
Metformin Treatment Is Not Associated with Altered PD-L1 Expression in Diabetic Patients with Oral Squamous Cell Carcinoma

 , , ,
, , ,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Cohort
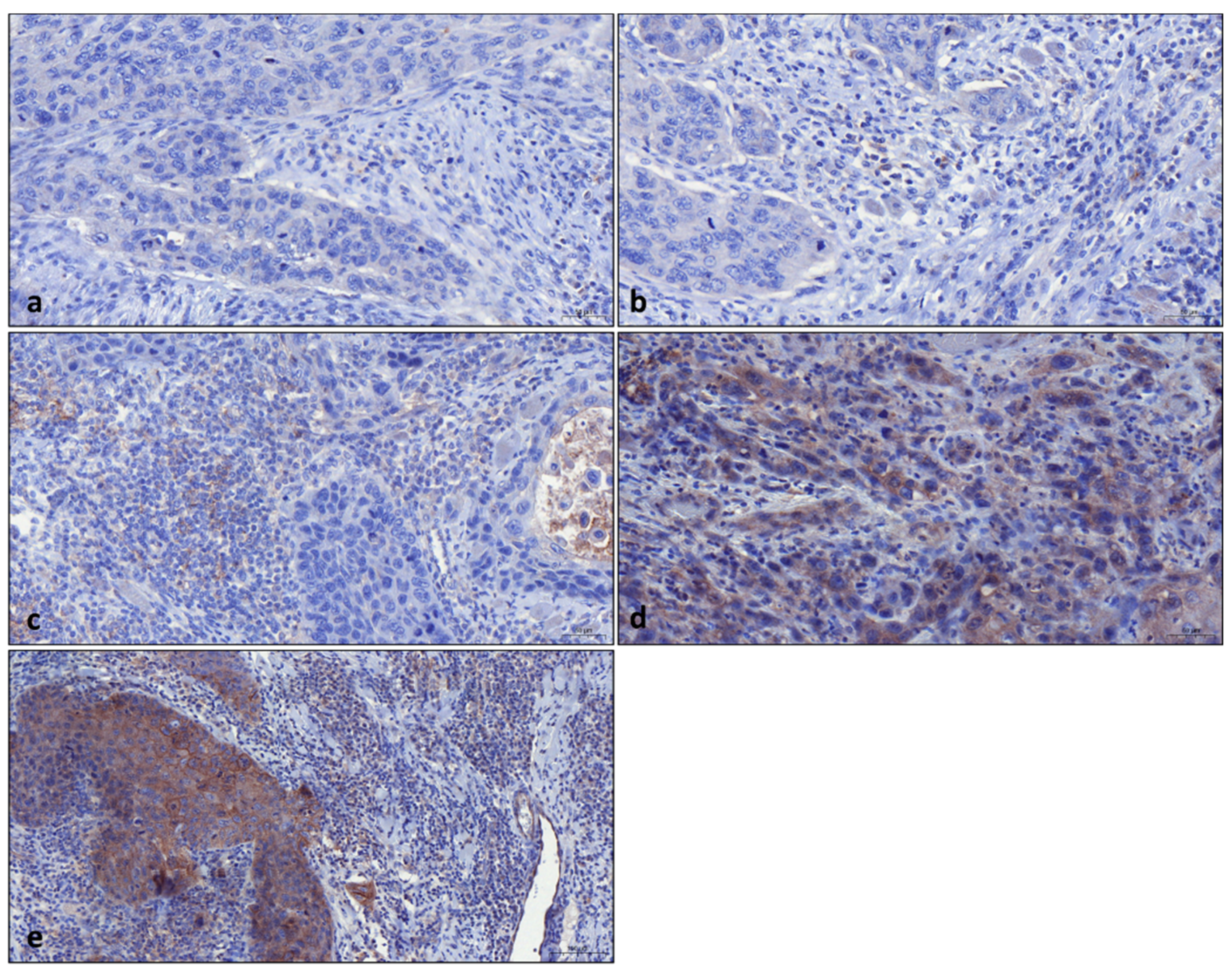
2.2. Tissue Samples and Immunohistochemistry
2.3. Statistical Methods
2.4. Ethics
3. Results
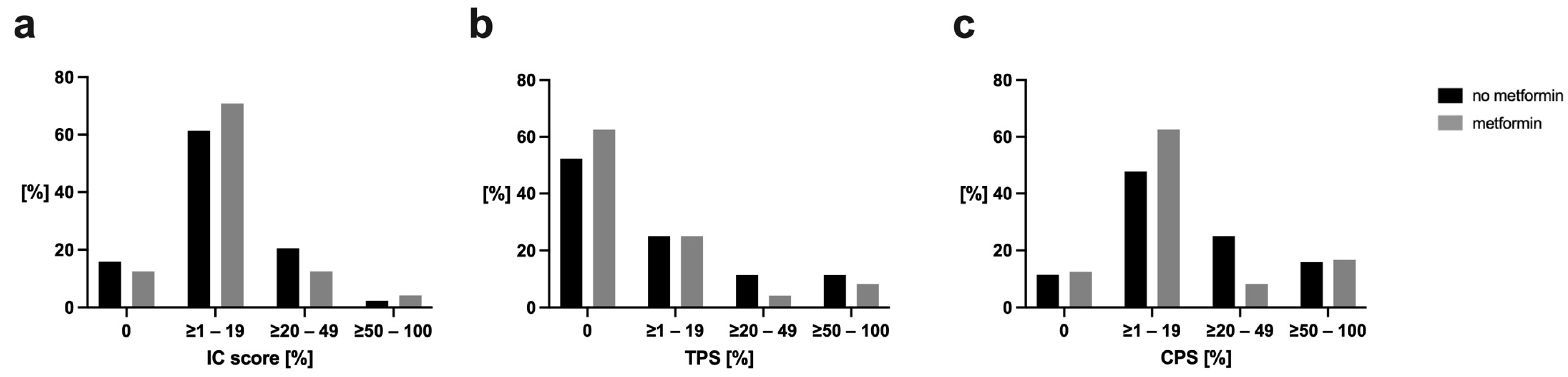
3.1. Immune Cell Score (IC)
3.2. Tumor Proportion Score (TPS)
3.3. Combined Positive Score (CPS)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ketabat, F.; Pundir, M.; Mohabatpour, F.; Lobanova, L.; Koutsopoulos, S.; Hadjiiski, L.; Chen, X.; Papagerakis, P.; Papagerakis, S. Controlled Drug Delivery Systems for Oral Cancer Treatment-Current Status and Future Perspectives. Pharmaceutics 2019, 11, 302. [Google Scholar] [CrossRef] [PubMed]
- Bagan, J.; Sarrion, G.; Jimenez, Y. Oral cancer: Clinical features. Oral Oncol. 2010, 46, 414–417. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Sun, P.; Dahlstrom, K.R.; Gross, N.; Li, G. Joint effect of human papillomavirus exposure, smoking and alcohol on risk of oral squamous cell carcinoma. BMC Cancer 2023, 23, 457. [Google Scholar] [CrossRef] [PubMed]
- Ujpál, M.; Matos, O.; Bíbok, G.; Somogyi, A.; Szabó, G.; Suba, Z. Diabetes and oral tumors in Hungary: Epidemiological correlations. Diabetes Care 2004, 27, 770–774. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.-H.; Wu, T.-Y.; Li, C.-C.; Lui, M.-T.; Chang, K.-W.; Kao, S.-Y. Impact of Diabetes Mellitus on the Prognosis of Patients with Oral Squamous Cell Carcinoma: A Retrospective Cohort Study. Ann. Surg. Oncol. 2010, 17, 2175–2183. [Google Scholar] [CrossRef]
- Global Guideline for Type 2 Diabetes: Recommendations for standard, comprehensive, and minimal care. Diabet. Med. 2006, 23, 579–593. [CrossRef]
- Bailey, C.J. Metformin: Historical overview. Diabetologia 2017, 60, 1566–1576. [Google Scholar] [CrossRef]
- Rena, G.; Hardie, D.G.; Pearson, E.R. The mechanisms of action of metformin. Diabetologia 2017, 60, 1577–1585. [Google Scholar] [CrossRef]
- Podhorecka, M.; Ibanez, B.; Dmoszynska, A. Metformin—Its potential anti-cancer and anti-aging effects. Postep. Hig. Med. Dosw. 2017, 71, 170–175. [Google Scholar] [CrossRef]
