
Achieving Textbook Outcomes in Colorectal Cancer Surgery Is Associated with Improved Long-Term Survival: Results of the Multicenter Prospective Cohort Study

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Statement
2.2. Study Setting and Patients
2.3. Textbook Outcome Definition
2.4. Study Outcomes
2.5. Statistical Analysis
3. Results
3.1. Study Patients
3.2. Contributors of Individual Parameters to Textbook Outcome
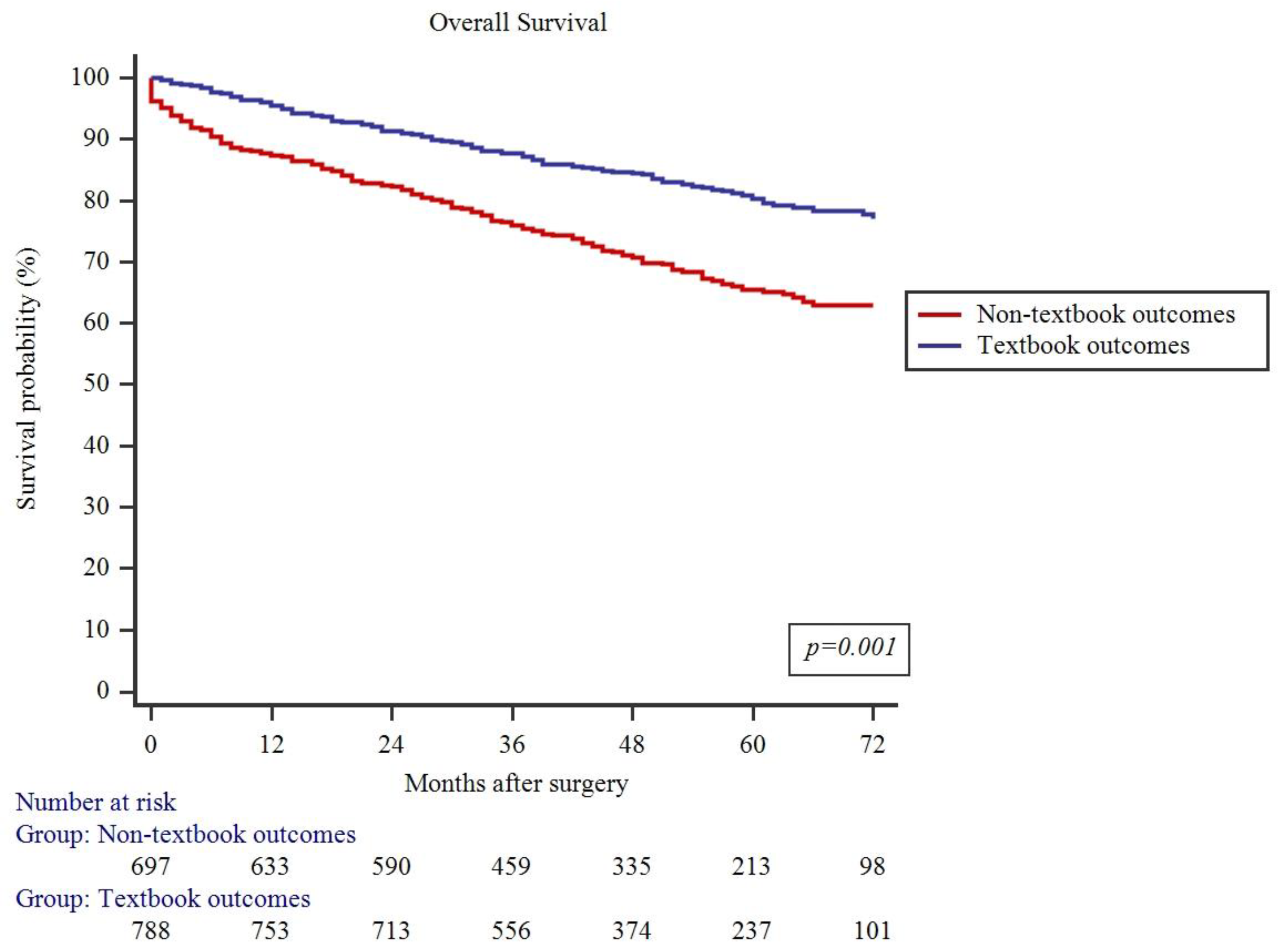
3.3. Association of Textbook Outcome and 5-Year DFS and OS Rates
3.4. Factors Associated with Textbook Outcome
3.5. Association of Textbook Outcome and Surgeon Volume
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Xi, Y.; Xu, P. Global Colorectal Cancer Burden in 2020 and Projections to 2040. Transl. Oncol. 2021, 14, 101174. [Google Scholar] [CrossRef] [PubMed]
- Dulskas, A.; Kuliavas, J.; Sirvys, A.; Bausys, A.; Kryzauskas, M.; Bickaite, K.; Abeciunas, V.; Kaminskas, T.; Poskus, T.; Strupas, K. Anastomotic Leak Impact on Long-Term Survival after Right Colectomy for Cancer: A Propensity-Score-Matched Analysis. J. Clin. Med. 2022, 11, 4375. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.-C.; Tian, Y.-F.; Liu, W.-S.; Chou, C.-L.; Cheng, L.-C.; Chu, S.-S.; Lee, C.-C. The Association between the Composite Quality Measure “Textbook Outcome” and Long Term Survival in Operated Colon Cancer. Med. (Baltim.) 2020, 99, e22447. [Google Scholar] [CrossRef]
- Bausys, A.; Kryzauskas, M.; Abeciunas, V.; Degutyte, A.E.; Bausys, R.; Strupas, K.; Poskus, T. Prehabilitation in Modern Colorectal Cancer Surgery: A Comprehensive Review. Cancers 2022, 14, 5017. [Google Scholar] [CrossRef] [PubMed]
- Boland, G.M.; Chang, G.J.; Haynes, A.B.; Chiang, Y.-J.; Chagpar, R.; Xing, Y.; Hu, C.-Y.; Feig, B.W.; You, Y.N.; Cormier, J.N. Association between Adherence to National Comprehensive Cancer Network Treatment Guidelines and Improved Survival in Patients with Colon Cancer. Cancer 2013, 119, 1593–1601. [Google Scholar] [CrossRef]
- Orangio, G.R. A National Accreditation Program for Rectal Cancer: A Long and Winding Road. Dis. Colon Rectum 2018, 61, 145–146. [Google Scholar] [CrossRef] [PubMed]
- Auer, R.C.; Balaa, F.K. Textbook Oncologic Outcome Summarizes the Perioperative Cancer Journey, but Should It Be Used to Judge Hospitals? Ann. Surg. Oncol. 2021, 28, 8025–8027. [Google Scholar] [CrossRef]
- Dijs-Elsinga, J.; Otten, W.; Versluijs, M.M.; Smeets, H.J.; Kievit, J.; Vree, R.; van der Made, W.J.; Marang-van de Mheen, P.J. Choosing a Hospital for Surgery: The Importance of Information on Quality of Care. Med. Decis. Mak. Int. J. Soc. Med. Decis. Mak. 2010, 30, 544–555. [Google Scholar] [CrossRef]
