
A Scoping Review of Technology-Based Approaches for Upper Limb Motor Rehabilitation after Stroke: Are We Really Targeting Severe Impairment?

 ,
,  ,
, 
Abstract
:1. Introduction
- (i)
- The actual severity of patients included in trials that explicitly declare to enroll severe subjects to confirm or refute the anecdotal notion of extreme variability in baseline motor impairment, which might be responsible for the hesitating translational success of such interventions [9];
- (ii)
- Whether some of these technological approaches have been more consistently tested on severe patients than others and eventually speculate on why they have.
2. Methods
2.1. Protocol and Eligibility Criteria
- Published between the period of 2008 and 2024;
- Written in English;
- Involved human participants in the framework of a randomized controlled trial.
- If they did not fit into the conceptual framework of the study (not a technology-based rehabilitative approach, wrong outcome);
- If they were reviews, study protocols, and meta-analyses.
2.2. Information Sources and Search Strategy
2.3. Selection of Sources of Evidence
2.4. Data Charting Process and Data Items
- First Author Name;
- Year of publication;
- Source;
- Population sample size (participants per group);
- Inclusion criteria in the RCT related to the upper limb impairment;
- Availability of the dataset used (Yes/No);
- ○
- ≤1 month (acute)
- ○
- ≤3 months (early subacute)
- ○
- ≤6 months (subacute)
- ○
- >6 months (chronic)
- Intervention type, classified as
- ○
- Brain–Computer Interface (BCI)
- ○
- Non-Invasive Brain Stimulation (NIBS)
- ○
- Peripheral Stimulation (PS)
- ○
- Robotic
- ○
- Virtual Reality (VR) and Visual
- Comparator, i.e., control interventions and/or comparison conditions;
- Active motor action required (Yes/Yes whenever possible/No):
- ○
- Yes, if the intervention type requires the participant’s residual motor ability (active motor exercise from the participant)
- ○
- Yes whenever possible refers to conditions foreseeing active motor exercise when feasible, with the technology providing assistance as needed (e.g., robotics)
- ○
- No otherwise
- Combination of technological interventions (Yes/No);
- Dose, expressed as minutes x number of sessions;
- Primary and secondary outcomes;
- Key Findings, classified as Positive, Positive on secondary analyses, and Negative. We define Key Findings as the following:
- ○
- Positive if between-group statistical analyses evaluated for the primary outcomes statistically confirm the hypothesis investigated in the study.
- ○
- Positive on secondary analyses if between-group statistical analyses evaluated for sub-items of the primary/secondary outcomes or considering sub-groups of the population under investigation confirm the hypothesis investigated in the study or if within-group statistical analyses evaluated for the primary/secondary outcomes reveal a statistical improvement only for the experimental group.
- ○
- Negative if between- and within-group analyses do not reveal statistically significant differences among groups.
- Stratification for secondary analyses according to an upper limb impairment criterion;
- Follow-up (Yes/No), i.e., if Yes, we reported the number of months after the end of the intervention;
- Setting: Inpatient/Outpatient.
2.5. Synthesis of Results
2.5.1. Descriptive and Frequency Analysis
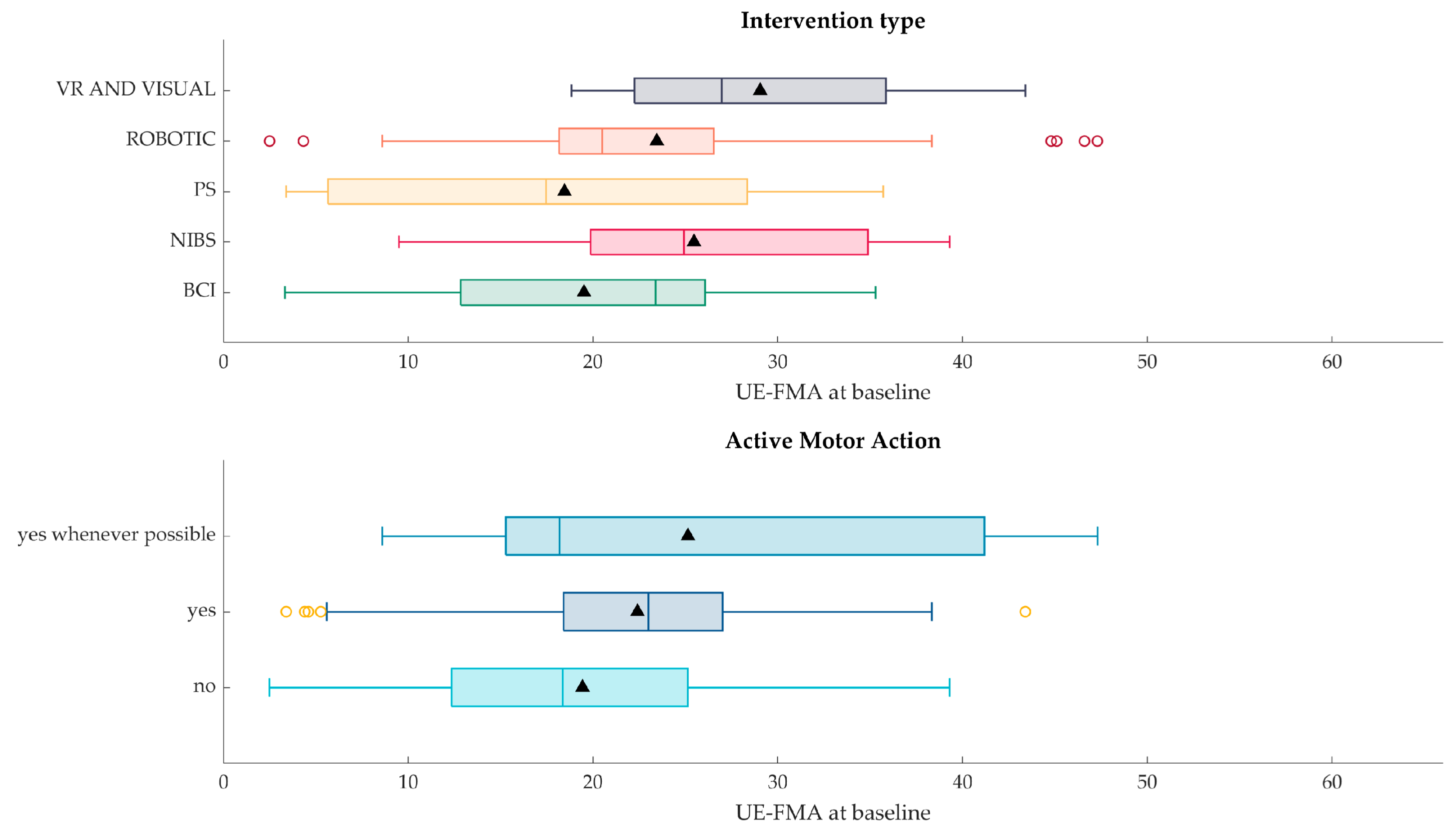
2.5.2. Association Analysis
- Type of intervention (e.g., Robotic, BCI, PS, …);
- Required active upper limb motor actions from the participant by the intervention itself.
3. Results
3.1. Selection of Sources of Evidence
- The rehabilitative intervention under investigation does not include a technology-based approach; videos/instruction displayed on screens or other devices of everyday use (personal computers, tablet, smartphones) were not included;
- The design of the study does not follow the randomized controlled trial design (wrong study design);
- The effectiveness of the rehabilitative intervention under investigation was not assessed in terms of motor function improvement (wrong outcome);
- The paper presents a study protocol, a review, or a meta-analysis.