- Heckman-Stoddard, B.M.; DeCensi, A.; Sahasrabuddhe, V.V.; Ford, L.G. Repurposing metformin for the prevention of cancer and cancer recurrence. Diabetologia 2017, 60, 1639–1647. [Google Scholar] [CrossRef]
- Lei, Y.; Yi, Y.; Liu, Y.; Liu, X.; Keller, E.T.; Qian, C.N.; Zhang, J.; Lu, Y. Metformin targets multiple signaling pathways in cancer. Chin. J. Cancer 2017, 36, 17. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Lu, S. Metformin inhibits esophagus cancer proliferation through upregulation of USP7. Cell. Physiol. Biochem. 2013, 32, 1178–1186. [Google Scholar] [CrossRef] [PubMed]
- Haas, M.; Lein, A.; Fuereder, T.; Schnoell, J.; Brkic, F.F.; Campion, N.J.; Liu, D.T.; Kadletz-Wanke, L.; Heiduschka, G.; Jank, B.J. Low free triiodothyronine and immune-related hyperthyroidism are associated with overall and progression-free survival in head and neck squamous cell carcinoma treated with pembrolizumab. Int. Immunopharmacol. 2023, 123, 110799. [Google Scholar] [CrossRef] [PubMed]
- Harrington, K.J.; Burtness, B.; Greil, R.; Soulières, D.; Tahara, M.; de Castro, G., Jr.; Psyrri, A.; Brana, I.; Basté, N.; Neupane, P.; et al. Pembrolizumab With or Without Chemotherapy in Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma: Updated Results of the Phase III KEYNOTE-048 Study. J. Clin. Oncol. 2023, 41, 790–802. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Liu, D.; Li, L. PD-1/PD-L1 pathway: Current researches in cancer. Am. J. Cancer Res. 2020, 10, 727–742. [Google Scholar]
- Cramer, J.D.; Burtness, B.; Ferris, R.L. Immunotherapy for head and neck cancer: Recent advances and future directions. Oral Oncol. 2019, 99, 104460. [Google Scholar] [CrossRef]
- Wang, R.; Zhao, Y. Effects of Metformin on JNK Signaling Pathway and PD-L1 Expression in Triple Negative Breast Cancer. Cancer Manag. Res. 2024, 16, 259–268. [Google Scholar] [CrossRef]
- Cha, J.H.; Yang, W.H.; Xia, W.; Wei, Y.; Chan, L.C.; Lim, S.O.; Li, C.W.; Kim, T.; Chang, S.S.; Lee, H.H.; et al. Metformin Promotes Antitumor Immunity via Endoplasmic-Reticulum-Associated Degradation of PD-L1. Mol. Cell 2018, 71, 606–620.e607. [Google Scholar] [CrossRef]