- Tsilimigras, D.I.; Pawlik, T.M.; Moris, D. Textbook Outcomes in Hepatobiliary and Pancreatic Surgery. World J. Gastroenterol. 2021, 27, 1524–1530. [Google Scholar] [CrossRef]
- Kolfschoten, N.E.; Kievit, J.; Gooiker, G.A.; van Leersum, N.J.; Snijders, H.S.; Eddes, E.H.; Tollenaar, R.A.E.M.; Wouters, M.W.J.M.; Mheen, P.J.M. de Focusing on Desired Outcomes of Care after Colon Cancer Resections; Hospital Variations in ‘Textbook Outcome’. Eur. J. Surg. Oncol. 2013, 39, 156–163. [Google Scholar] [CrossRef]
- Manatakis, D.K.; Tzardi, M.; Souglakos, J.; Tsiaoussis, J.; Agalianos, C.; Kyriazanos, I.D.; Pechlivanides, G.; Kordelas, A.; Tasis, N.; Gouvas, N.; et al. Achieving a Textbook Outcome in Colon Cancer Surgery Is Associated with Improved Long-Term Survival. Curr. Oncol. 2023, 30, 2879–2888. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of Surgical Complications. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Azevedo, J.M.; Panteleimonitis, S.; Mišković, D.; Herrando, I.; Al-Dhaheri, M.; Ahmad, M.; Qureshi, T.; Fernandez, L.M.; Harper, M.; Parvaiz, A. Textbook Oncological Outcomes for Robotic Colorectal Cancer Resections: An Observational Study of Five Robotic Colorectal Units. Cancers 2023, 15, 3760. [Google Scholar] [CrossRef] [PubMed]
- Maeda, Y.; Iwatsuki, M.; Mitsuura, C.; Morito, A.; Ohuchi, M.; Kosumi, K.; Eto, K.; Ogawa, K.; Baba, Y.; Iwagami, S.; et al. Textbook Outcome Contributes to Long-Term Prognosis in Elderly Colorectal Cancer Patients. Langenbecks Arch. Surg. 2023, 408, 245. [Google Scholar] [CrossRef] [PubMed]
- Voigt, K.R.; de Graaff, M.R.; Verhoef, C.; Kazemier, G.; Swijneburg, R.J.; Mieog, J.S.D.; Derksen, W.J.M.; Buis, C.I.; Gobardhan, P.D.; Dulk, M.D.; et al. Association of Modified Textbook Outcome and Overall Survival after Surgery for Colorectal Liver Metastases: A Nationwide Analysis. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2024, 50, 107972. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Kim, S.-H.; Choi, J.-H.; Choe, H.N.; Park, J.-H.; Kong, S.-H.; Kwak, Y.; Park, D.J.; Lee, H.S.; Lee, H.-J.; et al. Proposal of Modified Textbook Outcome for Improving the Quality of Gastric Cancer Surgery: A Single-Center Study. J. Clin. Oncol. 2022, 40, 270. Available online: https://ascopubs.org/doi/10.1200/JCO.2022.40.4_suppl.270 (accessed on 12 February 2024). [CrossRef]
- Mehta, R.; Tsilimigras, D.I.; Paredes, A.Z.; Sahara, K.; Moro, A.; Farooq, A.; White, S.; Ejaz, A.; Tsung, A.; Dillhoff, M.; et al. Comparing Textbook Outcomes among Patients Undergoing Surgery for Cancer at U. S. News & World Report Ranked Hospitals. J. Surg. Oncol. 2020, 121, 927–935. [Google Scholar] [CrossRef]