3.2. Results of Individual Sources of Evidence
3.3. Synthesis of Results
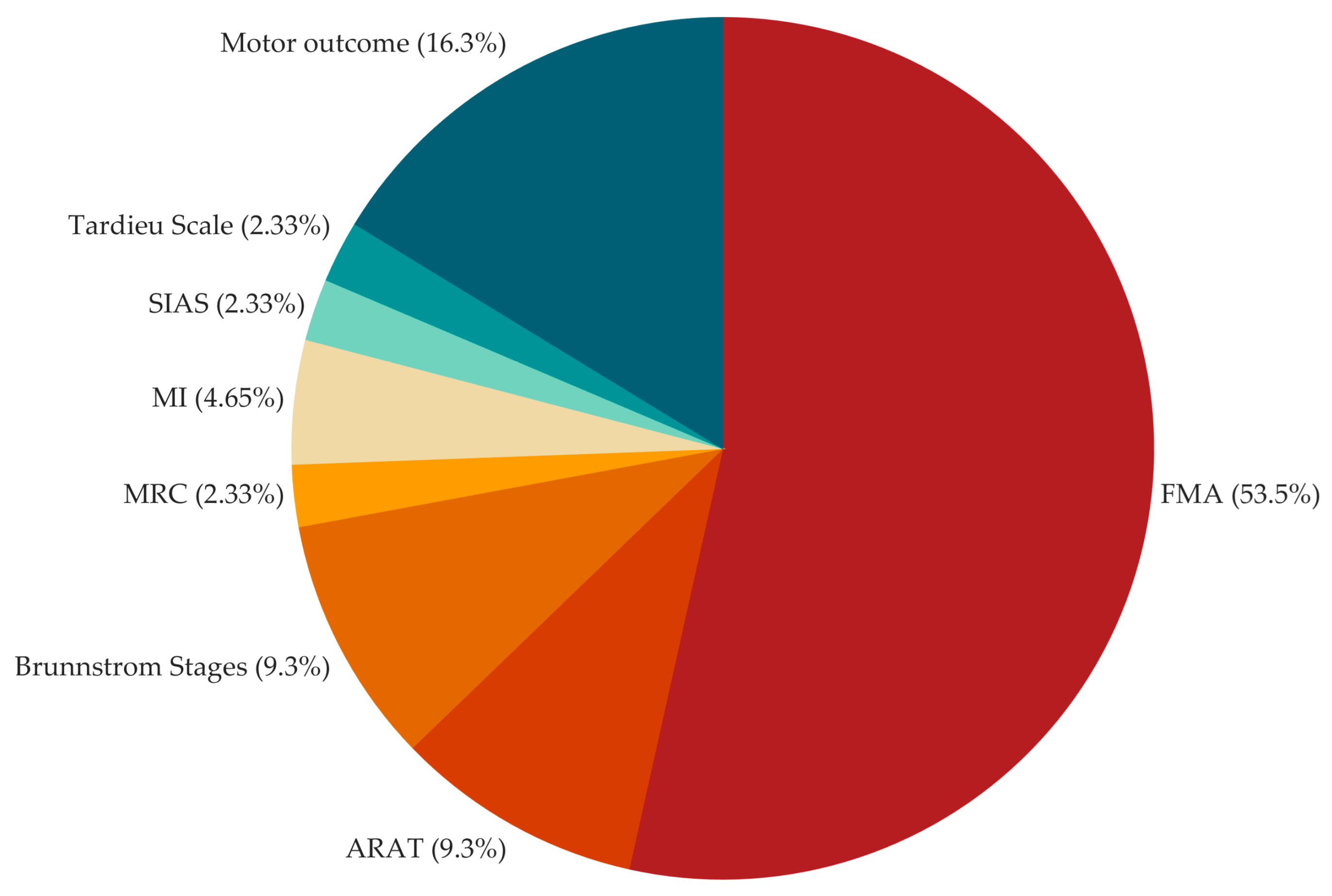
3.3.1. Descriptive and Frequency Results
3.3.2. Association Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Iosa, M.; Morone, G.; Fusco, A.; Bragoni, M.; Coiro, P.; Multari, M.; Venturiero, V.; De Angelis, D.; Pratesi, L.; Paolucci, S. Seven Capital Devices for the Future of Stroke Rehabilitation. Stroke Res. Treat. 2012, 2012, 187965. [Google Scholar] [CrossRef] [PubMed]
- Coscia, M.; Wessel, M.J.; Chaudary, U.; Millán, J.D.R.; Micera, S.; Guggisberg, A.; Vuadens, P.; Donoghue, J.; Birbaumer, N.; Hummel, F.C. Neurotechnology-Aided Interventions for Upper Limb Motor Rehabilitation in Severe Chronic Stroke. Brain 2019, 142, 2182–2197. [Google Scholar] [CrossRef] [PubMed]
- Ward, N.S.; Brander, F.; Kelly, K. Intensive Upper Limb Neurorehabilitation in Chronic Stroke: Outcomes from the Queen Square Programme. J. Neurol. Neurosurg. Psychiatry 2019, 90, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Tenberg, S.; Mueller, S.; Vogt, L.; Roth, C.; Happ, K.; Scherer, M.; Behringer, M.; Niederer, D. Comparative Effectiveness of Upper Limb Exercise Interventions in Individuals with Stroke: A Network Meta-Analysis. Stroke 2023, 54, 1839–1853. [Google Scholar] [CrossRef] [PubMed]
- Dboba, M.M.; Mohd Nordin, N.A.; Manaf, H.; Mohd Rasdi, H.F. Effect of Constraint-Induced Movement Therapy Combined with Neuromuscular Electrical Stimulation on Upper Extremity Function in Stroke Survivors: A Protocol for Systematic Review. Medicine 2023, 102, e34249. [Google Scholar] [CrossRef]
- Morone, G.; Paolucci, S.; Mattia, D.; Pichiorri, F.; Tramontano, M.; Iosa, M. The 3Ts of the New Millennium Neurorehabilitation Gym: Therapy, Technology, Translationality. Expert Rev. Med. Devices 2016, 13, 785–787. [Google Scholar] [CrossRef]
- Coupar, F.; Pollock, A.; Rowe, P.; Weir, C.; Langhorne, P. Predictors of Upper Limb Recovery after Stroke: A Systematic Review and Meta-Analysis. Clin. Rehabil. 2012, 26, 291–313. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic Review or Scoping Review? Guidance for Authors When Choosing between a Systematic or Scoping Review Approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Morone, G.; Pichiorri, F. Post-Stroke Rehabilitation: Challenges and New Perspectives. J. Clin. Med. 2023, 12, 550. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- McGowan, J.; Sampson, M.; Salzwedel, D.M.; Cogo, E.; Foerster, V.; Lefebvre, C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J. Clin. Epidemiol. 2016, 75, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Fugl-Meyer, A.R.; Jääskö, L.; Leyman, I.; Olsson, S.; Steglind, S. The Post-Stroke Hemiplegic Patient. 1. a Method for Evaluation of Physical Performance. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar] [CrossRef] [PubMed]
- Platz, T.; Pinkowski, C.; van Wijck, F.; Kim, I.-H.; di Bella, P.; Johnson, G. Reliability and Validity of Arm Function Assessment with Standardized Guidelines for the Fugl-Meyer Test, Action Research Arm Test and Box and Block Test: A Multicentre Study. Clin. Rehabil. 2005, 19, 404–411. [Google Scholar] [CrossRef]
- Stinear, C.; Ackerley, S.; Byblow, W. Rehabilitation Is Initiated Early after Stroke, but Most Motor Rehabilitation Trials Are Not: A Systematic Review. Stroke 2013, 44, 2039–2045. [Google Scholar] [CrossRef]
- Bernhardt, J.; Hayward, K.S.; Kwakkel, G.; Ward, N.S.; Wolf, S.L.; Borschmann, K.; Krakauer, J.W.; Boyd, L.A.; Carmichael, S.T.; Corbett, D.; et al. Agreed Definitions and a Shared Vision for New Standards in Stroke Recovery Research: The Stroke Recovery and Rehabilitation Roundtable Taskforce. Int. J. Stroke 2017, 12, 444–450. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the Sample Mean and Standard Deviation from the Sample Size, Median, Range and/or Interquartile Range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- Hesse, S.; Werner, C.; Pohl, M.; Mehrholz, J.; Puzich, U.; Krebs, H.I. Mechanical Arm Trainer for the Treatment of the Severely Affected Arm after a Stroke: A Single-Blinded Randomized Trial in Two Centers. Am. J. Phys. Med. Rehabil. 2008, 87, 779–788. [Google Scholar] [CrossRef]
- Lo, A.C.; Guarino, P.D.; Richards, L.G.; Haselkorn, J.K.; Wittenberg, G.F.; Federman, D.G.; Ringer, R.J.; Wagner, T.H.; Krebs, H.I.; Volpe, B.T.; et al. Robot-Assisted Therapy for Long-Term Upper-Limb Impairment after Stroke. N. Engl. J. Med. 2010, 362, 1772–1783. [Google Scholar] [CrossRef]
- Weber, D.J.; Skidmore, E.R.; Niyonkuru, C.; Chang, C.-L.; Huber, L.M.; Munin, M.C. Cyclic Functional Electrical Stimulation Does Not Enhance Gains in Hand Grasp Function When Used as an Adjunct to onabotulinumtoxinA and Task Practice Therapy: A Single-Blind, Randomized Controlled Pilot Study. Arch. Phys. Med. Rehabil. 2010, 91, 679–686. [Google Scholar] [CrossRef]
- Shindo, K.; Fujiwara, T.; Hara, J.; Oba, H.; Hotta, F.; Tsuji, T.; Hase, K.; Liu, M. Effectiveness of Hybrid Assistive Neuromuscular Dynamic Stimulation Therapy in Patients with Subacute Stroke: A Randomized Controlled Pilot Trial. Neurorehabilit. Neural Repair 2011, 25, 830–837. [Google Scholar] [CrossRef] [PubMed]
- Rosewilliam, S.; Malhotra, S.; Roffe, C.; Jones, P.; Pandyan, A.D. Can Surface Neuromuscular Electrical Stimulation of the Wrist and Hand Combined with Routine Therapy Facilitate Recovery of Arm Function in Patients with Stroke? Arch. Phys. Med. Rehabil. 2012, 93, 1715–1721.e1. [Google Scholar] [CrossRef] [PubMed]
