
Single-Center Experience with the Balloon-Expandable Myval Transcatheter Aortic Valve System in Patients with Bicuspid Anatomy: Procedural and 30-Day Follow-Up

 , and
, and
Abstract
:
1. Introduction
2. Methods
2.1. Study Design
2.2. Patient Population
- Age, sex, body mass index;
- Hypertension, diabetes mellitus, dyslipidemia, ischemic heart disease, prior myocardial infarction, prior percutaneous coronary intervention, prior coronary artery bypass grafting, peripheral artery disease, cerebrovascular disease, COPD, permanent pacemaker implantation (PPI), atrial fibrillation;
- Serum creatinin level, serum hemoglobin level, estimated glomerular filtration ratio, mean aortic valve gradient, global left ventricular ejection fraction;
- New York Heart Association (NYHA) functional class, Society of Thoracic Surgery (STS) score, and Euroscore II.
2.3. Device Description and Procedure
2.4. Sizing Method
2.5. Study Endpoints and Follow-Up
3. Statistical Methods
4. Results
4.1. Baseline Characteristics
4.2. Procedural Outcomes
4.3. Distribution of THV Sizes According to Valve Types
4.4. CT Measurements
4.5. VARC-2 Outcomes at 30-Day Follow-Up
4.6. Echocardiographic Outcomes
5. Discussion
- The TAVI procedure with the Myval THV system is safe with no significant differences in VARC-2 outcomes in the unmatched and propensity score-matched comparisons.
- The TAVI procedure with the Myval THV system is effective with no significant differences in hemodynamic performance between BAV and TAV patients based on invasive and non-invasive measurements. Moreover, ARI was significantly higher after the BAV TAVI procedure.
- The sizing method employed, in conjunction with the broad range of standard and intermediate/extra sizes, facilitated the suitability of all patients for the TAVI procedure irrespective of their anatomical dimensions. Also, there was a significantly lower rate of oversizing in BAV patients compared to TAV.
- Beyond the absence of major mechanical complications, the rate of PPI was high in both groups. No significant differences in risk factors were detected between BAV and TAV patients with post-TAVI PPI except for a tendency for higher aortic valve calcium scores in BAV patients in the unmatched comparison. Therefore, this high PPI rate seems to be more related to patient characteristics than the device used. The significantly higher proportion of LVOT calcium in the PPI group of the whole patient cohort may underscore this theory.
6. Study Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hoffman, J.I.; Kaplan, S. The incidence of congenital heart disease. J. Am. Coll. Cardiol. 2002, 39, 1890–1900. [Google Scholar] [CrossRef] [PubMed]
- Sievers, H.H.; Schmidtke, C. A classification system for the bicuspid aortic valve from 304 surgical specimens. J. Thorac. Cardiovasc. Surg. 2007, 133, 1226–1233. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Xiong, T.Y.; Li, Y.M.; Yao, Y.J.; He, J.J.; Yang, H.R.; Zhu, Z.K.; Chen, F.; Ou, Y.; Wang, X.; et al. Patients with Bicuspid Aortic Stenosis Undergoing Transcatheter Aortic Valve Replacement: A Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 2022, 9, 794850. [Google Scholar] [CrossRef]
- Kawamori, H.; Yoon, S.H.; Chakravarty, T.; Maeno, Y.; Kashif, M.; Israr, S.; Abramowitz, Y.; Mangat, G.; Miyasaka, M.; Rami, T.; et al. Computed tomography characteristics of the aortic valve and the geometry of SAPIEN 3 transcatheter heart valve in patients with bicuspid aortic valve disease. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 1408–1418. [Google Scholar] [CrossRef]
- Michelena, H.I.; Prakash, S.K.; Della Corte, A.; Bissell, M.M.; Anavekar, N.; Mathieu, P.; Bossé, Y.; Limongelli, G.; Bossone, E.; Benson, D.W.; et al. Bicuspid aortic valve: Identifying knowledge gaps and rising to the challenge from the International Bicuspid Aortic Valve Consortium (BAVCon). Circulation 2014, 129, 2691–2704. [Google Scholar] [CrossRef]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e35–e71. [Google Scholar] [CrossRef] [PubMed]