- Busweiler, L.A.D.; Schouwenburg, M.G.; van Berge Henegouwen, M.I.; Kolfschoten, N.E.; de Jong, P.C.; Rozema, T.; Wijnhoven, B.P.L.; van Hillegersberg, R.; Wouters, M.W.J.M.; van Sandick, J.W.; et al. Textbook Outcome as a Composite Measure in Oesophagogastric Cancer Surgery. Br. J. Surg. 2017, 104, 742–750. [Google Scholar] [CrossRef]
- Merath, K.; Chen, Q.; Bagante, F.; Beal, E.; Akgul, O.; Dillhoff, M.; Cloyd, J.M.; Pawlik, T.M. Textbook Outcomes Among Medicare Patients Undergoing Hepatopancreatic Surgery. Ann. Surg. 2020, 271, 1116–1123. [Google Scholar] [CrossRef]
- Fukuoka, A.; Makizumi, R.; Asano, T.; Hamabe, T.; Otsubo, T. Surgical Outcomes of Colorectal Cancer Surgery for ≥ 85-Year-Old Patients in Our Hospital: Retrospective Comparison of Short- and Long-Term Outcomes with Younger Patients. J. Anus Rectum Colon 2021, 5, 247–253. [Google Scholar] [CrossRef]
- Warps, A.K.; Detering, R.; Tollenaar, R.A.E.M.; Tanis, P.J.; Dekker, J.W.T. Dutch ColoRectal Audit group Textbook Outcome after Rectal Cancer Surgery as a Composite Measure for Quality of Care: A Population-Based Study. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2021, 47, 2821–2829. [Google Scholar] [CrossRef]
- van Roessel, S.; Mackay, T.M.; van Dieren, S.; van der Schelling, G.P.; Nieuwenhuijs, V.B.; Bosscha, K.; van der Harst, E.; van Dam, R.M.; Liem, M.S.L.; Festen, S.; et al. Textbook Outcome: Nationwide Analysis of a Novel Quality Measure in Pancreatic Surgery. Ann. Surg. 2020, 271, 155–162. [Google Scholar] [CrossRef] [PubMed]
- de Graaff, M.R.; Elfrink, A.K.E.; Buis, C.I.; Swijnenburg, R.-J.; Erdmann, J.I.; Kazemier, G.; Verhoef, C.; Mieog, J.S.D.; Derksen, W.J.M.; van den Boezem, P.B.; et al. Defining Textbook Outcome in Liver Surgery and Assessment of Hospital Variation: A Nationwide Population-Based Study. Eur. J. Surg. Oncol. 2022, 48, 2414–2423. [Google Scholar] [CrossRef] [PubMed]
- Naffouje, S.A.; Ali, M.A.; Kamarajah, S.K.; White, B.; Salti, G.I.; Dahdaleh, F. Assessment of Textbook Oncologic Outcomes Following Proctectomy for Rectal Cancer. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract 2022, 26, 1286–1297. [Google Scholar] [CrossRef] [PubMed]
- Huo, Y.R.; Phan, K.; Morris, D.L.; Liauw, W. Systematic Review and a Meta-Analysis of Hospital and Surgeon Volume/Outcome Relationships in Colorectal Cancer Surgery. J. Gastrointest. Oncol. 2017, 8, 534–546. [Google Scholar] [CrossRef] [PubMed]
