
Comparison of the Minimally Invasive Reverdin–Isham Lateral Translation Osteotomy Versus the Standard Reverdin–Isham Technique: A Pilot Prospective Cohort Study

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Inclusion and Exclusion Criteria
2.3. Study Variables
2.3.1. Outcome Measures
2.3.2. Exposure: Surgical Techniques
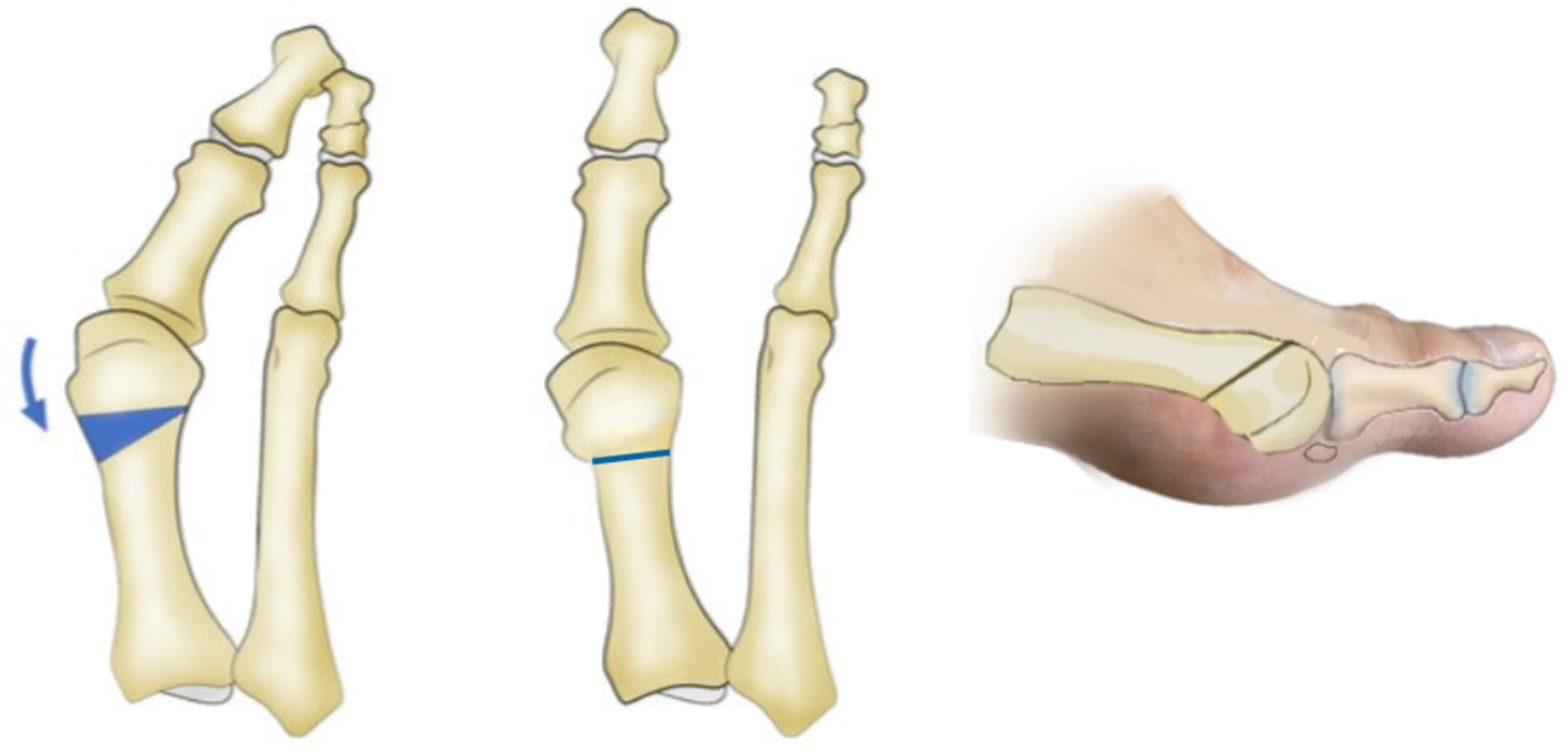
- The standard Reverdin–Isham osteotomy procedure was performed using the Shannon–Isham long burr perpendicular to the axis of the first metatarsal in the sagittal plane [18,19]. The mediolateral inclination in the frontal plane determines the degree of metatarsal shortening. Notably, the lateral cortex of the metatarsal remains preserved (Figure 1). This was accompanied by an adductor tenotomy through a perpendicular incision made with a Beaver 64 knife (Beaver-Visitec International, USA) using fluoroscopy to locate the lateral sesamoid, deepening until locating the adductor muscle. The stabilization of the osteotomy was achieved with a bandage that aligned the metatarsophalangeal joint and with post-surgical footwear, without using osteosynthesis material.