- Guimarães, T.A.; Farias, L.C.; Santos, E.S.; de Carvalho Fraga, C.A.; Orsini, L.A.; de Freitas Teles, L.; Feltenberger, J.D.; de Jesus, S.F.; de Souza, M.G.; Santos, S.H.; et al. Metformin increases PDH and suppresses HIF-1α under hypoxic conditions and induces cell death in oral squamous cell carcinoma. Oncotarget 2016, 7, 55057–55068. [Google Scholar] [CrossRef]
- Sobin, L.H.; Gospodarowicz, M.K.M.K.; Wittekind, C.C.; International Union against Cancer. TNM Classification of Malignant Tumours, 7th ed.; Wiley-Blackwell: Chichester, UK; Hoboken, NJ, USA, 2010. [Google Scholar]
- Mamilos, A.; Lein, A.; Winter, L.; Ettl, T.; Künzel, J.; Reichert, T.E.; Spanier, G.; Brochhausen, C. Tumor Immune Microenvironment Heterogeneity at the Invasion Front and Tumor Center in Oral Squamous Cell Carcinoma as a Perspective of Managing This Cancer Entity. J. Clin. Med. 2023, 12, 1704. [Google Scholar] [CrossRef]
- Mamilos, A.; Lein, A.; Winter, L.; Haas, M.; Reichert, T.E.; Ettl, T.; Künzel, J.; Spanier, G.; Brochhausen, C. Immunohistochemical Assessment of Microvessel Density in OSCC: Spatial Heterogeneity of Angiogenesis and Its Impact on Survival. Biomedicines 2023, 11, 2724. [Google Scholar] [CrossRef] [PubMed]
- Schildhaus, H.U. [Predictive value of PD-L1 diagnostics]. Pathologe 2018, 39, 498–519. [Google Scholar] [CrossRef] [PubMed]
- Schildhaus, H.U.; Weichert, W. Predictive diagnostics for checkpoint inhibitors. Pathologe 2021, 42, 380–390. [Google Scholar] [CrossRef] [PubMed]
- Wabitsch, S.; McCallen, J.D.; Kamenyeva, O.; Ruf, B.; McVey, J.C.; Kabat, J.; Walz, J.S.; Rotman, Y.; Bauer, K.C.; Craig, A.J.; et al. Metformin treatment rescues CD8(+) T-cell response to immune checkpoint inhibitor therapy in mice with NAFLD. J. Hepatol. 2022, 77, 748–760. [Google Scholar] [CrossRef]
- Munoz, L.E.; Huang, L.; Bommireddy, R.; Sharma, R.; Monterroza, L.; Guin, R.N.; Samaranayake, S.G.; Pack, C.D.; Ramachandiran, S.; Reddy, S.J.C.; et al. Metformin reduces PD-L1 on tumor cells and enhances the anti-tumor immune response generated by vaccine immunotherapy. J. Immunother. Cancer 2021, 9, e002614. [Google Scholar] [CrossRef]
