
The Association of Tobacco Smoking and Level of Apoptosis in the Long Head of the Biceps Chronic Tendinopathy—An Immunohistochemical Study


 ,
, 
 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Material and Methods
2.1. Preoperative Assessment
2.2. Surgical Technique
2.3. Histopathological Assessment
2.4. Clinical Evaluation
2.5. Ethics Statement
2.6. Statistical Analysis
3. Results
3.1. Surgical technique
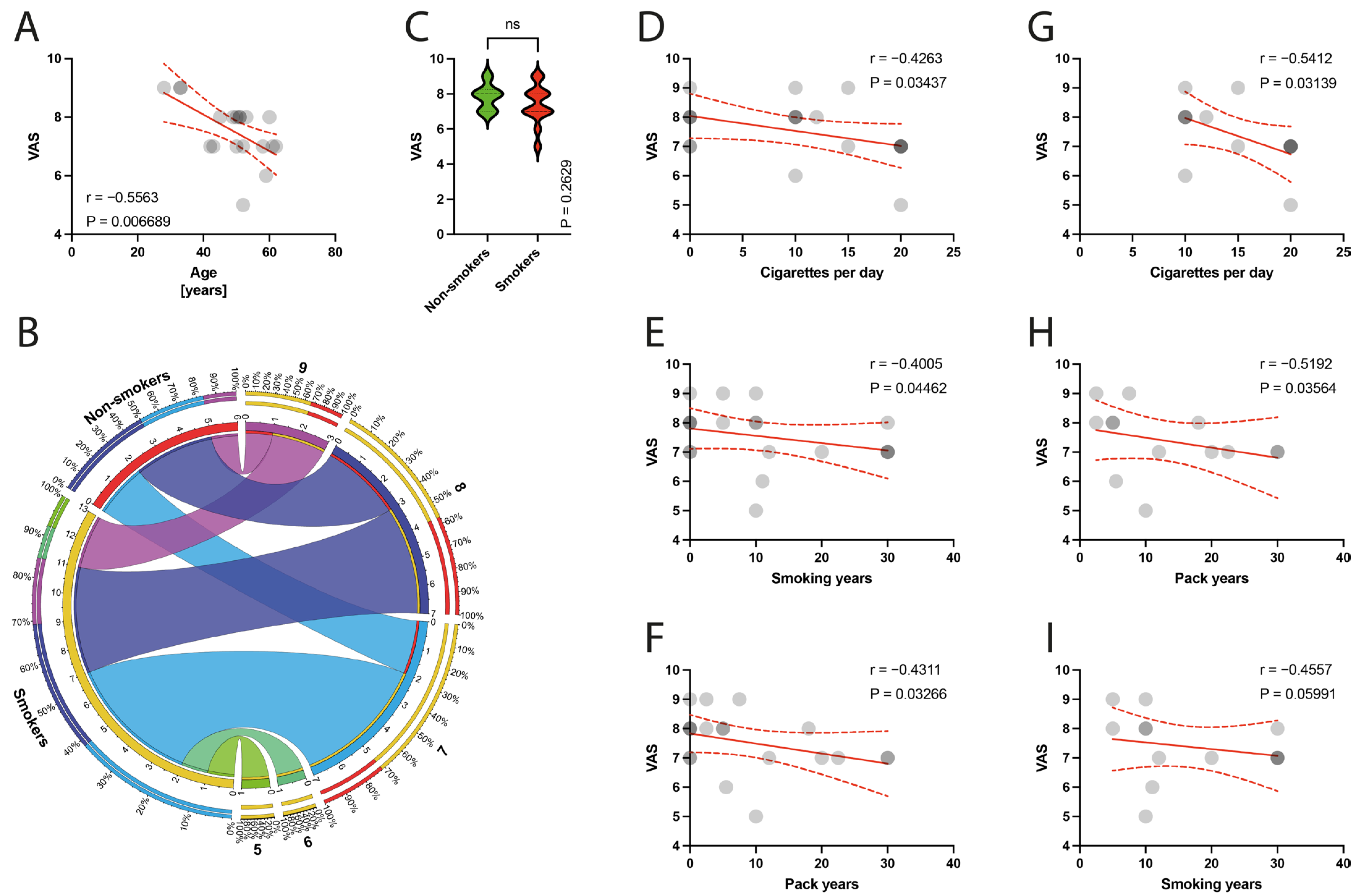
3.2. Clinical Outcomes
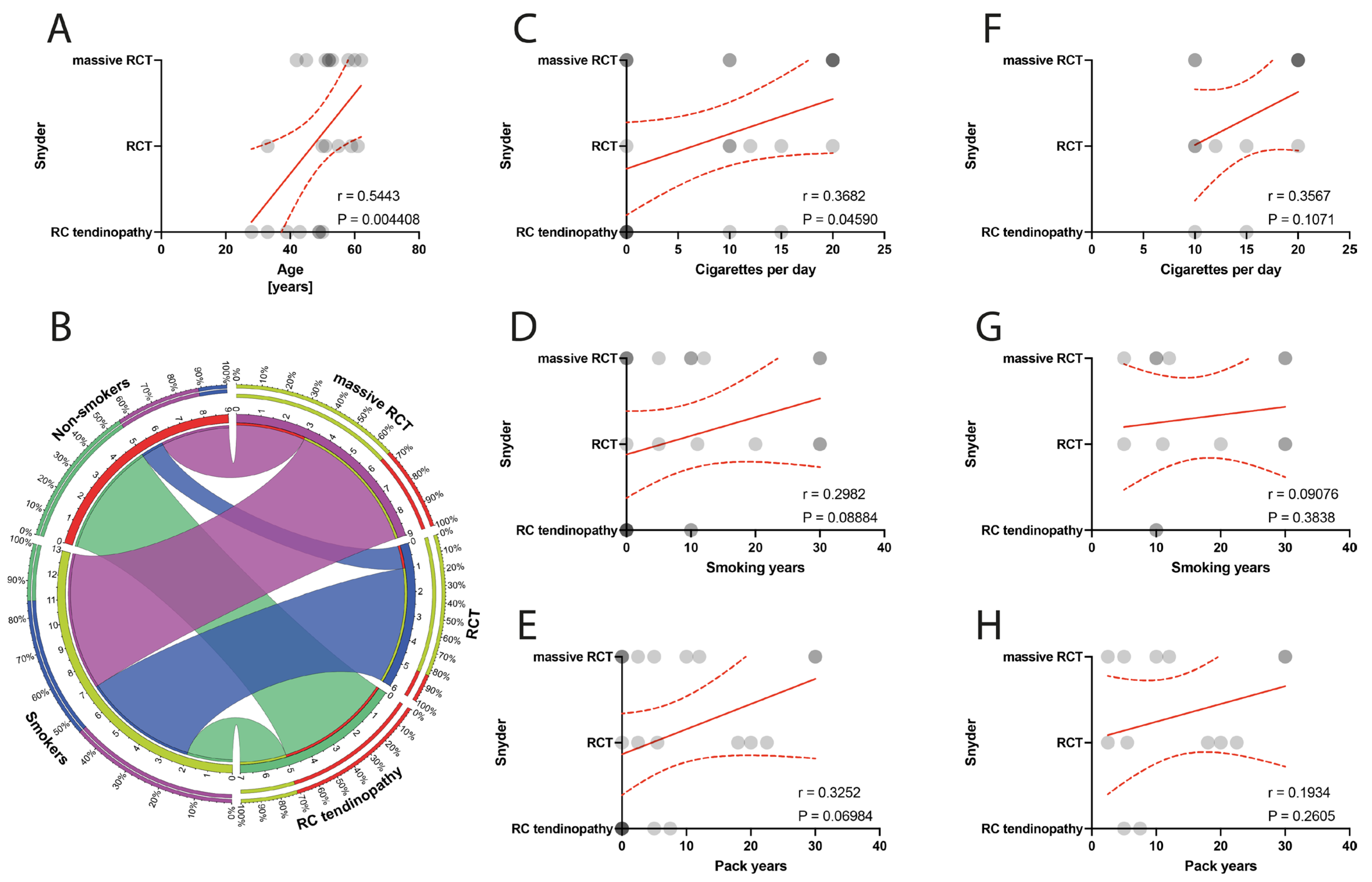
3.3. Immunohistochemical Examination
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abate, M.; Vanni, D.; Pantalone, A.; Salini, V. Cigarette Smoking and Musculoskeletal Disorders. Muscles Ligaments Tendons J. 2013, 3, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Baumgarten, K.M.; Gerlach, D.; Galatz, L.M.; Teefey, S.A.; Middleton, W.D.; Ditsios, K.; Yamaguchi, K. Cigarette Smoking Increases the Risk for Rotator Cuff Tears. Clin. Orthop. Relat. Res. 2010, 468, 1534–1541. [Google Scholar] [CrossRef] [PubMed]
- Ho, S. Adverse Effects of Smoking on Outcomes of Orthopaedic Surgery. J. Orthop. Trauma Rehabil. 2017, 23, 54–58. [Google Scholar] [CrossRef]
- Zabrzynski, J.; Gagat, M.; Paczesny, L.; Grzanka, D.; Huri, G. Correlation between Smoking and Neovascularization in Biceps Tendinopathy—A Functional Preoperative and Immunohistochemical Study. Ther. Adv. Chronic Dis. