
Chiropractic and Spinal Manipulation: A Review of Research Trends, Evidence Gaps, and Guideline Recommendations

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
3. Results
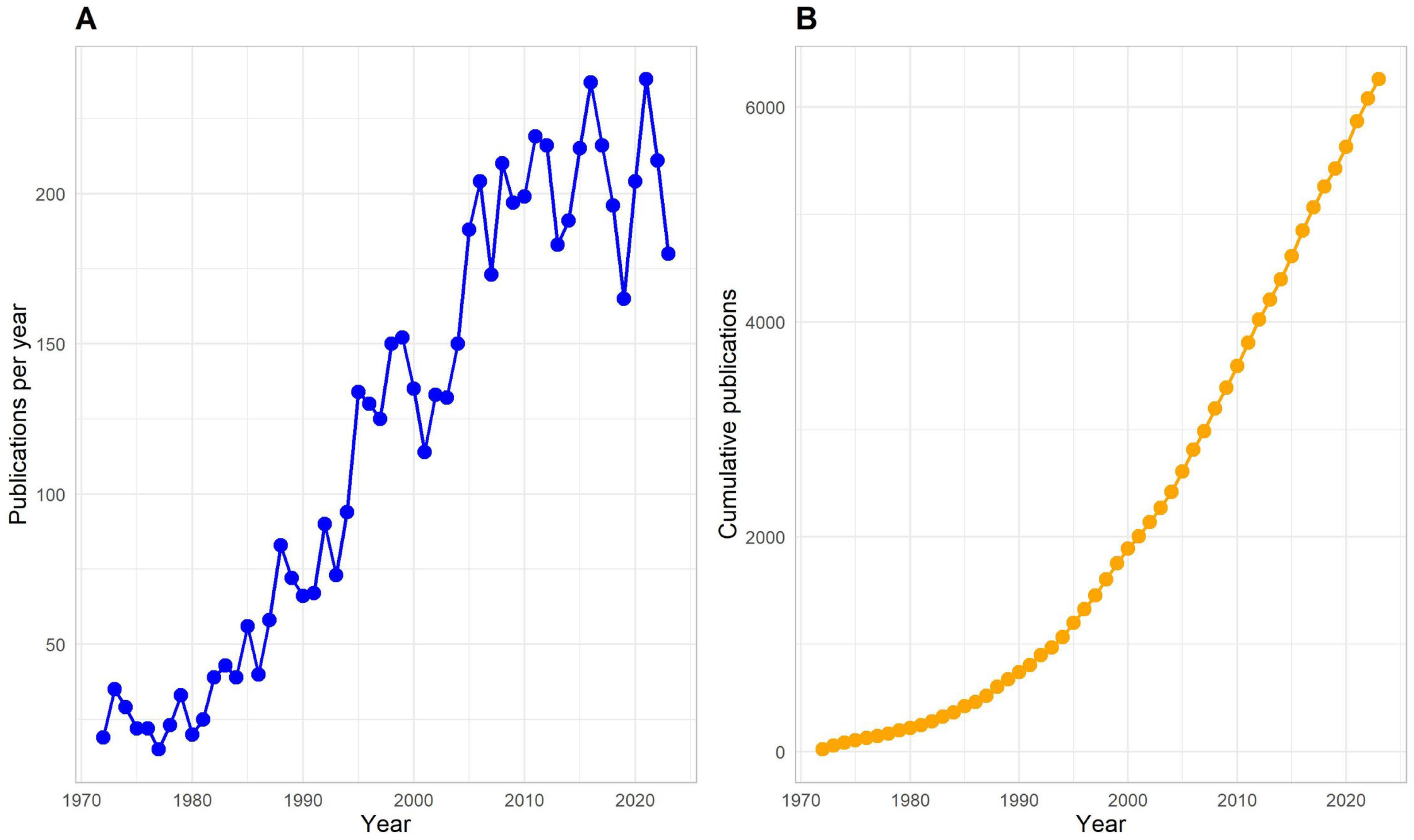
3.1. Publication Trends
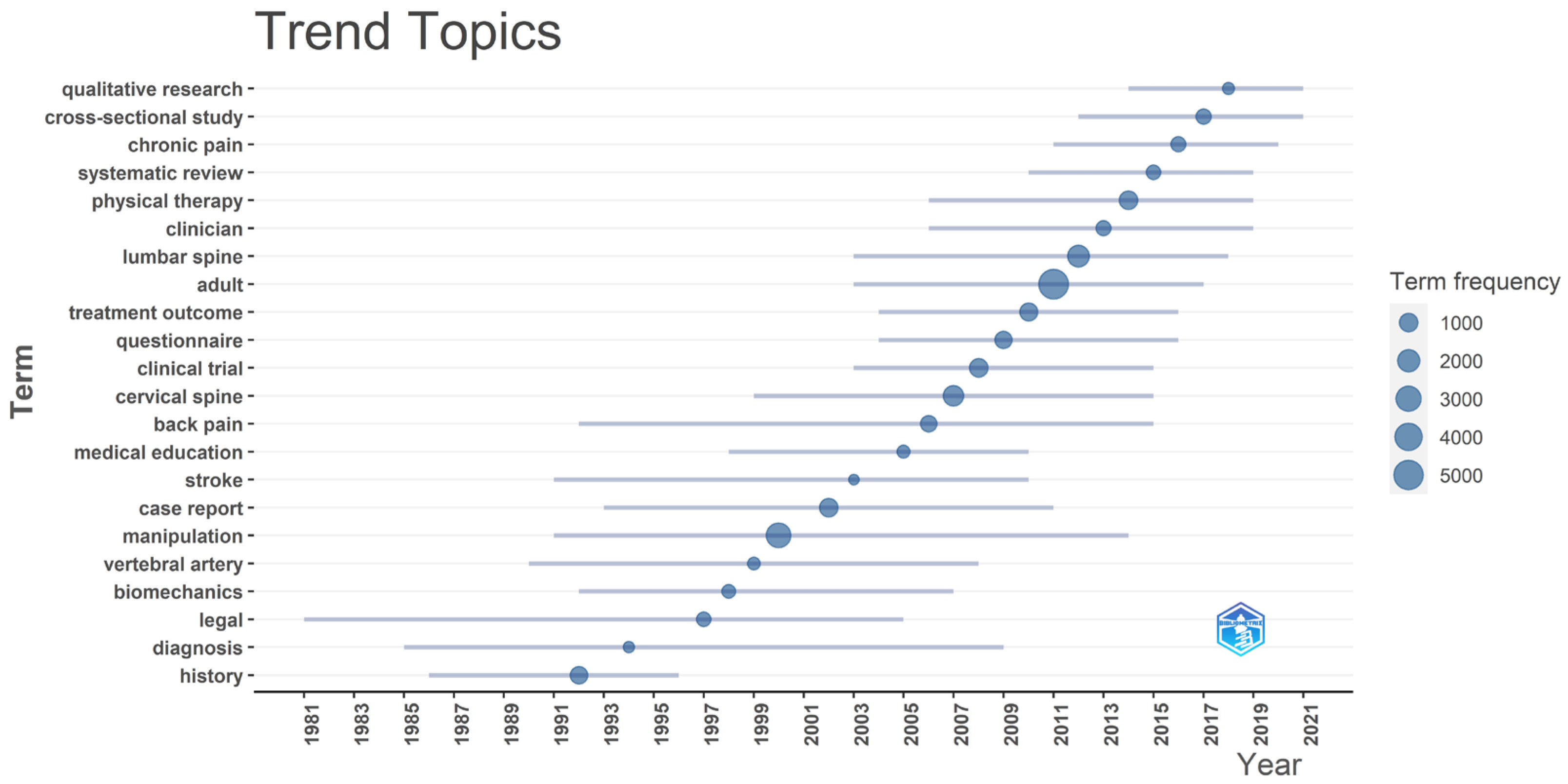
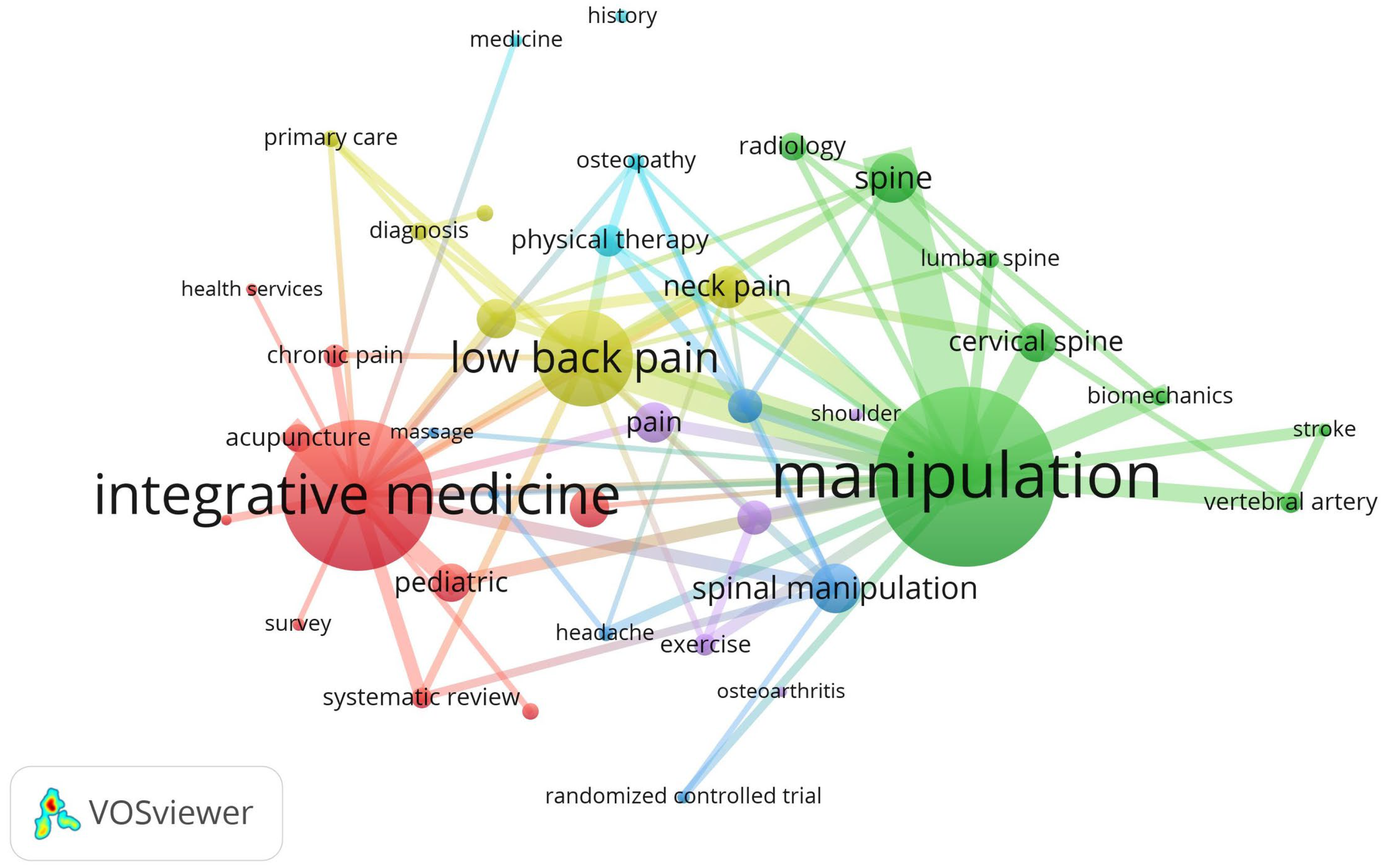
3.2. Keywords
3.3. Clinical Practice Guidelines
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Meeker, W.C.; Haldeman, S. Chiropractic: A Profession at the Crossroads of Mainstream and Alternative Medicine. Ann. Intern. Med. 2002, 136, 216–227. [Google Scholar] [CrossRef] [PubMed]
- Harwood, K.J.; Pines, J.M.; Andrilla, C.H.A.; Frogner, B.K. Where to Start? A Two Stage Residual Inclusion Approach to Estimating Influence of the Initial Provider on Health Care Utilization and Costs for Low Back Pain in the US. BMC Health Serv. Res. 2022, 22, 694. [Google Scholar] [CrossRef] [PubMed]
- Fenton, J.J.; Fang, S.-Y.; Ray, M.; Kennedy, J.; Padilla, K.; Amundson, R.; Elton, D.; Haldeman, S.; Lisi, A.J.; Sico, J.; et al. Longitudinal Care Patterns and Utilization among Patients with New-Onset Neck Pain by Initial Provider Specialty. Spine (Phila Pa 1976) 2023, 48, 1409–1418. [Google Scholar] [CrossRef] [PubMed]
- Beliveau, P.J.H.; Wong, J.J.; Sutton, D.A.; Simon, N.B.; Bussières, A.E.; Mior, S.A.; French, S.D. The Chiropractic Profession: A Scoping Review of Utilization Rates, Reasons for Seeking Care, Patient Profiles, and Care Provided. Chiropr. Man. Ther. 2017, 25, 35. [Google Scholar] [CrossRef]
- Tindle, H.A.; Davis, R.B.; Phillips, R.S.; Eisenberg, D.M. Trends in Use of Complementary and Alternative Medicine by US Adults: 1997–2002. Altern. Ther. Health Med. 2005, 11, 42–49. [Google Scholar]