- Chow, L.Q.M.; Haddad, R.; Gupta, S.; Mahipal, A.; Mehra, R.; Tahara, M.; Berger, R.; Eder, J.P.; Burtness, B.; Lee, S.H.; et al. Antitumor Activity of Pembrolizumab in Biomarker-Unselected Patients with Recurrent and/or Metastatic Head and Neck Squamous Cell Carcinoma: Results from the Phase Ib KEYNOTE-012 Expansion Cohort. J. Clin. Oncol. 2016, 34, 3838–3845. [Google Scholar] [CrossRef]
- Vos, J.L.; Elbers, J.B.W.; Krijgsman, O.; Traets, J.J.H.; Qiao, X.; van der Leun, A.M.; Lubeck, Y.; Seignette, I.M.; Smit, L.A.; Willems, S.M.; et al. Neoadjuvant immunotherapy with nivolumab and ipilimumab induces major pathological responses in patients with head and neck squamous cell carcinoma. Nat. Commun. 2021, 12, 7348. [Google Scholar] [CrossRef]
- Turnheim, K.; Waldhausl, W.K. Essentials of insulin pharmacokinetics. Wien Klin. Wochenschr. 1988, 100, 65–72. [Google Scholar]
- Zhao, X.; Liu, C.; Peng, L.; Wang, H. Metformin facilitates anti-PD-L1 efficacy through the regulation of intestinal microbiota. Genes Immun. 2024, 25, 7–13. [Google Scholar] [CrossRef]
- Henderson, D.; Frieson, D.; Zuber, J.; Solomon, S.S. Metformin Has Positive Therapeutic Effects in Colon Cancer and Lung Cancer. Am. J. Med. Sci. 2017, 354, 246–251. [Google Scholar] [CrossRef]
- Lin, H.; Yiu, D.C.; Chin, S.; Liu, K.; Yip, T.C. Metformin in patients with hepatocellular carcinoma receiving immunotherapy. J. Hepatol. 2023, 78, e180–e182. [Google Scholar] [CrossRef] [PubMed]
- Hua, Y.; Zheng, Y.; Yao, Y.; Jia, R.; Ge, S.; Zhuang, A. Metformin and cancer hallmarks: Shedding new lights on therapeutic repurposing. J. Transl. Med. 2023, 21, 403. [Google Scholar] [CrossRef] [PubMed]
- Saraei, P.; Asadi, I.; Kakar, M.A.; Moradi-Kor, N. The beneficial effects of metformin on cancer prevention and therapy: A comprehensive review of recent advances. Cancer Manag. Res. 2019, 11, 3295–3313. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Xin, D.; Guan, L.; Xu, M.; Yang, Y.; Chen, Y.; Yang, Y.; Wang-Gillam, A.; Wang, L.; Zong, S.; et al. Metformin Downregulates PD-L1 Expression in Esophageal Squamous Cell Catrcinoma by Inhibiting IL-6 Signaling Pathway. Front. Oncol. 2021, 11, 762523. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.J.; Zhang, Q.S.; Li, Z.Q.; Zhou, J.W.; Du, J. Metformin attenuates PD-L1 expression through activating Hippo signaling pathway in colorectal cancer cells. Am. J. Transl. Res. 2019, 11, 6965–6976. [Google Scholar]

