
High-Density Lipoprotein-Associated Paraoxonase-1 (PON-1) and Scavenger Receptor Class B Type 1 (SRB-1) in Coronary Artery Disease: Correlation with Disease Severity

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Material and Methods
2.1. Sample Collection and Serum Isolation
2.2. Biochemical Examination
2.3. Enzyme-Linked Immunosorbent Assay for PON-1 and SRB-1
2.4. Statistical Analysis
3. Results
3.1. Demographic and Baseline Characteristics of the Patients and Controls
3.2. Lipid Parameters and PON-1 and SRB-1 in Cases and Controls
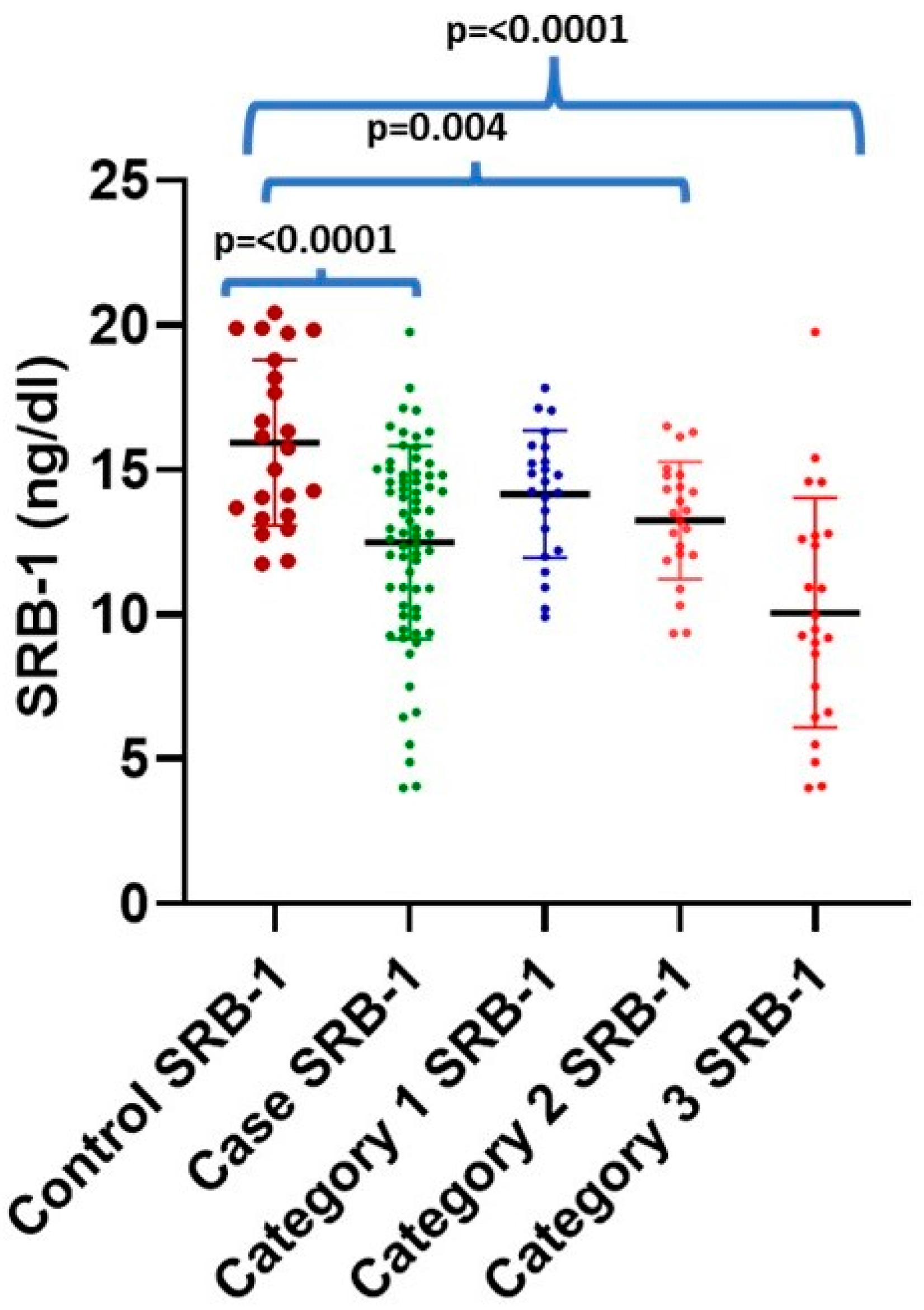
3.3. Intergroup Comparison of PON-1 and SRB-1 with Different Categories of CAD and Normal Control
3.4. Association of PON-1 and SRB-1 Level with Demographic Characteristics
3.5. Diagnostic Value of PON-1 and SRB-1 in Discriminating Cases from Controls
3.6. Diagnostic Value of SRB-1
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rao, G.H. Number one killer: Vascular disease. Ann. Clin. Diabetes Endocrinol. 2018, 1, 1008. [Google Scholar]
- Prabhakaran, D.; Jeemon, P.; Roy, A. Cardiovascular diseases in India: Current epidemiology and future directions. Circulation 2016, 133, 1605–1620. [Google Scholar] [CrossRef] [PubMed]
- Kratzer, A.; Giral, H.; Landmesser, U. High-density lipoproteins as modulators of endothelial cell functions: Alterations in patients with coronary artery disease. Cardiovasc. Res. 2014, 103, 350–361. [Google Scholar] [CrossRef] [PubMed]
- Kontush, A.; Chapman, M.J. Functionally defective high-density lipoprotein: A novel therapeutic target at the crossroads of dyslipidemia, inflammation, and atherosclerosis. Pharmacol. Rev. 2006, 58, 342–374. [Google Scholar] [CrossRef] [PubMed]
- Gong, M.; Wilson, M.; Kelly, T.; Su, W.; Dressman, J.; Kincer, J.; Matveev, S.V.; Guo, L.; Guerin, T.; Li, X.A.; et al. HDL-associated estradiol stimulates endothelial NO synthase and vasodilation in an SR-BI–dependent manner. J. Clin. Investig. 2003, 111, 1579–1587. [Google Scholar] [CrossRef]
- Mackness, B.; Durrington, P.N.; Mackness, M.I. Paraoxonase gene family and coronary heart disease. Curr. Opin. Lipidol. 2002, 13, 357–362. [Google Scholar] [CrossRef]
- Durrington, P.N.; Mackness, B.; Mackness, M.I. Paraoxonase and atherosclerosis. Arter. Thromb. Vasc. Biol. 2001, 21, 473–480. [Google Scholar] [CrossRef]
- McElveen, J.; Mackness, M.I.; Colley, C.M.; Peard, T.; Warner, S.; Walker, C.H. Distribution of paraoxon hydrolytic activity in the serum of patients after myocardial infarction. Clin. Chem. 1986, 32, 671–673. [Google Scholar] [CrossRef]
