Abstract
Background/Objectives: Integrating the cytotoxic drug busulfan into a high-dose chemotherapy regimen prior to autologous hematopoietic stem cell rescue in patients with high-risk neuroblastoma has improved the survival of children battling this deadly disease. Busulfan-induced toxicities can, however, be severe. Here, we describe the diagnosis and successful treatment of acute pulmonary injury by total-body-weight-adjusted busulfan therapy in two children with high-risk neuroblastoma. Case series: Patient 1 developed life-threatening biphasic acute respiratory failure on days +60 and +100 after busulfan therapy, requiring intubation and invasive mechanical ventilation. Despite intensive anti-inflammatory and immunomodulatory therapy, including systemic corticosteroids, topical inhalation regimens, azithromycin, nintedanib and extracorporal photopheresis, patient 1 required extended intensive care measures and non-invasive respiratory support for a total of 20 months. High-resolution computed tomography showed diffuse intra-alveolar and interstitial patterns. Patient 2 developed partial respiratory failure with insufficient oxygen saturation and dyspnea on day +52 after busulfan therapy. Symptoms were resolved after 6 months of systemic corticosteroids, topical inhalation regimens and azithromycin. High-resolution computed tomography showed atypical pneumonic changes with ground-glass opacities. While both patients fully recovered without evidence of pulmonary fibrosis, cancer therapy had to be paused and then modified until full recovery from busulfan-induced lung injury. Conclusions: Busulfan-induced lung injury requires prompt diagnosis and intervention. Symptoms and signs are nonspecific and difficult to differentiate from other causes. Therapeutic busulfan drug level monitoring and the identification of patients at risk for drug overdosing through promoter polymorphisms in the glutathione S-transferase alpha 1 gene encoding the main enzyme in busulfan metabolism are expected to reduce the risk of busulfan-induced toxicities.
1. Introduction
Busulfan is a key cytotoxic drug used in high-dose chemotherapy followed by autologous hematopoietic stem cell transplantation in patients with high-risk neuroblastoma [1,2,3]. The busulfan/melphalan high-dose chemotherapy (BuMel HD) regimen has become the standard of care in the SIOPEN high-risk (HR) strategy following the demonstration of its superiority over the carboplatin, etoposide and melphalan high-dose chemotherapy (CEM HD) regimen in the HR-NBL1/SIOPEN randomized phase 3 clinical trial (NCT01704716) [4]. In the HR-NBL1/SIOPEN trial, 50% of patients receiving the BuMel HD regimen, and only 38% receiving the CEM HD regimen, survived for 3 years without event. At the 5-year mark, 45% of patients receiving the BuMel HD regimen versus 33% receiving the CEM HD regimen survived without an event, while 5-year overall survival was 54% for the BuMel HD patient subgroup and 41% for the CEM HD patient subgroup [4].
Busulfan can, however, cause major toxicities, including sinusoidal obstruction syndrome and restrictive lung disease [2,5,6]. Busulfan-induced lung injury is a rare but critical complication that can trigger life-threatening acute or chronic respiratory failure [7,8]. The literature on managing busulfan-induced lung injury in the pediatric patient population is scarce, with only few reports existing [7,8,9]. Here, we share the clinical, radiological and laboratory features as well as the pulmonological and oncological management of two patients with high-risk neuroblastoma and busulfan-induced lung injury.
2. Case Report for Patient 1
A 5-year-old boy with metastasized high-risk neuroblastoma (primary thoracic tumor, multiple osteomedullar metastases; genetics: diploid MYCN, wildtype ALK) was transferred to our center with very good partial response at the end of induction and completely resected primary tumor for consolidation therapy (Figure 1) according to recommendations of the pan-European SIOPEN Group [10] and German Society of Pediatric Oncology and Hematology [11]. Busulfan dosages were adjusted to the total body weight, followed by autologous hematopoietic stem cell transplantation (10.48 × 106 CD34 + cells/kg body weight). Neutrophil and thrombocyte engraftment was achieved on days +12 and +19, respectively, and the patient was discharged in good clinical condition on day +30. Restaging on day +45 demonstrated stable disease according to the revised International Neuroblastoma Response Criteria [12]. At this timepoint, there was no evidence of lung injury during physical examination and monitoring of the vital parameters. Maintenance therapy was started with the GD2-directed dinutuximab beta monoclonal antibody on day +60.
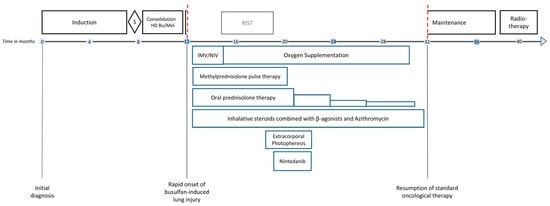
Figure 1.
Schematic diagram illustrating the medical interventions for busulfan-induced lung injury in patient 1 and its consequences for cancer therapy. Induction polychemotherapy was administered in accordance with the rapid platinum-containing induction schedule (carboplatin, cisplatin, vincristine, etoposide, cyclophosphamide) according to the SIOPEN HR-NBL1 protocol (NCT01704716). Consolidation therapy consisted of weight-adjusted high-dose chemotherapy with i.v. busulfan and melphalan (HD BuMel). Maintenance immunotherapy included five cycles of the monoclonal anti-GD2 antibody dinutuximab beta. Radiotherapy of the preoperative tumor bed was administered at 21.6 Gy. Acute respiratory failure and acute respiratory distress syndrome due to busulfan-induced lung injury required invasive mechanical ventilation (IMV) including nitric oxide supplementation followed by prolonged weaning employing non-invasive ventilation (NIV). A total of eight methylprednisolone pulses were administered. Oral prednisolone (2 mg/kg/d) was given in between pulses and was carefully tapered. RIST, molecularly targeted multimodal therapy consisting of metronomic courses of rapamycin/dasatinib and irinotecan/temozolomide. S, surgery. The red dashed line indicates the interruption of the standard oncological treatment of patient 1 due to busulfan-induced lung injury.
