchair athletes. J. Spinal Cord. Med. 2008, 31, 65–71. [Google Scholar]
- Kim, K.T.; Lee, S.; Oh, E.-S. Athletes with disabilities in the paralympic games: A framing analysis of television news. Manag. Sport Leis. 2017, 22, 255–275. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D.; CONSORT Group. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, C.B.B.; Hartz, C.S.; Santos, S.D.S.; Moreno, M.A. Effects of inspiratory muscle training with progressive loading on respiratory muscle function and sports performance in high-performance wheelchair basketball athletes: A randomized clinical trial. Int. J. Sports Physiol. Perform. 2020, 15, 238–242. [Google Scholar] [CrossRef]
- Nunes Junior, A.O.; Donzeli, M.A.; Novais Shimano, S.G.; de Oliveira, N.M.L.; Ruas, G.; Bertoncello, D. Effects of high-intensity inspiratory muscle training in rugby players. Rev. Bras. Med. Esporte 2018, 24, 216–219. [Google Scholar] [CrossRef]
- Akinci, B.; Emirza Cilbir, C.; Kocygit, A.; Kuran Aslan, G. Respiratory muscle training in para-athletes: A systematic review on the training protocols and effects on reported outcomes. J. Sport. Rehabil. 2024, 33, 387–395. [Google Scholar] [CrossRef]
- Hogarth, L.; Burkett, B.; Van de Vliet, P.; Payton, C. Maximal fully tethered swim performance in para swimmers with physical impairment. Int. J. Sports Physiol. 2020, 15, 816–824. [Google Scholar] [CrossRef] [PubMed]
- Dingley, A.; Pyne, D.; Burkett, B. Dry-land bilateral hand-force production and swimming performance in paralympic swimmers. Int. J. Sports Med. 2024, 35, 949–953. [Google Scholar]
- Chang, Y.C.; Chang, H.Y.; Ho, C.C.; Lee, P.F.; Chou, Y.C.; Tsai, M.W. Effects of 4-week inspiratory muscle training on sport performance in college 800-meter track runners. Medicina 2021, 57, 72. [Google Scholar] [CrossRef] [PubMed]
- American Thoracic Society/European Respiratory Society: ATS/ERS Statement on respiratory muscle testing. Am. J. Respir. Crit. Care Med. 2002, 166, 518–524. [CrossRef]
- Quanjer, P.H.; Tammeling, G.J.; Cotes, J.E.; Pedersen, O.F.; Peslin, R.; Yernault, J.C. Lung volumes and forced ventilatory flows. Eur. Respir. J. 1993, 6, 5–40. [Google Scholar] [CrossRef]
- Degens, P.; Merget, R. Reference values for spirometry of the European Coal and Steel Community: Time for change. Eur. Respir. J. 2008, 31, 687–688. [Google Scholar] [CrossRef]
- Deminice, R.; Papoti, M.; Zagatto, A.M.; do Prado Júnior, M.V. Validity of 30 minutes test (T-30) in aerobic capacity, stroke parameters and aerobic performance determination of trained swimmers. Rev. Bras. Med. Esporte 2007, 13, 173–176. [Google Scholar]
- Olbrecht, J.; Madsen, O.; Mader, A.; Liesen, H.; Hollman, W. Relationship between swimming velocity and lactate concentration during continuous and intermittent training exercises. Int. J. Sports Med. 2001, 6, 74–77. [Google Scholar] [CrossRef]
