Spinal Postures and Mobility in Children with Achondroplasia vs. Age- and Sex-Matched Healthy Individuals: A Preliminary Report

 ,
, 
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measurements
2.3. Data Processing
2.4. Statistical Analysis
3. Results
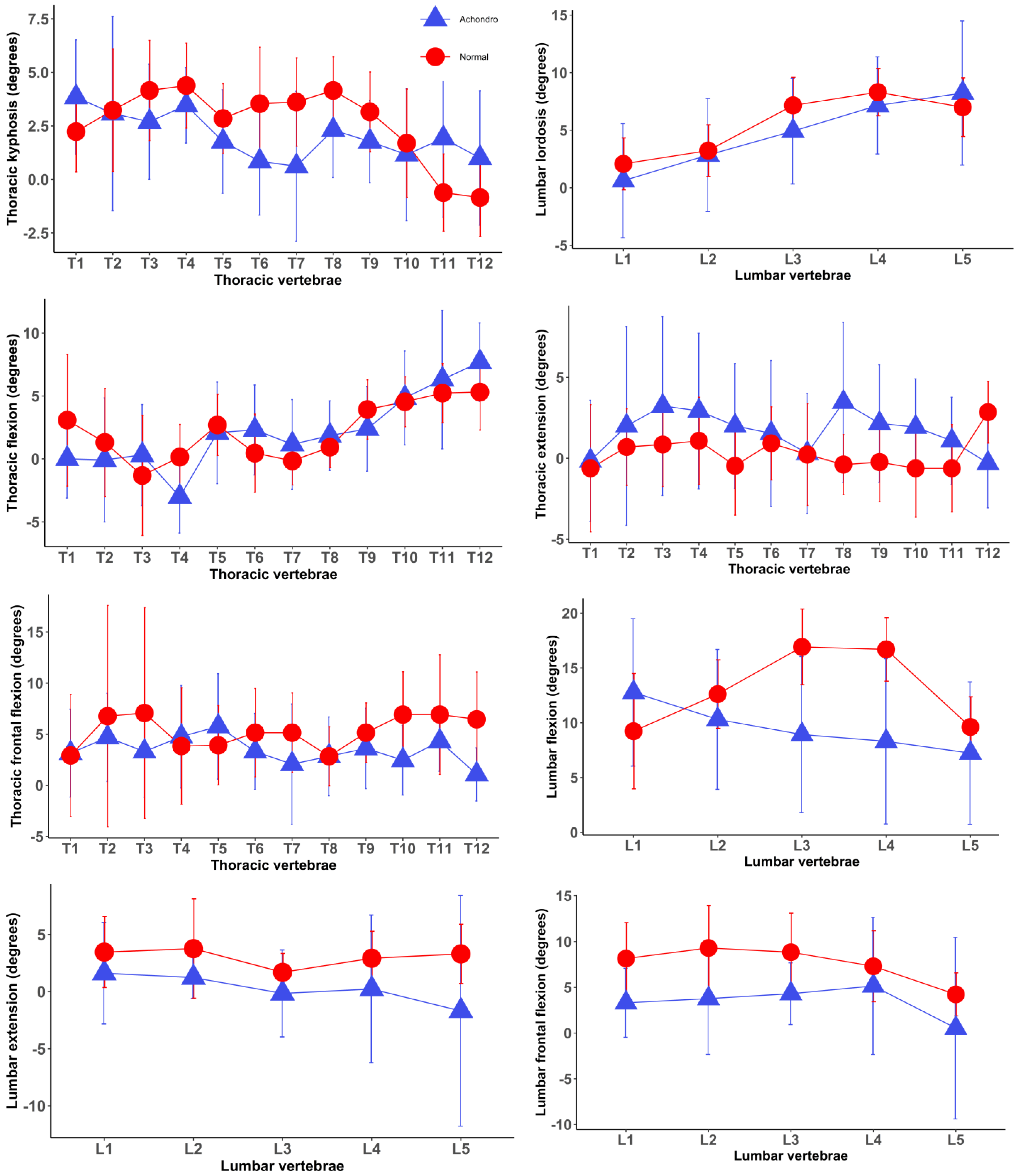
Associations of Achondroplastic Traits with Spinal Posture and Movements as well as Hip Motion
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Horton, W.A.; Hall, J.G.; Hecht, J.T. Achondroplasia. Lancet 2007, 370, 162–172. [Google Scholar] [CrossRef]
- Pauli, R.M. Achondroplasia: A comprehensive clinical review. Orphanet J. Rare Dis. 2019, 14, 1. [Google Scholar] [CrossRef] [PubMed]
- Ireland, P.J.; Pacey, V.; Zankl, A.; Edwards, P.; Johnston, L.M.; Savarirayan, R. Optimal management of complications associated with achondroplasia. Appl. Clin. Genet. 2014, 7, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Waller, D.K.; Correa, A.; Vo, T.M.; Wang, Y.; Hobbs, C.; Langlois, P.H.; Pearson, K.; Romitti, P.A.; Shaw, G.M.; Hecht, J.T. The population-based prevalence of achondroplasia and thanatophoric dysplasia in selected regions of the US. Am. J. Med. Genet. A 2008, 146a, 2385–2389. [Google Scholar] [CrossRef] [PubMed]
- Foreman, P.K.; van Kessel, F.; van Hoorn, R.; van den Bosch, J.; Shediac, R.; Landis, S. Birth prevalence of achondroplasia: A systematic literature review and meta-analysis. Am. J. Med. Genet. A 2020, 182, 2297–2316. [Google Scholar] [CrossRef] [PubMed]
- Baujat, G.; Legeai-Mallet, L.; Finidori, G.; Cormier-Daire, V.; Le Merrer, M. Achondroplasia. Best. Pract. Res. Clin. Rheumatol. 2008, 22, 3–18. [Google Scholar] [CrossRef]
- Kopits, S.E. Orthopedic aspects of achondroplasia in children. Basic. Life Sci. 1988, 48, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Hoover-Fong, J.; Cheung, M.S.; Fano, V.; Hagenas, L.; Hecht, J.T.; Ireland, P.; Irving, M.; Mohnike, K.; Offiah, A.C.; Okenfuss, E.; et al. Lifetime impact of achondroplasia: Current evidence and perspectives on the natural history. Bone 2021, 146, 115872. [Google Scholar] [CrossRef] [PubMed]