On day 62+, patient 1 developed rapid respiratory deterioration, requiring intubation and invasive mechanical ventilation (IMV) with 100% oxygen and 20 ppm nitric oxide, the latter due to refractory hypoxemia. A chest X-ray showed pathological signs compatible with right-sided pleuropneumonia and overall pulmonary edema (Figure 2A). Immunotherapy was halted. No pathogens were identified in bronchoalveolar lavage, respiratory swabs, blood, urine or stool samples. Broad empirical antibiotic and antifungal therapy was administered immediately after the collection of biospecimens for infectious disease work-up. Assuming a pulmonary cytokine-release syndrome, anti-interleukin 6 therapy with tocilizumab was administered without clear positive effect. After 5 days of IMV and intravenous hydrocortisone (100 mg/m2/d), patient 1 was extubated and continued with non-invasive high-flow nasal cannula therapy.
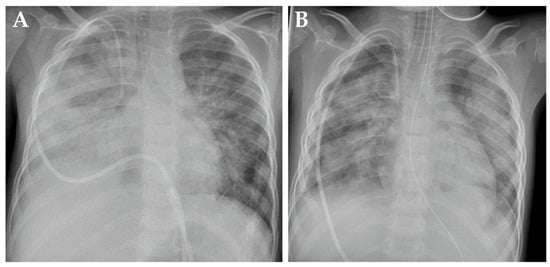
Figure 2.
Chest X-rays from patient 1 demonstrating signs of busulfan-induced lung injury on day +62 (A) and day +74 (B) after high-dose chemotherapy.
On day +74, respiratory failure with rapidly evolving tachydyspnoea recurred. The chest X-ray now demonstrated bilateral pulmonary infiltrates and pleural effusions (Figure 2B). Patient 1 was re-intubated and placed on IMV as an emergency measure for 6 days. Systemic inflammatory parameters were again high but without a causal pathogen (extensive testing). Empiric antibiotic and antifungal regimens were nevertheless applied. High-resolution computed tomography (HRCT) showed increased ground-glass opacification and consolidation, particularly in both lower lobes (Figure 3A). Busulfan-induced lung injury was the leading differential diagnosis at this stage, and a methylprednisolone pulse was administered (Figure 1). This anti-inflammatory therapy improved the respiratory situation, eventually enabling successful extubation. Patient 1 required non-invasive ventilation followed by high-flow nasal cannula therapy and continuous oxygen supplementation via a nasal cannula for 20 months (Figure 1).
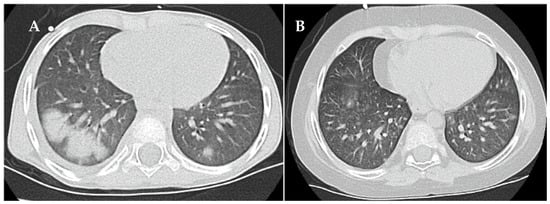
Figure 3.
High-resolution computed tomography findings of busulfan-induced lung injury in patient 1 at diagnosis (A) and at follow-up eight months after start of the anti-inflammatory and immunomodulatory therapy (B).
Treatment of busulfan-induced lung injury included a total of eight methylprednisolone pulses and continuous prednisolone therapy at a dose of 2 mg/kg/d, which could only be tapered from month 4 onwards (Figure 1). The systemic corticosteroid therapy, causing the full spectrum of Cushing’s disease, was combined with inhalative corticosteroids, inhalative short-acting β-agonists and oral azithromycin therapy in line with the graft-versus-host lung stage 1 treatment protocol used in the allogeneic setting, as we considered the evidence for successful anti-inflammatory therapy of the lung high when following these recommendations. In total, 15 cycles of extracorporal photopheresis were also performed to employ its immunomodulatory effects [13,14,15] against the as yet not fully understood molecular cascades causing lung injury (Figure 1). HRCT performed at 8 months after the clinical onset of busulfan-induced lung injury showed that the consolidation had resolved (Figure 3B). Spirometry presented a restrictive pattern with stepwise amelioration over time. To delay the potential initiation and progression of fibrotic processes in the lung, oral therapy with the small-molecule tyrosine kinase inhibitor, nintedanib, was administered for 3 months [16]. The patient fully recovered with no remaining signs of busulfan-induced lung injury in spirometry. Standard oncological therapy (radiotherapy of the preoperative thoracic tumor bed followed by immunotherapy) could not be administered. Therefore, four cycles of RIST therapy (NCT01467986) were administered as a bridging therapy, which needed to be discontinued to treat infectious complications, most likely due to the extended immunosuppression caused by the combination with corticosteroid therapy. Patient 1 resumed standard oncological therapy after recovery from the busulfan-induced lung injury and tolerated the dinutuximab beta-based maintenance therapy very well.