- Nahin, R.L.; Rhee, A.; Stussman, B. Use of Complementary Health Approaches Overall and for Pain Management by US Adults. JAMA 2024, 331, 613–615. [Google Scholar] [CrossRef]
- von Kuster, T., Jr. Chiropractic Health Care: A National Study of Cost of Education, Service Utilization, Number of Practicing Doctors of Chiropractic, and Other Key Policy Issues; Foundation for the Advancement of Chiropractic Tenets and Science: Washington, DC, USA, 1980; Volumes I–II, 353p. [Google Scholar]
- Cherkin, D.C.; Mootz, R.D. Chiropractic in the United States: Training, Practice and Research; AHCPR Publication No. 98-N002; Agency for Health Care Policy and Research, U.S. Department of Health and Human Services: Rockville, MD, USA, 1997.
- Simpson, J.K. The Five Eras of Chiropractic & the Future of Chiropractic as Seen through the Eyes of a Participant Observer. Chiropr. Ma. Therap. 2012, 20, 1. [Google Scholar] [CrossRef]
- Bigos, S.J.; Bowyer, R.; Brown, K.; Deyo, R.; Haldeman, S.; Hart, J.L.; Johnson, E.W.; Keller, R.; Kido, D.; Liang, M.H.; et al. Acute Low Back Problems in Adults: Assessment and Treatment. Agency for Health Care Policy and Research. Clin. Pract. Guidel. Quick Ref. Guide Clin. 1994, iii–iv, 1–25. [Google Scholar]
- United States Congress Conference Committees; U.S. Congress. HR 1: Social Security Amendments for 1972. Brief Description of Senate Amendments, Prepared for the Use of the Conferees; US Government Printing Office: Washington, DC, USA, 1972.
- Whedon, J.M.; Goertz, C.M.; Lurie, J.D.; Stason, W.B. Beyond Spinal Manipulation: Should Medicare Expand Coverage for Chiropractic Services? A Review and Commentary on the Challenges for Policy Makers. J. Chiropr. Humanit. 2013, 20, 9. [Google Scholar] [CrossRef]
- Pitt Launches a Doctor of Chiropractic Program. Available online: https://www.pitt.edu/pittwire/features-articles/pitt-chiropractic-program-lower-back-pain (accessed on 19 February 2024).