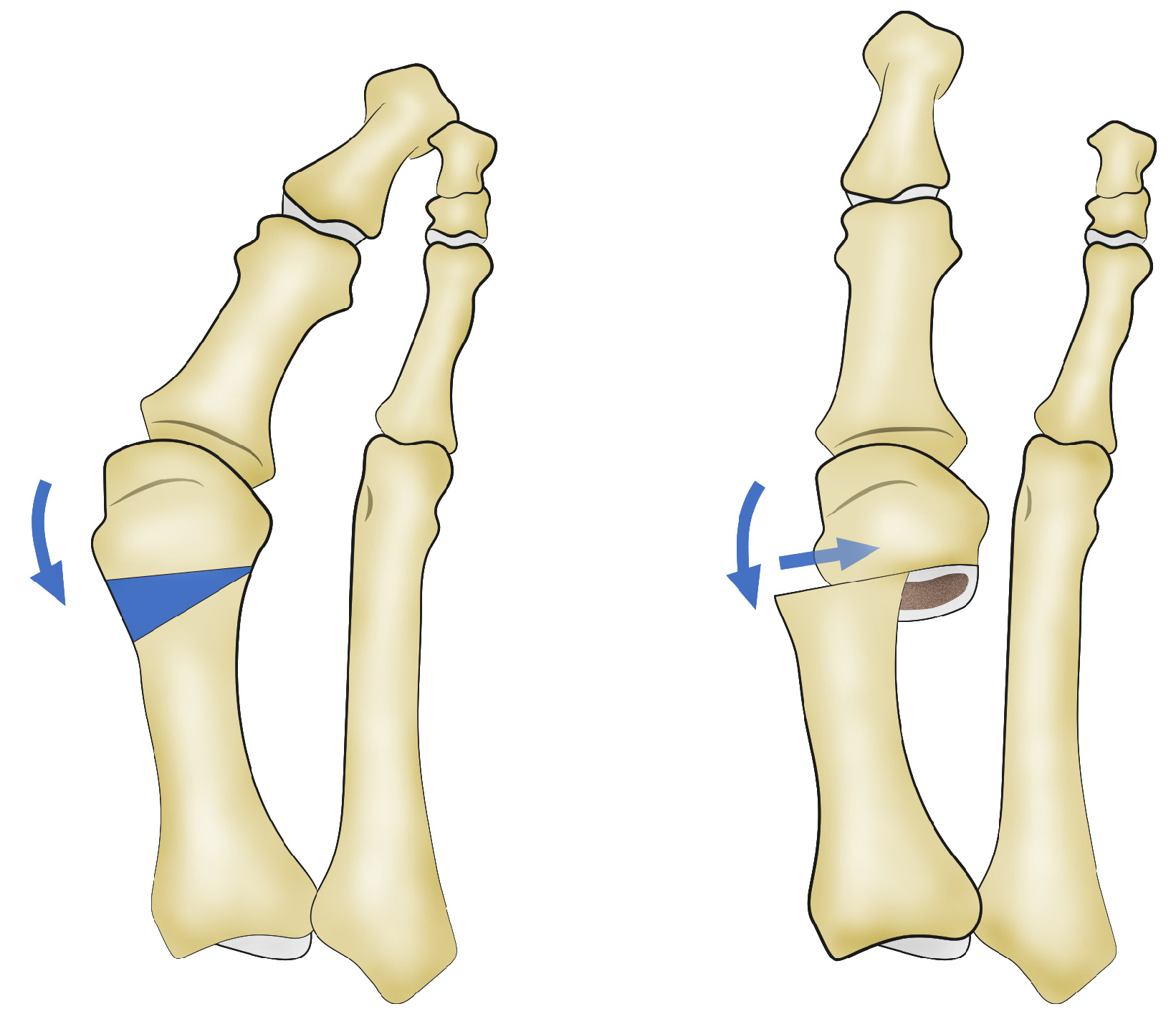
- The Reverdin–Isham lateral translation technique was performed by conducting the standard Reverdin–Isham osteotomy as described above, with the particularity of sectioning the lateral cortex so that the osteotomy of the metatarsal was complete, allowing for the lateral displacement of the metatarsal head toward the inside of the foot. A tenotomy of the adductor, a lateral capsulotomy, and the release of the collateral and suspensory ligaments were performed using the Beaver 64 scalpel (Beaver-Visitec International, Waltham, MA, USA) and a fluoroscope to locate the adductor muscle, following the same procedure as described above (Supplementary Figure S1). In this cohort, the capsulotomy was added through the same incision, locating first the metatarsophalangeal joint interline and making an incision of the dorsolateral phalangeal capsule. This procedure allows the lateral displacement of the head of the first metatarsal (Figure 2, Figure S2 and Figure S3). In cases of severe hallux valgus (Supplementary Figure S4), characterized by the valgus rotation of the metatarsal and a convex lateral cortex (Supplementary Figure S5), the osteotomy is indicated with a shortening design to allow a greater translation of the metatarsal head. This results in a concave lateral cortex and better correction of the intermetatarsal angle. This osteotomy is always accompanied by soft tissue release, as previously described (Supplementary Figure S6). Supplementary Figure S7 shows the anteroposterior view and the weight-bearing anteroposterior X-ray of the right foot with moderate hallux valgus from a patient who underwent a modified Reverdin–Isham osteotomy with lateral translation, before surgery and 6 months after surgery.
2.4. Follow Up
2.5. Sample Size
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cai, Y.; Song, Y.; He, M.; He, W.; Zhong, X.; Wen, H.; Wei, Q. Global prevalence and incidence of hallux valgus: A systematic review and meta-analysis. J. Foot Ankle Res. 2023, 16, 63. [Google Scholar] [CrossRef] [PubMed]
- Baravarian, B.; Briskin, G.B.; Burns, P. Buninectomía de Lapidus: Arthrosis rodesis de ls primera articulación, etatarsocuniforme. Clin. Podiatr. Med. Surg. 2004, 21, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Biz, C.; Corradin, M.; Petretta, I.; Aldegheri, R. Endolog technique for correction of hallux valgus: A prospective study of 30 patients with 4-year follow-up. J. Orthop. Surg. Res. 2015, 10, 102. [Google Scholar] [CrossRef] [PubMed]