3. Case Report for Patient 2
A 2.5-year-old boy was diagnosed with metastasized high-risk neuroblastoma in our center (primary tumor: bilateral abdominal sympathetic chains with infiltration of left kidney; metastases: osteomedullar lesions, lymph nodes; genetics: diploid MYCN, ALK R.1275Q mutation with allele frequency in tumor: 21.4%, blood plasma: 40.1%, bone marrow plasma: 40.5%). Patient 2 received therapy according to GPOH NB2017 Guidance for the high-risk group [11] including the BuMel HD regimen with total-body-weight-adjusted dosing of intravenous busulfan as also recommended by the pan-European SIOPEN Group [10] (Figure 4). Patient 2 had achieved a complete remission at the end of induction and developed hepatic sinusoidal obstruction syndrome on day +6 of the consolidation therapy, which was successfully treated with defibrotide [17,18]. Neutrophil engraftment was achieved on day +13 and platelet engraftment, slightly delayed, on day +60.
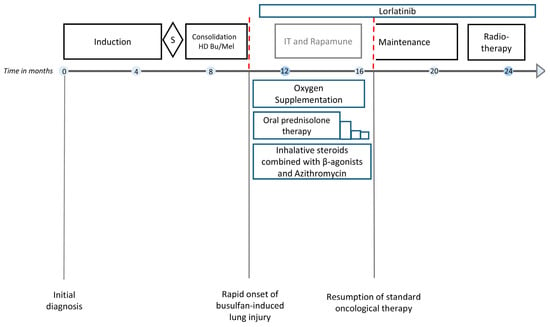
Figure 4.
Schematic diagram illustrating the medical interventions for busulfan-induced lung injury in patient 2 and its consequences for the treatment of high-risk neuroblastoma according to the GPOH NB2017 Guidance. Induction polychemotherapy was administered in accordance with the GPOH induction schedule (3xN5 cycle: vindesine, cisplatin, etoposide; 3xN6 cycle: vincristine, dacarbazine, ifosfamide, doxorubicin). Consolidation therapy consisted of weight-adjusted high-dose chemotherapy with i.v. busulfan and melphalan (HD Bu/Mel). Maintenance immunotherapy included five cycles with the monoclonal anti-GD2 antibody dinutuximab beta. Radiotherapy was given at 21.6 Gy to the preoperative tumor bed. Acute partial respiratory failure due to busulfan-induced lung injury required continuous oxygen supplementation. Oral prednisolone was started at 2 mg/kg/d, then gradually tapered. IT and rapamune, multimodal therapy consisting of metronomic courses of rapamune and irinotecan/temozolomide modified from the RIST scheme (NCT01467986), with the multityrosine kinase inhibitor dasatinib replaced by third-generation ALK tyrosine kinase inhibitor lorlatinib; S, surgery. The red dashed line indicates the interruption of the standard oncological treatment of patient 2 due to busulfan-induced lung injury.
At day +52 after autologous stem cell transplantation, patient 2 developed partial respiratory failure with dyspnea and need for continuous low-level oxygen. The chest X-ray showed moderate bilateral infiltrates and pulmonary venous congestion. HRCT imaging revealed atypical pneumonic changes, characterized by ground-glass opacification and patchy consolidation in the lower lobes (Figure 5A). An empirical antibiotic and antifungal therapy was initiated. No pathogen was identified in a comprehensive infectious diagnostic work-up. At disease onset, radiological signs and echocardiographic findings did not suggest pulmonary veno-occlusive disease. Systemic prednisolone therapy (2 mg/kg/d) stabilized respiratory status. Topical treatment comprising inhalative corticosteroids and short-acting β-agonists in combination with azithromycin was initiated. Patient 2 required continuous oxygen supplementation for 6 months (Figure 4). A modified version of the four-compound RIST therapy (NCT01467986, experimental arm; dasatinib multityrosine kinase inhibitor substituted by the third-generation ALK tyrosine kinase inhibitor, lorlatinib) was employed as a bridging oncological therapy for 6 months. The therapy was paused according to standard oncological procedures in case of (respiratory tract) infections. HRCT findings 6 months after partial respiratory failure onset showed regression of consolidations and opacities and no evidence of pulmonary fibrosis (Figure 5B). Patient 2 resumed and completed the standard oncological treatment regimen and has remained in first complete remission until the date of publication (Figure 4).
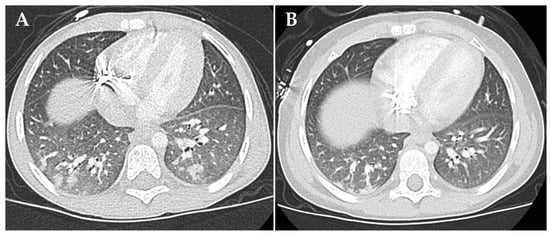
Figure 5.
High-resolution computed tomography findings of busulfan-induced lung injury in patient 2 at diagnosis (A) and six months after start of the anti-inflammatory therapy (B). (A) Shown are atypical pneumonic changes, characterized by ground-glass opacification and patchy consolidation in the lower lobes. (B) Shown is the regression of consolidations and opacities. There is no evidence of pulmonary fibrosis.