- Doctor of Chiropractic|University of Pittsburgh School of Health and Rehabilitation Sciences. Available online: https://www.shrs.pitt.edu/chiropractic (accessed on 24 June 2024).
- Schut, S.M. Postgraduate Training Opportunities for Chiropractors: A Description of United States Programs. J. Chiropr. Educ. 2024, 38, 104–114. [Google Scholar] [CrossRef]
- Himelfarb, I.; Hyland, J.; Ouzts, N.; Russell, M.; Sterling, T.; Johnson, C.; Green, B. National Board of Chiropractic Examiners: Practice Analysis of Chiropractic 2020; NBCE: Greeley, CO, USA, 2020. [Google Scholar]
- Burton, W.; Salsbury, S.A.; Goertz, C.M. Healthcare Provider Perspectives on Integrating a Comprehensive Spine Care Model in an Academic Health System: A Cross-Sectional Survey. BMC Health Serv. Res. 2024, 24, 125. [Google Scholar] [CrossRef] [PubMed]
- Salsbury, S.A.; Goertz, C.M.; Twist, E.J.; Lisi, A.J. Integration of Doctors of Chiropractic Into Private Sector Health Care Facilities in the United States: A Descriptive Survey. J. Manip. Physiol. Ther. 2018, 41, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Barry, E.S.; Merkebu, J.; Varpio, L. How to Conduct a State-of-the-Art Literature Review. J. Grad. Med. Educ. 2022, 14, 663–665. [Google Scholar] [CrossRef] [PubMed]
- Ninkov, A.; Frank, J.R.; Maggio, L.A. Bibliometrics: Methods for Studying Academic Publishing. Perspect. Med. Educ. 2022, 11, 173–176. [Google Scholar] [CrossRef]
- Miake-Lye, I.M.; Hempel, S.; Shanman, R.; Shekelle, P.G. What Is an Evidence Map? A Systematic Review of Published Evidence Maps and Their Definitions, Methods, and Products. Syst. Rev. 2016, 5, 28. [Google Scholar] [CrossRef]
- Guidelines-Standard-CINAHL. Available online: https://searchfilters.cadth.ca/link/76 (accessed on 14 March 2024).