- Maffulli, N.; Longo, U.G.; Marinozzi, A.; Denaro, V. Hallux valgus: Effectiveness and safety of minimally invasive surgery. A systematic review. Br. Med. Bull. 2011, 97, 149–167. [Google Scholar] [CrossRef]
- Trnk, H.J. Osteotomás para la corrección del hallux valgus. Foot Ankle Clin. N. Am. 2005, 10, 15–33. [Google Scholar] [CrossRef]
- Bosch, P.; Markowski, H.; Rannicher, V. Technik und erste ergebnisse osteotomia del metatarsiano I subkutanen distal. Orthop. Praxis 1990, 26, 51–56. [Google Scholar]
- Del Vecchio, J.J.; Ghioldi, M.E. Evolution of Minimally Invasive Surgery in Hallux Valgus. Foot Ankle Clin. 2020, 25, 79–95. [Google Scholar] [CrossRef]
- Caravelli, S.; Mosca, M.; Massimi, S.; Costa, G.G.; Lo Presti, M.; Fuiano, M.; Grassi, A.; Zaffagnini, S. Percutaneous treatment of hallux valgus: What’s the evidence? A systematic review. Musculoskelet. Surg. 2018, 102, 111–117. [Google Scholar] [CrossRef]
- Castellà, J.M.C.; Perich, B.C.; Sánchez, L.C.; López, R.E.G.; Segura, E.R.H.; Isham, S.A.; Gutiérrez, R.L.; Freixas, J.L.; Martínez, L.M.M.; Esteban, J.M.; et al. Cirugía Minimamente Invasiva del Pie; Glosa, Ed.; Fundación Dialnet: Logroño, Spain, 2017; pp. 29–33. [Google Scholar]
- Ji, L.; Wang, K.; Ding, S.; Sun, C.; Sun, S.; Zhang, M. Minimally Invasive vs. Open Surgery for Hallux Valgus: A Meta-Analysis. Front. Surg. 2022, 9, 843410. [Google Scholar] [CrossRef]
- Lewis, T.L.; Robinson, P.W.; Ray, R.; Dearden, P.M.C.; Goff, T.A.J.; Watt, C.; Lam, P. Five-Year Follow-up of Third-Generation Percutaneous Chevron and Akin Osteotomies (PECA) for Hallux Valgus. Foot Ankle Int. 2023, 44, 104–117. [Google Scholar] [CrossRef]
- Yousaf, A.; Saleem, J.; Al-Hilfi, L.; Kunasingam, K. Third-Generation Minimally Invasive Chevron Akin Osteotomy for Hallux Valgus: Three-Year Outcomes. Indian J. Orthop. 2023, 57, 1105–1111. [Google Scholar] [CrossRef] [PubMed]
- Malagelada, F.; Sahirad, C.; Dalmau-Pastor, M.; Vega, J.; Bhumbra, R.; Manzanares-Céspedes, M.C.; Laffenêtre, O. Minimally invasive surgery for hallux valgus: A systematic review of current surgical techniques. Int. Orthop. 2019, 43, 625–637. [Google Scholar] [CrossRef] [PubMed]
- Coughlin, M.J.; Mann, R.A. Hallux valgus. In Surgery of the foot and Ankle, 7th ed.; Mosby: St. Louis, MO, USA, 1999; pp. 150–362. [Google Scholar]