- Ochi, M.; Saeki, S.; Oda, T.; Matsushima, Y.; Hachisuka, K. Effects of Anodal and Cathodal Transcranial Direct Current Stimulation Combined with Robotic Therapy on Severely Affected Arms in Chronic Stroke Patients. J. Rehabil. Med. 2013, 45, 137–140. [Google Scholar] [CrossRef]
- Cordo, P.; Wolf, S.; Lou, J.-S.; Bogey, R.; Stevenson, M.; Hayes, J.; Roth, E. Treatment of Severe Hand Impairment Following Stroke by Combining Assisted Movement, Muscle Vibration, and Biofeedback. J. Neurol. Phys. Ther. 2013, 37, 194–203. [Google Scholar] [CrossRef]
- Krewer, C.; Hartl, S.; Müller, F.; Koenig, E. Effects of Repetitive Peripheral Magnetic Stimulation on Upper-Limb Spasticity and Impairment in Patients with Spastic Hemiparesis: A Randomized, Double-Blind, Sham-Controlled Study. Arch. Phys. Med. Rehabil. 2014, 95, 1039–1047. [Google Scholar] [CrossRef]
- Au-Yeung, S.S.Y.; Hui-Chan, C.W.Y. Electrical Acupoint Stimulation of the Affected Arm in Acute Stroke: A Placebo-Controlled Randomized Clinical Trial. Clin. Rehabil. 2014, 28, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Ang, K.K.; Chua, K.S.G.; Phua, K.S.; Wang, C.; Chin, Z.Y.; Kuah, C.W.K.; Low, W.; Guan, C. A Randomized Controlled Trial of EEG-Based Motor Imagery Brain-Computer Interface Robotic Rehabilitation for Stroke. Clin. EEG Neurosci. 2015, 46, 310–320. [Google Scholar] [CrossRef]
- Pichiorri, F.; Morone, G.; Petti, M.; Toppi, J.; Pisotta, I.; Molinari, M.; Paolucci, S.; Inghilleri, M.; Astolfi, L.; Cincotti, F.; et al. Brain-Computer Interface Boosts Motor Imagery Practice during Stroke Recovery. Ann. Neurol. 2015, 77, 851–865. [Google Scholar] [CrossRef]
- Pennati, G.V.; Da Re, C.; Messineo, I.; Bonzaiuti, D. How Could Robotic Training and Botolinum Toxin Be Combined in Chronic Post Stroke Upper Limb Spasticity? A Pilot Study. Eur. J. Phys. Rehabil. Med. 2015, 51, 381–387. [Google Scholar]
- Carrico, C.; Chelette, K.C.; Westgate, P.M.; Powell, E.; Nichols, L.; Fleischer, A.; Sawaki, L. Nerve Stimulation Enhances Task-Oriented Training in Chronic, Severe Motor Deficit after Stroke: A Randomized Trial. Stroke 2016, 47, 1879–1884. [Google Scholar] [CrossRef]
- Wu, X.; Guarino, P.; Lo, A.C.; Peduzzi, P.; Wininger, M. Long-Term Effectiveness of Intensive Therapy in Chronic Stroke. Neurorehabilit. Neural Repair 2016, 30, 583–590. [Google Scholar] [CrossRef]
- Frolov, A.A.; Mokienko, O.; Lyukmanov, R.; Biryukova, E.; Kotov, S.; Turbina, L.; Nadareyshvily, G.; Bushkova, Y. Post-Stroke Rehabilitation Training with a Motor-Imagery-Based Brain-Computer Interface (BCI)-Controlled Hand Exoskeleton: A Randomized Controlled Multicenter Trial. Front. Neurosci. 2017, 11, 400. [Google Scholar] [CrossRef] [PubMed]
- Tomić, T.J.D.; Savić, A.M.; Vidaković, A.S.; Rodić, S.Z.; Isaković, M.S.; Rodríguez-De-Pablo, C.; Keller, T.; Konstantinović, L.M. Arm Assist Robotic System versus Matched Conventional Therapy for Poststroke Upper Limb Rehabilitation: A Randomized Clinical Trial. BioMed Res. Int. 2017, 2017, 7659893. [Google Scholar] [CrossRef] [PubMed]
- Schick, T.; Schlake, H.-P.; Kallusky, J.; Hohlfeld, G.; Steinmetz, M.; Tripp, F.; Krakow, K.; Pinter, M.; Dohle, C. Synergy Effects of Combined Multichannel EMG-Triggered Electrical Stimulation and Mirror Therapy in Subacute Stroke Patients with Severe or Very Severe Arm/Hand Paresis. Restor. Neurol. Neurosci. 2017, 35, 319–332. [Google Scholar] [CrossRef]
- Brunner, I.; Skouen, J.S.; Hofstad, H.; Aßmus, J.; Becker, F.; Sanders, A.-M.; Pallesen, H.; Kristensen, L.Q.; Michielsen, M.; Thijs, L.; et al. Virtual Reality Training for Upper Extremity in Subacute Stroke (VIRTUES): A Multicenter RCT. Neurology 2017, 89, 2413–2421. [Google Scholar] [CrossRef]
- Rabadi, M.H.; Aston, C.E. Effect of Transcranial Direct Current Stimulation on Severely Affected Arm-Hand Motor Function in Patients after an Acute Ischemic Stroke: A Pilot Randomized Control Trial. Am. J. Phys. Med. Rehabil. 2017, 96, S178–S184. [Google Scholar] [CrossRef]
- Marquez-Chin, C.; Bagher, S.; Zivanovic, V.; Popovic, M.R. Functional Electrical Stimulation Therapy for Severe Hemiplegia: Randomized Control Trial Revisited. Can. J. Occup. Ther. 2017, 84, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Carrico, C.; Westgate, P.M.; Salmon Powell, E.; Chelette, K.C.; Nichols, L.; Pettigrew, L.C.; Sawaki, L. Nerve Stimulation Enhances Task-Oriented Training for Moderate-to-Severe Hemiparesis 3-12 Months after Stroke: A Randomized Trial. Am. J. Phys. Med. Rehabil. 2018, 97, 808–815. [Google Scholar] [CrossRef]
- Ding, L.; Wang, X.; Guo, X.; Chen, S.; Wang, H.; Jiang, N.; Jia, J. Camera-Based Mirror Visual Feedback: Potential to Improve Motor Preparation in Stroke Patients. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 1897–1905. [Google Scholar] [CrossRef]
- Conroy, S.S.; Wittenberg, G.F.; Krebs, H.I.; Zhan, M.; Bever, C.T.; Whitall, J. Robot-Assisted Arm Training in Chronic Stroke: Addition of Transition-to-Task Practice. Neurorehabilit. Neural Repair 2019, 33, 751–761. [Google Scholar] [CrossRef]