- Hollon, S.D.; Areán, P.A.; Craske, M.G.; Crawford, K.A.; Kivlahan, D.R.; Magnavita, J.J.; Ollendick, T.H.; Sexton, T.L.; Spring, B.; Bufka, L.F.; et al. Development of Clinical Practice Guidelines. Annu. Rev. Clin. Psychol. 2014, 10, 213–241. [Google Scholar] [CrossRef]
- AlRyalat, S.A.S.; Malkawi, L.W.; Momani, S.M. Comparing Bibliometric Analysis Using PubMed, Scopus, and Web of Science Databases. J. Vis. Exp. 2019, 152, e58494. [Google Scholar] [CrossRef]
- Pozsgai, G.; Lövei, G.L.; Vasseur, L.; Gurr, G.; Batáry, P.; Korponai, J.; Littlewood, N.A.; Liu, J.; Móra, A.; Obrycki, J.; et al. Irreproducibility in Searches of Scientific Literature: A Comparative Analysis. Ecol. Evol. 2021, 11, 14658–14668. [Google Scholar] [CrossRef]
- Covidence Systematic Review Software; Veritas Health Innovation: Melbourne, Australia, 2024.
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022. [Google Scholar]
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016; ISBN 978-3-319-24277-4. [Google Scholar]
- Wickham, H.; Vaughan, D.; Girlich, M. tidyr: Tidy Messy Data; R Package Version 1.3.1; Posit Software, PBC: Boston, MA, USA, 2024. [Google Scholar]
- Aria, M.; Cuccurullo, C. Bibliometrix: An R-Tool for Comprehensive Science Mapping Analysis. J. Informetr. 2017, 11, 959–975. [Google Scholar] [CrossRef]
- Van Eck, N.J.; Waltman, L. Software Survey: VOSviewer, a Computer Program for Bibliometric Mapping. Scientometrics 2010, 84, 523–538. [Google Scholar] [CrossRef]
- Wickham, H.; François, R.; Henry, L.; Müller, K.; Vaughan, D. dplyr: A Grammar of Data Manipulation; Posit Software, PBC: Boston, MA, USA, 2023. [Google Scholar]
- Kaptchuk, T.J.; Eisenberg, D.M. Chiropractic: Origins, Controversies, and Contributions. Arch. Intern. Med. 1998, 158, 2215–2224. [Google Scholar] [CrossRef] [PubMed]
- Jagbandhansingh, M.P. Most Common Causes of Chiropractic Malpractice Lawsuits. J. Manip. Physiol. Ther. 1997, 20, 60–64. [Google Scholar]
- Rubinstein, S.M.; de Zoete, A.; van Middelkoop, M.; Assendelft, W.J.J.; de Boer, M.R.; van Tulder, M.W. Benefits and Harms of Spinal Manipulative Therapy for the Treatment of Chronic Low Back Pain: Systematic Review and Meta-Analysis of Randomised Controlled Trials [with Consumer Summary]. BMJ 2019, 364, 1689. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, J.; Gass, M.L.; Maki, P.M.; Newton, K.M.; Pinkerton, J.V.; Taylor, M.; Utian, W.H. Nonhormonal Management of Menopause-Associated Vasomotor Symptoms: 2015 Position Statement of The North American Menopause Society. Menopause 2015, 22, 1155. [Google Scholar] [CrossRef]
- Alperovitch-Najenson, D.; Becker, A.; Belton, J.; Buchbinder, R.; Cadmus, E.O.; Cardosa, M.; Chaturvedi, S.K.; Chou, R.; Daitz, B.; Eldin, M.M.; et al. WHO Guideline for Non-Surgical Management of Chronic Primary Low Back Pain in Adults in Primary and Community Care Settings; World Health Organization: Geneva, Switzerland, 2023. [Google Scholar]
- Bier, J.D.; Scholten-Peeters, W.G.M.; Staal, J.B.; Pool, J.; van Tulder, M.W.; Beekman, E.; Knoop, J.; Meerhoff, G.; Verhagen, A.P. Clinical Practice Guideline for Physical Therapy Assessment and Treatment in Patients With Nonspecific Neck Pain. Phys. Ther. 2018, 98, 162–171. [Google Scholar] [CrossRef]
- Blanpied, P.R.; Gross, A.R.; Elliott, J.M.; Devaney, L.L.; Clewley, D.; Walton, D.M.; Sparks, C.; Robertson, E.K.; Altman, R.D.; Beattie, P.; et al. Neck Pain: Revision 2017: Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability and Health from the Orthopaedic Section of the American Physical Therapy Association. J. Orthop. Sports Phys. Ther. 2017, 47, A1–A83. [Google Scholar] [CrossRef]
- Bryans, R.; Decina, P.; Descarreaux, M.; Duranleau, M.; Marcoux, H.; Potter, B.; Ruegg, R.P.; Shaw, L.; Watkin, R.; White, E. Evidence-Based Guidelines for the Chiropractic Treatment of Adults with Neck Pain. J. Manip. Physiol. Ther. 2014, 37, 42–63. [Google Scholar] [CrossRef]
- Bussieres, A.E.; Stewart, G.; al-Zoubi, F.; Decina, P.; Descarreaux, M.; Haskett, D.; Hincapie, C.; Page, I.; Passmore, S.; Srbely, J.; et al. Spinal Manipulative Therapy and Other Conservative Treatments for Low Back Pain: A Guideline from the Canadian Chiropractic Guideline Initiative [with Consumer Summary]. J. Manip. Physiol. Ther. 2018, 41, 265–293. [Google Scholar] [CrossRef]
- Bussières, A.E.; Stewart, G.; Al-Zoubi, F.; Decina, P.; Descarreaux, M.; Hayden, J.; Hendrickson, B.; Hincapié, C.; Pagé, I.; Passmore, S.; et al. The Treatment of Neck Pain–Associated Disorders and Whiplash-Associated Disorders: A Clinical Practice Guideline. J. Manip. Physiol. Ther. 2016, 39, 523–564.e27. [Google Scholar] [CrossRef]