- Mylotte, D.; Lefevre, T.; Søndergaard, L.; Watanabe, Y.; Modine, T.; Dvir, D.; Bosmans, J.; Tchetche, D.; Kornowski, R.; Sinning, J.M.; et al. Transcatheter aortic valve replacement in bicuspid aortic valve disease. J. Am. Coll. Cardiol. 2014, 64, 2330–2339. [Google Scholar] [CrossRef]
- Mangieri, A.; Tchetchè, D.; Kim, W.K.; Pagnesi, M.; Sinning, J.M.; Landes, U.; Kornowski, R.; De Backer, O.; Nickenig, G.; Ielasi, A.; et al. Balloon Versus Self-Expandable Valve for the Treatment of Bicuspid Aortic Valve Stenosis: Insights From the BEAT International Collaborative Registrys. Circ. Cardiovasc. Interv. 2020, 13, e008714. [Google Scholar] [CrossRef]
- Vahidkhah, K.; Barakat, M.; Abbasi, M.; Javani, S.; Azadani, P.N.; Tandar, A.; Dvir, D.; Azadani, A.N. Valve thrombosis following transcatheter aortic valve replacement: Significance of blood stasis on the leaflets. Eur. J. Cardiothorac. Surg. 2017, 51, 927–935. [Google Scholar] [CrossRef]
- Vahidkhah, K.; Javani, S.; Abbasi, M.; Azadani, P.N.; Tandar, A.; Dvir, D.; Azadani, A.N. Blood Stasis on Transcatheter Valve Leaflets and Implications for Valve-in-Valve Leaflet Thrombosis. Ann. Thorac. Surg. 2017, 104, 751–759. [Google Scholar] [CrossRef]
- Makkar, R.R.; Fontana, G.; Jilaihawi, H.; Chakravarty, T.; Kofoed, K.F.; De Backer, O.; Asch, F.M.; Ruiz, C.E.; Olsen, N.T.; Trento, A.; et al. Possible Subclinical Leaflet Thrombosis in Bioprosthetic Aortic Valves. N. Engl. J. Med. 2015, 373, 2015–2024. [Google Scholar] [CrossRef] [PubMed]
- Pibarot, P.; Magne, J.; Leipsic, J.; Côté, N.; Blanke, P.; Thourani, V.H.; Hahn, R. Imaging for Predicting and Assessing Prosthesis-Patient Mismatch after Aortic Valve Replacement. JACC Cardiovasc. Imaging 2019, 12, 149–162. [Google Scholar] [CrossRef] [PubMed]
- Qiu, D.; Barakat, M.; Hopkins, B.; Ravaghi, S.; Azadani, A.N. Transcatheter aortic valve replacement in bicuspid valves: The synergistic effects of eccentric and incomplete stent deployment. J. Mech. Behav. Biomed. Mater. 2021, 121, 104621. [Google Scholar] [CrossRef]
- D’Agostino, R.B., Jr. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat. Med. 1998, 17, 2265–2281. [Google Scholar] [CrossRef]
- Sharma, S.K.; Rao, R.S.; Chandra, P.; Goel, P.K.; Bharadwaj, P.; Joseph, G.; Jose, J.; Mahajan, A.U.; Mehrotra, S.; Sengottovelu, G.; et al. First-in-human evaluation of a novel balloon-expandable transcatheter heart valve in patients with severe symptomatic native aortic stenosis: The MyVal-1 study. EuroIntervention 2020, 16, 421–429. [Google Scholar] [CrossRef]
- Achenbach, S.; Delgado, V.; Hausleiter, J.; Schoenhagen, P.; Min, J.K.; Leipsic, J.A. SCCT expert consensus document on computed tomography imaging before transcatheter aortic valve implantation (TAVI)/transcatheter aortic valve replacement (TAVR). J. Cardiovasc. Comput. Tomogr. 2012, 6, 366–380. [Google Scholar] [CrossRef]
- Tchetche, D.; de Biase, C.; van Gils, L.; Parma, R.; Ochala, A.; Lefevre, T.; Hovasse, T.; De Backer, O.; Sondergaard, L.; Bleiziffer, S.; et al. Bicuspid Aortic Valve Anatomy and Relationship with Devices: The BAVARD Multicenter Registry. Circ. Cardiovasc. Interv. 2019, 12, e007107. [Google Scholar] [CrossRef] [PubMed]
- Kasel, A.M.; Cassese, S.; Leber, A.W.; von Scheidt, W.; Kastrati, A. Fluoroscopy-guided aortic root imaging for TAVR: “follow the right cusp” rule. JACC Cardiovasc. Imaging 2013, 6, 274–275. [Google Scholar] [CrossRef]
- Petronio, A.S.; Angelillis, M.; De Backer, O.; Giannini, C.; Costa, G.; Fiorina, C.; Castriota, F.; Bedogni, F.; Laborde, J.C.; Søndergaard, L. Bicuspid aortic valve sizing for transcatheter aortic valve implantation: Development and validation of an algorithm based on multi-slice computed tomography. J. Cardiovasc. Comput. Tomogr. 2020, 14, 452–461. [Google Scholar] [CrossRef]
- Iannopollo, G.; Romano, V.; Buzzatti, N.; Ancona, M.; Ferri, L.; Russo, F.; Bellini, B.; Granada, J.F.; Chieffo, A.; Montorfano, M. Supra-annular sizing of transcatheter aortic valve prostheses in raphe-type bicuspid aortic valve disease: The LIRA method. Int. J. Cardiol. 2020, 317, 144–151. [Google Scholar] [CrossRef]