4. Discussion
Diagnosing drug-induced lung disease relies on the temporal association between exposure to the causative agent and onset of respiratory signs and symptoms [19]. Excluding other potential causes of lung damage is the most critical factor for accurate diagnosis [20,21]. Busulfan-induced lung injury is a diagnosis of exclusion due to the lack of unique clinical features, specific biomarkers and histological findings [22,23]. Thorough conduct of comprehensive diagnostic testing is essential, particularly to rule out infections frequently caused by atypical pathogens in immunocompromised patients [7]. Busulfan-induced lung injury is a complex and potentially life-threatening condition, exemplified in the clinical courses of our two patients, that requires prompt diagnosis and treatment [7,8,19]. Cancer therapy must, unfortunately, be interrupted in most cases, thus substantially increasing the risk for progressive disease or relapse in the patients affected.
Pulmonary toxicity associated with busulfan can range from mild interstitial pneumonitis to end-stage pulmonary fibrosis and occurs at variable times following drug administration [7,19]. Clinicians must be vigilant for respiratory symptoms in patients who receive busulfan and employ a multidisciplinary approach in case of complications. Regular monitoring of pulmonary function and imaging facilitate detection of very early signs of drug-induced lung injury [24]. HRCT is the preferred imaging modality to diagnose and monitor pulmonary toxicity over time [24,25]. Patterns associated with busulfan toxicity include ground-glass opacities, peripheral and peribronchial consolidation, centrilobular nodules and reticulation [23]. Persisting HRCT changes suggest drug-induced lung damage [23,25]. Pulmonary function tests (spirometry, lung diffusion testing) are required to measure pulmonary damage severity and assess therapy response [7,19,26].
Cell-mediated immune reactions, including cytokine release, are suspected to be at the root of busulfan-induced lung injury, although the pathophysiology has not yet been fully elucidated. Systemic anti-inflammatory corticosteroid therapy is, therefore, essential [7,27], with the severity of respiratory pathophysiology and response determining cumulative dose and therapy duration [26]. Apart from corticosteroids and supportive measures, no other evidence-based therapies for drug-induced pneumopathies exist to date.
The extended therapeutic approach applied in this case series is in line with treatment protocols for other lung diseases with substantial inflammatory activity, including pulmonary graft-versus-host disease, bronchiolitis obliterans syndrome and interstitial lung diseases. Topical therapy with inhalative corticosteroids was combined with short-acting β-agonists in line with the expert opinion for treating chronic inflammation [28,29]. The well-characterized anti-inflammatory and immunomodulatory properties of azithromycin [30] have been shown to reduce the incidence of infectious exacerbations in patients with chronic obstructive pulmonary disease [31] and non-cystic fibrosis bronchiectasis [32].
Extracorporeal photopheresis, which exposes mononuclear cells to ultraviolet A irradiation in the presence of a photosensitizing agent, acts by inducing apoptosis and dendritic cell differentiation from monocytes as well as modifying cytokine profiles and T-cell subpopulations to promote immune tolerance [13,14,15]. As excessive inflammatory processes are hypothesized to trigger busulfan-induced lung injury, with the eventual onset of tissue fibrosis [33], we also added multiple cycles of extracorporeal photopheresis to the treatment schedule for patient 1. We hypothesized that its immunomodulatory effects could attenuate the decline in pulmonary function [33,34,35] and help reduce the corticosteroid dose necessary to suppress inflammatory cascades in the lung [36]. The small-molecule tyrosine kinase inhibitor, nintedanib, has previously been shown to inhibit fibrotic remodeling of lung tissue in preclinical models [37,38]. Nintedanib effectively decelerated progression of fibrosis and respiratory function decline in adults with interstitial lung disease [16], and an acceptable safety profile was demonstrated in the phase 3 InPedILD trial (NCT04093024) in children with fibrosing interstitial lung disease [39]. To prevent fibrotic lung disease, we also treated patient 1 with nintedanib [16].
The pharmacokinetic properties of busulfan have been intensely studied in recent years [6,40,41]. Inter-patient variability of busulfan plasma concentration is high, risking stronger toxicity in patients with high plasma concentrations [42]. Busulfan clearance is particularly variable in the pediatric population and is higher in young children [6,43]. Several studies have highlighted the benefits of therapeutic drug monitoring approaches to busulfan dosing [41,44,45,46], which has become the standard of care in the allogeneic transplant setting. While total-body-weight-based dosing of intravenous busulfan has achieved the desired therapeutic drug level in the past [15,47], implementing advanced therapeutic drug monitoring may improve the toxicity profile of the BuMel HD regimen, which improves survival of patients with high-risk neuroblastoma [4]. The hepatic busulfan metabolism is mediated by glutathione S-transferases [48,49,50]. Functional promoter polymorphisms in the main enzyme, glutathione S-transferase alpha 1 (GSTA1), have been shown to influence enzyme activity and, thus, pharmacokinetics and toxicity [51,52,53,54]. Pharmacogenomic data obtained prior to implementation of the BuMel HD regimen may add information to better understand busulfan exposure and the double-edged sword of busulfan efficacy or toxicity in individual patients when associated with pharmacokinetics.
5. Conclusions
The busulfan drug used in the high-dose chemotherapy regimen against high-risk neuroblastoma can cause major toxicities including restrictive lung disease. This case series describes the multimodal therapy of busulfan-induced lung toxicity with varying severity, and its control and complete resolution of symptoms, in pediatric patients with high-risk neuroblastoma. Early diagnosis as well as systemic and topical anti-inflammatory and immunomodulatory therapies present the cornerstone of its management. Therapeutic drug monitoring combined with pharmacogenetics may contribute to reduce busulfan toxicity in this vulnerable patient group.