- Birkmeyer, J.D.; Stukel, T.A.; Siewers, A.E.; Goodney, P.P.; Wennberg, D.E.; Lucas, F.L. Surgeon Volume and Operative Mortality in the United States. N. Engl. J. Med. 2003, 349, 2117–2127. [Google Scholar] [CrossRef] [PubMed]
- Brusselaers, N.; Mattsson, F.; Lagergren, J. Hospital and Surgeon Volume in Relation to Long-Term Survival after Oesophagectomy: Systematic Review and Meta-Analysis. Gut 2014, 63, 1393–1400. [Google Scholar] [CrossRef]
- Kalagara, R.; Norain, A.; Chang, Y.-H.; Stucky, C.-C.; Wasif, N. Association of Textbook Outcome and Surgical Case Volume with Long-Term Survival in Patients Undergoing Surgical Resection for Pancreatic Cancer. J. Am. Coll. Surg. 2022, 235, 829–837. [Google Scholar] [CrossRef]
- Mehta, R.; Paredes, A.Z.; Tsilimigras, D.I.; Moro, A.; Sahara, K.; Farooq, A.; Dillhoff, M.; Cloyd, J.M.; Tsung, A.; Ejaz, A.; et al. Influence of Hospital Teaching Status on the Chance to Achieve a Textbook Outcome after Hepatopancreatic Surgery for Cancer among Medicare Beneficiaries. Surgery 2020, 168, 92–100. [Google Scholar] [CrossRef]
- Khalil, M.; Tsilimigras, D.I.; Endo, Y.; Khan, M.M.M.; Munir, M.M.; Katayama, E.; Rashid, Z.; Resende, V.; Dillhoff, M.; Cloyd, J.; et al. Association of Textbook Outcome and Hospital Volume with Long-Term Survival Following Resection for Hepatocellular Carcinoma: What Matters More? J. Gastrointest. Surg. 2023, 27, 2763–2770. [Google Scholar] [CrossRef]
- Levy, J.; Gupta, V.; Amirazodi, E.; Allen-Ayodabo, C.; Jivraj, N.; Jeong, Y.; Davis, L.E.; Mahar, A.L.; De Mestral, C.; Saarela, O.; et al. Gastrectomy Case Volume and Textbook Outcome: An Analysis of the Population Registry of Esophageal and Stomach Tumours of Ontario (PRESTO). Gastric Cancer 2020, 23, 391–402. [Google Scholar] [CrossRef]
- Sweigert, P.J.; Eguia, E.; Baker, M.S.; Link, C.M.; Hyer, J.M.; Paredes, A.Z.; Tsilimigras, D.I.; Husain, S.; Pawlik, T.M. Assessment of Cancer Center Variation in Textbook Oncologic Outcomes Following Colectomy for Adenocarcinoma. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract 2021, 25, 775–785. [Google Scholar] [CrossRef]
- Russolillo, N.; Gentile, V.; Ratti, F.; Ardito, F.; Serenari, M.; Lombardi, R.; Jovine, E.; Cescon, M.; Giuliante, F.; Aldrighetti, L.; et al. Incidence and Predictors of Textbook Outcome after Simultaneous Liver and Rectal Surgeries for Stage IV Rectal Cancer. Colorectal Dis. 2022, 24, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Tsilimigras, D.I.; Mehta, R.; Merath, K.; Bagante, F.; Paredes, A.Z.; Farooq, A.; Ratti, F.; Marques, H.P.; Silva, S.; Soubrane, O.; et al. Hospital Variation in Textbook Outcomes Following Curative-Intent Resection of Hepatocellular Carcinoma: An International Multi-Institutional Analysis. HPB 2020, 22, 1305–1313. [Google Scholar] [CrossRef] [PubMed]