- Kappetein, A.P.; Head, S.J.; Généreux, P.; Piazza, N.; van Mieghem, N.M.; Blackstone, E.H.; Brott, T.G.; Cohen, D.J.; Cutlip, D.E.; van Es, G.-A.; et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: The Valve Academic Research Consortium-2 consensus document. J. Thorac. Cardiovasc. Surg. 2013, 145, 6–23. [Google Scholar] [CrossRef] [PubMed]
- Sinning, J.-M.; Hammerstingl, C.; Vasa-Nicotera, M.; Adenauer, V.; Lema Cachiguango, S.J.; Scheer, A.-C.; Hausen, S.; Sedaghat, A.; Ghanem, A.; Müller, C.; et al. Aortic Regurgitation Index Defines Severity of Peri-Prosthetic Regurgitation and Predicts Outcome in Patients after Transcatheter Aortic Valve Implantation. J. Am. Coll. Cardiol. 2012, 59, 1134–1141. [Google Scholar] [CrossRef]
- Hopf, R.; Sündermann, S.H.; Born, S.; Ruiz, C.E.; Van Mieghem, N.M.; de Jaegere, P.P.; Maisano, F.; Falk, V.; Mazza, E. Postoperative analysis of the mechanical interaction between stent and host tissue in patients after transcatheter aortic valve implantation. J. Biomech. 2017, 53, 15–21. [Google Scholar] [CrossRef]
- Iannopollo, G.; Romano, V.; Buzzatti, N.; De Backer, O.; Søndergaard, L.; Merkely, B.; Prendergast, B.D.; Giannini, F.; Colombo, A.; Latib, A.; et al. A novel supra-annular plane to predict TAVI prosthesis anchoring in raphe-type bicuspid aortic valve disease: The LIRA plane. EuroIntervention 2020, 16, 259–261. [Google Scholar] [CrossRef]
- Magyari, B.; Kittka, B.; Goják, I.; Kasza, G.; Schönfeld, K.; Szapáry, L.B.; Simon, M.; Kiss, R.; Bertalan, A.; Várady, E.; et al. Single center experience with the balloon-expandable Myval transcatheter aortic valve system with the first 100 patients: 30-day and 1-year follow-up. Catheter. Cardiovasc. Interv. 2023, 102, 1317–1330. [Google Scholar] [CrossRef] [PubMed]
- Glikson, M.; Nielsen, J.C.; Kronborg, M.B.; Michowitz, Y.; Auricchio, A.; Barbash, I.M.; Barrabés, J.A.; Boriani, G.; Braunschweig, F.; Brignole, M.; et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: Developed by the Task Force on cardiac pacing and cardiac resynchronization therapy of the European Society of Cardiology (ESC) with the special contribution of the European Heart Rhythm Association (EHRA). Rev. Esp. Cardiol. Engl. Ed. 2022, 75, 430. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.H.; Kim, W.K.; Dhoble, A.; Milhorini Pio, S.; Babaliaros, V.; Jilaihawi, H.; Pilgrim, T.; De Backer, O.; Bleiziffer, S.; Vincent, F.; et al. Bicuspid Aortic Valve Morphology and Outcomes after Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2020, 76, 1018–1030. [Google Scholar] [CrossRef]
- Siontis, G.C.; Jüni, P.; Pilgrim, T.; Stortecky, S.; Büllesfeld, L.; Meier, B.; Wenaweser, P.; Windecker, S. Predictors of permanent pacemaker implantation in patients with severe aortic stenosis undergoing TAVR: A meta-analysis. J. Am. Coll. Cardiol. 2014, 64, 129–140. [Google Scholar] [CrossRef]
- van Rosendael, P.J.; Delgado, V.; Bax, J.J. Pacemaker implantation rate after transcatheter aortic valve implantation with early and new-generation devices: A systematic review. Eur. Heart J. 2018, 39, 2003–2013. [Google Scholar] [CrossRef]
- Delgado-Arana, J.R.; Gordillo-Monge, M.X.; Halim, J.; De Marco, F.; Trani, C.; Martin, P.; Infusino, F.; Ancona, M.; den Heijer, P.; Bedogni, F.; et al. Early clinical and haemodynamic matched comparison of balloon-expandable valves. Heart 2021, 108, 725–732. [Google Scholar] [CrossRef]
- Yoon, S.H.; Bleiziffer, S.; De Backer, O.; Delgado, V.; Arai, T.; Ziegelmueller, J.; Barbanti, M.; Sharma, R.; Perlman, G.Y.; Khalique, O.K.; et al. Outcomes in Transcatheter Aortic Valve Replacement for Bicuspid versus Tricuspid Aortic Valve Stenosis. J. Am. Coll. Cardiol. 2017, 69, 2579–2589. [Google Scholar] [CrossRef] [PubMed]
- Miyasaka, M.; Yoon, S.H.; Sharma, R.P.; Maeno, Y.; Jaideep, S.; Taguri, M.; Kato, S.; Kawamori, H.; Nomura, T.; Ochiai, T.; et al. Clinical Outcomes of Transcatheter Aortic Valve Implantation in Patients with Extremely Large Annulus and SAPIEN 3 Dimensions Based on Post-Procedural Computed Tomography. Circ. J. 2019, 83, 672–680. [Google Scholar] [CrossRef] [PubMed]