- Chou, R.; Côté, P.; Randhawa, K.; Torres, P.; Yu, H.; Nordin, M.; Hurwitz, E.L.; Haldeman, S.; Cedraschi, C. The Global Spine Care Initiative: Applying Evidence-Based Guidelines on the Non-Invasive Management of Back and Neck Pain to Low-and Middle-Income Communities. Eur. Spine J. 2018, 27, 851–860. [Google Scholar] [CrossRef]
- Côté, P.; Yu, H.; Shearer, H.M.; Randhawa, K.; Wong, J.J.; Mior, S.; Ameis, A.; Carroll, L.J.; Nordin, M.; Varatharajan, S.; et al. Non-Pharmacological Management of Persistent Headaches Associated with Neck Pain: A Clinical Practice Guideline from the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. Eur. J. Pain 2019, 23, 1051–1070. [Google Scholar] [CrossRef] [PubMed]
- Dowell, D.; Ragan, K.R.; Jones, C.M.; Baldwin, G.T.; Chou, R. CDC Clinical Practice Guideline for Prescribing Opioids for Pain—United States, 2022. MMWR Recomm. Rep. 2022, 71, 1–95. [Google Scholar] [CrossRef] [PubMed]
- Globe, G.; Farabaugh, R.J.; Hawk, C.; Morris, C.E.; Baker, G.; Whalen, W.M.; Walters, S.; Kaeser, M.; Dehen, M.; Augat, T. Clinical Practice Guideline: Chiropractic Care for Low Back Pain. J. Manip. Physiol. Ther. 2016, 39, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Hawk, C.; Amorin-Woods, L.; Evans, M.W.; Whedon, J.M.; Daniels, C.J.; Williams, R.D.; Parkin-Smith, G.; Taylor, D.N.; Anderson, D.; Farabaugh, R.; et al. The Role of Chiropractic Care in Providing Health Promotion and Clinical Preventive Services for Adult Patients with Musculoskeletal Pain: A Clinical Practice Guideline. J. Altern. Complement Med. 2021, 27, 850–867. [Google Scholar] [CrossRef]
- Hawk, C.; Schneider, M.J.; Haas, M.; Katz, P.; Dougherty, P.; Gleberzon, B.; Killinger, L.Z.; Weeks, J. Best Practices for Chiropractic Care for Older Adults: A Systematic Review and Consensus Update. J. Manip. Physiol. Ther. 2017, 40, 217–229. [Google Scholar] [CrossRef]
- Hawk, C.; Whalen, W.; Farabaugh, R.J.; Daniels, C.J.; Minkalis, A.L.; Taylor, D.N.; Anderson, D.; Anderson, K.; Crivelli, L.S.; Cark, M.; et al. Best Practices for Chiropractic Management of Patients with Chronic Musculoskeletal Pain: A Clinical Practice Guideline. J. Altern. Complement. Med. 2020, 26, 884–901. [Google Scholar] [CrossRef]
- Hegmann, K.T.; Travis, R.; Andersson, G.B.J.; Belcourt, R.M.; Carragee, E.J.; Donelson, R.; Eskay-Auerbach, M.; Galper, J.; Goertz, M.; Haldeman, S.; et al. Non-Invasive and Minimally Invasive Management of Low Back Disorders. J. Occup. Environ. Med. 2020, 62, e111. [Google Scholar] [CrossRef]
- Kawakami, M.; Takeshita, K.; Inoue, G.; Sekiguchi, M.; Fujiwara, Y.; Hoshino, M.; Kaito, T.; Kawaguchi, Y.; Minetama, M.; Orita, S.; et al. Japanese Orthopaedic Association (JOA) Clinical Practice Guidelines on the Management of Lumbar Spinal Stenosis, 2021—Secondary Publication. J. Orthop. Sci. 2023, 28, 46–91. [Google Scholar] [CrossRef]
- Keating, G.; Hawk, C.; Amorin-Woods, L.; Amorin-Woods, D.; Vallone, S.; Farabaugh, R.; Todd, A.; Ferrance, R.; Young, J.; O’Neill Bhogal, S.; et al. Clinical Practice Guideline for Best Practice Management of Pediatric Patients by Chiropractors: Results of a Delphi Consensus Process. J. Integr. Complement Med. 2024, 30, 216–232. [Google Scholar] [CrossRef]
- Kjaer, P.; Kongsted, A.; Hartvigsen, J.; Isenberg-Jørgensen, A.; Schiøttz-Christensen, B.; Søborg, B.; Krog, C.; Møller, C.M.; Halling, C.M.B.; Lauridsen, H.H.; et al. National Clinical Guidelines for Non-Surgical Treatment of Patients with Recent Onset Neck Pain or Cervical Radiculopathy. Eur. Spine J. 2017, 26, 2242–2257. [Google Scholar] [CrossRef]
- Kreiner, D.S.; Matz, P.; Bono, C.M.; Cho, C.H.; Easa, J.E.; Ghiselli, G.; Ghogawala, Z.; Reitman, C.A.; Resnick, D.K.; Watters, W.C.; et al. Guideline Summary Review: An Evidence-Based Clinical Guideline for the Diagnosis and Treatment of Low Back Pain. Spine J. 2020, 20, 998–1024. [Google Scholar] [CrossRef] [PubMed]
- Kreiner, D.S.; Hwang, S.W.; Easa, J.E.; Resnick, D.K.; Baisden, J.L.; Bess, S.; Cho, C.H.; DePalma, M.J.; Dougherty, P.; Fernand, R.; et al. An Evidence-Based Clinical Guideline for the Diagnosis and Treatment of Lumbar Disc Herniation with Radiculopathy. Spine J. 2014, 14, 180–191. [Google Scholar] [CrossRef] [PubMed]
- Kreiner, D.S.; Shaffer, W.O.; Baisden, J.L.; Gilbert, T.J.; Summers, J.T.; Toton, J.F.; Hwang, S.W.; Mendel, R.C.; Reitman, C.A. An Evidence-Based Clinical Guideline for the Diagnosis and Treatment of Degenerative Lumbar Spinal Stenosis (Update). Spine J. 2013, 13, 734–743. [Google Scholar] [CrossRef] [PubMed]