- van der Werf, L.R.; Wijnhoven, B.P.L.; Fransen, L.F.C.; van Sandick, J.W.; Nieuwenhuijzen, G.A.P.; Busweiler, L.A.D.; van Hillegersberg, R.; Wouters, M.W.J.M.; Luyer, M.D.P.; van Berge Henegouwen, M.I. A National Cohort Study Evaluating the Association Between Short-Term Outcomes and Long-Term Survival After Esophageal and Gastric Cancer Surgery. Ann. Surg. 2019, 270, 868–876. [Google Scholar] [CrossRef] [PubMed]
- Kulshrestha, S.; Bunn, C.; Patel, P.M.; Sweigert, P.J.; Eguia, E.; Pawlik, T.M.; Baker, M.S. Textbook Oncologic Outcome Is Associated with Increased Overall Survival after Esophagectomy. Surgery 2020, 168, 953–961. [Google Scholar] [CrossRef] [PubMed]
- van der Kaaij, R.T.; de Rooij, M.V.; van Coevorden, F.; Voncken, F.E.M.; Snaebjornsson, P.; Boot, H.; van Sandick, J.W. Using Textbook Outcome as a Measure of Quality of Care in Oesophagogastric Cancer Surgery. BJS Br. J. Surg. 2018, 105, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Sweigert, P.J.; Eguia, E.; Baker, M.S.; Paredes, A.Z.; Tsilimigras, D.I.; Dillhoff, M.; Ejaz, A.; Cloyd, J.; Tsung, A.; Pawlik, T.M. Assessment of Textbook Oncologic Outcomes Following Pancreaticoduodenectomy for Pancreatic Adenocarcinoma. J. Surg. Oncol. 2020, 121, 936–944. [Google Scholar] [CrossRef]
- ten Berge, M.G.; Beck, N.; Steup, W.H.; Verhagen, A.F.T.M.; van Brakel, T.J.; Schreurs, W.H.; Wouters, M.W.J.M.; the Dutch Lung Cancer Audit for Surgery Group. Textbook Outcome as a Composite Outcome Measure in Non-Small-Cell Lung Cancer Surgery. Eur. J. Cardiothorac. Surg. 2021, 59, 92–99. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Textbook Outcome (n = 795) | No Textbook Outcome (n = 729) | p-Value | ||
|---|---|---|---|---|
| Age | <75 | 640 (54.4%) | 536 (45.6%) | 0.001 |
| ≥75 | 155 (44.5%) | 193 (55.5%) | ||
| Gender | Female | 401 (52.6%) | 361 (47.4%) | 0.758 |
| Male | 394 (51.7%) | 368 (48.3%) | ||
| ASA | I–II | 526 (56.9%) | 399 (43.1%) | <0.001 |
| III–IV | 269 (44.9%) | 330 (55.1%) | ||
| Tumor location | Cecum | 54 (45.4%) | 65 (54.6%) | 0.356 |
| Ascending colon | 128 (53.3%) | 112 (46.7%) | ||
| Hepatic flexure | 32 (55.2%) | 26 (44.8%) | ||
| Transverse colon | 25 (45.5%) | 30 (54.5%) | ||
| Splenic flexure | 32 (60.4%) | 21 (39.6%) | ||
| Descending colon | 39 (57.4%) | 29 (42.6%) | ||
| Rectosigmoid | 71 (56.8%) | 54 (43.2%) | ||
| Sigmoid colon | 165 (54.5%) | 138 (45.5%) | ||
| Rectum | 249 (49.5%) | 254 (50.5%) | ||
| Colon or rectal cancer | Colon | 546 (53.4%) | 476 (46.6%) | 0.173 |