- Makkar, R.R.; Yoon, S.H.; Leon, M.B.; Chakravarty, T.; Rinaldi, M.; Shah, P.B.; Skipper, E.R.; Thourani, V.H.; Babaliaros, V.; Cheng, W.; et al. Association Between Transcatheter Aortic Valve Replacement for Bicuspid vs Tricuspid Aortic Stenosis and Mortality or Stroke. J. Am. Med. Assoc. 2019, 321, 2193–2202. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristic of Study Population (n = 269) | Tricuspid (n = 217) | Bicuspid (n = 52) | p Value | Tricuspid (n = 52) | Bicuspid (n = 52) | p Value | |
|---|---|---|---|---|---|---|---|
| Age (years) | 75 ± 7.3 | 76 ± 6.9 | 71 ± 7.1 | <0.001 | 72.3 ± 8.9 | 71 ± 7.1 | 0.430 |
| Men (n/%) | 165 (61.3) | 131 (60.4%) | 34 (65.4) | 0.505 | 37 (71.1) | 34 (65.4) | 0.527 |
| Body mass index (kg/m2) | 29 ± 5.3 | 29.3 ± 5.3 | 28.1 ± 5.4 | 0.165 | 28.1 ± 5.3 | 28.1 ± 5.4 | 0.997 |
| Body surface area (m2) | 1.94 ± 0.2 | 1.95 ± 0.24 | 1.92 ± 0.23 | 0.254 | 1.95 ± 0.26 | 1.92 ± 0.23 | 0.487 |
| Hypertension | 262 (97.4) | 211 (97.2) | 51 (98.1) | 0.732 | 51 (98.1) | 51 (98.1) | 1.0 |
| Diabetes mellitus | 116 (43.1) | 98 (45,2) | 18 (34,6) | 0.168 | 17 (32.7) | 18 (34.6) | 0.836 |
| Hyperlipidemia | 243 (90.3) | 197 (90.8) | 46 (88.5) | 0.611 | 46 (88.5) | 46 (88.5) | 1.0 |
| NYHA class III or IV | 223 (82.9) | 182 (83.9) | 41 (78.8) | 0.387 | 43 (82.7) | 41 (78.8) | 0.619 |
| Ischemic Heart Disease | 114 (42.4) | 98 (45.2) | 16 (30.7) | 0.059 | 17 (32.7) | 16 (30.8) | 0.833 |
| St.p. MI | 62 (23) | 53 (24.4) | 9 (17.3) | 0.274 | 9 (17.3) | 9 (17.3) | 1.0 |
| St.p. PCI | 91 (33.8) | 79 (36.4) | 12 (23.1) | 0.068 | 13 (25.0) | 12 (23.1) | 0.819 |
| St.p. CABG | 46 (17.1) | 42 (19.4) | 4 (7.7) | * 0.045 | 4 (7.7) | 4 (7.7) | 1.0 |
| Peripheral artery disease | 40 (14.9) | 31 (14.3) | 9 (17.3) | 0.582 | 8 (15.4) | 9 (17.3) | 0.791 |
| Cerebrovascular disease | 38 (14.1) | 32 (14.7) | 6 (11.5) | 0.551 | 4 (7.7) | 6 (11.5) | 0.506 |
| COPD | 40 (14.9) | 27 (12.4) | 13 (25.0) | * 0.023 | 10 (19.2) | 13 (25.0) | 0.478 |
| Previous BAV | 10 (3.7) | 9 (4.1) | 1 (1.9) | 0.446 | 3 (5.8) | 1 (1.9) | 0.308 |
| Permanent PM | 25 (9.3) | 23 (10.6) | 2 (3.8) | 0.132 | 2 (3.8) | 2 (3.8) | 1.0 |
| Atrial fibrillation | 53 (19.7) | 46 (21,2) | 7 (13.5) | 0.208 | 9 (17.3) | 7 (13.5) | 0.587 |
| Logistic EuroSCORE (%) | 14.9 ± 14.4 | 15.5 ± 15.2 | 12.2 ± 10.4 | 0.131 | 11.3 ± 10.8 | 12.2 ± 10.4 | 0.663 |
| Logistic EuroSCORE II (%) | 4.8 ± 5.1 | 5.2 ± 5.4 | 3.3 ± 3.2 | * 0.002 | 3.2 ± 2.5 | 3.3 ± 3.2 | 0.770 |
| STS score (%) | 6.2 ± 4.3 | 6.4 ± 4.4 | 5.2 ± 3.3 | 0.069 | 4.7 ± 3.9 | 5.2 ± 3.3 | 0.505 |
| Calcium score of the aortic valve | 3374 ± 1174 | 3238 ± 1682 | 3911 ± 2554 | 0.081 | 3574 ± 1769 | 3911 ± 2554 | 0.444 |
| Serum creatinine (umol/L) | 101.8 ± 44.8 | 103.5 ± 48.1 | 94.6 ± 25.8 | 0.199 | 96.4 ± 31.3 | 94.6 ± 25.8 | 0.754 |
| Estimated GFR (mL/min) | 67.6 ± 26.4 | 66.6 ± 27.2 | 71.9 ± 22.9 | 0.188 | 72.3 ± 29.2 | 71.9 ± 22.9 | 0.952 |
| St.p. MVR | 4 (1.5) | 4 (1.8) | 0 (0.0) | 0.324 | 0 (0.0) | 0 (0.0) | NA |
| St.p. AVR | 1 (0.4) | 1 (0.5) | 0 (0.0) | 0.624 | 0 (0.0) | 0 (0.0) | NA |
| Dialysis | 3 (1.1) | 2 (0.9) | 1 (1.9) | 0.537 | 0 (0.0) | 1 | 0.315 |
| Procedure status | |||||||
| elective | 253 (94) | 204 (94) | 49 (94.2) | 0.952 | 48 (92.3) | 49 (94.2) | 0.696 |
| urgent | 15 (5.6) | 12 (5.5) | 3 (5.8) | 0.946 | 3 (5.8) | 3 (5.8) | 1.0 |
| acut | 1 (0.4) | 1 (0.5) | 0 (0.0) | 0.624 | 1 (1.9) | 0 (0.0) | 0.315 |
| Unmatched (n = 269) | Matched (n = 52) | |||||
|---|---|---|---|---|---|---|
| Baseline Echocardiographic Parameters of the Study Population (n = 269) | Tricuspid (n = 217) | Bicuspid (n = 52) | p Value | Tricuspid (n = 52) | Bicuspid (n = 52) | p Value |
| Mean LVEF | 55.5 ± 12.8 | 54.2 ± 13.6 | 0.543 | 54.8 ± 14.1 | 54.3 ± 13.6 | 0.827 |
| Mean AoVmax (m/s) | 4.4 ± 0.7 | 4.4 ± 0.7 | 0.966 | 4.4 ± 0.8 | 4.4 ± 0.7 | 0.919 |
| Aortic peak gradient (Hgmm) | 80.2 ± 25.7 | 79.9 ± 24.1 | 0.928 | 79.7 ± 29.1 | 79.9 ± 24.1 | 0.975 |