- Patra, S.K.; Singh, K.; Singh, R. Paraoxonase-1: A better atherosclerotic risk predictor than HDL in type 2 diabetes mellitus. Diabetes Metab. Syndr. Clin. Res. Rev. 2013, 7, 108–111. [Google Scholar] [CrossRef]
- Esparragón, F.R.; Trujillo, Y.H.; Reyes, A.M.; Ortega, E.H.; Medina, A.; Pérez, J.C. Concerning the significance of paraoxonase-1 and SRB-1 genes in atherosclerosis. Rev. Española Cardiol. 2006, 59, 154–164. [Google Scholar]
- McCarthy, J.J.; Lehner, T.; Reeves, C.; Moliterno, D.J.; Newby, L.K.; Rogers, W.J.; Topol, E.J. Association of genetic variants in the HDL receptor, SRB-1, with abnormal lipids in women with coronary artery disease. J. Med. Genet. 2003, 40, 453–458. [Google Scholar] [CrossRef] [PubMed]
- Saddar, S.; Carriere, V.; Lee, W.R.; Tanigaki, K.; Yuhanna, I.S.; Parathath, S.; Morel, E.; Warrier, M.; Sawyer, J.K.; Gerard, R.D.; et al. Scavenger receptor class B type I is a plasma membrane cholesterol sensor. Circ. Res. 2013, 112, 140–151. [Google Scholar] [CrossRef]
- Zhang, Y.; Da Silva, J.R.; Reilly, M.; Billheimer, J.T.; Rothblat, G.H.; Rader, D.J. Hepatic expression of scavenger receptor class B type I (SR-BI) is a positive regulator of macrophage reverse cholesterol transport in vivo. J. Clin. Investig. 2005, 115, 2870–2874. [Google Scholar] [CrossRef] [PubMed]
- King, S.B., III; Smith, S.C., Jr.; Hirshfeld, J.W., Jr.; Jacobs, A.K.; Morrison, D.A.; Williams, D.O.; Feldman, T.E.; Kern, M.J.; O’Neill, W.W.; Schaff, H.V.; et al. 2007 Focused Update of the ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines: 2007 Writing Group to Review New Evidence and Update the ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention, Writing on Behalf of the 2005 Writing Committee. Circulation 2008, 117, 261–295. [Google Scholar]
- Joshi, P.; Islam, S.; Pais, P.; Reddy, S.; Dorairaj, P.; Kazmi, K.; Pandey, M.R.; Haque, S.; Mendis, S.; Rangarajan, S.; et al. Risk factors for early myocardial infarction in South Asians compared with individuals in other countries. JAMA 2007, 297, 286–294. [Google Scholar] [CrossRef]
- Geldsetzer, P.; Manne-Goehler, J.; Theilmann, M.; Davies, J.I.; Awasthi, A.; Danaei, G.; Gaziano, T.A.; Vollmer, S.; Jaacks, L.M.; Baernighausen, T.; et al. Geographic and sociodemographic variation of cardiovascular disease risk in India: A cross-sectional study of 797,540 adults. PLoS Med. 2018, 15, e1002581. [Google Scholar] [CrossRef] [PubMed]
- Sun, T.; Hu, J.; Yin, Z.; Xu, Z.; Zhang, L.; Fan, L.; Zhuo, Y.; Wang, C. Low serum paraoxonase-1 activity levels predict coronary artery disease severity. Oncotarget 2017, 8, 19443. [Google Scholar] [CrossRef] [PubMed]