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Roemer, E.; Stabbert, R.; Rustemeier, K.; Veltel, D.J.; Meisgen, T.J.; Reininghaus, W.; Carchman, R.A.; Gaworski, C.L.; Podraza, K.F. Chemical Composition, Cytotoxicity and Mutagenicity of Smoke from US Commercial and Reference Cigarettes Smoked under Two Sets of Machine Smoking Conditions. Toxicology 2004, 195, 31–52. [Google Scholar] [CrossRef] [PubMed]
- Cheema, A.N.; Newton, J.B.; Boorman-Padgett, J.F.; Weiss, S.N.; Nuss, C.A.; Gittings, D.J.; Farber, D.C.; Soslowsky, L.J. Nicotine Impairs Intra-substance Tendon Healing after Full Thickness Injury in a Rat Model. J. Orthop. Res. 2019, 37, 94–103. [Google Scholar] [CrossRef]
- Lundgreen, K.; Lian, Ø.B.; Scott, A.; Fearon, A.; Engebretsen, L. 58 Smokers Have Worse Rotator Cuff Teartendon Degeneration and Apoptosis. Br. J. Sports Med. 2014, 48, A37–A38. [Google Scholar] [CrossRef]
- Zabrzyński, J.; Huri, G.; Gagat, M.; Łapaj, Ł.; Yataganbaba, A.; Szwedowski, D.; Askin, M.; Paczesny, Ł. The Impact of Smoking on Clinical Results Following the Rotator Cuff and Biceps Tendon Complex Arthroscopic Surgery. J. Clin. Med. 2021, 10, 599. [Google Scholar] [CrossRef]
- Zabrzyński, J.; Gagat, M.; Łapaj, Ł.; Paczesny, Ł.; Yataganbaba, A.; Szwedowski, D.; Huri, G. Relationship between Long Head of the Biceps Tendon Histopathology and Long-Term Functional Results in Smokers. A Time to Reevaluate the Bonar Score? Ther. Adv. Chronic Dis. 2021, 12, 204062232199026. [Google Scholar] [CrossRef]
- Zabrzyński, J.; Łapaj, Ł.; Paczesny, Ł.; Zabrzyńska, A.; Grzanka, D. Tendon—Function-Related Structure, Simple Healing Process and Mysterious Ageing. Folia Morphol. 2018, 77, 416–427. [Google Scholar] [CrossRef]