| Aortic mean gradient (Hgmm) | 47.8 ± 15.5 | 47.6 ± 15.9 | 0.949 | 47.6 ± 17.5 | 47.6 ± 15.8 | 0.988 |
| Mitral insufficiency III or IV | 45 | 7 | 0.233 | 7 | 7 | 1.0 |
| Tricuspid insufficiency III or IV | 38 | 9 | 0.972 | 8 | 9 | 0.791 |
| Unmatched (n = 269) | Matched (n = 52) | ||||||
|---|---|---|---|---|---|---|---|
| Variable | Overall (n = 269) | Tricuspid (n = 217) | Bicuspid (n = 52) | p Value | Tricuspid (n = 52) | Bicuspid (n = 52) | p Value |
| Type of anesthesia | |||||||
| general | 15 | 11 | 4 | 0.459 | 0 | 4 | * 0.041 |
| local | 255 | 207 | 48 | 0.369 | 52 | 48 | * 0.041 |
| Access site | |||||||
| femoral (percutaneous) | 265 | 216 | 49 | * 0.005 | 52 | 49 | 0.079 |
| femoral (surgical) | 2 | 0 | 2 | * 0.004 | 0 | 2 | 0.153 |
| subclavia | 2 | 1 | 1 | 0.270 | 0 | 1 | 0.315 |
| axillaris | 0 | 0 | 0 | NA | 0 | 0 | NA |
| direct aortic | 0 | 0 | 0 | NA | 0 | 0 | NA |
| Contrast agent | 225.3 ± 99.5 | 224.5 ± 100.2 | 230 ± 97.4 | 0.719 | 218.7 ± 92.1 | 230 ± 97.4 | 0.544 |
| Operation duration (min) | 85.4 ± 29.5 | 82.6 ± 28.2 | 95.5 ± 34.2 | * 0.005 | 78.5 ± 24.3 | 95.5 ± 34.2 | * 0.004 |
| Predilatation | 269 | 217 | 52 | 1.000 | 52 | 52 | 1.000 |
| Postdilatation | 34 | 28 | 6 | 0.790 | 6 | 6 | 1.000 |
| Preimpl. mean AV gradient | 53.6 ± 18.2 | 53.9 ± 18.5 | 52.6 ± 17.0 | 0.658 | 55.4 ± 19.9 | 52.6 ± 17 | 0.452 |
| Postimpl. mean AV gradient | 6.4 ± 6.2 | 6.4 ± 6.3 | 6.3 ± 5.8 | 0.942 | 6.1 ± 5.5 | 6.3 ± 5.8 | 0.868 |
| ARI | 29 ± 18.7 | 28.7 ± 20.5 | 30.4 ± 9.2 | 0.576 | 25.8 ± 8.5 | 30.4 ± 9.2 | * 0.014 |
| Unmatched (n = 269) | Matched (n = 104) | |||||
|---|---|---|---|---|---|---|
| Non PM (n = 193) | PM (n = 76) | p-Value | Non PM (n = 75) | PM (n = 29) | p-Value | |
| Age | 75.1 ± 6.9 | 74.8 ± 8.1 | 0.712 | 71.8 ± 7.3 | 71.1 ± 9.8 | 0.672 |
| Euroscore | 15.7 ± 15.5 | 12.7 ± 11 | 0.077 | 12.1 ± 11 | 10.8 ± 9.3 | 0.567 |
| Euroscore II | 5.1 ± 5.4 | 4.3 ± 4.1 | 0.286 | 3.3 ± 2.9 | 3.2 ± 2.8 | 0.902 |
| STS score | 6.1 ± 3.8 | 6.2 ± 5.2 | 0.993 | 4.9 ± 3 | 5.1 ± 5 | 0.817 |
| Ca score | 3393 ± 1943 | 3304 ± 1778 | 0.737 | 3687 ± 2177 | 3880 ± 2253 | 0.694 |
| Ca in LVOT | 59 (30.5%) | 36 (47.4%) | 0.009 | 26 (34.7%) | 13 (44.8%) | 0.337 |
| Oversizing | 6.3 ± 4.7 | 6.8 ± 4.1 | 0.490 | 5.5 ± 5 | 5.8 ± 4.4 | 0.723 |
| THV implantation depth | ||||||
| Left coronary side (mm) | 5.4 ± 2.1 | 5.7 ± 1.9 | 0.254 | 5.4 ± 2.1 | 5.5 ± 2.1 | 0.886 |
| Non coronary side (mm) | 6.2 ± 1.9 | 6.3 ± 1.8 | 0.831 | 6.2 ± 2.1 | 6.1 ± 2.2 | 0.939 |
| Right coronary side (mm) | 5.9 ± 1.9 | 6.1 ± 1.8 | 0.506 | 6 ± 1.9 | 6 ± 2.0 | 0.884 |
| Average depth (mm) | 5.8 ± 1.9 | 6.0 ± 1.8 | 0.477 | 5.9 ± 1.9 | 5.9 ± 2 | 0.943 |
| THV size | ||||||
| 21.5 | 8 | 2 | 0.555 | 4 | 2 | 0.759 |
| 23 | 26 | 11 | 0.830 | 7 | 2 | 0.692 |
| 24.5 | 48 | 17 | 0.666 | 16 | 5 | 0.641 |
| 26 | 38 | 15 | 0.993 | 13 | 3 | 0.376 |
| 27.5 | 42 | 17 | 0.914 | 18 | 9 | 0.463 |
| 29 | 17 | 8 | 0.662 | 8 | 2 | 0.559 |
| 30.5 | 8 | 5 | 0.402 | 7 | 4 | 0.507 |
| 32 | 5 | 1 | 0.524 | 2 | 2 | 0.314 |
| Standard size | 81 (41.9%) | 34 (44.7%) | 0.680 | 28 (37.3%) | 7 (24.1%) | 0.202 |
| Intermediate/extra size | 111 (58.1%) | 42 (55.3%) | 0.680 | 47 (62.7%) | 22 (75.9%) | 0.202 |
| Unmatched (n = 76) | Matched (n = 29) | |||||
|---|---|---|---|---|---|---|
| TAV-PM (n = 59) | BAV-PM (n = 17) | p-Value | TAV-PM (n = 12) | BAV-PM (n = 17) | p-Value | |
| Age | 75.8 ± 7.8 | 71.6 ± 8.2 | 0.031 | 71.2 ± 12.1 | 71 ± 8.2 | 0.977 |
| Euroscore | 12.9 ± 11.9 | 11.9 ± 7.4 | 0.723 | 9.2 ± 11.7 | 11.9 ± 7.4 | 0.451 |
| Euroscore II | 4.7 ± 4.5 | 3 ± 2.2 | 0.042 | 3.4 ± 3.6 | 3.0 ± 2.2 | 0.738 |
| STS score | 6.7 ± 5.8 | 4.2 ± 1.1 | 0.002 | 6.3 ± 7.7 | 4.2 ± 1.1 | 0.356 |
| Ca score | 3112 ± 1568 | 3975 ± 2310 | 0.087 | 3753 ± 2271 | 3975 ± 2310 | 0.802 |
| Ca in LVOT | 29 (49.1%) | 7 (41.2%) | 0.562 | 6 (50%) | 7 (41.2%) | 0.638 |
| Oversizing | 7.3 ± 3.9 | 4.9 ± 4 | 0.038 | 7.1 ± 4.7 | 4.9 ± 4.0 | 0.184 |
| THV implantation depth | ||||||