- Iaccarino, G.; Ciccarelli, M.; Sorriento, D.; Galasso, G.; Campanile, A.; Santulli, G.; Cipolletta, E.; Cerullo, V.; Cimini, V.; Altobelli, G.G.; et al. Ischemic neoangiogenesis enhanced by β2-adrenergic receptor overexpression: A novel role for the endothelial adrenergic system. Circ. Res. 2005, 97, 1182–1189. [Google Scholar] [CrossRef]
- Gupta, N.; Singh, S.; Maturu, V.N.; Sharma, Y.P.; Gill, K.D. Paraoxonase-1 (PON-1) polymorphisms, haplotypes and activity in predicting cad risk in North-West Indian Punjabis. PLoS ONE 2011, 6, e17805. [Google Scholar] [CrossRef]
- Litvinov, D.; Mahini, H.; Garelnabi, M. Antioxidant and anti-inflammatory role of paraoxonase-1: Implication in arteriosclerosis diseases. N. Am. J. Med. Sci. 2012, 4, 523. [Google Scholar]
- Fortunato, G.; Rubba, P.; Panico, S.; Trono, D.; Tinto, N.; Mazzaccara, C.; De Michele, M.; Iannuzzi, A.; Vitale, D.F.; Salvatore, F.; et al. A paraoxonase gene polymorphism, PON-1 (55), as an independent risk factor for increased carotid intima-media thickness in middle-aged women. Atherosclerosis 2003, 167, 141–148. [Google Scholar] [CrossRef]
- Coombes, R.H.; Crow, J.A.; Dail, M.; Chambers, H.W.; Wills, R.W.; Chambers, J.E.; Bertolet, B.D. for CARe. Relationship of Human Paraoxonase-1 (PON-1) Serum Activity and Genotype with Atherosclerosis in Individuals from the Deep South. Pharmacogenet. Genom. 2011, 21, 867. [Google Scholar] [CrossRef] [PubMed]
- Bhaskar, S.; Ganesan, M.; Chandak, G.R.; Mani, R.; Idris, M.M.; Khaja, N.; Gulla, S.; Kumar, U.; Movva, S.; Vattam, K.K.; et al. Association of PON-1 and APOA 5 gene polymorphisms in a cohort of Indian patients having coronary artery disease with and without type 2 diabetes. Genet. Test. Mol. Biomark. 2011, 15, 507–512. [Google Scholar] [CrossRef]
- Efrat, M.; Aviram, M. Macrophage paraoxonase-1 (PON-1) binding sites. Biochem. Biophys. Res. Commun. 2008, 376, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, Z.; Babaei, S.; Maguire, G.F.; Draganov, D.; Kuksis, A.; La Du, B.N.; Connelly, P.W. Paraoxonase-1 reduces monocyte chemotaxis and adhesion to endothelial cells due to oxidation of palmitoyl, linoleoyl glycerophosphorylcholine. Cardiovasc. Res. 2003, 57, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Chistiakov, D.A.; Melnichenko, A.A.; Orekhov, A.N.; Bobryshev, Y.V. Paraoxonase and atherosclerosis-related cardiovascular diseases. Biochimie 2017, 132, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Mackness, M.I.; Arrol, S.; Mackness, B.; Durrington, P.N. Alloenzymes of paraoxonase and effectiveness of high-density lipoproteins in protecting low-density lipoprotein against lipid peroxidation. Lancet 1997, 349, 851–852. [Google Scholar] [CrossRef]