- Bedeschi, M.F.; Mora, S.; Antoniazzi, F.; Boero, S.; Ravasio, R.; Scarano, G.; Selicorni, A.; Sessa, M.; Verdoni, F.; Zampino, G.; et al. The clinical management of children with achondroplasia in Italy: Results of clinician and parent/caregiver surveys. J. Endocrinol. Investig. 2024, 47, 345–356. [Google Scholar] [CrossRef]
- Ireland, P.J.; McGill, J.; Zankl, A.; Ware, R.S.; Pacey, V.; Ault, J.; Savarirayan, R.; Sillence, D.; Thompson, E.M.; Townshend, S.; et al. Functional performance in young Australian children with achondroplasia. Dev. Med. Child. Neurol. 2011, 53, 944–950. [Google Scholar] [CrossRef]
- Kitoh, H.; Kitakoji, T.; Kurita, K.; Katoh, M.; Takamine, Y. Deformities of the elbow in achondroplasia. J. Bone Jt. Surg. Br. 2002, 84, 680–683. [Google Scholar] [CrossRef]
- Kopits, S.E. Thoracolumbar kyphosis and lumbosacral hyperlordosis in achondroplastic children. Basic. Life Sci. 1988, 48, 241–255. [Google Scholar] [CrossRef] [PubMed]
- Sadler, S.G.; Spink, M.J.; Ho, A.; De Jonge, X.J.; Chuter, V.H. Restriction in lateral bending range of motion, lumbar lordosis, and hamstring flexibility predicts the development of low back pain: A systematic review of prospective cohort studies. BMC Musculoskelet. Disord. 2017, 18, 179. [Google Scholar] [CrossRef] [PubMed]
- Al Kaissi, A.; Ganger, R.; Klaushofer, K.; Rumpler, M.; Grill, F. Achondroplasia manifesting as enchondromatosis and ossification of the spinal ligaments: A case report. J. Med. Case Rep. 2008, 2, 263. [Google Scholar] [CrossRef] [PubMed]
- Livanelioglu, A.; Kaya, F.; Nabiyev, V.; Demirkiran, G.; Fırat, T. The validity and reliability of “Spinal Mouse” assessment of spinal curvatures in the frontal plane in pediatric adolescent idiopathic thoraco-lumbar curves. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2016, 25, 476–482. [Google Scholar] [CrossRef] [PubMed]