- Osti, L.; Buda, M.; Del Buono, A.; Osti, R.; Massari, L.; Maffulli, N. Apoptosis and Rotator Cuff Tears: Scientific Evidence from Basic Science to Clinical Findings. Br. Med. Bull. 2017, 122, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Egerbacher, M.; Arnoczky, S.P.; Caballero, O.; Lavagnino, M.; Gardner, K.L. Loss of Homeostatic Tension Induces Apoptosis in Tendon Cells: An In Vitro Study. Clin. Orthop. Relat. Res. 2008, 466, 1562–1568. [Google Scholar] [CrossRef] [PubMed]
- Lundgreen, K.; Lian, O.B.; Engebretsen, L.; Scott, A. Tenocyte Apoptosis in the Torn Rotator Cuff: A Primary or Secondary Pathological Event? Br. J. Sports Med. 2011, 45, 1035–1039. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.F.; Chen, C.H.; Cao, Y.; Avanessian, B.; Wang, X.T.; Tang, J.B. Molecular Events of Cellular Apoptosis and Proliferation in the Early Tendon Healing Period. J. Hand Surg. 2010, 35, 2–10. [Google Scholar] [CrossRef]
- Li, K.; Deng, Y.; Deng, G.; Chen, P.; Wang, Y.; Wu, H.; Ji, Z.; Yao, Z.; Zhang, X.; Yu, B.; et al. High Cholesterol Induces Apoptosis and Autophagy through the ROS-Activated AKT/FOXO1 Pathway in Tendon-Derived Stem Cells. Stem Cell Res. Ther. 2020, 11, 131. [Google Scholar] [CrossRef] [PubMed]
- Ditsios, K.; Agathangelidis, F.; Boutsiadis, A.; Karataglis, D.; Papadopoulos, P. Long Head of the Biceps Pathology Combined with Rotator Cuff Tears. Available online: https://www.hindawi.com/journals/aorth/2012/405472/ (accessed on 7 November 2018).