Author Contributions
Conceptualization, H.E.D.; writing—original draft preparation, all authors; visualization, S.C. and S.V.; supervision, A.G., M.A.M., A.E. and H.E.D.; project administration, A.E. and H.E.D.; funding acquisition, A.E. and H.E.D. All authors have read and agreed to the published version of the manuscript.
Funding
This project was supported by a grant from the Deutsche Krebshilfe (German Cancer Aid) within the funding program Cancer Therapy Studies, grant number 70113414 (study name: HR-NBL2/SIOPEN).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. Patients were enrolled in the registry for neonates, infants, children, adolescents, and adults with newly diagnosed and/or relapsed neuroblastic tumors (NB Registry 2016), which was approved by the Ethics Committee of Cologne University on 3 April 2017.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Hartmann, O.; Valteau-Couanet, D.; Vassal, G.; Lapierre, V.; Brugières, L.; Delgado, R.; Couanet, D.; Lumbroso, J.; Benhamou, E. Prognostic factors in metastatic neuroblastoma in patients over 1 year of age treated with high-dose chemotherapy and stem cell transplantation: A multivariate analysis in 218 patients treated in a single institution. Bone Marrow Transplant. 1999, 23, 789–795. [Google Scholar] [CrossRef] [PubMed]
- Proust-Houdemont, S.; Pasqualini, C.; Blanchard, P.; Dufour, C.; Benhamou, E.; Goma, G.; Semeraro, M.; Raquin, M.-A.; Hartmann, O.; Valteau-Couanet, D. Busulfan-melphalan in high-risk neuroblastoma: The 30-year experience of a single institution. Bone Marrow Transplant. 2016, 51, 1076–1081. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Granger, M.M.; Naranjo, A.; Bagatell, R.; DuBois, S.G.; McCune, J.S.; Tenney, S.C.; Weiss, B.D.; Mosse, Y.P.; Asgharzadeh, S.; Grupp, S.A.; et al. Myeloablative Busulfan/Melphalan Consolidation following Induction Chemotherapy for Patients with Newly Diagnosed High-Risk Neuroblastoma: Children’s Oncology Group Trial ANBL12P1. Transplant. Cell. Ther. 2021, 27, 490.e1–490.e8. [Google Scholar] [CrossRef] [PubMed]
- Ladenstein, R.; Pötschger, U.; Pearson, A.D.J.; Brock, P.; Luksch, R.; Castel, V.; Yaniv, I.; Papadakis, V.; Laureys, G.; Malis, J.; et al. Busulfan and melphalan versus carboplatin, etoposide, and melphalan as high-dose chemotherapy for high-risk neuroblastoma (HR-NBL1/SIOPEN): An international, randomised, multi-arm, open-label, phase 3 trial. Lancet Oncol. 2017, 18, 500–514. [Google Scholar] [CrossRef] [PubMed]
- Schechter, T.; Perez-Albuerne, E.; Lin, T.F.; Irwin, M.S.; Essa, M.; Desai, A.V.; Frangoul, H.; Yanik, G.; Dupuis, L.L.; Jacobsohn, D.; et al. Veno-occlusive disease after high-dose busulfan-melphalan in neuroblastoma. Bone Marrow Transplant. 2020, 55, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Veal, G.J.; Nguyen, L.; Paci, A.; Riggi, M.; Amiel, M.; Valteau-Couanet, D.; Brock, P.; Ladenstein, R.; Vassal, G. Busulfan pharmacokinetics following intravenous and oral dosing regimens in children receiving high-dose myeloablative chemotherapy for high-risk neuroblastoma as part of the HR-NBL-1/SIOPEN trial. Eur. J. Cancer 2012, 48, 3063–3072. [Google Scholar] [CrossRef] [PubMed]
- Matijasic, N.; Bonevski, A.; Tokic Pivac, V.; Pavic, I. busulfan-induced Lung Injury in Pediatric Oncology Patients-Review of the Literature with an Illustrative Case. Pediatr. Allergy Immunol. Pulmonol. 2019, 32, 86–91. [Google Scholar] [CrossRef]
- Jain, R.; Gupta, K.; Bhatia, A.; Bansal, A.; Bansal, D. Hepatic Sinusoidal-obstruction Syndrome and busulfan-induced Lung Injury in a Post-autologous Stem Cell Transplant Recipient. Indian Pediatr. 2017, 54, 765–770. [Google Scholar] [CrossRef]
- Pearl, M. Busulfan lung. Am. J. Dis. Child. 1977, 131, 650–652. [Google Scholar]
- Michel, G.; Valteau-Couanet, D.; Gentet, J.C.; Esperou, H.; Socié, G.; Méchinaud, F.; Doz, F.; Neven, B.; Bertrand, Y.; Galambrun, C.; et al. Weight-based strategy of dose administration in children using intravenous busulfan: Clinical and pharmacokinetic results. Pediatr. Blood Cancer 2012, 58, 90–97. [Google Scholar] [CrossRef]
- Simon, T.; Hero, B.; Schulte, J.H.; Deubzer, H.; Hundsdoerfer, P.; von Schweinitz, D.; Fuchs, J.; Schmidt, M.; Prasad, V.; Krug, B.; et al. 2017 GPOH Guidelines for Diagnosis and Treatment of Patients with Neuroblastic Tumors. Klin. Padiatr. 2017, 229, 147–167. [Google Scholar] [CrossRef] [PubMed]