- Maglischo, E. Swimming Even Faster; Mayfield Publishing Company: Mountain View, CA, USA, 1993. [Google Scholar]
- Almeida, T.A.F.; Pessôa Filho, D.M.; Espada, M.C.; Reis, J.F.; Sancassani, A.; Massini, D.A.; Santos, F.J.; Alves, F.B. Physiological responses during high-intensity interval training in young swimmers. Front. Physiol. 2021, 1, 662029. [Google Scholar] [CrossRef] [PubMed]
- Vašíčková, J.; Neumannová, K.; Svozil, Z. The effect of respiratory muscle training on fin-wwimmers’ performance. J. Sports Sci. Med. 2017, 16, 521–526. [Google Scholar] [PubMed]
- Nepomuceno Júniora, B.R.V.; Gómezb, T.B.; Neto, M.G. Use of Powerbreathe® in inspiratory muscle training for athletes: Systematic review. Fisioter. Mov. 2016, 29, 821–830. [Google Scholar] [CrossRef]
- Romer, L.M.; McConnell, A.K.; Jones, D.A. Effects of inspiratory muscle training upon recovery time during high-intensity, repetitive sprint activity. Int. J. Sports Med. 2002, 23, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Ewards, A.M.; Cooke, C.B. Oxygen uptake kinetics and maximal aerobic power are unaffected by inspiratory muscle training in healthy subjects where time to exhaustion is extended. Eur. J. Appl. Physiol. 2004, 93, 139–144. [Google Scholar] [CrossRef]
- Galvan, C.C.; Cataneo, A.J. Effect of respiratory muscle training on pulmonary function in preoperative preparation of tobacco smokers. Acta Cir. Bras. 2007, 22, 98–104. [Google Scholar] [CrossRef]
- Alwohayeb, N.S.; Alenazi, B.A.; Albuainain, F.A.; Alrayes, M.M. A comparison between two types of resistive inspiratory muscle training devices in normal subjects in regard to pulmonary functions. Int. J. Phys. Med. Rehabil. 2018, 6, 449. [Google Scholar] [CrossRef]
- Patsaki, I.; Kouvarakos, A.; Vasileiadis, I.; Koumantakis, G.A.; Ischaki, E.; Grammatopoulou, E.; Kotanidou, A.; Magira, E.E. Low-Medium and High-Intensity Inspiratory Muscle Training in Critically Ill Patients: A Systematic Review and Meta-Analysis. Medicine 2024, 60, 869. [Google Scholar] [CrossRef] [PubMed]
- Lorca-Santiago, J.; Jiménez, S.L.; Pareja-Galeano, H.; Lorenzo, A. Inspiratory muscle training in intermittent sports modalities: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 4448. [Google Scholar] [CrossRef]
- Illi, S.K.; Held, U.; Frank, I.; Spengler, C.M. Effect of respiratory muscle training on exercise performance in healthy individuals: A systematic review and meta-analysis. Sports Med. 2012, 42, 707–724. [Google Scholar] [CrossRef]
- Cavalcante Silva, R.L.; Hall, E.; Maior, A.S. Inspiratory muscle training improves performance of a repeated sprints ability test in professional soccer players. J. Bodyw. Mov. Ther. 2019, 23, 452–455. [Google Scholar] [CrossRef]