- Payo Ollero, J.; Montiel Terrón, V.; Alfonso Olmos García, M.; Villas Tomé, C. Resultado funcional esperable tras una artrodesis bilateral de tobillo. Valoración de 3 casos y revisión de la literature [Functional outcome expected after a bilateral ankle arthrodesis. Assessment of 3 cases and review of the literature]. Rev. Pie Tobillo. 2018, 32, 35–42. [Google Scholar]
- Kitaoka, H.B.; Alexander, I.J.; Adelaar, R.S.; Nunley, J.A.; Myerson, M.S.; Sanders, M. Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int. 1994, 15, 349–353. [Google Scholar] [CrossRef]
- Schneider, W.; Jurenitsch, S. Normative data for the American Orthopedic Foot and Ankle Society ankle-hindfoot, midfoot, hallux and lesser toes clinical rating system. Int. Orthop. 2016, 40, 301–306. [Google Scholar] [CrossRef]
- Severyns, M.; Carret, P.; Brunier-Agot, L.; Debandt, M.; Odri, G.A.; Rouvillain, J.L. Reverdin-Isham procedure for mild or moderate hallux valgus: Clinical and radiographic outcomes. Musculoskelet. Surg. 2019, 103, 161–166. [Google Scholar] [CrossRef]
- Biz, C.; Fosser, M.; Dalmau-Pastor, M.; Corradin, M.; Rodà, M.G.; Aldegheri, R.; Ruggieri, P. Functional and radiographic outcomes of hallux valgus correction by mini-invasive surgery with Reverdin-Isham and Akin percutaneous osteotomies: A longitudinal prospective study with a 48-month follow-up. J. Orthop. Surg. Res. 2016, 11, 157. [Google Scholar] [CrossRef]
- Portaluri, M. Hallux valgus correction by the method of Bosch: A clinical evaluation. Foot Ankle Clin. 2000, 5, 499–511. [Google Scholar]
- Magnan, B.; Samaila, E.; Viola, G.; Bartolozzi, P. Minimally invasive retrocapital osteotomy of the first metatarsal in hallux valgus deformity. Oper. Orthop. Traumatol. 2008, 20, 89–96. [Google Scholar] [CrossRef]
- Giannini, S.; Faldini, C.; Vannini, F.; Bevoni, R.; Biagini, C. Surgical treatment of hallux valgus: A clinical prospective randomized study comparing linear distal metatarsal osteotomy with scarf osteotomy. Orthop. Proc. 2009, 91-B (Suppl. 1), 162. [Google Scholar] [CrossRef]
- Bia, A.; Guerra-Pinto, F.; Pereira, B.S.; Corte-Real, N.; Oliva, X.M. Percutaneous Osteotomies in Hallux Valgus: A Systematic Review. J. Foot Ankle Surg. 2018, 57, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Trnka, H.; Krenn, S.; Schuh, R. Minimally invasive hallux valgus surgery: A critical review of the evidence. Int. Orthop. 2013, 37, 1731–1735. [Google Scholar] [CrossRef] [PubMed]
- Meier, P.J.; Kenzora, J.E. The risks and benefits of distal first metatarsal osteotomies. Foot Ankle. 1985, 6, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Laughlin, T.J. Complications of distal first metatarsal osteotomies. Foot Ankle Surg. 1996, 34, 524–531. [Google Scholar] [CrossRef]