- Out, R.; Hoekstra, M.; Spijkers, J.A.; Kruijt, J.K.; van Eck, M.; Bos, I.S.; Twisk, J.; Van Berkel, T.J. Scavenger receptor class B type I is solely responsible for the selective uptake of cholesteryl esters from HDL by the liver and the adrenals in mice. J. Lipid Res. 2004, 45, 2088–2095. [Google Scholar] [CrossRef]
- Ji, Y.; Wang, N.; Ramakrishnan, R.; Sehayek, E.; Huszar, D.; Breslow, J.L.; Tall, A.R. Hepatic scavenger receptor BI promotes rapid clearance of high-density lipoprotein free cholesterol and its transport into bile. J. Biol. Chem. 1999, 274, 33398–33402. [Google Scholar] [CrossRef]
- Varban, M.L.; Rinninger, F.; Wang, N.; Fairchild-Huntress, V.; Dunmore, J.H.; Fang, Q.; Gosselin, M.L.; Dixon, K.L.; Deeds, J.D.; Acton, S.L.; et al. Targeted mutation reveals a central role for SR-BI in hepatic selective uptake of high-density lipoprotein cholesterol. Proc. Natl. Acad. Sci. USA 1998, 95, 4619–4624. [Google Scholar] [CrossRef]
- Rigotti, A.; Trigatti, B.L.; Penman, M.; Rayburn, H.; Herz, J.; Krieger, M. A targeted mutation in the murine gene encoding the high-density lipoprotein (HDL) receptor scavenger receptor class B type I reveals its key role in HDL metabolism. Proc. Natl. Acad. Sci. USA 1997, 94, 12610–12615. [Google Scholar] [CrossRef] [PubMed]
- Braun, A.; Trigatti, B.L.; Post, M.J.; Sato, K.; Simons, M.; Edelberg, J.M.; Rosenberg, R.D.; Schrenzel, M.; Krieger, M. Loss of SR-BI expression leads to the early onset of occlusive atherosclerotic coronary artery disease, spontaneous myocardial infarctions, severe cardiac dysfunction, and premature death in apolipoprotein E–deficient mice. Circ. Res. 2002, 90, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Covey, S.D.; Krieger, M.; Wang, W.; Penman, M.; Trigatti, B.L. Scavenger receptor class B type I–mediated protection against atherosclerosis in LDL receptor–negative mice involve its expression in bone marrow–derived cells. Arter. Thromb. Vasc. Biol. 2003, 23, 1589–1594. [Google Scholar] [CrossRef]
- Huszar, D.; Varban, M.L.; Rinninger, F.; Feeley, R.; Arai, T.; Fairchild-Huntress, V.; Donovan, M.J.; Tall, A.R. Increased LDL Cholesterol and Atherosclerosis in LDL Receptor–Deficient Mice with Attenuated Expression of Scavenger Receptor B1. Arter. Thromb. Vasc. Biol. 2000, 20, 1068–1073. [Google Scholar] [CrossRef]
- Wang, N.; Arai, T.; Ji, Y.; Rinninger, F.; Tall, A.R. Liver-specific overexpression of scavenger receptor BI decreases levels of very low-density lipoprotein ApoB, low-density lipoprotein ApoB, and high-density lipoprotein in transgenic mice. J. Biol. Chem. 1998, 273, 32920–32926. [Google Scholar] [CrossRef]