- Rodgers, H.; Bosomworth, H.; Krebs, H.I.; van Wijck, F.; Howel, D.; Wilson, N.; Aird, L.; Alvarado, N.; Andole, S.; Cohen, D.L.; et al. Robot Assisted Training for the Upper Limb after Stroke (RATULS): A Multicentre Randomised Controlled Trial. Lancet 2019, 394, 51–62. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Murguialday, A.; Curado, M.R.; Broetz, D.; Yilmaz, Ö.; Brasil, F.L.; Liberati, G.; Garcia-Cossio, E.; Cho, W.; Caria, A.; Cohen, L.G.; et al. Brain-Machine Interface in Chronic Stroke: Randomized Trial Long-Term Follow-Up. Neurorehabil. Neural Repair 2019, 33, 188–198. [Google Scholar] [CrossRef] [PubMed]
- Takebayashi, T.; Takahashi, K.; Domen, K.; Hachisuka, K. Impact of Initial Flexor Synergy Pattern Scores on Improving Upper Extremity Function in Stroke Patients Treated with Adjunct Robotic Rehabilitation: A Randomized Clinical Trial. Top. Stroke Rehabil. 2020, 27, 516–524. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Park, G.; Cho, D.Y.; Kim, H.Y.; Lee, J.-Y.; Kim, S.; Park, S.-B.; Shin, J.-H. Comparisons between End-Effector and Exoskeleton Rehabilitation Robots Regarding Upper Extremity Function among Chronic Stroke Patients with Moderate-to-Severe Upper Limb Impairment. Sci. Rep. 2020, 10, 1806. [Google Scholar] [CrossRef] [PubMed]
- Chew, E.; Teo, W.-P.; Tang, N.; Ang, K.K.; Ng, Y.S.; Zhou, J.H.; Teh, I.; Phua, K.S.; Zhao, L.; Guan, C. Using Transcranial Direct Current Stimulation to Augment the Effect of Motor Imagery-Assisted Brain-Computer Interface Training in Chronic Stroke Patients—Cortical Reorganization Considerations. Front. Neurol. 2020, 11, 948. [Google Scholar] [CrossRef]
- Lin, C.-W.; Kuo, L.-C.; Lin, Y.-C.; Su, F.-C.; Lin, Y.-A.; Hsu, H.-Y. Development and Testing of a Virtual Reality Mirror Therapy System for the Sensorimotor Performance of Upper Extremity: A Pilot Randomized Controlled Trial. IEEE Access 2021, 9, 14725–14734. [Google Scholar] [CrossRef]
- Hu, Y.-Q.; Gao, T.-H.; Li, J.; Tao, J.-C.; Bai, Y.-L.; Lu, R.-R. Motor Imagery-Based Brain-Computer Interface Combined with Multimodal Feedback to Promote Upper Limb Motor Function after Stroke: A Preliminary Study. Evid.-Based Complement. Altern. Med. 2021, 2021, 1116126. [Google Scholar] [CrossRef]
- Boasquevisque, D.D.S.; Servinsckins, L.; De Paiva, J.P.Q.; Dos Santos, D.G.; Soares, P.; Pires, D.S.; Meltzer, J.A.; Plow, E.B.; De Freitas, P.F.; Speciali, D.S.; et al. Contralesional Cathodal Transcranial Direct Current Stimulation Does Not Enhance Upper Limb Function in Subacute Stroke: A Pilot Randomized Clinical Trial. Neural Plast. 2021, 2021, 8858394. [Google Scholar] [CrossRef]
- Dawson, J.; Liu, C.Y.; Francisco, G.E.; Cramer, S.C.; Wolf, S.L.; Dixit, A.; Alexander, J.; Ali, R.; Brown, B.L.; Feng, W.; et al. Vagus Nerve Stimulation Paired with Rehabilitation for Upper Limb Motor Function after Ischaemic Stroke (VNS-REHAB): A Randomised, Blinded, Pivotal, Device Trial. Lancet 2021, 397, 1545–1553. [Google Scholar] [CrossRef]
- Llorens, R.; Fuentes, M.A.; Borrego, A.; Latorre, J.; Alcañiz, M.; Colomer, C.; Noé, E. Effectiveness of a Combined Transcranial Direct Current Stimulation and Virtual Reality-Based Intervention on Upper Limb Function in Chronic Individuals Post-Stroke with Persistent Severe Hemiparesis: A Randomized Controlled Trial. J. NeuroEngineering Rehabil. 2021, 18, 108. [Google Scholar] [CrossRef]
- Cantillo-Negrete, J.; Carino-Escobar, R.I.; Carrillo-Mora, P.; Rodriguez-Barragan, M.A.; Hernandez-Arenas, C.; Quinzaños-Fresnedo, J.; Hernandez-Sanchez, I.R.; Galicia-Alvarado, M.A.; Miguel-Puga, A.; Arias-Carrion, O. Brain-Computer Interface Coupled to a Robotic Hand Orthosis for Stroke Patients’ Neurorehabilitation: A Crossover Feasibility Study. Front. Hum. Neurosci. 2021, 15, 656975. [Google Scholar] [CrossRef] [PubMed]
- Takebayashi, T.; Takahashi, K.; Okita, Y.; Kubo, H.; Hachisuka, K.; Domen, K. Impact of the Robotic-Assistance Level on Upper Extremity Function in Stroke Patients Receiving Adjunct Robotic Rehabilitation: Sub-Analysis of a Randomized Clinical Trial. J. NeuroEngineering Rehabil. 2022, 19, 25. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.-F.; Zhang, D.; Zhang, J.; Hai, H.; Zhao, Y.-Y.; Ma, Y.-W. A Randomized Controlled Trial of Repetitive Peripheral Magnetic Stimulation Applied in Early Subacute Stroke: Effects on Severe Upper-Limb Impairment. Clin. Rehabil. 2022, 36, 693–702. [Google Scholar] [CrossRef] [PubMed]
- Schrader, M.; Sterr, A.; Kettlitz, R.; Wohlmeiner, A.; Buschfort, R.; Dohle, C.; Bamborschke, S. The Effect of Mirror Therapy Can Be Improved by Simultaneous Robotic Assistance. Restor. Neurol. Neurosci. 2022, 40, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Ohnishi, H.; Miyasaka, H.; Shindo, N.; Ito, K.; Tsuji, S.; Sonoda, S. Effectiveness of Repetitive Facilitative Exercise Combined with Electrical Stimulation Therapy to Improve Very Severe Paretic Upper Limbs in with Stroke Patients: A Randomized Controlled Trial. Occup. Ther. Int. 2022, 2022, 4847363. [Google Scholar] [CrossRef]
- Huang, Y.-J.; Wang, S.-M.; Chen, C.; Chen, C.-A.; Wu, C.-W.; Chen, J.-J.; Peng, C.-W.; Lin, C.-W.; Huang, S.-W.; Chen, S.-C. High-Definition Transcranial Direct Current with Electrical Theta Burst on Post-Stroke Motor Rehabilitation: A Pilot Randomized Controlled Trial. Neurorehabilit. Neural Repair 2022, 36, 645–654. [Google Scholar] [CrossRef] [PubMed]
- Wong, Y.; Li, C.-J.-Z.; Ada, L.; Zhang, T.; Månum, G.; Langhammer, B. Upper limb training a with hand orthosis in early subacute stroke: A pilot randomized trial. J. Rehabil. Med. 2022, 54, jrm00279. [Google Scholar] [CrossRef]