| Left coronary side (mm) | 5.6 ± 1.9 | 5.9 ± 1.9 | 0.516 | 4.9 ± 2.4 | 5.9 v 1.9 | 0.179 |
| Non coronary side (mm) | 6.2 ± 1.9 | 6.5 ± 1.7 | 0.515 | 5.6 ± 2.7 | 6.5 ± 1.7 | 0.282 |
| Right coronary side (mm) | 6.0 ± 1.9 | 6.4 ± 1.6 | 0.411 | 5.4 ± 2.6 | 6.4 ± 1.6 | 0.218 |
| Average depth (mm) | 5.9 ± 1.8 | 6.3 ± 1.6 | 0.460 | 5.3 ± 2.5 | 6.3 ± 1.6 | 0.205 |
| THV size | ||||||
| 21.5 | 1 | 1 | 0.342 | 1 | 1 | 0.798 |
| 23 | 10 | 1 | 0.253 | 1 | 1 | 0.798 |
| 24.5 | 14 | 3 | 0.596 | 2 | 3 | 0.945 |
| 26 | 13 | 2 | 0.349 | 1 | 2 | 0.765 |
| 27.5 | 12 | 5 | 0.429 | 4 | 5 | 0.822 |
| 29 | 8 | 0 | 0.108 | 2 | 0 | 0.081 |
| 30.5 | 1 | 4 | 0.001 | 1 | 4 | 0.286 |
| 32 | 0 | 1 | 0.061 | 0 | 1 | 0.393 |
| Standard size | 31 (52.5%) | 3 (17.6%) | 0.011 | 4 (33.3%) | 3 (17.6%) | 0.331 |
| Intermediate/extra size | 28 (47.5%) | 14 (82.4%) | 0.011 | 8 (66.7%) | 14 (82.4%) | 0.331 |
| Unmatched (n = 269) | Matched (n = 52) | |||||
|---|---|---|---|---|---|---|
| THV Size | Tricuspid (n = 217) | Bicuspid (n = 52) | p Value | Tricuspid (n = 52) | Bicuspid (n = 52) | p Value |
| 21.5 | 6 | 4 | 0.092 | 2 | 4 | 0.400 |
| 23 | 34 | 3 | 0.063 | 6 | 3 | 0.295 |
| 24.5 | 54 | 11 | 0.572 | 10 | 11 | 0.807 |
| 26 | 49 | 4 | 0.015 | 12 | 4 | 0.030 |
| 27.5 | 45 | 14 | 0.333 | 13 | 14 | 0.823 |
| 29 | 20 | 5 | 0.929 | 5 | 5 | 1.0 |
| 30.5 | 5 | 8 | <0.0001 | 4 | 8 | 0.220 |
| 32 | 3 | 3 | 0.054 | 0 | 3 | 0.079 |
| Oversizing (%) | 6.9 ± 4.4 | 4.8 ± 4.7 | 0.002 | 6.4 ± 4.9 | 4.8 ± 4.7 | 0.044 |
| Standard size | 103 (47.5%) | 12 (23.1%) | 0.001 | 23 (44.2%) | 12 (23.1%) | 0.022 |
| Intermediate/extra size | 113 (52.5%) | 40 (76.9%) | 0.001 | 29 (55.8%) | 40 (76.9%) | 0.022 |
| 0.337 * | <0.0001 ** | 0.239 * | <0.0001 ** | |||
| THV Size | Bicuspid (n = 52) | Bicuspid Re-Size (n = 52) | p Value |
|---|---|---|---|
| 20 | 0 | 1 | |
| 21.5 | 4 | NA | |
| 23 | 3 | 9 | |
| 24.5 | 11 | NA | |
| 26 | 4 | 16 | |
| 27.5 | 14 | NA | |
| 29 | 5 | 18 | |
| 30.5 | 8 | NA | |
| 32 | 3 | 8 | |
| Oversize (%) | 4.76 ± 4.7 | 8.3 ± 9.3 | 0.017 |
| Unmatched (n = 269) | Matched (n = 52) | |||||
|---|---|---|---|---|---|---|
| Variable | Tricuspid (n = 217) | Bicuspid (n = 52) | p Value | Tricuspid (n = 52) | Bicuspid (n = 52) | p Value |
| Aortic anulus perimeter | 79.5 ± 6.9 | 83.9 ± 9.8 | 0.003 | 81.1 ± 7.1 | 83.9 ± 9.7 | 0.097 |
| Aortic anulus perimeter derived Ø | 25.4 ± 2.2 | 26.7 ± 3.1 | 0.004 | 25.8 ± 2.3 | 26.7 ± 3.1 | 0.097 |
| Aortic anulus area | 494 ± 85 | 551.4 ± 125.4 | 0.003 | 511.5 ± 89.1 | 551.3 ± 125.4 | 0.065 |
| Aortic anulus area derived Ø | 24.9 ± 2.1 | 26.3 ± 3.0 | 0.004 | 25.4 ± 2.2 | 26.3 ± 3.0 | 0.090 |
| Aortic anulus Ø, min | 22.5 ± 2.0 | 23.6 ± 2.9 | 0.013 | 22.8 ± 2.2 | 23.6 ± 2.9 | 0.155 |
| Aortic anulus Ø, max | 28.0 ± 2.5 | 29.3 ± 3.6 | 0.025 | 28.6 ± 2.6 | 29.3 ± 3.6 | 0.270 |
| Aortic anulus Ø, average | 25.3 ± 2.1 | 26.4 ± 3.1 | 0.013 | 25.7 ± 2.3 | 26.4 ± 3.1 | 0.186 |
| Aortic anulus, Eccentricity | 0.20 ± 0.05 | 0.19 ± 0.07 | 0.574 | 0.2 ± 0.05 | 0.19 ± 0.07 | 0.490 |
| RCA height | 16.8 ± 3.1 | 17.5 ± 3.1 | 0.194 | 16.8 ± 2.8 | 17.5 ± 3.1 | 0.291 |
| LM height | 13.5 ± 3 | 14.9 ± 3.1 | 0.004 | 14.5 ± 3.1 | 14.9 ± 3.1 | 0.534 |
| SOV diameter, left | 33.4 ± 3.4 | 33.3 ± 7.6 | 0.980 | 33.9 ± 3.9 | 33.3 ± 5.3 | 0.588 |
| SOV diameter, right | 31.6 ± 3.1 | 33.4 ± 5.3 | 0.040 | 31.8 ± 3.3 | 33.4 ± 5.3 | 0.097 |
| SOV diameter, non | 33.1 ± 3.3 | 36.9 ± 4.9 | <0.0001 | 33.3 ± 3.2 | 36.9 ± 5.0 | <0.0001 |
| SOV height | 10.2 ± 1.9 | 10.7 ± 2.7 | 0.116 | 10.2 ± 2 | 10.7 ± 2.7 | 0.215 |
| Ascending aorta diameter, min | 34.0 ± 3.8 | 39.9 ± 5.5 | <0.0001 | 33.9 ± 3.9 | 39.5 ± 5.5 | <0.0001 |
| Ascending aorta diameter, max | 35.7 ± 3.8 | 41.4 ± 5.8 | <0.0001 | 35.6 ± 3.7 | 41.4 ± 5.8 | <0.0001 |
| Ascending aorta diameter, average | 34.8 ± 3.8 | 40.5 ± 5.6 | <0.0001 | 34.7 ± 3.8 | 40.5 ± 5.6 | <0.0001 |
| Ascending aorta perimeter | 109 ± 12.1 | 125.1 ± 18.3 | <0.0001 | 109 ± 12.5 | 125.1 ± 18.3 | <0.0001 |
| Ascending aorta perimeter derived Ø | 34.7 ± 3.9 | 39.8 ± 5.8 | <0.0001 | 34.7 ± 3.9 | 39.8 ± 5.8 | <0.0001 |