- Bauer, T.; Biau, D.; Lortat-Jacob, A.; Hardy, P. Percutaneous hallux valgus correction using the Reverdin-Isham osteotomy. Orthop. Traumatol. Surg. Res. 2010, 96, 407–416. [Google Scholar] [CrossRef]
- Baumhauer, J.F.; Nawoczenski, D.A.; DiGiovanni, B.F.; Wilding, G.E. Reliability and validity of the american orthopaedic foot and ankle society clinical eating scales: A pilot study for the hallux and lesser toes. Foot Ankle Int. 2006, 27, 1014–1019. [Google Scholar] [CrossRef]
- Shazadeh Safavi, P.; Janney, C.; Jupiter, D.; Kunzler, D.; Bui, R.; Panchbhavi, V.K. A Systematic Review of the Outcome Evaluation Tools for the Foot and Ankle. Foot Ankle Spec. 2019, 12, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Leigheb, M.; Vaiuso, D.; Rava, E.; Pogliacomi, F.; Samaila, E.M.; Grassi, F.A.; Sabbatini, M. Translation, cross-cultural adaptation, reliability, and validation of the Italian version of the American Orthopaedic Foot and Ankle Society—MetaTarsoPhalangeal-InterPhalangeal Scale (AOFAS-MTP-IP) for the hallux. Acta Biomed. 2019, 90 (Suppl. 12), 118–126. [Google Scholar] [CrossRef]
- SooHoo, N.F.; Shuler, M.; Fleming, L.L. Evaluation of the validity of the AOFAS clinical rating systems by correlation to the SF-36. Foot Ankle Int. 2003, 24, 50–55. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Total Sample n = 60 | RIT Cohort n = 30 | RI Cohort n = 30 | |||
|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | p-Value a | ||
| Sex | Male | 6 (10.0) | 2 (6.7) | 4 (13.3) | 0.671 |
| Female | 54 (90.0) | 28 (93.3) | 26 (86.7) | ||
| Foot | Right | 29 (48.3) | 15 (50) | 14 (46.7) | 0.796 |
| Left | 31 (51.7) | 15 (50) | 16 (53.3) | ||
| Bunion | No | 3 (5.0) | 2 (6.7) | 1 (3.3) | 1.000 |
| Yes | 57 (95.0) | 28 (93.3) | 29 (96.7) | ||
| Paresthesia | No | 40 (66.7) | 22 (73.3) | 18 (60) | 0.273 |
| Yes | 20 (33.3) | 8 (26.7) | 12 (40) | ||
| Pressure pain | No | 7 (11.7) | 6 (20) | 1 (3.3) | 0.044 |
| Yes | 53 (88.3) | 24 (80) | 29 (96.7) | ||
| Altered MTF mobility | No | 9 (15.0) | 7 (23.3) | 2 (6.7) | 0.145 |
| Yes | 51 (85.0 | 23 (76.7) | 28 (93.3) | ||
| Transfer of central metatarsal load | No | 20 (33.3) | 3 (10) | 17 (56.7) | <0.001 |
| Yes | 40 (66.7) | 27 (90) | 13 (43.3) | ||
| Metatarsal index | Index Minus | 41 (68.3) | 19 (63.3) | 22 (73.3) | 0.028 |
| Index Plus | 4 (6.7) | 0 (0) | 4 (13.3) | ||
| Index Plus-Minus | 15 (25%) | 11 (36.7) | 4 (13.3) | ||