- Cordo, P.; Wolf, S.; Rymer, W.Z.; Byl, N.; Stanek, K.; Hayes, J.R. Assisted Movement with Proprioceptive Stimulation Augments Recovery from Moderate-To-Severe Upper Limb Impairment during Subacute Stroke Period: A Randomized Clinical Trial. Neurorehabilit. Neural Repair 2022, 36, 239–250. [Google Scholar] [CrossRef] [PubMed]
- Takebayashi, T.; Takahashi, K.; Amano, S.; Gosho, M.; Sakai, M.; Hashimoto, K.; Hachisuka, K.; Uchiyama, Y.; Domen, K. Robot-Assisted Training as Self-Training for Upper-Limb Hemiplegia in Chronic Stroke: A Randomized Controlled Trial. Stroke 2022, 53, 2182–2191. [Google Scholar] [CrossRef]
- Williamson, J.N.; James, S.A.; He, D.; Li, S.; Sidorov, E.V.; Yang, Y. High-Definition Transcranial Direct Current Stimulation for Upper Extremity Rehabilitation in Moderate-to-Severe Ischemic Stroke: A Pilot Study. Front. Hum. Neurosci. 2023, 17, 1286238. [Google Scholar] [CrossRef]
- Dawson, J.; Engineer, N.D.; Cramer, S.C.; Wolf, S.L.; Ali, R.; O’Dell, M.W.; Pierce, D.; Prudente, C.N.; Redgrave, J.; Feng, W.; et al. Vagus Nerve Stimulation Paired with Rehabilitation for Upper Limb Motor Impairment and Function after Chronic Ischemic Stroke: Subgroup Analysis of the Randomized, Blinded, Pivotal, VNS-REHAB Device Trial. Neurorehabilit. Neural Repair 2023, 37, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Liu, Z.; Gu, J.; Tan, J.; Hu, T. Effectiveness of Soft Robotic Glove versus Repetitive Transcranial Magnetic Stimulation in Post-Stroke Patients with Severe Upper Limb Dysfunction: A Randomised Controlled Trial. Front. Neurol. 2023, 13, 887205. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.-J.; He, C.; Xu, J.; Zheng, C.-J.; Wu, J.; Xia, N.; Hua, Q.; Xia, W.-G.; Xiong, C.-H.; Huang, X.-L. Exoskeleton-Assisted Anthropomorphic Movement Training for the Upper Limb after Stroke: The EAMT Randomized Trial. Stroke 2023, 54, 1464–1473. [Google Scholar] [CrossRef] [PubMed]
- Feingold-Polak, R.; Barzel, O.; Levy-Tzedek, S. Socially Assistive Robot for Stroke Rehabilitation: A Long-Term in-the-Wild Pilot Randomized Controlled Trial. IEEE Trans. Neural Syst. Rehabil. Eng. 2024, 32, 1616–1626. [Google Scholar] [CrossRef]
- Brunner, I.; Lundquist, C.B.; Pedersen, A.R.; Spaich, E.G.; Dosen, S.; Savic, A. Brain Computer Interface Training with Motor Imagery and Functional Electrical Stimulation for Patients with Severe Upper Limb Paresis after Stroke: A Randomized Controlled Pilot Trial. J. NeuroEngineering Rehabil. 2024, 21, 10. [Google Scholar] [CrossRef]
- Duncan, P.W.; Wallace, D.; Lai, S.M.; Johnson, D.; Embretson, S.; Laster, L.J. The Stroke Impact Scale Version 2.0. Evaluation of Reliability, Validity, and Sensitivity to Change. Stroke 1999, 30, 2131–2140. [Google Scholar] [CrossRef]
- Sulter, G.; Steen, C.; De Keyser, J. Use of the Barthel Index and Modified Rankin Scale in Acute Stroke Trials. Stroke 1999, 30, 1538–1541. [Google Scholar] [CrossRef]
- Morris, D.M.; Uswatte, G.; Crago, J.E.; Cook III, E.W.; Taub, E. The Reliability of the Wolf Motor Function Test for Assessing Upper Extremity Function after Stroke. Arch. Phys. Med. Rehabil. 2001, 82, 750–755. [Google Scholar] [CrossRef]
- Sivan, M.; O’Connor, R.J.; Makower, S.; Levesley, M.; Bhakta, B. Systematic Review of Outcome Measures Used in the Evaluation of Robot-Assisted Upper Limb Exercise in Stroke. J. Rehabil. Med. 2011, 43, 181–189. [Google Scholar] [CrossRef]
- Gladstone, D.J.; Danells, C.J.; Black, S.E. The Fugl-Meyer Assessment of Motor Recovery after Stroke: A Critical Review of Its Measurement Properties. Neurorehabil. Neural Repair 2002, 16, 232–240. [Google Scholar] [CrossRef]
- Woodbury, M.L.; Velozo, C.A.; Richards, L.G.; Duncan, P.W. Rasch Analysis Staging Methodology to Classify Upper Extremity Movement Impairment after Stroke. Arch. Phys. Med. Rehabil. 2013, 94, 1527–1533. [Google Scholar] [CrossRef] [PubMed]
- Woytowicz, E.J.; Rietschel, J.C.; Goodman, R.N.; Conroy, S.S.; Sorkin, J.D.; Whitall, J.; McCombe Waller, S. Determining Levels of Upper Extremity Movement Impairment by Applying a Cluster Analysis to the Fugl-Meyer Assessment of the Upper Extremity in Chronic Stroke. Arch. Phys. Med. Rehabil. 2017, 98, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Luft, A.R.; McCombe-Waller, S.; Whitall, J.; Forrester, L.W.; Macko, R.; Sorkin, J.D.; Schulz, J.B.; Goldberg, A.P.; Hanley, D.F. Repetitive Bilateral Arm Training and Motor Cortex Activation in Chronic Stroke: A Randomized Controlled Trial. JAMA 2004, 292, 1853–1861. [Google Scholar] [CrossRef]
- Zeiler, S.R.; Krakauer, J.W. The Interaction between Training and Plasticity in the Poststroke Brain. Curr. Opin. Neurol. 2013, 26, 609–616. [Google Scholar] [CrossRef]
- Alexander, J.; Langhorne, P.; Kidd, L.; Wu, O.; McConnachie, A.; van Wijck, F.; Dawson, J. SaeboGlove Therapy for Upper Limb Disability and Severe Hand Impairment after Stroke (SUSHI): Study Protocol for a Randomised Controlled Trial. Eur. Stroke J. 2021, 6, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Dai, W.; Yang, X.; Liu, C.; Ding, H.; Guo, C.; Zhu, Y.; Dong, M.; Qian, Y.; Fang, L.; Wang, T.; et al. Effects of Repetitive Transcranial Magnetic Stimulation over the Contralesional Dorsal Premotor Cortex on Upper Limb Function in Severe Ischaemic Stroke: Study Protocol for a Randomised Controlled Trial. BMJ Open 2023, 13, e074037. [Google Scholar] [CrossRef]