| Ascending aorta area | 954.3 ± 215.8 | 1267.3 ± 362.2 | <0.0001 | 954.6 ± 218.1 | 1267.3 ± 362.2 | <0.0001 |
| Ascending aorta area derived Ø | 34.6 ± 3.9 | 39.7 ± 5.8 | <0.0001 | 34.6 ± 3.9 | 39.8 ± 5.8 | <0.0001 |
| STJ Ø, min | 27.9 ± 2.9 | 32.2 ± 4.4 | <0.0001 | 28.3 ± 3.0 | 32.2 ± 4.4 | <0.0001 |
| STJ Ø, max | 29.8 ± 3.2 | 35.1 ± 5.1 | <0.0001 | 30.3 ± 3.2 | 35.1 ± 5.1 | <0.0001 |
| STJ Ø, average | 28.9 ± 3.0 | 33.7 ± 4.7 | <0.0001 | 29.3 ± 3.1 | 33.7 ± 4.7 | <0.0001 |
| STJ perimeter | 90.3 ± 11.3 | 104.9 ± 14.9 | <0.0001 | 92 ± 9.7 | 104.9 ± 15.0 | <0.0001 |
| STJ perimeter derived Ø | 28.9 ± 3.1 | 33.4 ± 4.7 | <0.0001 | 29.3 ± 3.1 | 33.4 ± 4.8 | <0.0001 |
| STJ area | 659.4 ± 140.2 | 887.1 ± 255.1 | <0.0001 | 677.8 ± 143.8 | 887.1 ± 255.2 | <0.0001 |
| STJ area derived Ø | 28.8 ± 3.0 | 33.3 ± 4.7 | <0.0001 | 29.2 ± 3.1 | 33.3 ± 4.7 | <0.0001 |
| LVOT Ø, min | 22.2 ± 2.6 | 23.5 ± 3.1 | 0.009 | 22.5 ± 2.5 | 23.5 ± 3.1 | 0.092 |
| LVOT Ø, max | 28.9 ± 2.8 | 29.9 ± 3.9 | 0.067 | 29.5 ± 2.8 | 29.9 ± 3.9 | 0.504 |
| LVOT Ø, average | 25.4 ± 2.9 | 26.7 ± 3.4 | 0.014 | 26.0 ± 2.5 | 26.7 ± 3.4 | 0.234 |
| LVOT eccentricity | 0.23 ± 0.06 | 0.22 ± 0.06 | 0.085 | 0.24 ± 0.05 | 0.22 ± 0.06 | 0.043 |
| LVOT perimeter | 80.7 ± 7.7 | 84.9 ± 11.4 | 0.0014 | 82.6 ± 8.1 | 84.9 ± 11.4 | 0.225 |
| LVOT perimeter derived Ø | 26.8 ± 16.8 | 27.0 ± 3.6 | 0.928 | 26.3 ± 2.6 | 27.0 ± 3.6 | 0.216 |
| LVOT area | 501.1 ± 97.9 | 560.9 ± 145.3 | 0.006 | 523.2 ± 102.1 | 560.9 ± 145.3 | 0.129 |
| LVOT area derived Ø | 25.1 ± 2.5 | 26.5 ± 3.5 | 0.011 | 25.7 ± 2.5 | 26.5 ± 3.5 | 0.187 |
| Impl. Angulation | 47.4 ± 8.1 | 53 ± 10.9 | 0.001 | 47.2 ± 7.8 | 53 ± 10.9 | 0.003 |
| Horizontal aorta (n/%) | 85/39.2 | 28/53.8 | 0.054 | 20/38.5 | 28/53.8 | 0.116 |
| Aortopathy | 16 (7.4%) | 32 (61.5%) | <0.0001 | 3 (5.8%) | 32 (61.5%) | <0.0001 |
| Postprocedural Outcomes (<72 h after the Index Procedure) of the Study Population (n = 269) | Unmatched (n = 269) | Matched (n = 52) | |||||
|---|---|---|---|---|---|---|---|
| Tricuspid (n = 217) | Bicuspid (n = 52) | p Value | Tricuspid (n = 52) | Bicuspid (n = 52) | p Value | ||
| Outcome | No. (%) of Events | ||||||
| In-hospital mortality | 3 (1.1%) | 3 (1.4%) | 0 | 0.394 | 0 | 0 | NA |
| Device success | 267 (99.3%) | 215 (99.1%) | 52 (100%) | 0.487 | 52 (100%) | 52 (100%) | NA |
| Myocardial infarction | 0 | 0 | 0 | NA | 0 | 0 | NA |
| Coronary obstruction | 0 | 0 | 0 | NA | 0 | 0 | NA |
| TIA | 1 (0.4%) | 0 | 1 (1.9%) | 0.041 | 0 | 1 (1.9%) | 0.315 |
| Stroke | 3 (1.2%) | 2 (0.9%) | 1 (1.9%) | 0.537 | 0 | 1 (1.9%) | 0.315 |
| Acute kidney injure, stage 2 or 3 | 5 (1.8%) | 5 (2.3%) | 0 | 0.269 | 1 (1.9%) | 0 | 0.315 |
| Minor vascular complications | 19 (7.1%) | 15 (6.9%) | 4 (7.4%) | 0.844 | 3 (5.7%) | 4 (7.7%) | 0.696 |
| Major vascular complications | 7 (2.6%) | 5 (2.3%) | 2 (3.8%) | 0.530 | 0 | 2 (3.8%) | 0.475 |
| Permanent Pacemaker Implantation | 76 (31.1%) | 59 (30.4%) | 17 (34%) | 0.429 | 12 (24%) | 17 (34%) | 0.274 |
| Cardiac tamponade | 1 (0.4%) | 1 (0.5%) | 0 | 0.624 | 0 | 0 | NA |
| Annulus rupture | 0 | 0 | 0 | NA | 0 | 0 | NA |
| Valve malpositioning | 1 (0.4%) | 1 (0.5%) | 0 | 0.624 | 0 | 0 | NA |
| Need for a second valve | 0 | 0 | 0 | NA | 0 | 0 | NA |
| Postprocedural AR grade III or IV | 0 | 0 | 0 | NA | 0 | 0 | NA |
| VARC-2 Outcomes at 30 Days Follow-Up | Unmatched (n = 269) | Matched (n = 52) | |||||
|---|---|---|---|---|---|---|---|
| Tricuspid (n = 217) | Bicuspid (n = 52) | p Value | Tricuspid (n = 52) | Bicuspid (n = 52) | p Value | ||
| 30-Day Cumulative Clinical Outcomes (n = 269) | No. (%) of Events | ||||||
| All-cause mortality | 5 (1.8%) | 5 (2.3%) | 0 | 0.269 | 0 | 0 | NA |
| Cardiac mortality | 1 (0.4%) | 1 (0.5%) | 0 | 0.623 | 0 | 0 | NA |
| All stroke | 3 (1.2%) | 2 (0.9%) | 1 (1.9%) | 0.537 | 0 | 1 (1.9%) | 0.315 |
| Life-threatening bleeding | 1 (0.4%) | 1 (0.5%) | 0 | 0.623 | 0 | 0 | NA |
| Acute kidney injury, stage 2 or 3 | 2 (2.4%) | 2 (0.9%) | 0 | 0.486 | 0 | 0 | NA |
| Coronary artery obstruction | 0 | 0 | 0 | NA | 0 | 0 | NA |