- Santiago-Torres, J.; Flanigan, D.C.; Butler, R.B.; Bishop, J.Y. The Effect of Smoking on Rotator Cuff and Glenoid Labrum Surgery: A Systematic Review. Am. J. Sports Med. 2015, 43, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Belay, E.S.; Wittstein, J.R.; Garrigues, G.E.; Lassiter, T.E.; Scribani, M.; Goldner, R.D.; Bean, C.A. Biceps Tenotomy Has Earlier Pain Relief Compared to Biceps Tenodesis: A Randomized Prospective Study. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 4032–4037. [Google Scholar] [CrossRef]
- Lundgreen, K.; Lian, O.B.; Scott, A.; Nassab, P.; Fearon, A.; Engebretsen, L. Rotator Cuff Tear Degeneration and Cell Apoptosis in Smokers versus Nonsmokers. Arthroscopy 2014, 30, 936–941. [Google Scholar] [CrossRef]
- Zabrzyński, J.; Huri, G.; Gryckiewicz, S.; Çetik, R.M.; Szwedowski, D.; Łapaj, Ł.; Gagat, M.; Paczesny, Ł. Biceps Tenodesis versus Tenotomy with Fast Rehabilitation Protocol-A Functional Perspective in Chronic Tendinopathy. J. Clin. Med. 2020, 9, 3938. [Google Scholar] [CrossRef]
- Vaishnav, S.; Millett, P.J. Arthroscopic Rotator Cuff Repair: Scientific Rationale, Surgical Technique, and Early Clinical and Functional Results of a Knotless Self-Reinforcing Double-Row Rotator Cuff Repair System. J. Shoulder Elb. Surg. 2010, 19, 83–90. [Google Scholar] [CrossRef]
- Rossi, L.A.; Chahla, J.; Verma, N.N.; Millett, P.J.; Ranalletta, M. Rotator Cuff Retears. JBJS Rev. 2020, 8, e0039. [Google Scholar] [CrossRef] [PubMed]
- Scott, A.; Khan, K.M.; Heer, J.; Cook, J.L.; Lian, O.; Duronio, V. High Strain Mechanical Loading Rapidly Induces Tendon Apoptosis: An Ex Vivo Rat Tibialis Anterior Model. Br. J. Sports Med. 2005, 39, e25. [Google Scholar] [CrossRef] [PubMed]
- Igney, F.H.; Krammer, P.H. Death and Anti-Death: Tumour Resistance to Apoptosis. Nat. Rev. Cancer 2002, 2, 277–288. [Google Scholar] [CrossRef] [PubMed]
- Satou, T. Warm drug solution injected into tumor vessel may enhance antitumor effect. Gan Kagaku Ryoho 1990, 17, 1763–1767. [Google Scholar]
- Yuan, J.; Murrell, G.A.C.; Wei, A.-Q.; Wang, M.-X. Apoptosis in Rotator Cuff Tendonopathy. J. Orthop. Res. 2002, 20, 1372–1379. [Google Scholar] [CrossRef] [PubMed]
- Benson, R.T.; McDonnell, S.M.; Knowles, H.J.; Rees, J.L.; Carr, A.J.; Hulley, P.A. Tendinopathy and Tears of the Rotator Cuff Are Associated with Hypoxia and Apoptosis. J. Bone Jt. Surg. Br. Vol. 2010, 92, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.-T.; Jou, I.-M.; Yang, C.-C.; Lin, C.-J.; Yang, C.-Y.; Su, F.-C.; Su, W.-R. The Severity of the Long Head Biceps Tendinopathy in Patients with Chronic Rotator Cuff Tears: Macroscopic versus Microscopic Results. J. Shoulder Elb. Surg. 2014, 23, 1099–1106. [Google Scholar] [CrossRef]
- Chen, J.; Wang, A.; Xu, J.; Zheng, M. In Chronic Lateral Epicondylitis, Apoptosis and Autophagic Cell Death Occur in the Extensor Carpi Radialis Brevis Tendon. J Shoulder Elb. Surg 2010, 19, 355–362. [Google Scholar] [CrossRef]