- Gonzalez-Santos, J.; Soto-Camara, R.; Rodriguez-Fernández, P.; Jimenez-Barrios, M.; Gonzalez-Bernal, J.; Collazo-Riobo, C.; Jahouh, M.; Bravo-Anguiano, Y.; Trejo-Gabriel-Galan, J.M. Effects of Home-Based Mirror Therapy and Cognitive Therapeutic Exercise on the Improvement of the Upper Extremity Functions in Patients with Severe Hemiparesis after a Stroke: A Protocol for a Pilot Randomised Clinical Trial. BMJ Open 2020, 10, e035768. [Google Scholar] [CrossRef]
- Kinoshita, S.; Ikeda, K.; Yasuno, S.; Takahashi, S.; Yamada, N.; Okuyama, Y.; Sasaki, N.; Hada, T.; Kuriyama, C.; Suzuki, S.; et al. Dose-Response of rPMS for Upper Limb Hemiparesis after Stroke. Medicine 2020, 99, e20752. [Google Scholar] [CrossRef]
- Lee, S.H.; Kim, W.-S.; Park, J.; Kim, J.; Paik, N.-J. Effects of Anodal Transcranial Direct Current Stimulation over the Contralesional Hemisphere on Motor Recovery in Subacute Stroke Patients with Severe Upper Extremity Hemiparesis: Study Protocol for a Randomized Controlled Trial. Medicine 2020, 99, e19495. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, L.; Wang, S.; Long, L.; Zang, Q.; Jia, G. Efficacy and Safety of Electroacupuncture at Auricular Concha Region in Promoting of Rehabilitation of Ischemic Stroke Patients with Upper Limb Motor Dysfunction: A Study Protocol for a Randomized Pilot Trial. Medicine 2022, 101, e28047. [Google Scholar] [CrossRef]
- Mizuno, K.; Abe, T.; Ushiba, J.; Kawakami, M.; Ohwa, T.; Hagimura, K.; Ogura, M.; Okuyama, K.; Fujiwara, T.; Liu, M. Evaluating the Effectiveness and Safety of the Electroencephalogram-Based Brain-Machine Interface Rehabilitation System for Patients with Severe Hemiparetic Stroke: Protocol for a Randomized Controlled Trial (BEST-BRAIN Trial). JMIR Res. Protoc. 2018, 7, e12339. [Google Scholar] [CrossRef] [PubMed]
- Mohan, A.; Knutson, J.S.; Cunningham, D.A.; Widina, M.; O’Laughlin, K.; Arora, T.; Li, X.; Sakaie, K.; Wang, X.; Uchino, K.; et al. Contralaterally Controlled Functional Electrical Stimulation Combined with Brain Stimulation for Severe Upper Limb Hemiplegia-Study Protocol for a Randomized Controlled Trial. Front. Neurol. 2022, 13, 869733. [Google Scholar] [CrossRef]
- Rodgers, H.; Shaw, L.; Bosomworth, H.; Aird, L.; Alvarado, N.; Andole, S.; Cohen, D.L.; Dawson, J.; Eyre, J.; Finch, T.; et al. Robot Assisted Training for the Upper Limb after Stroke (RATULS): Study Protocol for a Randomised Controlled Trial. Trials 2017, 18, 340. [Google Scholar] [CrossRef]
- Stoykov, M.E.; Biller, O.M.; Wax, A.; King, E.; Schauer, J.M.; Fogg, L.F.; Corcos, D.M. Bilateral Upper Extremity Motor Priming (BUMP) plus Task-Specific Training for Severe, Chronic Upper Limb Hemiparesis: Study Protocol for a Randomized Clinical Trial. Trials 2022, 23, 523. [Google Scholar] [CrossRef] [PubMed]
- van Lieshout, E.C.C.; Visser-Meily, J.M.A.; Neggers, S.F.W.; van der Worp, H.B.; Dijkhuizen, R.M. Brain Stimulation for Arm Recovery after Stroke (B-STARS): Protocol for a Randomised Controlled Trial in Subacute Stroke Patients. BMJ Open 2017, 7, e016566. [Google Scholar] [CrossRef] [PubMed]
- Wei, D.; Hua, X.-Y.; Zheng, M.-X.; Wu, J.-J.; Xu, J.-G. Effectiveness of Robot-Assisted Virtual Reality Mirror Therapy for Upper Limb Motor Dysfunction after Stroke: Study Protocol for a Single-Center Randomized Controlled Clinical Trial. BMC Neurol. 2022, 22, 307. [Google Scholar] [CrossRef]
- Wei, X.; Xia, N.; Li, Y.-A.; Gu, M.; Zhang, T.; Gao, W.; Liu, Y. Immediate and Short-Term Effects of Continuous Theta Burst Transcranial Magnetic Stimulation over Contralesional Premotor Area on Post-Stroke Spasticity in Patients with Severe Hemiplegia: Study Protocol for a Randomized Controlled Trial. Front. Neurol. 2022, 13, 895580. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author Name, Year of Publication | Population Sample Size (Participants per Group) | Severity of the Impairment (UE-FMA and/or ARAT per Group) | IC | Time Since Injury | Intervention Type | Active Motor Action Required | Comparator | Primary Outcome Measures | Key Findings |
|---|---|---|---|---|---|---|---|---|---|
| Hesse, 2008 [18] | EG: 27 CG: 27 | UE-FMA | Yes | ES | PS, Robotic | Yes, whenever possible | Different Technology | UE- FMA | Neg |
| EG: 8.8 ± 4.5 | |||||||||
| CG: 8.6 ± 3.5 | |||||||||
| Lo, 2010 [19] | EG: 47 CG1: 46 CG2: 27 | UE-FMA | Yes | C | Robotic | Yes | Dose Equivalent UL Training, Usual Care | UE- FMA | Pos On Sec |
| EG: 19.7 ± 10.7 | |||||||||
| CG1: 17.3 ± 8.4 | |||||||||
| CG2: 20.3 ± 9.0 | |||||||||
| Weber, 2010 [20] | EG: 10 CG: 13 | ARAT | Yes | C | PS | Yes | Without Technology | MAL | Neg |
| EG: 19.5 ± 13.9 | |||||||||
| CG: 25.8 ± 15.5 | |||||||||
| Shindo, 2011 [21] | EG: 10 CG: 10 | UE-FMA | Yes | ES | PS | Yes | Without technology | UE-FMA | Pos |
| EG: 24.4 ± 10.9 | |||||||||
| CG: 23.0 ± 13.1 | |||||||||
| ARAT | |||||||||
| EG: 9.3 ± 8.4 | |||||||||
| CG: 15.8 ± 13.7 | |||||||||
| Rosewilliam, 2012 [22] | EG: 31 CG: 36 | ARAT | Yes | A/ES | PS | No | Usual Care | ARAT | Neg |
| EG: 0.0 ± 0.0 | |||||||||
| CG: 0.6 ± 3.5 | |||||||||
| Ochi, 2013 [23] | EG: 9 CG: 9 | UE-FMA | Yes | C | NIBS, Robotic | No | Different Parameters | UE-FMA | Pos On Sec |
| EG: 23.2 ± 16.6 | |||||||||
| CG: 23.6 ± 16.7 | |||||||||
| Cordo, 2013 [24] | EG1: 22 EG2: 21 | UE-FMA | Yes | C | PS, Robotic | Yes | Different Technology | UE-FMA | Pos On Sec |
| EG1: 23.1 ± 8.8 | |||||||||
| EG2: 19.4 ± 6.2 | |||||||||
| Krewer, 2014 [25] | EG: 31 CG: 32 | UE-FMA | Yes | C | PS | No | Sham Stimulation | MTS UE-FMA | Pos On Sec |