- Ueda, Y.; Royer, L.; Gong, E.; Zhang, J.; Cooper, P.N.; Francone, O.; Rubin, E.M. Lower plasma levels and accelerated clearance of high-density lipoprotein (HDL) and non-HDL cholesterol in scavenger receptor class B type I transgenic mice. J. Biol. Chem. 1999, 274, 7165–7171. [Google Scholar] [CrossRef]
- Webb, N.R.; de Beer, M.C.; Yu, J.; Kindy, M.S.; Daugherty, A.; van der Westhuyzen, D.R.; de Beer, F.C. Overexpression of SR-BI by adenoviral vector promotes clearance of apoA-I, but not apoB, in human apoB transgenic mice. J. Lipid Res. 2002, 43, 1421–1428. [Google Scholar] [CrossRef] [PubMed]
- Kozarsky, K.F.; Donahee, M.H.; Rigotti, A.; Iqbal, S.N.; Edelman, E.R.; Krieger, M. Overexpression of the HDL receptor SR-BI alters plasma HDL and bile cholesterol levels. Nature 1997, 387, 414–417. [Google Scholar] [CrossRef] [PubMed]
- Kozarsky, K.F.; Donahee, M.H.; Glick, J.M.; Krieger, M.; Rader, D.J. Gene transfer and hepatic overexpression of the HDL receptor SR-BI reduces atherosclerosis in the cholesterol-fed LDL receptor–deficient mouse. Arter. Thromb. Vasc. Biol. 2000, 20, 721–727. [Google Scholar] [CrossRef]
- Zanoni, P.; Khetarpal, S.A.; Larach, D.B.; Hancock-Cerutti, W.F.; Millar, J.S.; Cuchel, M.; DerOhannessian, S.; Kontush, A.; Surendran, P.; Saleheen, D.; et al. Rare variant in scavenger receptor BI raises HDL cholesterol and increases risk of coronary heart disease. Science 2016, 351, 1166–1171. [Google Scholar] [CrossRef]
- Koenig, S.N.; Sucharski, H.C.; Jose, E.M.; Dudley, E.K.; Madiai, F.; Cavus, O.; Argall, A.D.; Williams, J.L.; Murphy, N.P.; Keith, C.B.; et al. Inherited variants in SCARB1 cause severe early onset coronary artery disease. Circ. Res. 2021, 129, 296–307. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Chambliss, K.L.; Gao, X.; Yuhanna, I.S.; Behling-Kelly, E.; Bergaya, S.; Ahmed, M.; Michaely, P.; Luby-Phelps, K.; Darehshouri, A.; et al. SRB-1 drives endothelial cell LDL transcytosis via DOCK4 to promote atherosclerosis. Nature 2019, 569, 565–569. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Li, L.; Liu, R.; Song, Y.; Zhang, X.; Niu, W.; Kumar, A.K.; Guo, Z.; Hu, Z. Obesity-induced overexpression of miRNA-24 regulates cholesterol uptake and lipid metabolism by targeting SRB-1. Gene 2018, 668, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Shen, W.J.; Azhar, S.; Kraemer, F.B. SRB-1: A unique multifunctional receptor for cholesterol influx and efflux. Annu. Rev. Physiol. 2018, 80, 95–116. [Google Scholar] [CrossRef]
- Jiang, C. The Role of SRB-1 in Lipid Metabolism and Inflammation in 3T3-L1 Adipocytes. Available online: https://opencommons.uconn.edu/usp_projects/35 (accessed on 13 August 2024).