- Guy, J.H.; Edwards, A.M.; Deakin, G.B. Inspiratory muscle training improves exercise tolerance in recreational soccer players without concomitant gain in soccer-specific fitness. J. Strength Cond. Res. 2014, 28, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Ohya, T.; Kusanagi, K.; Koizumi, J.; Ando, R.; Katayama, K.; Suzuki, Y. Effect of moderate- or high-intensity inspiratory muscle strength training on maximal inspiratory mouth pressure and swimming performance in highly trained competitive swimmers. Int. J. Sports Physiol. Perform. 2022, 17, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Brown, P.I.; Sharpe, G.R.; Johnson, M.A. Inspiratory muscle training abolishes the blood lactate increase associated with volitional hyperpnoea superimposed on exercise and accelerates lactate and oxygen uptake kinetics at the onset of exercise. Eur. J. Appl. Physiol. 2012, 112, 2117–2129. [Google Scholar] [CrossRef] [PubMed]
- Witt, J.D.; Guenette, J.A.; Rupert, J.L.; McKenzie, D.C.; Sheel, A.W. Inspiratory muscle training attenuates the human respiratory muscle metaboreflex. J. Physiol. 2007, 584 Pt 3, 1019–1028. [Google Scholar] [CrossRef]
- Cipriano, G.F.; Cipriano, G., Jr.; Santos, F.V.; Güntzel Chiappa, A.M.; Pires, L.; Cahalin, L.P.; Chiappa, G.R. Current insights of inspiratory muscle training on the cardiovascular system: A systematic review with meta-analysis. Integr. Blood Press. Control. 2019, 12, 1–11. [Google Scholar] [CrossRef]
- de Abreu, R.M.; Rehder-Santos, P.; Minatel, V.; Dos Santos, G.L.; Catai, A.M. Effects of inspiratory muscle training on cardiovascular autonomic control: A systematic review. Auton. Neurosci. 2017, 208, 29–35. [Google Scholar] [CrossRef]

{kind=link}
| Variable | Group I n = 8 | Group II n = 8 | t/χ2 | p |
|---|---|---|---|---|
| Age [years] | 16.75 ± 2.66 | 17.88 ± 4.39 | −0.62 | 0.5452 |
| Body mass [kg] | 61.75 ± 11.18 | 61.38 ± 13.71 | 0.06 | 0.9530 |
| Body height [m] | 1.77 ± 0.09 | 1.69 ± 0.09 | 1.62 | 0.1278 |
| BMI [kg/m2] | 19.68 ± 1.76 | 21.24 ± 3.39 | −1.16 | 0.2666 |
| Sports experience [years] | 8 ± 3 | 7 ± 2 | 1.08 | 0.2036 |
| Sports achievements | World Cup medallist, senior men’s MP medallist—n = 7 finalist of Tokyo IP, 5th place at Senior World Championships in 400 m freestyle—n = 1 participant of Tokio IP—n = 1 | World Cup medallist, senior men’s MP medallist—n = 7 participant in Tokyo IP, World Cup medallist—n = 1 Participant of Senior Men’s European Championships in 202—n = 1 Participant of Tokio IP—n = 1 | - | - |
| Swim class | S10—n = 5 S9—n = 3 SB10—n = 4 SB9—n = 2 SB8—n = 2 SM10—n = 5 SM9—n = 3 | S10—n = 1 S9—n = 4 S8—n = 1 S7—n = 2 SB9—n = 3 SB8—n = 3 SB6—n = 2 SM10—n = 1 SM9—n = 4 SM8—n = 1 SM7—n = 2 | 1901 | - |
| Type of dysfunction (disability) |