| Minor vascular complications | 19 (7.1%) | 15 (6.9%) | 4 (7.7%) | 0.844 | 3 (5.7%) | 4 (7.7%) | 0.696 |
| Major vascular complications | 7 (2.6%) | 5 (2.3%) | 2 (3.8%) | 0.530 | 0 | 2 (3.8%) | 0.475 |
| New pacemaker implantation | 76 (31.1%) | 59 (30.4%) | 17 (34%) | 0.429 | 12 (24%) | 17 (34%) | 0.274 |
| Valve-related dysfunction requiring repeat procedure (BAV, TAVI, or SAVR) | 0 | 0 | 0 | NA | 0 | 0 | NA |
| NYHA class III or IV | 2 (2.4%) | 2 (0.9%) | 0 | 0.621 | 0 | 0 | NA |
| Prosthetic valve endocarditis | 0 | 0 | 0 | NA | 0 | 0 | NA |
| Prosthetic valve thrombosis | 0 | 0 | 0 | NA | 0 | 0 | NA |
| Thrombo-embolic events | 0 | 0 | 0 | NA | 0 | 0 | NA |
| Transthoracic Echocardiography Follow Up Data | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Unmatched (n = 269) | Unmatched (n = 266) | Unmatched (n = 264) | |||||||
| Tricuspid Baseline (n = 217) | Bicuspid Baseline (n = 52) | p Value | Tricuspid Discharge (n = 214) | Bicuspid Discharge (n = 52) | p Value | Tricuspid 30-Days (n = 212) | Bicuspid 30-Days (n = 52) | p Value | |
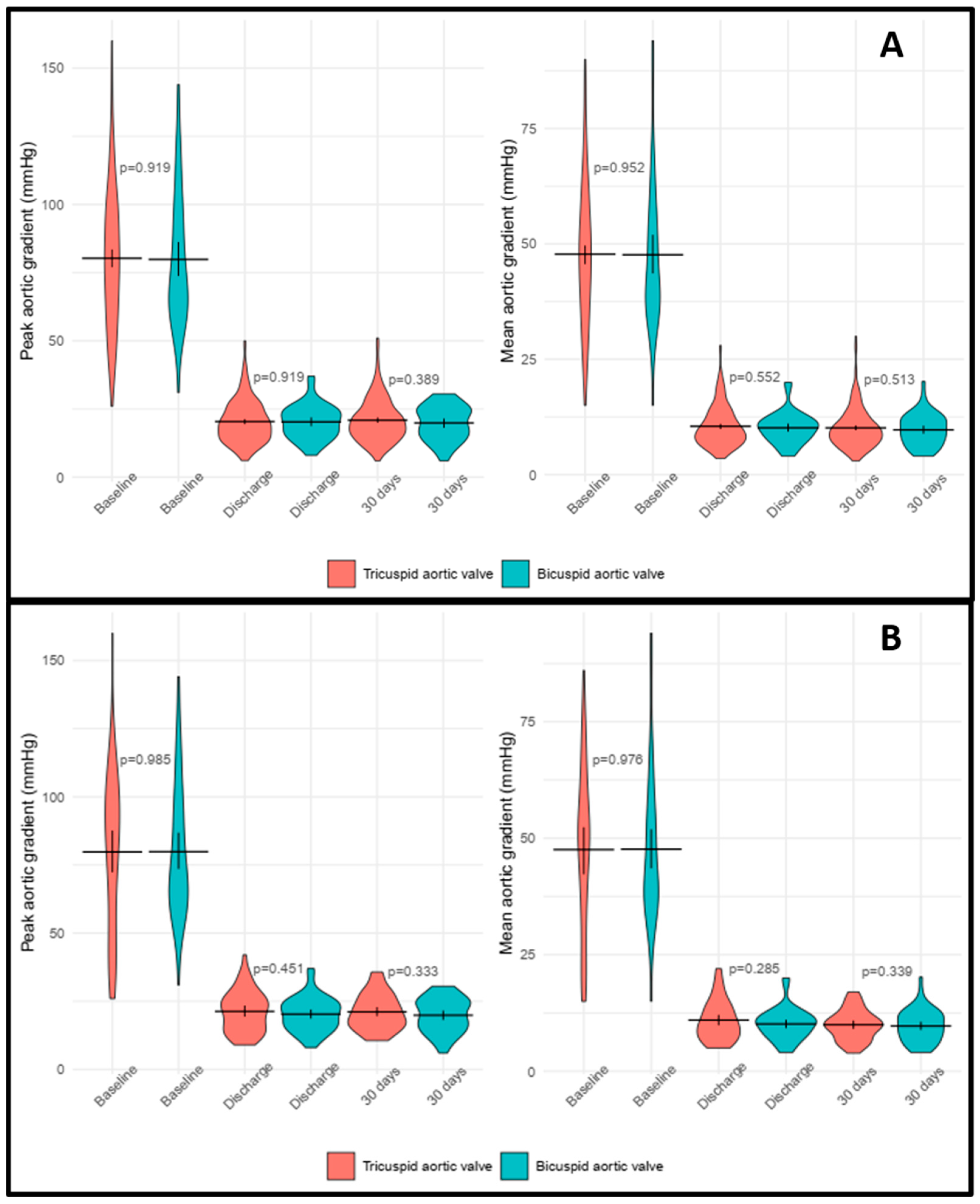
| Peak aortic gradient, mmHg * | 80.3 ± 25.7 | 79.9 ± 24.1 | 0.919 | 20.4 ± 7.7 | 20.3 ± 6.2 | 0.919 | 20.9 ± 7.8 | 19.9 ± 6.3 | 0.389 |
| Mean aortic gradient, mmHg * | 47.8 ± 15.5 | 47.6 ± 15.9 | 0.952 | 10.5 ± 4.3 | 10.1 ± 3.4 | 0.552 | 10.1 ± 4.3 | 9.7 ± 3.5 | 0.513 |
| LVEF, % | 55.5 ± 12.7 | 54.2 ± 13.6 | 0.517 | 56 ± 9.7 | 56.4 ± 12.1 | 0.812 | 59.7 ± 10.3 | 59.1 ± 11.7 | 0.688 |
| Aortic regurgitation grade 2 or above | 81 (37.3%) | 19 (36.5%) | 0.916 | 12 (5.6%) | 1 (1.9%) | 0.269 | 4 (1.8%) | 1 (1.9%) | 0.986 |
| Paravalvular leakage trace/mild | NA | NA | NA | 4 (1.8%) | 2 (3.8%) | 0.389 | 8 (3.7%) | 3 (5.7%) | 0.519 |
| Paravalvular leakage moderate or above | NA | NA | NA | 2 (0.9%) | 0 | 0.484 | 1 (1.9%) | 0 | 0.620 |
| Matched (n = 52) | Matched (n = 52) | Matched (n = 52) | |||||||
| Tricuspid Baseline (n = 52) | Bicuspid Baseline (n = 52) | p Value | Tricuspid Discharge (n = 52) | Bicuspid Discharge (n = 52) | p Value | Tricuspid 30-Days (n = 52) | Bicuspid 30-Days (n = 52) | p Value | |
| Peak aortic gradient, mmHg * | 79.8 ± 29.1 | 79.9 ± 24.1 | 0.985 | 21.3 ± 7.6 | 20.3 ± 6.2 | 0.451 | 21.1 ± 6.6 | 19.9 ± 6.3 | 0.333 |
| Mean aortic gradient, mmHg * | 47.5 ± 17.6 | 47.6 ± 15.9 | 0.976 | 10.9 ± 4.3 | 10.1 ± 3.4 | 0.285 | 9.9 ± 3.2 | 9.7 ± 3.5 | 0.339 |
| LVEF, % | 55 ± 13.9 | 54.2 ± 13.6 | 0.771 | 55 ± 10.3 | 56.4 ± 12.1 | 0.531 | 60.3 ± 11.5 | 59.1 ± 11.7 | 0.601 |
| Aortic regurgitation grade 2 or above | 23 (44.2%) | 19 (36.5%) | 0.424 | 3 (5.7%) | 1 | 0.308 | 1 (1.9%) | 1 (1.9%) | 1 |
| Paravalvular leakage trace/mild | NA | NA | NA | 3 (5.7%) | 2 | 0.647 | 5 (9.6%) | 3 (5.7%) | 0.462 |
| Paravalvular leakage moderate or above | NA | NA | NA | 1 (1.9%) | 0 | 0.315 | 1 (1.9%) | 0 | 0.315 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magyari, B.; Kittka, B.; Goják, I.; Schönfeld, K.; Szapáry, L.B.; Simon, M.; Kiss, R.; Bertalan, A.; Várady, E.; Gyimesi, A.; et al. Single-Center Experience with the Balloon-Expandable Myval Transcatheter Aortic Valve System in Patients with Bicuspid Anatomy: Procedural and 30-Day Follow-Up. J. Clin. Med. 2024, 13, 513. https://doi.org/10.3390/jcm13020513
Magyari B, Kittka B, Goják I, Schönfeld K, Szapáry LB, Simon M, Kiss R, Bertalan A, Várady E, Gyimesi A, et al. Single-Center Experience with the Balloon-Expandable Myval Transcatheter Aortic Valve System in Patients with Bicuspid Anatomy: Procedural and 30-Day Follow-Up. Journal of Clinical Medicine. 2024; 13(2):513. https://doi.org/10.3390/jcm13020513
Chicago/Turabian StyleMagyari, Balázs, Bálint Kittka, Ilona Goják, Kristóf Schönfeld, László Botond Szapáry, Mihály Simon, Rudolf Kiss, Andrea Bertalan, Edit Várady, András Gyimesi, and et al. 2024. "Single-Center Experience with the Balloon-Expandable Myval Transcatheter Aortic Valve System in Patients with Bicuspid Anatomy: Procedural and 30-Day Follow-Up" Journal of Clinical Medicine 13, no. 2: 513. https://doi.org/10.3390/jcm13020513