- Perrone, M.A.; Donatucci, B.; Salvati, A.; Gualtieri, P.; De Lorenzo, A.; Romeo, F.; Bernardini, S. Inflammation, oxidative stress and gene expression: The postprandial approach in professional soccer players to reduce the risk of muscle injuries and early atherosclerosis. Med. Sport 2019, 72, 234–243. [Google Scholar] [CrossRef]
- López-Candales, A.; Sawalha, K. Improving diagnostic assessments in the ever-changing landscape of atherosclerosis. J. Cardiovasc. Med. 2023, 24, 221–229. [Google Scholar] [CrossRef]
- Perrone, M.A.; Gualtieri, P.; Gratteri, S.; Ali, W.; Sergi, D.; Muscoli, S.; Cammarano, A.; Bernardini, S.; Di Renzo, L.; Romeo, F. Effects of postprandial hydroxytyrosol and derivates on oxidation of LDL, cardiometabolic state and gene expression: A nutrigenomic approach for cardiovascular prevention. J. Cardiovasc. Med. 2019, 20, 419–426. [Google Scholar] [CrossRef]
- Cimmino, G.; Muscoli, S.; De Rosa, S.; Cesaro, A.; Perrone, M.A.; Selvaggio, S.; Selvaggio, G.; Aimo, A.; Pedrinelli, R.; Mercuro, G.; et al. Evolving concepts in the pathophysiology of atherosclerosis: From endothelial dysfunction to thrombus formation through multiple shades of inflammation. J. Cardiovasc. Med. 2023, 24 (Suppl. S2), e156–e167. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Variables | Controls (n = 23) | CAD Cases (n = 69) | p-Value |
|---|---|---|---|
| Age (Years) | 49.08 ± 14.09 | 57.55 ± 8.59 | <0.000 |
| Sex (Male/Female) | (14/9) | (65/4) | <0.000 |
| Alcohol Consumer (N) | 2 (8.6%) | 25 (36.23%) | <0.012 |
| Family History | 2 (8.6%) | 18 (20.0%) | 0.486 |
| Dietary Habits * | (13/10) | (23/46) | 0.048 |
| Nature of Work # | (5/15/3) | (8/51/10) | 0.480 |
| Smoker (N) | 6 (26%) | 34 (49.27%) | <0.052 |
| Hypertensive (N) | 4 (17.39%) | 24 (34.78%) | <0.116 |
| BMI (kg/m2) | 23.34 ± 3.43 | 24.22 ± 3.80 | <0.325 |
| Obesity $ | 4 (17.3%) | 21 (30.4%) | <0.223 |
| Healthy Controls | 23 (25%) | - | |
| Single-Vessel Stenosis (CAD-I) | 23 (25%) | ||
| Double-Vessel Stenosis (CAD-II) | 23 (25%) | ||
| Triple-Vessel Stenosis (CAD-III) | 23 (25% |
| Variables | Controls (n = 23) | CAD Cases (n = 69) | p Value |
|---|---|---|---|
| Total Cholesterol (mg/dL) | 142.4 ± 41.5 | 142.2 ± 40.1 | 0.983 |
| High-Density Lipoprotein (HDL) (mg/dL) | 50.65 ± 12.43 | 44.76 ± 8.15 | 0.011 |
| Low-Density Lipoprotein (LDL) (mg/dL) | 63.41 ± 31.96 | 67.29 ± 35.49 | 0.731 |
| Very-Low-Density Lipoprotein (VLDL) (mg/dL) | 33.03 ± 11.81 | 33.84 ± 17.90 | 0.840 |
| Triglyceride (mg/dL) | 166.67 ± 89.47 | 166.34 ± 88.07 | 0.942 |