|
| 3279 | - |
| Training Week | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| Training load (cm H2O) | 20% MIP | 30% MIP | 30% MIP | 40% MIP | 40% MIP | 50% MIP | 50% MIP | 50% MIP |
| Training session [seriesxnumber of breaths] | 2 × 30 | 2 × 30 | 2 × 30 | 2 × 30 | 2 × 30 | 2 × 30 | 2 × 30 | 2 × 30 |
| Training Week | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| Training load (cm H2O) | 15% MIP | |||||||
| Training session [seriesnumber of breaths] | 1 × 60 | |||||||
| Variables | Test I | Test II | Test III | |||
|---|---|---|---|---|---|---|
| Group I | Group II | Group I | Group II | Group I | Group II | |
| MIP [kPa] | 10.38 ± 2.49 | 9.86 ± 3.17 | 14.21 ± 2.97 | 9.76 ± 2.93 | 12.77 ± 3.16 | 9.61 ± 2.85 |
| MIP [%] | 96.37 ± 21.31 | 96.35 ± 18.24 | 132.03 ± 25.24 | 94.95 ± 14.94 | 118.96 ± 25.92 | 93.95 ± 14.29 |
| MEP [kPa] | 10.87 ± 2.35 | 9.25 ± 3.84 | 13.06 ± 2.57 | 9.43 ± 4.38 | 12.58 ± 3.80 | 9.26 ± 4.21 |
| MEP [%] | 80.70 ± 13.92 | 72.52 ± 23.55 | 98.60 ± 23.43 | 73.76 ± 27.02 | 94.55 ± 24.70 | 72.66 ± 25.68 |
| Variables | Tests I–II in Group I | Tests I–II in Group II | Tests I–III in Group I | Tests I–III in Group II | Tests II–III in Group I | Tests II–III in Group II | Tests II–III in Group II | Test II in Group I and Test II in Group II | Test III in Group I and Test III in Group II |
|---|---|---|---|---|---|---|---|---|---|
| MIP [kPa] | 0.0000 | 0.8559 | 0.0001 | 0.6413 | 0.0121 | 0.7757 | 0.7258 | 0.0076 | 0.0460 |
| MIP [%] | 0.0000 | 0.7832 | 0.0001 | 0.6381 | 0.0152 | 0.8447 | 0.9985 | 0.0018 | 0.0244 |
| MEP [kPa] | 0.0081 | 0.8105 | 0.0340 | 0.9846 | 0.5388 | 0.8255 | 0.3816 | 0.0598 | 0.0825 |
| MEP [%] | 0.0061 | 0.8380 | 0.0295 | 0.9808 | 0.5067 | 0.8568 | 0.4930 | 0.0466 | 0.0765 |
| Variables | Test I | Test II | Test III | |||
|---|---|---|---|---|---|---|
| Group I | Group II | Group I | Group II | Group I | Group II | |
| T-30 [m] | 1902.50 ± 187.45 | 1643.75 ± 461.33 | 1960.00 ± 207.83 | 1635.63 ± 399.12 | 1940.00 ± 204.28 | 1632.50 ± 401.17 |
| Borg scale—RPE scale | 12.88 ± 0.99 | 13.13 ± 1.13 | 11.88 ± 1.13 | 13.50 ± 1.2 | 12.00 ± 0.93 | 13.88 ± 1.13 |
| La [mmol] d-77% | 4.05 ± 2.17 | 3.54 ± 1.39 | 3.69 ± 1.99 | 3.74 ± 1.09 | 4.00 ± 2.11 | 3.65 ± 1.30 |
| La [mmol] d-83% | 4.99 ± 2.97 | 3.91 ± 1.77 | 4.81 ± 2.93 | 4.19 ± 1.69 | 4.91 ± 2.93 | 4.09 ± 1.60 |
| La [mmol] d-88% | 5.95 ± 2.99 | 4.55 ± 1.57 | 5.69 ± 2.82 | 4.69 ± 1.46 | 5.80 ± 2.94 | 4.64 ± 1.56 |
| La [mmol] d-93% | 9.96 ± 3.54 | 7.10 ± 1.85 | 9.83 ± 3.38 | 7.10 ± 1.81 | 9.89 ± 3.47 | 7.23 ± 1.90 |
| La [mmol] d-100% | 15.91 ± 2.51 | 15.59 ± 2.59 | 15.74 ± 2.40 | 15.70 ± 2.58 | 15.84 ± 2.44 | 15.71 ± 2.60 |
| HR d-77% | 122.50 ± 9.55 | 121.88 ± 13.83 | 121.25 ± 8.78 | 125.50 ± 8.88 | 123.00 ± 8.57 | 123.88 ± 12.30 |