{kind=link}
{kind=link}
| Total | No Metformin | Metformin | ||||
|---|---|---|---|---|---|---|
| Variable/Category | n | n | (% total) | n | (% total) | p-value |
| Number of patients | 68 | 44 | (100.0%) | 24 | (100.0%) | |
| Age | ||||||
| ≥70 | 22 | 14 | (31.8%) | 8 | (33.3%) | |
| <70 | 46 | 30 | (68.2%) | 16 | (66.7%) | p = 0.898 |
| Gender | ||||||
| male | 51 | 32 | (72.7%) | 19 | (79.2%) | |
| female | 17 | 12 | (27.3%) | 5 | (20.8%) | p = 0.558 |
| Smoking history | ||||||
| never | 23 | 12 | (27.3%) | 11 | (45.8%) | |
| smoker | 45 | 32 | (72.7%) | 13 | (54.2%) | p = 0.122 |
| Alcohol abuse | ||||||
| no | 22 | 14 | (31.8%) | 8 | (33.3%) | |
| yes | 46 | 30 | (68.2%) | 16 | (66.7%) | p = 0.898 |
| Primary site | ||||||
| buccal mucosa | 9 | 6 | (13.6%) | 3 | (12.5%) | |
| upper alveolus | 2 | 0 | (0.0%) | 2 | (8.3%) | |
| lower alveolus | 11 | 8 | (18.2%) | 3 | (12.5%) | |
| hard palate | 7 | 5 | (11.4%) | 2 | (8.3%) | |
| tongue | 20 | 14 | (31.8%) | 6 | (25.0%) | |
| floor of the mouth | 19 | 11 | (25.0%) | 8 | (33.3%) | p = 0.528 |
| T | ||||||
| 1 | 23 | 16 | (36.4%) | 7 | (29.2%) | |
| 2 | 23 | 13 | (29.5%) | 10 | (41.7%) | |
| 3 | 9 | 6 | (13.6%) | 3 | (12.5%) | |
| 4 | 13 | 9 | (20.5%) | 4 | (16.7%) | p = 0.798 |
| N | ||||||
| 0 | 11 | 9 | (20.5%) | 2 | (8.3%) | |
| 1 | 0 | 0 | (0.0%) | 0 | (0.0%) | |
| 2 | 11 | 7 | (15.9%) | 4 | (16.7%) | |
| 3 | 6 | 4 | (9.1%) | 2 | (8.3%) | p = 0.658 |
| M | ||||||
| unknown | 9 | 0 | (0.0%) | 9 | (37.5%) | |
| no spread | 50 | 37 | (84.1%) | 13 | (54.2%) | |
| any spread | 9 | 7 | (15.9%) | 2 | (8.3%) | p < 0.001 |
| Grade | ||||||
| 1 | 2 | 1 | (2.3%) | 1 | (4.2%) | |
| 2 | 58 | 36 | (81.8%) | 22 | (91.7%) | |
| 3 | 8 | 7 | (15.9%) | 1 | (4.2%) | p = 0.335 |
| Stage | ||||||
| I | 17 | 11 | (25.0%) | 6 | (25.0%) | |
| II | 12 | 7 | (15.9%) | 5 | (20.8%) | |
| III | 13 | 9 | (20.5%) | 4 | (16.7%) | |
| IV | 26 | 17 | (38.6%) | 9 | (37.5%) | p = 0.968 |