- Puzzitiello, R.N.; Patel, B.H.; Forlenza, E.M.; Nwachukwu, B.U.; Allen, A.A.; Forsythe, B.; Salzler, M.J. Adverse Impact of Corticosteroids on Rotator Cuff Tendon Health and Repair: A Systematic Review of Basic Science Studies. Arthrosc. Sports Med. Rehabil. 2020, 2, e161–e169. [Google Scholar] [CrossRef]
- Pearce, C.J.; Ismail, M.; Calder, J.D. Is Apoptosis the Cause of Noninsertional Achilles Tendinopathy? Am. J. Sports Med. 2009, 37, 2440–2444. [Google Scholar] [CrossRef]
- Tuoheti, Y.; Itoi, E.; Pradhan, R.L.; Wakabayashi, I.; Takahashi, S.; Minagawa, H.; Kobayashi, M.; Okada, K.; Shimada, Y. Apoptosis in the Supraspinatus Tendon with Stage II Subacromial Impingement. J. Shoulder Elb. Surg. 2005, 14, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Lundgreen, K.; Lian, Ø.; Scott, A.; Engebretsen, L. Increased Levels of Apoptosis and P53 in Partial-Thickness Supraspinatus Tendon Tears. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 1636–1641. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Hashemi, S.; Han, W.; Song, Y.; Lim, Y. Exposure and Risk Assessment of Second- and Third-Hand Tobacco Smoke Using Urinary Cotinine Levels in South Korea. Int. J. Environ. Res. Public Health 2022, 19, 3746. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Hashemi, S.; Kim, T.; Park, J.; Park, M.; Han, W.; Park, D.; Lim, Y. Risk Assessment and Estimation of Controlling Safe Distance for Exposure to Particulate Matter from Outdoor Secondhand Tobacco Smoke. Air Qual. Atmos. Health. 2023, 1–16. [Google Scholar] [CrossRef]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jaworski, Ł.M.; Zabrzyński, J.; Millett, P.J.; Rupp, M.-C.; Familiari, F.; Huri, G.; Antosik, P.; Błachowski, M.; Wiciński, M.; Gagat, M. The Association of Tobacco Smoking and Level of Apoptosis in the Long Head of the Biceps Chronic Tendinopathy—An Immunohistochemical Study. J. Clin. Med. 2024, 13, 684. https://doi.org/10.3390/jcm13030684
Jaworski ŁM, Zabrzyński J, Millett PJ, Rupp M-C, Familiari F, Huri G, Antosik P, Błachowski M, Wiciński M, Gagat M. The Association of Tobacco Smoking and Level of Apoptosis in the Long Head of the Biceps Chronic Tendinopathy—An Immunohistochemical Study. Journal of Clinical Medicine. 2024; 13(3):684. https://doi.org/10.3390/jcm13030684
Chicago/Turabian StyleJaworski, Łukasz M., Jan Zabrzyński, Peter J. Millett, Marco-Christopher Rupp, Filippo Familiari, Gazi Huri, Paulina Antosik, Michał Błachowski, Michał Wiciński, and Maciej Gagat. 2024. "The Association of Tobacco Smoking and Level of Apoptosis in the Long Head of the Biceps Chronic Tendinopathy—An Immunohistochemical Study" Journal of Clinical Medicine 13, no. 3: 684. https://doi.org/10.3390/jcm13030684
APA StyleJaworski, Ł. M., Zabrzyński, J., Millett, P. J., Rupp, M.-C., Familiari, F., Huri, G., Antosik, P., Błachowski, M., Wiciński, M., & Gagat, M. (2024). The Association of Tobacco Smoking and Level of Apoptosis in the Long Head of the Biceps Chronic Tendinopathy—An Immunohistochemical Study. Journal of Clinical Medicine, 13(3), 684. https://doi.org/10.3390/jcm13030684