| HR d-83% | 140.25 ± 6.71 | 134.38 ± 9.97 | 138.25 ± 7.03 | 137.63 ± 8.96 | 146.88 ± 21.64 | 135.63 ± 8.48 |
| HR d-88% | 150.00 ± 7.87 | 143.00 ± 8.32 | 148.38 ± 7.42 | 143.75 ± 8.10 | 148.75 ± 7.89 | 143.88 ± 8.43 |
| HR d-93% | 163.00 ± 9.96 | 158.25 ± 11.59 | 162.00 ± 9.47 | 159.25 ± 11.65 | 162.25 ± 9.60 | 159.25 ± 11.65 |
| HR d-100% | 180.88 ± 8.29 | 183.63 ± 8.93 | 179.88 ± 7.74 | 183.88 ± 7.70 | 180.13 ± 8.37 | 184.63 ± 9.24 |
| Variables | Tests I–II in Group I | Tests I–II in Group II | Tests I–III in Group I | Tests I–III in Group II | Tests II–III in Group I | Tests II–III in Group II | Test I in Group I and Test I in Group II | Test II in Group I and Test II in Group II | Test III in Group I and Test III in Group II |
|---|---|---|---|---|---|---|---|---|---|
| T-30 (1) [m] | 0.0020 | 0.6337 | 0.0344 | 0.5101 | 0.2455 | 0.8543 | 0.1388 | 0.0691 | 0.0831 |
| Borg RPE scale | 0.0054 | 0.2680 | 0.0135 | 0.0318 | 0.7092 | 0.2680 | 0.6493 | 0.0064 | 0.0021 |
| La (1) [mmol] d-77% | 0.0006 | 0.0409 | 0.5963 | 0.2380 | 0.0023 | 0.3564 | 0.5627 | 0.9547 | 0.6917 |
| La (1) [mmol] d-83% | 0.0259 | 0.0009 | 0.3221 | 0.0259 | 0.1897 | 0.1897 | 0.3852 | 0.6104 | 0.5027 |
| La (1) [mmol] d-88% | 0.0001 | 0.0252 | 0.0154 | 0.1434 | 0.0631 | 0.3969 | 0.2490 | 0.4048 | 0.3349 |
| La (1) [mmol] d-93% | 0.0089 | 1.0000 | 0.1361 | 0.0162 | 0.2114 | 0.0162 | 0.0585 | 0.0700 | 0.0760 |
| La (1) [mmol] d-100% | 0.0043 | 0.0552 | 0.1930 | 0.0345 | 0.0862 | 0.8257 | 0.8002 | 0.9767 | 0.9224 |
| HR (1) d-77% | 0.3030 | 0.0050 | 0.6779 | 0.1043 | 0.1529 | 0.1834 | 0.9069 | 0.4314 | 0.8700 |
| HR (1) d-83% | 0.6536 | 0.4671 | 0.1441 | 0.7789 | 0.0605 | 0.6536 | 0.3210 | 0.9152 | 0.0627 |
| HR(1) d-88% | 0.0000 | 0.0307 | 0.0007 | 0.0129 | 0.2649 | 0.7074 | 0.1022 | 0.2674 | 0.2435 |
| HR(1) d-93% | 0.0015 | 0.0015 | 0.0132 | 0.0015 | 0.3853 | 1.0000 | 0.3894 | 0.6151 | 0.5837 |
| HR(1) d-100% | 0.0608 | 0.6290 | 0.1539 | 0.0608 | 0.6290 | 0.1539 | 0.5229 | 0.3566 | 0.3016 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okrzymowska, P.; Seidel, W.; Rozek-Piechura, K. The Effectiveness and Validity of Inspiratory Muscle Training in the Training Process of Disabled Swimmers. J. Clin. Med. 2024, 13, 5365. https://doi.org/10.3390/jcm13185365
Okrzymowska P, Seidel W, Rozek-Piechura K. The Effectiveness and Validity of Inspiratory Muscle Training in the Training Process of Disabled Swimmers. Journal of Clinical Medicine. 2024; 13(18):5365. https://doi.org/10.3390/jcm13185365
Chicago/Turabian StyleOkrzymowska, Paulina, Wojciech Seidel, and Krystyna Rozek-Piechura. 2024. "The Effectiveness and Validity of Inspiratory Muscle Training in the Training Process of Disabled Swimmers" Journal of Clinical Medicine 13, no. 18: 5365. https://doi.org/10.3390/jcm13185365