- Lisi, A.J.; Salsbury, S.A.; Hawk, C.; Vining, R.D.; Wallace, R.B.; Branson, R.; Long, C.R.; Burgo-Black, A.L.; Goertz, C.M. Chiropractic Integrated Care Pathway for Low Back Pain in Veterans: Results of a Delphi Consensus Process. J. Manip. Physiol. Ther. 2018, 41, 137–148. [Google Scholar] [CrossRef]
- Macfarlane, G.J.; Kronisch, C.; Dean, L.E.; Atzeni, F.; Häuser, W.; Fluß, E.; Choy, E.; Kosek, E.; Amris, K.; Branco, J.; et al. EULAR Revised Recommendations for the Management of Fibromyalgia. Ann. Rheum. Dis. 2017, 76, 318–328. [Google Scholar] [CrossRef]
- Ma, K.; Zhuang, Z.-G.; Wang, L.; Liu, X.-G.; Lu, L.-J.; Yang, X.-Q.; Lu, Y.; Fu, Z.-J.; Song, T.; Huang, D.; et al. The Chinese Association for the Study of Pain (CASP): Consensus on the Assessment and Management of Chronic Nonspecific Low Back Pain. Pain Res. Manag. 2019, 2019, e8957847. [Google Scholar] [CrossRef]
- Matz, P.G.; Meagher, R.J.; Lamer, T.; Tontz, W.L.; Annaswamy, T.M.; Cassidy, R.C.; Cho, C.H.; Dougherty, P.; Easa, J.E.; Enix, D.E.; et al. Guideline Summary Review: An Evidence-Based Clinical Guideline for the Diagnosis and Treatment of Degenerative Lumbar Spondylolisthesis. Spine J. 2016, 16, 439–448. [Google Scholar] [CrossRef]
- National Guideline Centre (UK). Low Back Pain and Sciatica in over 16s: Assessment and Management; National Institute for Health and Care Excellence (NICE): London, UK, 2016. [Google Scholar]
- National Guideline Centre (UK). Low Back Pain and Sciatica in over 16s: Assessment and Management; National Institute for Health and Care Excellence: Guidelines; National Institute for Health and Care Excellence (NICE): London, UK, 2020; ISBN 978-1-4731-2186-7. [Google Scholar]
- Qaseem, A.; Wilt, T.J.; McLean, R.M.; Forciea, M.A. Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of Physicians. Ann. Intern. Med. 2017, 166, 514–530. [Google Scholar] [CrossRef]
- Stochkendahl, M.J.; Kjaer, P.; Hartvigsen, J.; Kongsted, A.; Aaboe, J.; Andersen, M.; Andersen, M.O.; Fournier, G.; Hojgaard, B.; Jensen, M.B.; et al. National Clinical Guidelines for Non-Surgical Treatment of Patients with Recent Onset Low Back Pain or Lumbar Radiculopathy. Eur. Spine J. 2018, 27, 60–75. [Google Scholar] [CrossRef]
- Weis, C.A.; Pohlman, K.; Barrett, J.; Clinton, S.; da Silva-Oolup, S.; Draper, C.; Lee, J.; Kumar, R.; O’Beirne, M.; Stuber, K.; et al. Best-Practice Recommendations for Chiropractic Care for Pregnant and Postpartum Patients: Results of a Consensus Process. J. Manip. Physiol. Ther. 2022, 45, 469–489. [Google Scholar] [CrossRef]
- Whalen, W.; Farabaugh, R.J.; Hawk, C.; Minkalis, A.L.; Lauretti, W.; Crivelli, L.S.; Wyatt, L.; Sheppard, M.; Walters, S.A. Best-Practice Recommendations for Chiropractic Management of Patients with Neck Pain. J. Manip. Physiol. Ther. 2019, 42, 635–650. [Google Scholar] [CrossRef]
- Whalen, W.M.; Hawk, C.; Farabaugh, R.J.; Daniels, C.J.; Taylor, D.N.; Anderson, K.R.; Crivelli, L.S.; Anderson, D.R.; Thomson, L.M.; Sarnat, R.L. Best Practices for Chiropractic Management of Adult Patients with Mechanical Low Back Pain: A Clinical Practice Guideline for Chiropractors in the United States. J. Manip. Physiol. Ther. 2022, 45, 551–565. [Google Scholar] [CrossRef]
- Yu, H.; Côté, P.; Wong, J.J.; Shearer, H.M.; Mior, S.; Cancelliere, C.; Randhawa, K.; Ameis, A.; Carroll, L.J.; Nordin, M.; et al. Noninvasive Management of Soft Tissue Disorders of the Shoulder: A Clinical Practice Guideline from the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. Eur. J. Pain 2021, 25, 1644–1667. [Google Scholar] [CrossRef]
- Weis, C.A.; Stuber, K.; Murnaghan, K.; Wynd, S. Adverse Events from Spinal Manipulations in the Pregnant and Postpartum Periods: A Systematic Review and Update. J. Can. Chiropr. Assoc. 2021, 65, 32–49. [Google Scholar]
- Trager, R.J.; Dusek, J.A. Chiropractic Case Reports: A Review and Bibliometric Analysis. Chiropr. Man. Ther. 2021, 29, 17. [Google Scholar] [CrossRef]
- Whedon, J.M.; Petersen, C.L.; Schoellkopf, W.J.; Haldeman, S.; MacKenzie, T.A.; Lurie, J.D. The Association between Cervical Artery Dissection and Spinal Manipulation among US Adults. Eur. Spine J. 2023, 32, 3497–3504. [Google Scholar] [CrossRef]
- Whedon, J.M.; Petersen, C.L.; Li, Z.; Schoelkopf, W.J.; Haldeman, S.; MacKenzie, T.A.; Lurie, J.D. Association between Cervical Artery Dissection and Spinal Manipulative Therapy—A Medicare Claims Analysis. BMC Geriatr. 2022, 22, 917. [Google Scholar] [CrossRef]
- Church, E.W.; Sieg, E.P.; Zalatimo, O.; Hussain, N.S.; Glantz, M.; Harbaugh, R.E. Systematic Review and Meta-Analysis of Chiropractic Care and Cervical Artery Dissection: No Evidence for Causation. Cureus 2016, 8, e498. [Google Scholar] [CrossRef]