| RIT Cohort (n = 30) | RI Cohort (n = 30) | p-Value c | |
|---|---|---|---|
| Pain (VAS) a | |||
| Preoperative | 8.33, SD 0.84 (7–10) | 7.17, SD 0.83 (5–8) | |
| Postoperative | 1.17, SD 1.23 (0–6) | 0.47, SD 0.73 (0–2) | |
| p value b | <0.001 | <0.001 | |
| Difference | −7.17 | −6.70 | 0.137 |
| AOFAS score a | |||
| Preoperative | 41.07, SD 15.49 (5–70) | 51.33, SD 16.20 (5–80) | |
| Postoperative | 88.33, SD 7.73 (73–100) | 93.83, SD 9.38 (70–100) | |
| p value b | <0.001 | <0.001 | |
| Difference | 47.27 | 42.50 | 0.203 |
| MPA a | |||
| Preoperative | 33.40, SD 12.48 (2–54) | 23.80, SD 7.84 (11–42) | |
| Postoperative | 10.27, SD 3.62 (3–20) | 10.60, SD 3.46 (3–18) | |
| p value b | <0.001 | <0.001 | |
| Difference | −23.13 | −13.20 | <0.001 |
| IMA a | |||
| Preoperative | 17.03, SD 4.65 (10–34) | 12.53, SD 2.73 (8–18) | |
| Postoperative | 11.10, SD 2.83 (8–21) | 9.23, SD 0.82 (8–11) | |
| p value b | <0.001 | <0.001 | |
| Difference | −5.93 | −3.30 | 0.001 |
| PASA a | |||
| Preoperative | 13.10, SD 6.18 (7–41) | 7.50, SD 2.45 (4–14) | |
| Postoperative | 5.87, SD 1.93 (2–9) | 2.37, SD 1.40 (0–5) | |
| p value b | <0.001 | <0.001 | |
| Difference | −7.23 | −5.13 | 0.201 |
| DASA a | |||
| Preoperative | 10.87, SD 4.48 (2–19) | 7.53, SD 2.97 (4–16) | |
| Postoperative | 5.23, SD 2.31 (1–11) | 2.00, SD 1.78 (0–5) | |
| p value b | <0.001 | <0.001 | |
| Difference | −5.63 | −5.53 | 0.964 |
| Sesamoid position a | |||
| Preoperative | 6.00, SD 1.34 (1–7) | 2.80, SD 1.37 (1–7) | |
| Postoperative | 1.77, SD 0.68 (1–3) | 1.23, SD 0.43 (1–2) | |
| p value b | <0.001 | <0.001 | |
| Difference | −4.23 | −1.57 | <0.001 |
| Raw Adjustment | Multivariate Adjustment | |||||||
|---|---|---|---|---|---|---|---|---|
| Betas | Error | p-Value | Betas | Error | p-Value | % R2 | ||
| DELTA_Pain (VAS) | Intercept | −6.70 | 0.21 | <0.001 | −7.29 | 0.81 | <0.001 | 0.6 |
| RIT | −0.47 | 0.31 | 0.135 | −0.36 | 0.37 | 0.335 | ||
| DELTA_Total AOFAS score | Intercept | 42.50 | 2.46 | <0.001 | 33.21 | 8.98 | <0.001 | 3.9 |
| RIT | 4.77 | 3.48 | 0.177 | 1.05 | 4.06 | 0.795 | ||
| DELTA_MPA | Intercept | −13.20 | 1.68 | <0.001 | 0.19 | 5.89 | 0.974 | 29.4 |
| RIT | −9.93 | 2.38 | <0.001 | −7.23 | 2.66 | 0.009 | ||
| DELTA_IMA | Intercept | −3.30 | 0.53 | <0.001 | −1.37 | 1.92 | 0.477 | 19.8 |
| RIT | −2.63 | 0.75 | <0.001 | −3.63 | 0.87 | <0.001 | ||
| DELTA_PASA | Intercept | −5.13 | 0.95 | <0.001 | −6.90 | 3.57 | 0.060 | 2.5 |
| RIT | −2.10 | 1.34 | 0.124 | −2.28 | 1.61 | 0.164 | ||