| PON-1 (ng/dL) | 60.36 ± 12.63 | 32.65 ± 14.67 | 0.000 |
| SRB-1 (ng/dL) | 15.85 ± 2.76 | 12.49 ± 3.34 | 0.000 |
| CAD-I | CAD-II | CAD-III | |
| SRB-1 (ng/dL) | 38.74 ± 19.41 | 32.16 ± 12.45 | 27.05 ± 7.86 |
| PON-1 (ng/dL) | 14.15 ± 2.20 | 14.25 ± 2.02 | 10.06 ± 3.97 |
| Multiple Comparisons (Tukey-HSD) | |||||||
|---|---|---|---|---|---|---|---|
| Dependent Variable | (I) GROUP | (J) GROUP | Mean Difference (I − J) | Std. Error | Sig. * | 95% Confidence Interval | |
| Lower Bound | Upper Bound | ||||||
| PON-1 | CONTROL | CATEGORY-1 | 21.62 * | 4.04 | 0.000 | 11.02 | 32.22 |
| CATEGORY-2 | 28.20 * | 4.04 | 0.000 | 17.60 | 38.80 | ||
| CATEGORY-3 | 33.30 * | 4.04 | 0.000 | 22.71 | 43.90 | ||
| CATEGORY-1 | CATEGORY-2 | 6.58 | 4.04 | 0.369 | −4.01 | 17.18 | |
| CATEGORY-3 | 11.68 * | 4.04 | 0.025 | 1.08 | 22.28 | ||
| CATEGORY-2 | CATEGORY-1 | −6.58 | 4.04 | 0.369 | −17.18 | 4.01 | |
| CATEGORY-3 | 5.10 | 4.04 | 0.590 | −5.49 | 15.70 | ||
| CATEGORY-3 | CATEGORY-1 | −11.68 * | 4.04 | 0.025 | −22.28 | −1.08 | |
| CATEGORY-2 | −5.10 | 4.04 | 0.590 | −15.70 | 5.49 | ||
| SRB-1 | CONTROL | CATEGORY-1 | 1.69 | 0.83 | 0.190 | −0.50 | 3.89 |
| CATEGORY-2 | 2.59 * | 0.83 | 0.014 | 0.39 | 4.79 | ||
| CATEGORY-3 | 5.78 * | 0.83 | 0.000 | 3.59 | 7.98 | ||
| CATEGORY-1 | CATEGORY-2 | 0.90 | 0.83 | 0.707 | −1.29 | 3.09 | |
| CATEGORY-3 | 4.09 * | 0.83 | 0.000 | 1.89 | 6.29 | ||
| CATEGORY-2 | CATEGORY-1 | 0.90 | 0.83 | 0.707 | −3.09 | 1.29 | |
| CATEGORY-3 | 3.19 * | 0.83 | 0.001 | 0.99 | 5.39 | ||
| CATEGORY-3 | CATEGORY-1 | −4.09 * | 0.83 | 0.000 | −6.29 | −1.89 | |
| CATEGORY-2 | −3.19 * | 0.83 | 0.001 | −5.39 | −0.99 | ||
| Cases | Controls | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n (%) | PON-1 Mean ± SD | p Value | SRB-1 Mean ± SD | p Value | n (%) | PON-1 Mean ± SD | p Value | SRB-1 Mean ± SD | p Value | ||
| Tobacco use | Yes | 46 (66.67) | 32.76 ± 15.85 | 0.932 | 12.37 ± 3.26 | 0.942 | 13 (56.5) | 61.96 ± 11.73 | 0.584 | 15.31 ± 2.82 | 0.654 |
| No | 23 (33.3) | 32.43 ± 12.05 | 12.73 ± 3.48 | 10 (43.5) | 58.81 ± 13.42 | 16.40 ± 2.45 | |||||
| Alcohol use | Yes | 8 (11.6) | 27.14 ± 10.56 | 0.26 | 13.47 ± 3.53 | 0.823 | 2 (8.7) | 59.75 ± 2.25 | 0.513 | 14.19 ± 0.09 | 0.587 |
| No | 61 (88.4) | 33.37 ± 14.86 | 12.35 ± 3.26 | 21 (91.3) | 60.77 ± 12.75 | 15.91 ± 2.81 | |||||
| Family history | Yes | 4 (5.8) | 32.29 ± 14.47 | 0.419 | 12.55 ± 3.39 | 0.523 | 2 (8.7) | 74.75 ± 3.95 | 0.105 | 14.99 ± 1.69 | 0.432 |
| No | 65 (94.2) | 38.45 ± 14.91 | 11.36 ± 1.15 | 21 (91.3) | 59.27 ± 12.24 | 15.83 ± 2.80 | |||||