- Swait, G.; Finch, R. What Are the Risks of Manual Treatment of the Spine? A Scoping Review for Clinicians. Chiropr. Man. Ther. 2017, 25, 37. [Google Scholar] [CrossRef]
- Chu, E.C.-P.; Trager, R.J.; Lee, L.Y.-K.; Niazi, I.K. A Retrospective Analysis of the Incidence of Severe Adverse Events among Recipients of Chiropractic Spinal Manipulative Therapy. Sci. Rep. 2023, 13, 1254. [Google Scholar] [CrossRef]
- Farabaugh, R.; Hawk, C.; Taylor, D.; Daniels, C.; Noll, C.; Schneider, M.; McGowan, J.; Whalen, W.; Wilcox, R.; Sarnat, R.; et al. Cost of Chiropractic versus Medical Management of Adults with Spine-Related Musculoskeletal Pain: A Systematic Review. Chiropr. Man. Ther. 2024, 32, 8. [Google Scholar] [CrossRef]
- Trager, R.J.; Cupler, Z.A.; Srinivasan, R.; Casselberry, R.M.; Perez, J.A.; Dusek, J.A. Association between Chiropractic Spinal Manipulation and Gabapentin Prescription in Adults with Radicular Low Back Pain: Retrospective Cohort Study Using US Data. BMJ Open 2023, 13, e073258. [Google Scholar] [CrossRef]
- Kazis, L.E.; Ameli, O.; Rothendler, J.; Garrity, B.; Cabral, H.; McDonough, C.; Carey, K.; Stein, M.; Sanghavi, D.; Elton, D.; et al. Observational Retrospective Study of the Association of Initial Healthcare Provider for New-Onset Low Back Pain with Early and Long-Term Opioid Use. BMJ Open 2019, 9, e028633. [Google Scholar] [CrossRef]
- Trager, R.J.; Gliedt, J.A.; Labak, C.M.; Daniels, C.J.; Dusek, J.A. Association between Spinal Manipulative Therapy and Lumbar Spine Reoperation after Discectomy: A Retrospective Cohort Study. BMC Musculoskelet Disord. 2024, 25, 46. [Google Scholar] [CrossRef]
- Trager, R.J.; Cupler, Z.A.; Srinivasan, R.; Casselberry, R.M.; Perez, J.A.; Dusek, J.A. Chiropractic Spinal Manipulation and Likelihood of Tramadol Prescription in Adults with Radicular Low Back Pain: A Retrospective Cohort Study Using US Data. BMJ Open 2024, 14, e078105. [Google Scholar] [CrossRef]
- Côté, P.; Negrini, S.; Donzelli, S.; Kiekens, C.; Arienti, C.; Ceravolo, M.G.; Gross, D.P.; Battel, I.; Ferriero, G.; Lazzarini, S.G.; et al. Introduction to Target Trial Emulation in Rehabilitation: A Systematic Approach to Emulate a Randomized Controlled Trial Using Observational Data. Eur. J. Phys. Rehabil. Med. 2024, 60, 145–153. [Google Scholar] [CrossRef]
- Listl, S.; Jürges, H.; Watt, R.G. Causal Inference from Observational Data. Community Dent. Oral Epidemiol. 2016, 44, 409–415. [Google Scholar] [CrossRef]
- Trager, R.J.; Baumann, A.N.; Rogers, H.; Tidd, J.; Orellana, K.; Preston, G.; Baldwin, K. Efficacy of Manual Therapy for Sacroiliac Joint Pain Syndrome: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Man. Manip. Ther. 2024, 103, e39117. [Google Scholar] [CrossRef]
- Pershing, M.; Hirekhan, O.; Syed, A.; Elliott, J.O.; Toot, J. Documentation of International Classification of Headache Disorders Criteria in Patient Medical Records: A Retrospective Cohort Analysis. Cureus 2024, 16, e52209. [Google Scholar] [CrossRef]
- Minen, M.T.; Lindberg, K.; Wells, R.E.; Suzuki, J.; Grudzen, C.; Balcer, L.; Loder, E. Survey of Opioid and Barbiturate Prescriptions in Patients Attending a Tertiary Care Headache Center. Headache 2015, 55, 1183–1191. [Google Scholar] [CrossRef]
- Moore, C.; Adams, J.; Leaver, A.; Lauche, R.; Sibbritt, D. The Treatment of Migraine Patients within Chiropractic: Analysis of a Nationally Representative Survey of 1869 Chiropractors. BMC Complement Altern. Med. 2017, 17, 519. [Google Scholar] [CrossRef] [PubMed]
- Rist, P.M.; Hernandez, A.; Bernstein, C.; Kowalski, M.; Osypiuk, K.; Vining, R.; Long, C.R.; Goertz, C.; Song, R.; Wayne, P.M. The Impact of Spinal Manipulation on Migraine Pain and Disability: A Systematic Review and Meta-Analysis. Headache 2019, 59, 532–542. [Google Scholar] [CrossRef] [PubMed]
- Wayne, P.M. Chiropractic Care for Episodic Migraine; ClinicalTrials.gov Identifier: NCT06229834; Brigham and Women’s Hospital: Boston, MA, USA, 2024. [Google Scholar]
- Schneider, M.J.; Ammendolia, C.; Murphy, D.R.; Glick, R.M.; Hile, E.; Tudorascu, D.L.; Morton, S.C.; Smith, C.; Patterson, C.G.; Piva, S.R. Comparative Clinical Effectiveness of Nonsurgical Treatment Methods in Patients with Lumbar Spinal Stenosis: A Randomized Clinical Trial [with Consumer Summary]. JAMA Netw. Open 2019, 2, e186828. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Condition/Author | Year | Timing | Recommendation |
|---|---|---|---|
| Cervical radiculopathy | |||
| Chou | 2018 | NA | In favor: multimodal |