| Perineural invasion | ||||||
| no | 63 | 41 | (93.2%) | 22 | (91.7%) | |
| yes | 5 | 3 | (6.8%) | 2 | (8.3%) | p = 0.819 |
| Lymph vessel invasion | ||||||
| no | 53 | 34 | (77.3%) | 19 | (79.2%) | |
| yes | 15 | 10 | (22.7%) | 5 | (20.8%) | p = 0.857 |
| Blood vessel invasion | ||||||
| no | 66 | 42 | (95.5%) | 24 | (100.0%) | |
| yes | 2 | 2 | (4.5%) | 0 | (0.0%) | p = 0.289 |
| No Metformin | Metformin | |||||
|---|---|---|---|---|---|---|
| PD-L1 score | n | (% total) | n | (% total) | p-value | |
| IC | ||||||
| <1 | 7 | (15.9%) | 3 | (12.5%) | ||
| ≥1–<20 | 27 | (61.4%) | 17 | (70.8%) | ||
| ≥20–<50 | 9 | (20.5%) | 3 | (12.5%) | ||
| ≥50–100 | 1 | (2.3%) | 1 | (4.2%) | p = 0.748 | |
| TPS | ||||||
| <1 | 23 | (52.3%) | 15 | (62.5%) | ||
| ≥1–<20 | 11 | (25.0%) | 6 | (25.0%) | ||
| ≥20–<50 | 5 | (11.4%) | 1 | (4.2%) | ||
| ≥50–100 | 5 | (11.4%) | 2 | (8.3%) | p = 0.818 | |
| CPS | ||||||
| <1 | 5 | (11.4%) | 3 | (12.5%) | ||
| ≥1–<20 | 21 | (47.7%) | 15 | (62.5%) | ||
| ≥20–<50 | 11 | (25.0%) | 2 | (8.3%) | ||
| ≥50–100 | 7 | (15.9%) | 4 | (16.7%) | p = 0.387 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mamilos, A.; Winter, L.; Lein, A.; Spoerl, S.; Ludwig, N.; Ettl, T.; Künzel, J.; Reichert, T.; Spanier, G.; Brochhausen, C. Metformin Treatment Is Not Associated with Altered PD-L1 Expression in Diabetic Patients with Oral Squamous Cell Carcinoma. J. Clin. Med. 2024, 13, 5632. https://doi.org/10.3390/jcm13185632
Mamilos A, Winter L, Lein A, Spoerl S, Ludwig N, Ettl T, Künzel J, Reichert T, Spanier G, Brochhausen C. Metformin Treatment Is Not Associated with Altered PD-L1 Expression in Diabetic Patients with Oral Squamous Cell Carcinoma. Journal of Clinical Medicine. 2024; 13(18):5632. https://doi.org/10.3390/jcm13185632
Chicago/Turabian StyleMamilos, Andreas, Lina Winter, Alexander Lein, Steffen Spoerl, Nils Ludwig, Tobias Ettl, Julian Künzel, Torsten Reichert, Gerrit Spanier, and Christoph Brochhausen. 2024. "Metformin Treatment Is Not Associated with Altered PD-L1 Expression in Diabetic Patients with Oral Squamous Cell Carcinoma" Journal of Clinical Medicine 13, no. 18: 5632. https://doi.org/10.3390/jcm13185632