- Mannion, A.F.; Knecht, K.; Balaban, G.; Dvorak, J.; Grob, D. A new skin-surface device for measuring the curvature and global and segmental ranges of motion of the spine: Reliability of measurements and comparison with data reviewed from the literature. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2004, 13, 122–136. [Google Scholar] [CrossRef] [PubMed]
- Bayartai, M.E.; Schaer, C.E.; Luomajoki, H.; Tringali, G.; De Micheli, R.; Sartorio, A. Differences in spinal posture and mobility between children/adolescents with obesity and age-matched normal-weight individuals. Sci. Rep. 2022, 12, 15570. [Google Scholar] [CrossRef] [PubMed]
- Kellis, E.; Adamou, G.; Tzilios, G.; Emmanouilidou, M. Reliability of spinal range of motion in healthy boys using a skin-surface device. J. Manip. Physiol. Ther. 2008, 31, 570–576. [Google Scholar] [CrossRef] [PubMed]
- Nouh, M.R. Imaging of the spine: Where do we stand? World J. Radiol. 2019, 11, 55–61. [Google Scholar] [CrossRef]
- Guermazi, M.; Ghroubi, S.; Kassis, M.; Jaziri, O.; Keskes, H.; Kessomtini, W.; Ben Hammouda, I.; Elleuch, M.H. Validity and reliability of Spinal Mouse to assess lumbar flexion. Ann. Readapt. Med. Phys. 2006, 49, 172–177. [Google Scholar] [CrossRef]
- R Core Team, R. A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Chan, B.K.C. Data Analysis Using R Programming. In Biostatistics for Human Genetic Epidemiology; Chan, B.K.C., Ed.; Springer International Publishing: Cham, Switzerland, 2018; pp. 47–122. [Google Scholar]
- Odeh, O.O.; Featherstone, A.M.; Bergtold, J.S. Reliability of Statistical Software. Am. J. Agric. Econ. 2010, 92, 1472–1489. [Google Scholar] [CrossRef]
- Lenth, R.V. Emmeans: Estimated Marginal Means, Aka Least-Squares Means. R Package Version 1.6.3. 2021. Available online: https://cran.r-project.org/package=emmeans (accessed on 27 March 2024).