| EG: 5 (4–27) | |||||||||
| CG: 4 (4–9) | |||||||||
| Au-Yeung, 2014 [26] | EG: 29 CG1: 21 CG2: 23 | ARAT | Yes | A | PS | No | Sham Stimulation, Usual Care | Force measures | Pos |
| EG: 8.9 ± 17.6 | |||||||||
| CG1: 3.1 ± 8.2 | |||||||||
| CG2: 9.2 ± 16.3 | |||||||||
| Ang, 2015 [27] | EG: 11 CG: 14 | UE-FMA | Yes | C | BCI, Robotic | Yes | Different Combination | UE-FMA | Neg |
| EG: 26.3 ± 10.3 | |||||||||
| CG: 26.5 ± 18.2 | |||||||||
| Pichiorri, 2015 [28] | EG: 14 CG: 14 | UE-FMA | No | ES/S | BCI, VR and Visual | No | Without Technology | UE-FMA | Pos |
| EG: 23.4 ± 17.3 | |||||||||
| CG: 24.2 ± 18.2 | |||||||||
| Pennati, 2015 [29] | EG1: 8 EG2: 7 | UE-FMA | No | C | Robotic | Yes | Different Combination | UE-FMA BBT FIM MAS | Neg |
| EG1: 29.25 ± 13.91 | |||||||||
| EG2: 18.14 ± 5.27 | |||||||||
| Carrico, 2016 [30] | EG: 18 CG: 18 | UE-FMA | Yes | C | PS | Yes | Sham Stimulation | UE-FMA | Pos |
| EG: 25.7 ± 13.3 | |||||||||
| CG: 22.8 ± 15.0 | |||||||||
| ARAT | |||||||||
| EG: 13.9 ± 12.3 | |||||||||
| CG: 10.4 ± 11.2 | |||||||||
| Wu, 2016 [31] | EG: 99 CG: 28 | UE-FMA | Yes | C | Robotic | Yes | Usual Care | UE-FMA | Pos |
| EG: 18.5 ± 9.7 | |||||||||
| CG: 20.3 ± 9.0 | |||||||||
| Frolov, 2017 [32] | EG: 55 CG: 19 | UE-FMA | No | S/C | BCI, Robotic | No | Sham Control | UE-FMA ARAT | Pos On Sec |
| EG: 24.0 (12.0–40.0) | |||||||||
| CG: 12.0 (11.0–49.0) | |||||||||
| ARAT | |||||||||
| EG: 4.0 (0.0–31.0) | |||||||||
| CG: 3.0 (0.0–30.0) | |||||||||
| Tomic, 2017 [33] | EG: 13 CG: 13 | UE-FMA | Yes | ES | Robotic | Yes | Dose Equivalent UL Training | UE-FMA | Pos |
| EG: 26.5 ± 7.7 | |||||||||
| CG: 26.6 ± 7.5 | |||||||||
| Schick, 2017 [34] | EG: 16 CG: 17 | UE-FMA | Yes | ES | PS | No | Different Combination | UE-FMA | Pos On Sec |
| EG: 16.67 ± 10.80 | |||||||||
| CG: 16.29 ± 9.00 | |||||||||
| Brunner, 2017 [35] | EG: 57 CG: 55 | ARAT | Yes | ES | VR and Visual | Yes | Dose Equivalent UL Training | ARAT | Neg |
| EG: 25.8 ± 18.3 | |||||||||
| CG: 24.2 ± 18.6 | |||||||||
| Rabadi, 2017 [36] | EG: 8 CG: 8 | ARAT | Yes | A | NIBS | No | Sham Stimulation | ARAT | Neg |
| EG: 4.0 ± 10.9 | |||||||||
| CG: 1.9 ± 4.2 | |||||||||
| Marquez-Chin, 2017 [37] | EG: 10 CG: 11C | UE-FMA | Yes | A/ES | PS | Yes | Usual Care | FIM UE-FMA | Pos |
| EG: 3.4 ± 4.8 | |||||||||
| CG: 4.4 ± 4.6 | |||||||||
| Carrico, 2018 [38] | EG: 33 CG: 22 | UE-FMA | Yes | S/C | PS | No | Sham Stimulation | WMFT | Pos |
| EG: 18.48 ± 12.75 | |||||||||
| CG: 18.23 ± 13.34 | |||||||||
| ARAT | |||||||||
| EG: 11.58 ± 12.80 | |||||||||
| CG: 13.36 ± 14.68 | |||||||||
| Ding, 2018 [39] | EG: 38 CG: 41 | UE-FMA | No | S/C | VR and Visual | Yes | Dose Equivalent UL Training | UE-FMA | Pos |
| EG: 25.66 ± 17.63 | |||||||||
| CG: 18.85 ± 16.38 | |||||||||
| Conroy, 2019 [40] | EG: 22 CG: 19 | UE-FMA | Yes | C | Robotic | Yes | Different Combination | UE-FMA | Pos On Sec |
| EG: 20.7 ± 8.5 | |||||||||
| CG: 21.6 ± 8.5 | |||||||||
| Rodgers, 2019 [41] | EG: 239 CG1: 246 CG2: 223 | UE-FMA | Yes | S/C | Robotic | Yes, whenever possible | Dose Equivalent UL Training, Usual care | ARAT | Neg |
| EG: 18.0 ± 13.1 | |||||||||
| CG1: 18.2 ± 14.1 | |||||||||
| CG2: 18.2 ± 13.9 | |||||||||
| ARAT | |||||||||
| EG: 8.5 ± 11.9 | |||||||||
| CG1: 8.7 ± 11.9 | |||||||||
| CG2: 8.1 ± 11.5 | |||||||||
| Ramos-Murguialday, 2019 [42] | EG: 16 CG: 12 | UE-FMA | Yes | C | BCI, Robotic | Yes | Sham Control | UE-FMA (54) | Pos On Sec |
| EG: 11.16 ± 1.73 | |||||||||
| CG: 13.29 ± 2.86 | |||||||||
| Takebayashi, 2020 [43] | EG: 30 CG: 26 | UE-FMA | Yes | ES | Robotic | Yes, whenever possible | Dose Equivalent UL Training | UE-FMA | Pos On Sec |
| EG: 47.3 ± 7.4 (mild) | |||||||||
| CG: 45.1 ± 19.4 (mild) | |||||||||
| EG: 30.3 ± 12.5 (moderate) | |||||||||
| CG: 25.8 ± 10.5 (moderate) | |||||||||
| EG: 16.1 ± 10.5 (severe) | |||||||||
| CG: 14.8 ± 4.7 (severe) | |||||||||
| Lee, 2020 [44] | EG1: 19 EG2: 19 | UE-FMA | Yes | S/C | Robotic | Yes, whenever possible | Different Technology | UE-FMA WMFT | (*) |
| EG1: 15.37 ± 5.14 | |||||||||
| EG2: 15.26 ± 4.37 | |||||||||
| Chew, 2020 [45] | EG: 10 CG: 9 | UE-FMA | Yes | C | BCI, NIBS | No | Sham Stimulation | UE-FMA | Pos On Sec |
| EG: 35.3 ± 7.8 | |||||||||
| CG: 32.6 ± 8.1 | |||||||||
| Lin, 2021 [46] | EG: 9 CG: 9 | UE-FMA | Yes | C | VR and Visual | Yes | Without technology | UE-FMA | Pos |
| EG: 43.4 ± 14.5 | |||||||||
| CG: 28.3 ± 18.1 | |||||||||
| Hu, 2021 [47] | EG: 7 CG: 5 | UE-FMA | Yes | S/C | BCI, VR and Visual | No | Without technology | UE-FMA | Pos On Sec |
| EG: 12.70 ± 8.80 | |||||||||
| CG: 13.80 ± 6.65 | |||||||||
| ARAT | |||||||||
| EG: 3.29 ± 5.79 | |||||||||
| CG: 6.60 ± 12.29 | |||||||||
| Boasquevisque, 2021 [48] | EG: 15 CG: 15 | UE-FMA | No | A/ES | NIBS | No | Sham Stimulation | Safety (**) | Neg |
| EG: 46 (8–56.8) | |||||||||
| CG: 22.5 (8.8–43.5) | |||||||||
| Dawson, 2021 [49] | EG: 53 CG: 54 | UE-FMA | Yes | C | PS | Yes | Sham Stimulation | UE-FMA | Pos |
| EG: 34.4 ± 8.2 | |||||||||
| CG: 35.7 ± 7.8 | |||||||||
| Llorens, 2021 [50] | EG: 14 CG: 15 | UE-FMA | Yes | C | NIBS, VR and Visual | Yes | Usual Care | UE-FMA | Pos |
| EG: 9.50 ± 5.11 | |||||||||
| CG: 9.87 ± 4.82 | |||||||||
| Cantillo-Negrete, 2021 [51] | 10 crossover study | UE-FMA | Yes | S/C | BCI, Robotic | No | Usual Care | UE-FMA | Neg |
| 17.5 ± 15.3 | |||||||||
| ARAT | |||||||||