| Rectum | 249 (49.6%) | 253 (50.4%) | ||
| T stage | T1–T2 | 196 (50.3%) | 194 (49.7%) | 0.411 |
| T3–T4 | 593 (52.7%) | 532 (47.3%) | ||
| N stage | N0 | 466 (51.7%) | 436 (48.3%) | 0.639 |
| N+ | 329 (52.9%) | 293 (47.1%) | ||
| M stage | 0 | 745 (52.6%) | 671 (47.4%) | 0.231 |
| 1 | 50 (46.3%) | 58 (53.7%) | ||
| TNM Stage | 1 | 157 (49.5%) | 160 (50.5%) | 0.308 |
| 2 | 292 (53.0%) | 259 (47.0%) | ||
| 3 | 297 (54.1%) | 252 (45.9%) | ||
| 4 | 49 (45.8%) | 58 (53.2%) | ||
| Surgical approach | Open | 447 (46.7%) | 511 (53.3%) | <0.001 |
| MI | 348 (61.5%) | 218 (38.5%) | ||
| Type of surgery | Right hemicolectomy | 227 (51.0%) | 218 (49.0%) | 0.204 |
| Transverse colectomy | 13 (46.4%) | 15 (53.6%) | ||
| Left hemicolectomy | 93 (55.0%) | 76 (45.0%) | ||
| Sigmoidectomy | 149 (58.0%) | 108 (42.0%) | ||
| Rectosigmoidectomy | 26 (42.6%) | 35 (57.4%) | ||
| Rectal resection | 287 (50.9%) | 277 (49.1%) | ||
| Risk Factor | Odds Ratio | 95% C.I. | p-Value | |
|---|---|---|---|---|
| Age | >75 years | 1.207 | 0.935–1.559 | 0.149 |
| ASA | III–IV | 1.497 | 1.203–1.863 | <0.001 |
| Surgical approach | Minimally invasive | 0.570 | 0.460–0.706 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kryzauskas, M.; Bausys, A.; Abeciunas, V.; Degutyte, A.E.; Bickaite, K.; Bausys, R.; Poskus, T. Achieving Textbook Outcomes in Colorectal Cancer Surgery Is Associated with Improved Long-Term Survival: Results of the Multicenter Prospective Cohort Study. J. Clin. Med. 2024, 13, 1304. https://doi.org/10.3390/jcm13051304
Kryzauskas M, Bausys A, Abeciunas V, Degutyte AE, Bickaite K, Bausys R, Poskus T. Achieving Textbook Outcomes in Colorectal Cancer Surgery Is Associated with Improved Long-Term Survival: Results of the Multicenter Prospective Cohort Study. Journal of Clinical Medicine. 2024; 13(5):1304. https://doi.org/10.3390/jcm13051304
Chicago/Turabian StyleKryzauskas, Marius, Augustinas Bausys, Vilius Abeciunas, Austeja Elzbieta Degutyte, Klaudija Bickaite, Rimantas Bausys, and Tomas Poskus. 2024. "Achieving Textbook Outcomes in Colorectal Cancer Surgery Is Associated with Improved Long-Term Survival: Results of the Multicenter Prospective Cohort Study" Journal of Clinical Medicine 13, no. 5: 1304. https://doi.org/10.3390/jcm13051304
APA StyleKryzauskas, M., Bausys, A., Abeciunas, V., Degutyte, A. E., Bickaite, K., Bausys, R., & Poskus, T. (2024). Achieving Textbook Outcomes in Colorectal Cancer Surgery Is Associated with Improved Long-Term Survival: Results of the Multicenter Prospective Cohort Study. Journal of Clinical Medicine, 13(5), 1304. https://doi.org/10.3390/jcm13051304