- Park, J.R.; Bagatell, R.; Cohn, S.L.; Pearson, A.D.; Villablanca, J.G.; Berthold, F.; Burchill, S.; Boubaker, A.; McHugh, K.; Nuchtern, J.G.; et al. Revisions to the International Neuroblastoma Response Criteria: A Consensus Statement From the National Cancer Institute Clinical Trials Planning Meeting. J. Clin. Oncol. 2017, 35, 2580–2587. [Google Scholar] [CrossRef] [PubMed]
- Lamioni, A.; Parisi, F.; Isacchi, G.; Giorda, E.; Di Cesare, S.; Landolfo, A.; Cenci, F.; Bottazzo, G.F.; Carsetti, R. The immunological effects of extracorporeal photopheresis unraveled: Induction of tolerogenic dendritic cells in vitro and regulatory T cells in vivo. Transplantation 2005, 79, 846–850. [Google Scholar] [CrossRef] [PubMed]
- Xia, C.Q.; Campbell, K.A.; Clare-Salzler, M.J. Extracorporeal photopheresis-induced immune tolerance: A focus on modulation of antigen-presenting cells and induction of regulatory T cells by apoptotic cells. Curr. Opin. Organ Transplant. 2009, 14, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Couriel, D.; Hosing, C.; Saliba, R.; Shpall, E.J.; Andelini, P.; Popat, U.; Donato, M.; Champlin, R. Extracorporeal photopheresis for acute and chronic graft-versus-host disease: Does it work? Biol. Blood Marrow Transplant. 2006, 12 (Suppl. 2), 37–40. [Google Scholar] [CrossRef] [PubMed]
- Flaherty, K.R.; Wells, A.U.; Cottin, V.; Devaraj, A.; Walsh, S.L.F.; Inoue, Y.; Richeldi, L.; Kolb, M.; Tetzlaff, K.; Stowasser, S.; et al. Nintedanib in Progressive Fibrosing Interstitial Lung Diseases. N. Engl. J. Med. 2019, 381, 1718–1727. [Google Scholar] [CrossRef]
- Corbacioglu, S.; Greil, J.; Peters, C.; Wulffraat, N.; Laws, H.J.; Dilloo, D.; Strahm, B.; Gross-Wieltsch, U.; Sykora, K.W.; Ridolfi-Lüthy, A.; et al. Defibrotide in the treatment of children with veno-occlusive disease (VOD): A retrospective multicentre study demonstrates therapeutic efficacy upon early intervention. Bone Marrow Transplant. 2004, 33, 189–195. [Google Scholar] [CrossRef]
- Richardson, P.G.; Riches, M.L.; Kernan, N.A.; Brochstein, J.A.; Mineishi, S.; Termuhlen, A.M.; Arai, S.; Grupp, S.A.; Guinan, E.C.; Martin, P.L.; et al. Phase 3 trial of defibrotide for the treatment of severe veno-occlusive disease and multi-organ failure. Blood 2016, 127, 1656–1665. [Google Scholar] [CrossRef]
- Limper, A.H. Chemotherapy-induced lung disease. Clin. Chest Med. 2004, 25, 53–64. [Google Scholar] [CrossRef]
- Ellis, S.J.; Cleverley, J.R.; Müller, N.L. Drug-induced lung disease: High-resolution CT findings. AJR Am. J. Roentgenol. 2000, 175, 1019–1024. [Google Scholar] [CrossRef]
- Distefano, G.; Fanzone, L.; Palermo, M.; Tiralongo, F.; Cosentino, S.; Inì, C.; Galioto, F.; Vancheri, A.; Torrisi, S.E.; Mauro, L.A.; et al. HRCT Patterns of Drug-Induced Interstitial Lung Diseases: A Review. Diagnostics 2020, 10, 244. [Google Scholar] [CrossRef] [PubMed]
- Matsuno, O. Drug-induced interstitial lung disease: Mechanisms and best diagnostic approaches. Respir. Res. 2012, 13, 39. [Google Scholar] [CrossRef] [PubMed]
- Cleverley, J.R.; Screaton, N.J.; Hiorns, M.P.; Flint, J.D.; Müller, N.L. Drug-induced lung disease: High-resolution CT and histological findings. Clin. Radiol. 2002, 57, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Massin, F.; Fur, A.; Reybet-Degat, O.; Camus, P.; Jeannin, L. Busulfan-induced pneumopathy. Rev. Mal. Respir. 1987, 4, 3–10. [Google Scholar] [PubMed]
- Padley, S.P.; Adler, B.; Hansell, D.M.; Müller, N.L. High-resolution computed tomography of drug-induced lung disease. Clin. Radiol. 1992, 46, 232–236. [Google Scholar] [CrossRef]
- Conte, P.; Ascierto, P.A.; Patelli, G.; Danesi, R.; Vanzulli, A.; Sandomenico, F.; Tarsia, P.; Cattelan, A.; Comes, A.; De Laurentiis, M.; et al. Drug-induced interstitial lung disease during cancer therapies: Expert opinion on diagnosis and treatment. ESMO Open 2022, 7, 100404. [Google Scholar] [CrossRef]
- Oliner, H.; Schwartz, R.; Rubio, F.; Dameshek, W. Interstitial pulmonary fibrosis following busulfan therapy. Am. J. Med. 1961, 31, 134–139. [Google Scholar] [CrossRef]