| 4.3 ± 6.4 | |||||||||
| Takebayashi, 2022 [52] | EG1: 17 EG2: 13 | UE-FMA | Yes | ES | Robotic | Yes, whenever possible | Different Parameters | UE-FMA WMFT | Pos On Sec |
| EG1: 14.8 ± 7.0 (severe) | |||||||||
| EG2: 20.0 ± 5.6 (severe) | |||||||||
| EG1: 44.8 ± 5.2 (moderate) | |||||||||
| EG2: 46.6 ± 6.8 (moderate) | |||||||||
| Jiang, 2022 [53] | EG: 24 CG: 20 | UE-FMA | Yes | A | PS | No | Usual Care | UE-FMA | Pos |
| EG: 12.38 ± 2.26 | |||||||||
| CG: 12.30 ± 2.39 | |||||||||
| Schrader, 2022 [54] | EG: 14 CG: 10 | UE-FMA | Yes | A/S/C | Robotic | No | Without Technology | UE-FMA (60) | Pos |
| EG: 4.00 (0.75–8.25) | |||||||||
| CG: 3.00 (0.00–4.50) | |||||||||
| Ohnishi, 2022 [55] | EG1: 25 EG2: 22 EG3: 26 CG: 26 | UE-FMA | Yes | ES | PS | Yes | Different Parameters, Usual Care | SIAS UE-FMA MAS FIM | Pos |
| EG1: 4.0 (4.0–9.0) | |||||||||
| EG2: 4.0 (4.0–8.8) | |||||||||
| EG3: 4.0 (3.0–8.8) | |||||||||
| CG: 4.0 (4.0–5.8) | |||||||||
| Huang, 2022 [56] | EG: 13 CG: 11 | UE-FMA | Yes | C | NIBS | No | Sham Stimulation | UE-FMA | Pos On Sec |
| EG: 39.3 ± 17.9 | |||||||||
| CG: 34.2 ± 15.9 | |||||||||
| Wong, 2022 [57] | EG: 15 CG: 15 | UE-FMA | Yes | A/ES | PS | Yes | Without Technology | ARAT | Neg |
| EG: 31 ± 11 | |||||||||
| CG: 35 ± 14 | |||||||||
| ARAT | |||||||||
| EG: 19 ± 11 | |||||||||
| CG: 23 ± 19 | |||||||||
| Cordo, 2022 [58] | EG: 44 CG: 39 | UE-FMA | Yes | ES/S | PS, Robotic | Yes | Different Parameters | UE-FMA | Pos |
| EG: 20.9 ± 9.9 | |||||||||
| CG: 23.7 ± 11.2 | |||||||||
| Takebayashi, 2022 [59] | EG1: 42 EG2: 39 CG: 36 | UE-FMA | Yes | C | Robotic | Yes | Without Technology | UE-FMA | Pos On Sec |
| EG1: 25.9 ± 8.6 | |||||||||
| EG2: 26.5 ± 11.0 | |||||||||
| CG: 25.0 ± 0.9 | |||||||||
| Williamson, 2023 [60] | 8 crossover study | UE-FMA | Yes | ES/S/C | NIBS | No | Different Parameters, Sham Stimulation | UE-FMA | Pos |
| 27.7 ± 16.3 | |||||||||
| Dawson, 2023 [61] | EG: 53 CG: 55 | UE-FMA | Yes | C | PS | Yes | Sham Stimulation | UE-FMA | Pos |
| EG: 34.4 ± 8.2 | |||||||||
| CG: 35.7 ± 7.8 | |||||||||
| Wang, 2023 [62] | EG1: 23 EG2: 23 CG: 23 | UE-FMA | Yes | ES/S | NIBS, Robotic | Yes | Different Technology, Usual care | UE-FMA BI | Pos |
| EG1: 9 (IQR: 12) | |||||||||
| EG2: 11 (IQR: 8) | |||||||||
| CG: 14 (IQR: 16) | |||||||||
| Chen, 2023 [63] | EG: 40 CG: 40 | UE-FMA | Yes | A/ES | Robotic | Yes | Usual Care | UE-FMA | Pos |
| EG: 18.5 ± 10.5 | |||||||||
| CG: 19.4 ± 10.4 | |||||||||
| Feingold-Polak, 2024 [64] | EG1: 10 EG2: 8 CG: 8 | UE-FMA (60) | Yes | S | Robotic | Yes | Different Technology, Usual Care | UE-FMA (60) ARAT MAL SIS | Pos On Sec |
| EG1: 42 (17–53) | |||||||||
| EG2: 41 (17–54) | |||||||||
| CG: 39 (18–58) | |||||||||
| ARAT | |||||||||
| EG1: 36 (15–51) | |||||||||
| EG2: 38 (6–57) | |||||||||
| CG: 33(17–53) | |||||||||
| Brunner, 2024 [65] | EG: 15 CG: 20 | UE-FMA | Yes | A/ES | BCI, PS | No | Usual Care | ARAT | Neg |
| EG: 4 (2–4) | |||||||||
| CG: 4 (2–4) | |||||||||
| ARAT | |||||||||
| EG: 0 (0–0) | |||||||||
| CG: 0 (0–0) |
| Outcome | As Primary Number of Studies | As Secondary Number of Studies |
|---|---|---|
| Upper Extremity Fugl-Meyer Assessment | 38 | 5 |
| Action Research Arm Test | 8 | 8 |
| Wolf Motor Function Test | 3 | 10 |
| Functional Independence Measure | 3 | 2 |
| Modified Ashworth Scale | 2 | 9 |
| Motor Activity Log | 2 | 6 |
| Stroke Impact Scale | 1 | 11 |
| Barthel Index | 1 | 11 |
| Box and Block Test | 1 | 4 |
| Stroke Impairment Assessment Set: knee–mouth and finger function test | 1 | |
| Modified Tardieu Scale | 1 | |
| Goal Attainment Scaling | 2 | |
| Motricity Index | 2 | |
| Medical Research Council Scale | 2 | |
| National Institutes of Health Stroke Scale | 2 | |
| Finger–Nose Test | 1 | |
| Jebsen–Taylor Hand Function Test | 1 | |
| Hamilton Depression Scale | 1 | |
| Mental Rotation Task | 1 | |
| Modified Rankin Scale | 1 | |
| Montreal Cognitive Assessment | 1 | |
| Nine-hole peg test | 1 | |
| Nottingham Sensory Assessment | 1 | |
| Numeric Rating Scale Pain | 1 | |
| Rancho Los Amigos Scale | 1 | |
| Rivermead Assessment of Somatosensory Performance | 1 | |
| Stroke Specific Quality of Life Scale | 1 | |
| Motor Outcome (kinematic, kinetic, electromyographic parameters) | 1 | 10 |
| Brain Outcome (transcranial magnetic stimulation and electroencephalographic parameters) | 5 | |
| Safety (adverse events) | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colamarino, E.; Morone, G.; Toppi, J.; Riccio, A.; Cincotti, F.; Mattia, D.; Pichiorri, F. A Scoping Review of Technology-Based Approaches for Upper Limb Motor Rehabilitation after Stroke: Are We Really Targeting Severe Impairment? J. Clin. Med. 2024, 13, 5414. https://doi.org/10.3390/jcm13185414
Colamarino E, Morone G, Toppi J, Riccio A, Cincotti F, Mattia D, Pichiorri F. A Scoping Review of Technology-Based Approaches for Upper Limb Motor Rehabilitation after Stroke: Are We Really Targeting Severe Impairment? Journal of Clinical Medicine. 2024; 13(18):5414. https://doi.org/10.3390/jcm13185414
Chicago/Turabian StyleColamarino, Emma, Giovanni Morone, Jlenia Toppi, Angela Riccio, Febo Cincotti, Donatella Mattia, and Floriana Pichiorri. 2024. "A Scoping Review of Technology-Based Approaches for Upper Limb Motor Rehabilitation after Stroke: Are We Really Targeting Severe Impairment?" Journal of Clinical Medicine 13, no. 18: 5414. https://doi.org/10.3390/jcm13185414