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Siebens, A.A.; Hungerford, D.S.; Kirby, N.A. Curves of the achondroplastic spine: A new hypothesis. Johns. Hopkins Med. J. 1978, 142, 205–210. [Google Scholar] [PubMed]
- Sung, Y.B.; Lee, J.H.; Park, Y.H. Effects of thoracic mobilization and manipulation on function and mental state in chronic lower back pain. J. Phys. Ther. Sci. 2014, 26, 1711–1714. [Google Scholar] [CrossRef] [PubMed]
- Mizoguchi, Y.; Akasaka, K.; Otsudo, T.; Shimada, N.; Naka, H. Efficacy of semi-customized exercises in preventing low back pain in high school volleyball players: A randomized controlled trial. Medicine 2022, 101, e30358. [Google Scholar] [CrossRef] [PubMed]
- Johnson, K.D.; Grindstaff, T.L. Thoracic region self-mobilization: A clinical suggestion. Int. J. Sports Phys. Ther. 2012, 7, 252–256. [Google Scholar] [PubMed]
- Panjabi, M.M. Clinical spinal instability and low back pain. J. Electromyogr. Kinesiol. Off. J. Int. Soc. Electrophysiol. Kinesiol. 2003, 13, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Mansfield, P.J.; Neumann, D.A. Chapter 9—Structure and Function of the Hip. In Essentials of Kinesiology for the Physical Therapist Assistant, 3rd ed.; Mansfield, P.J., Neumann, D.A., Eds.; Mosby: St. Louis, MO, USA, 2019; pp. 233–277. [Google Scholar]
- Broström, E.W.; Antonissen, L.; von Heideken, J.; Esbjörnsson, A.-C.; Hagenäs, L.; Naili, J.E. Gait in children with achondroplasia—A cross-sectional study on joint kinematics and kinetics. BMC Musculoskelet. Disord. 2022, 23, 397. [Google Scholar] [CrossRef] [PubMed]
- Roach, S.M.; San Juan, J.G.; Suprak, D.N.; Lyda, M.; Bies, A.J.; Boydston, C.R. Passive hip range of motion is reduced in active subjects with chronic low back pain compared to controls. Int. J. Sports Phys. Ther. 2015, 10, 13–20. [Google Scholar]
- Godges, J.J.; Macrae, H.; Longdon, C.; Tinberg, C.; Macrae, P.G. The effects of two stretching procedures on hip range of motion and gait economy. J. Orthop. Sports Phys. Ther. 1989, 10, 350–357. [Google Scholar] [CrossRef]
- Ingber, R.S. Iliopsoas myofascial dysfunction: A treatable cause of “failed” low back syndrome. Arch. Phys. Med. Rehabil. 1989, 70, 382–386. [Google Scholar] [PubMed]


{kind=link}
| Variables | Children with Achondroplasia (N = 13) | Healthy Children (N = 13) | p-Value |
|---|---|---|---|
| Age (years) | 10.6 (2.8) | 11.1 (2.6) | 0.57 w |
| Sex (female) | 38% | 38% | 1 c |
| Weight (kg) | 25.9 (9.6) | 41.3 (14.0) | 0.003 I |
| Height (cm) | 110.1 (18.1) | 146.3 (15.3) | <0.0001 I |
| BMI (kg/m2) | 20.7 (2.6) | 18.6 (2.7) | 0.06 I |
| Spinal length (mm) | 353.1 (46.4) | 387.7 (41.0) | 0.56 I |
| Variables | Children with Achondroplasia n = 13 | Healthy Children n = 13 | Differences in Spinal Posture and Mobility (95% CI) | p-Value | ||
|---|---|---|---|---|---|---|
| EMM | SE | EMM | SE | |||
| Spinal postures | ||||||
| Thoracic Kyphosis (Th1-12) | 25.1 | 3.9 | 31.2 | 3.9 | −6.1 (−17.6 to 5.3) | 0.27 |