- Barnes, P.J. Scientific rationale for inhaled combination therapy with long-acting β2-agonists and corticosteroids. Eur. Respir. J. 2002, 19, 182–191. [Google Scholar] [CrossRef]
- Bos, S.; Murray, J.; Marchetti, M.; Cheng, G.S.; Bergeron, A.; Wolff, D.; Sander, C.; Sharma, A.; Badawy, S.M.; Peric, Z.; et al. ERS/EBMT clinical practice guidelines on treatment of pulmonary chronic graft-versus-host disease in adults. Eur. Respir. J. 2024, 63, 2301727. [Google Scholar] [CrossRef]
- Vos, R.; Vanaudenaerde, B.M.; Verleden, S.E.; Ruttens, D.; Vaneylen, A.; Van Raemdonck, D.E.; Dupont, L.J.; Verleden, G.M. Anti-inflammatory and immunomodulatory properties of azithromycin involved in treatment and prevention of chronic lung allograft rejection. Transplantation 2012, 94, 101–109. [Google Scholar] [CrossRef]
- Uzun, S.; Djamin, R.S.; Kluytmans, J.A.; Mulder, P.G.; van’t Veer, N.E.; Ermens, A.A.M.; Pelle, A.J.; Hoogsteden, H.C.; Aerts, J.G.J.V.; van der Eerden, M.M. Azithromycin maintenance treatment in patients with frequent exacerbations of chronic obstructive pulmonary disease (COLUMBUS): A randomised, double-blind, placebo-controlled trial. Lancet Respir. Med. 2014, 2, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.; Jayaram, L.; Karalus, N.; Eaton, T.; Tong, C.; Hockey, H.; Milne, D.; Fergusson, W.; Tuffery, C.; Sexton, P.; et al. Azithromycin for prevention of exacerbations in non-cystic fibrosis bronchiectasis (EMBRACE): A randomised, double-blind, placebo-controlled trial. Lancet 2012, 380, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Del Fante, C.; Perotti, C. Extracorporeal photopheresis for bronchiolitis obliterans syndrome after allogeneic stem cell transplant: An. emerging therapeutic approach? Transfus. Apher. Sci. 2017, 56, 17–19. [Google Scholar] [CrossRef] [PubMed]
- Reschke, R.; Zimmerlich, S.; Döhring, C.; Behre, G.; Ziemer, M. Effective Extracorporeal Photopheresis of Patients with Transplantation Induced Acute Intestinal GvHD and Bronchiolitis Obliterans Syndrome. Biomedicines 2022, 10, 1887. [Google Scholar] [CrossRef]
- The EPI Study Group; Hage, C.A.; Klesney-Tait, J.; Wille, K.; Arcasoy, S.; Yung, G.; Hertz, M.; Chan, K.M.; Morrell, M.; Goldberg, H.; et al. Extracorporeal photopheresis to attenuate decline in lung function due to refractory obstructive allograft dysfunction. Transfus. Med. 2021, 31, 292–302. [Google Scholar]
- Flowers, M.E.; Apperley, J.F.; van Besien, K.; Elmaagacli, A.; Grigg, A.; Reddy, V.; Bacigalupo, A.; Kolb, H.-J.; Bouzas, L.; Michallet, M.; et al. A multicenter prospective phase 2 randomized study of extracorporeal photopheresis for treatment of chronic graft-versus-host disease. Blood 2008, 112, 2667–2674. [Google Scholar] [CrossRef] [PubMed]
- Redente, E.F.; Aguilar, M.A.; Black, B.P.; Edelman, B.L.; Bahadur, A.N.; Humphries, S.M.; Lynch, D.A.; Wollin, L.; Riches, D.W.H. Nintedanib reduces pulmonary fibrosis in a model of rheumatoid arthritis-associated interstitial lung disease. Am. J. Physiol. Lung Cell. Mol. Physiol. 2018, 314, L998–L1009. [Google Scholar] [CrossRef]
- Wollin, L.; Distler, J.H.W.; Redente, E.F.; Riches, D.W.H.; Stowasser, S.; Schlenker-Herceg, R.; Maher, T.M.; Kolb, M. Potential of nintedanib in treatment of progressive fibrosing interstitial lung diseases. Eur. Respir. J. 2019, 54, 1900161. [Google Scholar] [CrossRef]
- Deterding, R.; Young, L.R.; DeBoer, E.M.; Warburton, D.; Cunningham, S.; Schwerk, N.; Flaherty, K.R.; Brown, K.K.; Dumistracel, M.; Erhardt, E.; et al. Nintedanib in children and adolescents with fibrosing interstitial lung diseases. Eur. Respir. J. 2023, 61, 2201512. [Google Scholar] [CrossRef]
- Dalle, J.H.; Wall, D.; Theoret, Y.; Duval, M.; Shaw, L.; Larocque, D.; Taylor, C.; Gardiner, J.; Vachon, M.F.; Champagne, M.A. Intravenous busulfan for allogeneic hematopoietic stem cell transplantation in infants: Clinical and pharmacokinetic results. Bone Marrow Transplant. 2003, 32, 647–651. [Google Scholar] [CrossRef]
- Choong, E.; Uppugunduri, C.R.S.; Marino, D.; Kuntzinger, M.; Doffey-Lazeyras, F.; Lo Piccolo, R.; Chalandon, Y.; Peters, C.; Daali, Y.; Ansari, M. Therapeutic drug monitoring of busulfan for the management of pediatric patients: Cross-validation of methods and long-term performance. Ther. Drug Monit. 2018, 40, 84–92. [Google Scholar]