| DELTA_DASA | Intercept | −5.53 | 0.62 | <0.001 | −7.01 | 2.36 | 0.004 | 5.2 |
| RIT | −0.10 | 0.89 | 0.911 | 0.35 | 1.06 | 0.743 | ||
| DELTA_Sesamoid_Position | Intercept | −1.56 | 0.23 | <0.001 | −2.00 | 0.83 | 0.02 | 54.5 |
| RIT | −2.66 | 0.32 | <0.001 | −2.25 | 0.37 | <0.001 | ||
| Study | Technique | MPA Improvement | IMA Improvement | PASA Improvement | AOFAS Score Improvement |
|---|---|---|---|---|---|
| Present Study | Reverdin–Isham (Standard) | 13.20 | 3.30 | 5.13 | 42.50 |
| Reverdin–Isham with Lateral Translation (RIT) | 23.13 | 5.93 | 7.23 | 47.27 | |
| Malagelada et al. [13] | Reverdin–Isham | 8.6–17.1 | 0.9–5.2 | NR | 33.1–49.8 |
| Bösch | 10–19.7 | 4.8–9.6 | NR | 30.2–53.7 | |
| Bia et al. [23] | Reverdin–Isham | 9.3–15 | 0.2–5 | NR | 35.2–45 |
| Bösch (Percutaneous) | 19.6 | 9.5 | NR | 42.2 | |
| Caravelli et al. [8] | Bösch | 16.5 | 6 | NR | 20 |
| Reverdin–Isham | 14 | 3 | NR | 20 | |
| Trnka et al. [24] | Bösch | 17–20.9 | 3–3.5 | NR | NR |
| Reverdin–Isham | 18.9 | 4 | NR | 41 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belda-Donat, M.; Marti-Martinez, L.M.; Lorca-Gutierrez, R.; Naranjo-Ruiz, C.; Chacón-Giráldez, F.; Barrios, C. Comparison of the Minimally Invasive Reverdin–Isham Lateral Translation Osteotomy Versus the Standard Reverdin–Isham Technique: A Pilot Prospective Cohort Study. J. Clin. Med. 2024, 13, 5468. https://doi.org/10.3390/jcm13185468
Belda-Donat M, Marti-Martinez LM, Lorca-Gutierrez R, Naranjo-Ruiz C, Chacón-Giráldez F, Barrios C. Comparison of the Minimally Invasive Reverdin–Isham Lateral Translation Osteotomy Versus the Standard Reverdin–Isham Technique: A Pilot Prospective Cohort Study. Journal of Clinical Medicine. 2024; 13(18):5468. https://doi.org/10.3390/jcm13185468
Chicago/Turabian StyleBelda-Donat, Maria, Luis M. Marti-Martinez, Rubén Lorca-Gutierrez, Carmen Naranjo-Ruiz, Fernando Chacón-Giráldez, and Carlos Barrios. 2024. "Comparison of the Minimally Invasive Reverdin–Isham Lateral Translation Osteotomy Versus the Standard Reverdin–Isham Technique: A Pilot Prospective Cohort Study" Journal of Clinical Medicine 13, no. 18: 5468. https://doi.org/10.3390/jcm13185468
APA StyleBelda-Donat, M., Marti-Martinez, L. M., Lorca-Gutierrez, R., Naranjo-Ruiz, C., Chacón-Giráldez, F., & Barrios, C. (2024). Comparison of the Minimally Invasive Reverdin–Isham Lateral Translation Osteotomy Versus the Standard Reverdin–Isham Technique: A Pilot Prospective Cohort Study. Journal of Clinical Medicine, 13(18), 5468. https://doi.org/10.3390/jcm13185468