| Obesity | Yes | 10 (14.5) | 36.86 ± 10.81 | 0.330 | 12.30 ± 2.56 | 0.895 | 5 (21.7) | 66.47 ± 12.05 | 0.329 | 17.30 ± 2.70 | 0.422 |
| No | 59 (85.5) | 31.93 ± 14.99 | 12.51 ± 3.42 | 18 (78.3) | 59.38 ± 12.29 | 15.41 ± 2.61 | |||||
| Hypertension | Yes | 30 (43.5) | 38.97 ± 16.08 | 0.002 | 12.73 ± 3.37 | 0.622 | 5 (21.7) | 57.52 ± 13.27 | 0.545 | 18.49 ± 1.48 | 0.983 |
| No | 39 (56.5) | 28.34 ± 11.33 | 12.32 ± 3.29 | 18 (78.3) | 61.60 ± 12.17 | 14.95 ± 2.48 | |||||
| Marker | Cutoff Value | AUC | p Value | Sensitivity (95% CI) | Specificity (95% CI) |
|---|---|---|---|---|---|
| PON-1 | |||||
| Case vs. Control | <39.10 | 0.93 | <0.0001 | 75.36 (64.04–84.01) | 100.0 (85.13–100.0) |
| Category 1 vs. Control | <44.90 | 0.86 | <0.0001 | 73.91 53.53–87.45 | 90.91 (72.19–98.38) |
| Category 2 vs. Control | <38.15 | 0.94 | <0.0001 | 73.91 (53.53–87.45) | 100.0 (85.13–100.0) |
| Category 3 vs. Control | <39.10 | 0.99 | <0.0001 | 95.65 (79.01–99.78) | 100.0 (85.13–100.0) |
| SRB-1 | |||||
| Case vs. Control | <13.63 | 0.75 | 0.0005 | 57.97 46.21–68.89 | 72.73 51.85–86.85 |
| Category 1 vs. Control | <14.94 | 0.62 | 0.112 | 60.87 40.79–77.84 | 54.55 34.66–73.08 |
| Category 2 vs. Control | <13.63 | 0.72 | 0.008 | 56.52 (36.81–74.37) | 72.73 (51.85–86.85) |
| Category 3 vs. Control | <12.75 | 0.88 | <0.001 | 78.26 (58.10–90.34) | 90.91 (72.19–98.38) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kumar, M.; Ali, W.; Yadav, K.; Kaumri, S.; Mishra, S.; Nardi, P.; Iellamo, F.; Bernardini, S.; Pradhan, A.; Perrone, M.A. High-Density Lipoprotein-Associated Paraoxonase-1 (PON-1) and Scavenger Receptor Class B Type 1 (SRB-1) in Coronary Artery Disease: Correlation with Disease Severity. J. Clin. Med. 2024, 13, 5480. https://doi.org/10.3390/jcm13185480
Kumar M, Ali W, Yadav K, Kaumri S, Mishra S, Nardi P, Iellamo F, Bernardini S, Pradhan A, Perrone MA. High-Density Lipoprotein-Associated Paraoxonase-1 (PON-1) and Scavenger Receptor Class B Type 1 (SRB-1) in Coronary Artery Disease: Correlation with Disease Severity. Journal of Clinical Medicine. 2024; 13(18):5480. https://doi.org/10.3390/jcm13185480
Chicago/Turabian StyleKumar, Manish, Wahid Ali, Kusum Yadav, Swati Kaumri, Sridhar Mishra, Paolo Nardi, Ferdinando Iellamo, Sergio Bernardini, Akshyaya Pradhan, and Marco Alfonso Perrone. 2024. "High-Density Lipoprotein-Associated Paraoxonase-1 (PON-1) and Scavenger Receptor Class B Type 1 (SRB-1) in Coronary Artery Disease: Correlation with Disease Severity" Journal of Clinical Medicine 13, no. 18: 5480. https://doi.org/10.3390/jcm13185480