- Ansari, M.; Théoret, Y.; Rezgui, M.A.; Peters, C.; Mezziani, S.; Desjean, C.; Vachon, M.-F.; Champagne, M.A.; Duval, M.; Krajinovic, M.; et al. Association between busulfan exposure and outcome in children receiving intravenous busulfan before hematopoietic stem cell transplantation. Ther. Drug Monit. 2014, 36, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Bostrom, B.; Enockson, K.; Johnson, A.; Bruns, A.; Blazar, B. Plasma pharmacokinetics of high-dose oral busulfan in children and adults undergoing bone marrow transplantation. Pediatr. Transplant. 2003, 7 (Suppl. 3), 12–18. [Google Scholar] [CrossRef] [PubMed]
- Andersson, B.S.; Thall, P.F.; Valdez, B.C.; Milton, D.R.; Al-Atrash, G.; Chen, J.; Gulbis, A.; Chu, D.; Martinez, C.; Parmar, S.; et al. Fludarabine with pharmacokinetically guided IV busulfan is superior to fixed-dose delivery in pretransplant conditioning of AML/MDS patients. Bone Marrow Transplant. 2017, 52, 580–587. [Google Scholar] [CrossRef] [PubMed]
- Bartelink, I.H.; van Reij, E.M.; Gerhardt, C.E.; van Maarseveen, E.M.; de Wildt, A.; Versluys, B.; Lindemans, C.; Bierings, M.; Boelens, J.J. Fludarabine and exposure-targeted busulfan compares favorably with busulfan/cyclophosphamide-based regimens in pediatric hematopoietic cell transplantation: Maintaining efficacy with less toxicity. Biol. Blood Marrow Transplant. 2014, 20, 345–353. [Google Scholar] [CrossRef]
- Bartelink, I.H.; Lalmohamed, A.; van Reij, E.M.; Dvorak, C.C.; Savic, R.M.; Zwaveling, J.; Bredius, R.G.M.; Egberts, A.C.G.; Bierings, M.; Kletzel, M.; et al. Association of busulfan exposure with survival and toxicity after haemopoietic cell transplantation in children and young adults: A multicentre, retrospective cohort analysis. Lancet Haematol. 2016, 3, e526–e536. [Google Scholar] [CrossRef]
- Vassal, G.; Michel, G.; Espérou, H.; Gentet, J.C.; Valteau-Couanet, D.; Doz, F.; Mechinaud, F.; Galambrun, C.; Neven, B.; Zouabi, H.; et al. Prospective validation of a novel IV busulfan fixed dosing for paediatric patients to improve therapeutic AUC targeting without drug monitoring. Cancer Chemother. Pharmacol. 2008, 61, 113–123. [Google Scholar] [CrossRef]
- Hassan, Z.; Hellström-Lindberg, E.; Alsadi, S.; Edgren, M.; Hägglund, H.; Hassan, M. The effect of modulation of glutathione cellular content on busulphan-induced cytotoxicity on hematopoietic cells in vitro and in vivo. Bone Marrow Transplant. 2002, 30, 141–147. [Google Scholar] [CrossRef]
- DeLeve, L.D.; Wang, X. Role of oxidative stress and glutathione in busulfan toxicity in cultured murine hepatocytes. Pharmacology 2000, 60, 143–154. [Google Scholar] [CrossRef]
- Kim, M.G.; Kwak, A.; Choi, B.; Ji, E.; Oh, J.M.; Kim, K. Effect of glutathione S-transferase genetic polymorphisms on busulfan pharmacokinetics and veno-occlusive disease in hematopoietic stem cell transplantation: A meta-analysis. Basic Clin. Pharmacol. Toxicol. 2019, 124, 691–703. [Google Scholar] [CrossRef]
- Choi, B.; Kim, M.G.; Han, N.; Kim, T.; Ji, E.; Park, S.; Kim, I.-W.; Oh, J.M. Population pharmacokinetics and pharmacodynamics of busulfan with GSTA1 polymorphisms in patients undergoing allogeneic hematopoietic stem cell transplantation. Pharmacogenomics 2015, 16, 1585–1594. [Google Scholar] [CrossRef] [PubMed]
- Ansari, M.; Curtis, P.H.; Uppugunduri, C.R.S.; Rezgui, M.A.; Nava, T.; Mlakar, V.; Lesne, L.; Théoret, Y.; Chalandon, Y.; Dupuis, L.L.; et al. GSTA1 diplotypes affect busulfan clearance and toxicity in children undergoing allogeneic hematopoietic stem cell transplantation: A multicenter study. Oncotarget 2017, 8, 90852–90867. [Google Scholar] [CrossRef] [PubMed]
- Bredschneider, M.; Klein, K.; Mürdter, T.E.; Marx, C.; Eichelbaum, M.; Nüssler, A.K.; Neuhaus, P.; Zanger, U.M.; Schwab, M. Genetic polymorphisms of glutathione S-transferase A1, the major glutathione S-transferase in human liver: Consequences for enzyme expression and busulfan conjugation. Clin. Pharmacol. Ther. 2002, 71, 479–487. [Google Scholar] [CrossRef]
- Mlakar, V.; Curtis, P.H.; Armengol, M.; Ythier, V.; Dupanloup, I.; Hassine, K.B.; Lesne, L.; Murr, R.; Mlakar, S.J.; Nava, T.; et al. The analysis of GSTA1 promoter genetic and functional diversity of human populations. Sci. Rep. 2021, 11, 5038. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).