| Lumbar lordosis | 23.4 | 3.8 | 27.7 | 3.8 | −4.3 (−6.8 to 15.5) | 0.43 |
| Sacral kyphosis | 15.8 | 3.4 | 17.9 | 3.4 | −2.1 (−12.1 to 7.9) | 0.66 |
| Posture of each individual spinal segment | ||||||
| T1/2 | 3.9 | 0.6 | 2.2 | 0.6 | 1.6 (−0.6 to 3.6) | 0.08 |
| T2/3 | 3.3 | 1.1 | 3.3 | 1.1 | 0.001 (−3.1 to 3.1) | 0.99 |
| T3/4 | 2.8 | 0.6 | 4.4 | 0.6 | −1.6 (−3.5 to 0.2) | 0.08 |
| T4/5 | 3.4 | 0.5 | 4.3 | 0.5 | −0.8 (−2.4 to 0.7) | 0.26 |
| T5/6 | 1.8 | 0.6 | 2.8 | 0.6 | −1.1 (−2.8 to 0.7) | 0.22 |
| T6/7 | 0.6 | 0.6 | 3.2 | 0.6 | −2.6 (−4.6 to −0.6) | 0.01 * |
| T7/8 | 0.8 | 0.8 | 3.7 | 0.8 | −2.9 (−5.2 to −0.6) | 0.02 * |
| T8/9 | 2.2 | 0.5 | 4.0 | 0.5 | −1.8 (−3.4 to −0.2) | 0.02 * |
| T9/10 | 1.9 | 0.5 | 3.1 | 0.5 | −1.2 (−2.6 to 0.2) | 0.08 |
| T10/11 | 1.3 | 0.8 | 1.7 | 0.8 | −0.4 (−2.7 to 1.8) | 0.71 |
| T11/12 | 2.7 | 0.8 | −0.5 | 0.8 | 2.7 (0.4 to 4.9) | 0.02 * |
| T12/L1 | 1.2 | 0.6 | −0.7 | 0.6 | 2.0 (0.1 to 3.9) | 0.03 * |
| L1/2 | −0.5 | 1.1 | −1.9 | 1.1 | 1.4 (−1.8 to 4.7) | 0.36 |
| L2/3 | −2.9 | 1.1 | −3.4 | 1.1 | 0.5 (−2.7 to 3.6) | 0.75 |
| L3/4 | −4.8 | 1.0 | −7.3 | 1.0 | 2.4 (−0.5 to 5.4) | 0.11 |
| L4/5 | −7.2 | 0.9 | −8.4 | 0.9 | 1.3 (−1.5 to 4.0) | 0.35 |
| L5/S1 | −8.4 | 1.4 | −7.1 | 1.4 | −1.3 (−5.3 to 2.8) | 0.52 |
| Spinal mobility | ||||||
| Thoracic (°) | ||||||
| Flexion | 24.3 | 4.2 | 25.6 | 4.2 | −1.3 (−13.6 to 11.0) | 0.83 |
| Extension | 19.4 | 4.2 | 2.9 | 4.2 | 16.5 (4.4 to 28.7) | 0.009 * |
| Lateral flexion | 41.1 | 6.9 | 61.4 | 6.9 | −20.4 (−40.6 to −0.1) | 0.04 * |
| Lumbar (°) | ||||||
| Flexion | 47.0 | 4.1 | 64.4 | 4.1 | −17.4 (−29.4 to −5.4) | 0.006 * |
| Extension | 1.7 | 2.9 | 15.9 | 2.9 | −14.2 (−22.8 to −5.7) | 0.002 * |
| Lateral flexion | 17.3 | 3.0 | 36.9 | 3.0 | −19.6 (−28.4 to −10.7) | 0.0001 * |
| Hip mobility | ||||||
| Hip (°) | ||||||
| Flexion | 43.7 | 5.8 | 41.7 | 5.8 | 2.0 (−14.9 to 18.9) | 0.81 |
| Extension | 5.2 | 3.3 | 17.1 | 3.3 | −11.9 (−2.4 to −21.5) | 0.01 * |
| Lumbar-to-hip ratio | 0.5 | 0.04 | 0.6 | 0.04 | −0.08 (−0.22 to 0.05) | 0.22 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bayartai, M.-E.; Luomajoki, H.; Aliverti, A.; LoMauro, A.; Tringali, G.; Sartorio, A. Spinal Postures and Mobility in Children with Achondroplasia vs. Age- and Sex-Matched Healthy Individuals: A Preliminary Report. J. Clin. Med. 2024, 13, 2135. https://doi.org/10.3390/jcm13072135
Bayartai M-E, Luomajoki H, Aliverti A, LoMauro A, Tringali G, Sartorio A. Spinal Postures and Mobility in Children with Achondroplasia vs. Age- and Sex-Matched Healthy Individuals: A Preliminary Report. Journal of Clinical Medicine. 2024; 13(7):2135. https://doi.org/10.3390/jcm13072135
Chicago/Turabian StyleBayartai, Munkh-Erdene, Hannu Luomajoki, Andrea Aliverti, Antonella LoMauro, Gabriella Tringali, and Alessandro Sartorio. 2024. "Spinal Postures and Mobility in Children with Achondroplasia vs. Age- and Sex-Matched Healthy Individuals: A Preliminary Report" Journal of Clinical Medicine 13, no. 7: 2135. https://doi.org/10.3390/jcm13072135