| Cervicogenic headache | |||
| Côté | 2019 | NA | In favor |
| Degenerative lumbar spinal stenosis | |||
| Kawakami | 2023 | NA | Insufficient evidence |
| Kreiner | 2013 | NA | Insufficient evidence |
| Degenerative lumbar spondylolisthesis | |||
| Matz | 2016 | NA | Insufficient evidence |
| Developmental concerns | |||
| Keating | 2023 | NA | Insufficient evidence |
| Disease prevention | |||
| Hawk | 2021 | NA | Not in favor |
| Fibromyalgia | |||
| Hawk | 2020 | NA | In favor: multimodal |
| Macfarlane | 2017 | NA | Not in favor |
| Improving immune function | |||
| Hawk | 2021 | NA | Not in favor |
| Low back pain | |||
| Alperovitch-Najenson | 2023 | Chronic | In favor: multimodal |
| Bussières | 2018 | Acute or subacute | Not in favor |
| Bussières | 2018 | Chronic | In favor |
| Chou | 2018 | Acute | In favor: multimodal |
| Globe | 2016 | Acute | In favor |
| Globe | 2016 | Chronic | In favor |
| Hawk | 2020 | Chronic | In favor: multimodal |
| Hegmann | 2020 | Acute | In favor: multimodal |
| Hegmann | 2020 | Chronic | In favor: multimodal |
| Kreiner | 2020 | Acute | In favor |
| Kreiner | 2020 | Chronic | In favor |
| Lisi | 2018 | Acute or subacute | In favor |
| Lisi | 2018 | Chronic | In favor |
| Ma | 2019 | Chronic | In favor |
| NICE (UK) | 2016 | NA | In favor: multimodal |
| NICE (UK) | 2020 | NA | In favor: multimodal |
| Qaseem | 2017 | Acute or subacute | In favor |
| Stochkendahl | 2018 | Acute or subacute | In favor: multimodal |
| Whalen | 2022 | NA | In favor: multimodal |
| LBP in older individuals | |||
| Hawk | 2017 | NA | Insufficient evidence |
| Menopause-associated vasomotor symptoms | |||
| Carpenter | 2015 | NA | Not in favor |
| Neck pain | |||
| Bier | 2018 | NA | In favor: multimodal |
| Blanpied | 2017 | Chronic | In favor: multimodal |
| Bryans | 2014 | Acute or subacute | In favor: multimodal |
| Bryans | 2014 | Chronic | In favor |
| Bussières | 2016 | Acute or subacute | In favor |
| Bussières | 2016 | Chronic | In favor: multimodal |
| Chou | 2018 | Acute | In favor: multimodal |
| Hawk | 2020 | Chronic | In favor: multimodal |
| Kjaer | 2017 | Acute or subacute | In favor: multimodal |
| Whalen | 2019 | Acute or subacute | In favor: multimodal |
| Whalen | 2019 | Chronic | In favor: multimodal |
| Neck pain with headache | |||
| Blanpied | 2017 | Subacute | In favor |
| Neck pain with mobility deficits | |||
| Blanpied | 2017 | Acute or subacute | In favor |
| Neck pain with movement coordination deficits | |||
| Blanpied | 2017 | Subacute | In favor: multimodal |
| Pregnancy-related or postpartum LBP and/or PGP | |||
| Weis | 2022 | NA | In favor |
| Sciatica/LR | |||
| Bussières | 2018 | NA | In favor: multimodal |
| Chou | 2018 | NA | In favor: multimodal |
| Kreiner | 2014 | NA | In favor |
| NICE (UK) | 2016 | NA | In favor: multimodal |
| NICE (UK) | 2020 | NA | In favor: multimodal |
| Stochkendahl | 2018 | Acute or subacute | In favor: multimodal |
| Sciatica/LR (with progressive motor loss) | |||
| Hegmann | 2020 | NA | Not in favor |
| Sciatica/LR (without deficit) | |||
| Hegmann | 2020 | NA | In favor: multimodal |
| Shoulder pain | |||
| Yu | 2021 | NA | In favor |
| Tension-type headache | |||
| Côté | 2019 | Chronic | Not in favor |
| Côté | 2019 | Episodic | Not in favor |
| Dowell | 2022 | NA | In favor |
| Hawk | 2020 | Chronic | In favor: multimodal |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trager, R.J.; Bejarano, G.; Perfecto, R.-P.T.; Blackwood, E.R.; Goertz, C.M. Chiropractic and Spinal Manipulation: A Review of Research Trends, Evidence Gaps, and Guideline Recommendations. J. Clin. Med. 2024, 13, 5668. https://doi.org/10.3390/jcm13195668
Trager RJ, Bejarano G, Perfecto R-PT, Blackwood ER, Goertz CM. Chiropractic and Spinal Manipulation: A Review of Research Trends, Evidence Gaps, and Guideline Recommendations. Journal of Clinical Medicine. 2024; 13(19):5668. https://doi.org/10.3390/jcm13195668
Chicago/Turabian StyleTrager, Robert J., Geronimo Bejarano, Romeo-Paolo T. Perfecto, Elizabeth R. Blackwood, and Christine M. Goertz. 2024. "Chiropractic and Spinal Manipulation: A Review of Research Trends, Evidence Gaps, and Guideline Recommendations" Journal of Clinical Medicine 13, no. 19: 5668. https://doi.org/10.3390/jcm13195668
APA StyleTrager, R. J., Bejarano, G., Perfecto, R.-P. T., Blackwood, E. R., & Goertz, C. M. (2024). Chiropractic and Spinal Manipulation: A Review of Research Trends, Evidence Gaps, and Guideline Recommendations. Journal of Clinical Medicine, 13(19), 5668. https://doi.org/10.3390/jcm13195668